UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
Form 10-K
(Mark One)
| x | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended December 31, 2013
OR
| ¨ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from_______to_______
Commission file number: 000-53012
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
(Exact name of registrant as specified in its charter)
Delaware (State or other jurisdiction of incorporation or organization) | | 90-0687379 (I.R.S. Employer Identification No.) |
| | | |
709 S. Harbor City Blvd., Suite 250, Melbourne, FL (Address of principal executive offices) | | 32901 (Zip Code) |
Registrant’s telephone number, including area code(321) 725-0090
Securities registered pursuant to Section 12(b) of the Act:
| Title of each class | | Name of each exchange on which registered |
| N/A | | N/A |
Securities registered pursuant to Section 12(g) of the Act:
Common Stock, par value $0.001 per share
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yeso Nox
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or 15(d) of the Act. Yeso Nox
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. YesxNoo
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate website, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes x No o
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K (§ 229.405 of this chapter) is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K.o
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of “large accelerated filer,” “accelerated filer” and “smaller reporting company��� in Rule 12b-2 of the Exchange Act.
Large accelerated filero Accelerated filer o Non-accelerated filer o Smaller reporting company x
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Act). Yeso Nox
The aggregate market value of the voting and non-voting common equity held by non-affiliates computed by reference to the price at which the common equity was last sold as of the last business day of the registrant’s most recently completed second fiscal quarter was $4,844,685.
As of March 27, 2014, there were 16,793,248 shares of common stock, par value $0.001 per share, outstanding.
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
TABLE OF CONTENTS
| | | | Page |
| | | | | |
| | PART I | | | |
| | | | | |
| Item 1. | Business | | | 1 |
| Item 1A. | Risk Factors | | | 12 |
| Item 1B. | Unresolved Staff Comments | | | 23 |
| Item 2. | Properties | | | 23 |
| Item 3. | Legal Proceedings | | | 24 |
| Item 4. | Mine Safety Disclosures | | | 24 |
| | | | | |
| | PART II | | | |
| | | | | |
| Item 5. | Market for Registrant's Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities | | | 24 |
| Item 6. | Selected Financial Data | | | 27 |
| Item 7. | Management's Discussion and Analysis of Financial Condition and Results of Operations | | | 27 |
| Item 7A. | Quantitative and Qualitative Disclosures about Market Risk | | | 34 |
| Item 8. | Financial Statements and Supplementary Data | | | 34 |
| Item 9. | Changes in and Disagreements with Accountants on Accounting and Financial Disclosure | | | 34 |
| Item 9A. | Controls and Procedures | | | 34 |
| Item 9B. | Other Information | | | 35 |
| | | | | |
| | PART III | | | |
| | | | | |
| Item 10. | Directors, Executive Officers and Corporate Governance | | | 35 |
| Item 11. | Executive Compensation | | | 38 |
| Item 12. | Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters | | | 39 |
| Item 13. | Certain Relationships and Related Transactions, and Director Independence | | | 42 |
| Item 14. | Principal Accounting Fees and Services | | | 43 |
| | | | | |
| | PART IV | | | |
| | | | | |
| Item 15. | Exhibits, Financial Statement Schedules | | | 44 |
PART I
This report may contain forward-looking statements within the meaning of Securities Act of 1933, as amended, or the Securities Exchange Act of 1934, as amended, or the Private Securities Litigation Reform Act of 1995. Investors are cautioned that such forward-looking state to all comments are based on our management’s beliefs and assumptions and on information currently available to our management and involve risks and uncertainties. Forward-looking statements include statements regarding our plans, strategies, objectives, expectations and intentions, which are subject to change at any time at our discretion. Forward-looking statements include our assessment, from time to time of our competitive position, the industry environment, potential growth opportunities and the effects of regulation. Forward-looking statements include all statements that are not historical facts and can be identified by terms such as “anticipates,” “believes,” “could,” “estimates,” “expects,” “hopes,” “intends,” “may,” “plans,” “potential,” “predicts,” “projects,” “should,” “will,” “would” or similar expressions.
Forward-looking statements involve known and unknown risks, uncertainties and other factors which may cause our actual results, performance or achievements to be materially different from any future results, performance or achievements expressed or implied by the forward-looking statements. We discuss many of these risks in greater detail in “Risk Factors.” Given these uncertainties, you should not place undue reliance on these forward-looking statements. Also, forward-looking statements represent our management’s beliefs and assumptions only as of the date of this report. You should read this report and the documents that we reference in this report and have filed as exhibits to the report completely and with the understanding that our actual future results may be materially different from what we expect. Except as required by law, we assume no obligation to update these forward-looking statements publicly, or to update the reasons actual results could differ materially from those anticipated in these forward-looking statements, even if new information becomes available in the future.
ITEM 1. BUSINESS
History
First Choice Healthcare Solutions, Inc.’s (“FCHS,” “the Company,” “we,” “our” or “us”) mission is to transform, via acquisition and restructuring, multi-specialty clinics or physician-owned practices in the southeastern United States into world class, state-of-the-art medical centers of excellence, thereby establishing and extending ‘First Choice Healthcare Solutions’ brand and reputation as a profitable, well-managed enterprise committed to improving the quality of lives of the caregivers it employs and the health and wellness of the patients and families it serves.
We were incorporated in the State of Colorado on May 2007. In February 2012, we completed a merger with First Choice Healthcare Solutions, Inc., a Delaware corporation formed exclusively for the purpose of merging with the Company, pursuant to which (a) the Company’s state of incorporation changed from Colorado to Delaware (the “Reincorporation”) and (b) the Company’s name changed from Medical Billing Assistance, Inc. to First Choice Healthcare Solutions, Inc.
Our Business
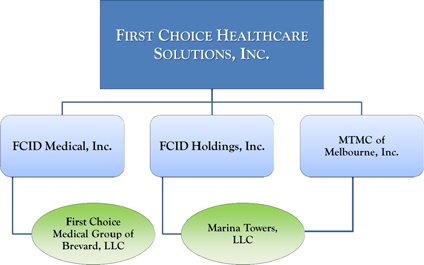
The Company operates in two segments, healthcare services and real estate, through five wholly-owned subsidiaries:
| · | FCID Medical, Inc., which is the subsidiary under which our present center of excellence is owned and operated and future centers of excellence will be owned and operated; |
| · | First Choice Medical Group of Brevard, LLC, which is the Company’s flagship medical center of excellence located in Melbourne, Florida, wholly-owned and operated by FCID Medical, Inc.; |
| · | FCID Holdings, Inc. which operates the Company’s real estate interests, and owns a 99% interest in Marina Towers, LLC; |
| · | MTMC of Melbourne, Inc., which owns a 1% ownership stake in Marina Towers, LLC; and |
| · | Marina Towers, LLC, which owns and operates Marina Towers, a Class A, 78,000 square foot, six-story building located on the Indian River in Melbourne, Florida. |
Diagram 1. First Choice Healthcare Solutions, Inc. Legal Corporate Structure
By distinguishing our medical centers of excellence as premier destinations for clinically superior, patient-centric care that is coordinated across a patient’s care continuum, we expect to deliver more meaningful and collaborative doctor-patient experiences, accurate diagnoses, effective treatment plans, faster recoveries and materially reduced costs. Currently, our strategic focus is to grow in the southeastern United States through selective employment of physicians and/or the acquisition of physician practices that fit our defined acquisition criteria, including the following:
| · | presents the opportunity for FCHS to introduce additional ancillary revenue channels (i.e. on-site magnetic resonance imaging (MRI), X-ray, physical therapy, diagnostic equipment, synergistic medical disciplines, durable medical equipment (DME), related health and wellness products, etc.) that will support and promote enhanced, well-coordinated, patient-centric care while supporting and promoting profitable business operations; |
| · | due diligence supporting economies of scale in billing, collections, purchasing, advertising and compliance that can be fully leveraged to reduce expenses and fuel income growth; and |
| · | creates the opportunity to increase awareness of FCHS’s brand; and aligns with and materially complements our Company’s inherent value proposition to patients, referring physicians and medical institutions, insurers, employers and other healthcare stakeholders in the local markets we serve. |
Healthcare Services
Model for Medical Centers of Excellence
FCHS’s model for each medical center of excellence is strictly defined to ensure that our high standards for patient care and attention can be fostered and preserved. Ideally, a center will:
| · | employ, on average, ten specialty physicians – all of whom are subject to a rigorous qualification and hiring process; |
| · | provide for the combination of synergistic medical disciplines and supported by related in-house ancillary diagnostic services and technologies, i.e. orthopedics/neurology/interventional pain medicine; |
| · | be capable of generating $16-$20 million when operating at optimal economic capacity; and |
| · | be housed in a commercial building, in close geographic proximity to a primary hospital(s), and allows for 12,000-16,000 square feet of usable space for build-out consideration. |
Because FCHS’s leadership view themselves as guardians of their ideals relating to optimal patient experience of care, we continually reinforce the importance of hiring, training, evaluating, compensating and supporting a workforce committed to patient-centered care. Just as vital, we engage our employees in all aspects of process design and treat them with the same dignity and respect that they are expected to show patients and family members. Central to the success of our Company’s long term growth strategy is attracting and recruiting top tier physicians and care specialists that rank in the top percentile of performance in the local markets we serve; and creating a work environment and corporate culture that serves to engage, motivate and retain them.
Due to sweeping healthcare reform, increased regulatory and reimbursement mandates and the financial challenges each of these impose, remaining in private practice is quickly losing its appeal for many physicians. In fact, according to a nationwide survey published in 2013 by recruiting firm Jackson Healthcare, one-third of U.S. physicians plan to leave private medical practice within the next ten years in favor of employment by hospitals and multi-specialty medical groups. Thus, the opportunity for our Company to attract key medical talent has never been more robust.
Our systems of operation unburden the Company’s physicians from productivity-driven, assembly line medicine, and materially diminish the cognitive overload and exhaustion that makes medical care anything but caring or patient-centered. More specifically, the many advantages and benefits of choosing employment by FCHS are being enabled to focus exclusively on delivering excellent patient care; higher income potential; freedom from day-to-day practice administration, including marketing and generating new patient leads; access to state-of-the-art technology, diagnostics and services; and camaraderie and collaboration with a cadre of first rate caregivers dedicated to common, patient-centered goals and objectives. The requirements for running the day-to-day business functions of the centers are the sole responsibility of our management team – and not the physicians. Simply put, doctors get to be doctors.
Currently, we are actively engaged in identifying and pursuing discussions with prospective acquisitions in key target markets – with those being largely in the southeastern U.S. We anticipate investing $4-$6 million to acquire and/or develop one or more medical centers of excellence during the next 12 months, each center may require up to 6-12 months to achieve optimal economic capacity, depending on the number of physicians and physician assistants to be employed, the medical service mix and the type of diagnostic and ancillary services to be offered. However, there can be no assurance that we will be able to negotiate acceptable terms for, or find suitable candidates for, such acquisition.
Medical Service Mix
Like other successful business models for professional medical services, ours is designed to offer the most synergistic and profitable medical service mix. By their nature, some combinations of medical specialties can be more revenue positive than others. Physicians need access to diagnostic equipment and ancillary services, such as MRI, X-ray, DME and physical therapy. Moreover, patients expect their physicians to have access to the best diagnostic and service delivery equipment. Without diagnostic services, many medical practices will find it difficult to maintain their current margins of profitability.
We integrate both medical specialties and diagnostic/ancillary services in our centers to maintain or enhance our profits. While one specialty may have high reimbursements for their professional service but insufficient volume to profitably support the necessary ancillary services, another medical specialty may have a lower professional service reimbursement but high volume ancillary services use. Operating independently, each specialty group would face retreating profit margins and confront significant challenges to maintaining high service levels with adequate equipment and current technologies. However, operating together, they create the optimal mix of professional service fee income and ancillary services income. Since the combination is more profitable than either of its components, there is a favorable opportunity to sustain profit margins that will allow each center to maintain high service levels with state-of-the-art equipment and technologies.
Scalable Back Office and Economies of Scale
Fixed cost legacy administrative functions have subjected many established medical centers to a downward spiral of diminishing profit margins and losses. In legacy medical centers, administrative management, billing, compliance, accounting, marketing, advertising, scheduling, customer service and record keeping functions represent fixed overhead for the practice. The fixed administrative overhead of a practice has the effect of reducing profit margins as the practice experiences declining revenues as a result of lower patient volumes from increasing competition, lower pricing, lower reimbursements or loss of patients to competitors.
A key to our success is our ability to employ a highly experienced team of business managers supported by an array of professional, experienced and healthcare compliant subcontractors. Using the best project management practices, our business managers contract services for billing, compliance, accounting, marketing, advertising, legal, information technology and record keeping functions. The cost of our ‘back office operation’ does not increase in direct relation to our volume, allowing us to sustain profit margins with a cost effective and scalable back office. As the number of physicians increases, so do the economies of scale for our back office. The economies of scale support selecting the best in class subcontractors, while allowing our medical centers of excellence to operate cost effectively with higher service levels.
Specifically, we provide all of the administrative services to support the practice of medicine by our physicians and improve operating efficiencies of our medical centers of excellence:
| · | Recruiting and Credentialing. We have proven experience in locating, qualifying, recruiting and retaining experienced physicians. In addition to the verification of credentials, licenses and references of all prospective physician candidates, each caregiver undergoes level two background checks. We maintain a national database of practicing physicians In addition to our database of physicians, we recruit locally through trade advertising, the American Academy of Orthopaedic Surgeons and referrals from our physicians. |
| · | Billing, Collection and Reimbursement. We assume responsibility for contracting with third-party payors for all of our physicians; and we are responsible for billing, collection and reimbursement for services rendered by our physicians. In all instances, however, we do not assume responsibility for charges relating to services provided by hospitals or other referring physicians with whom we collaborate. Such charges are separately billed and collected by the hospitals or other physicians. The majority of our third party payors remit by EFT and wire transfers. Accordingly, every aspect of the business is positioned to achieve high productivity and lower administrative headcounts and per capita expense. We provide our physicians with a training curriculum that emphasizes detailed documentation of and proper coding protocol for all procedures performed and services provided, and we provide comprehensive internal auditing processes, all of which are designed to achieve appropriate coding, billing and collection of revenue for physician services. All of our billing and collection operations are controlled and will continue to be controlled from our business offices located at our corporate headquarters in Melbourne, Florida. |
| · | Risk Management and Other Services. We maintain a risk management program focused on reducing risk, including the identification and communication of potential risk areas to our medical staff. We maintain professional liability coverage for our group of healthcare professionals. Through our risk management staff, we conduct risk management programs for loss prevention and early intervention in order to prevent or minimize professional liability claims. In addition, we provide a multi-faceted compliance program that is designed to assist our multi-specialty centers of excellence in complying with increasingly complex laws and regulations. We also manage all information technology, facilities management, legal support, marketing support, regulatory compliance and other services. |
Developing and operating additional multi-specialty medical centers of excellence in other geographic areas will take advantage of the economies of scale for our administrative back office functions. Our plan calls for opening up multiple centers in multiple states and cities at a pace that will allow us to maintain the same levels of quality and acceptable profitability from each location. We believe that the scalable structure of our administrative back office functions will efficiently support our expansion plans.
High Technology Infrastructure Supporting High Touch Patient Experiences
Successful retail models in other industries already effectively use telecommunications, remote computing, mobile computing, cloud computing, virtual networks and other leading-edge technologies to manage geographically diverse operating units. These technologies create the infrastructure to allow a central management team to monitor, direct and control geographically dispersed operating units and subcontractors, including national operations.
We believe that the FCHS business model incorporates the best of these technologies. A central management team monitors, directs and controls our multi-specialty medical centers of excellence and all the necessary support subcontractors. FCMG’s administrative operations center on a secure paperless practice management platform. We utilize a state-of-the-art, cloud-based electronic medical record (“EMR”) management system, which provides 24/7, secure, online access to each patient’s test results from virtually anywhere in world, including X-ray and MRI images, diagnosis, patient and doctor notes, visit reports, billing information, insurance coverage, patient identification and personalized care delivery requirements. Our EMR system fully complies with all stages of Meaningful Use standards defined by the Centers for Medicare & Medicaid Services Incentive Programs. These programs govern the use of electronic health records and allow us to earn incentive payments from the U.S. government, pursuant to the Health Information Technology for Economic and Clinical Health (HITECH) Act, which was enacted as part of the American Recovery and Reinvestment Act of 2009. See “HIPAA and Other Privacy Laws.”
We intend to grow by replicating our multi-specialty medical centers of excellence, supported by our standardized policies, procedures and clinic setup guidelines. The administrative functions can be quickly scaled to handle multiple additional centers. As we roll out our business model, we expect our administrative core and clinic retail model to maintain economies of scale for all of our multi-specialty medical centers of excellence.
Referral and Partnering Relationships
Our business model is influenced by the direct contact and daily interaction that our physicians have with their patients, and emphasizes a patient-centric, shared clinical approach that also serves to address the needs of our various “partners,” including hospitals, third-party payors and referring physicians, our physicians and, most importantly, our patients. Our relationships with all of our partners are important to our continued success.
Hospitals
Our relationships with our hospital partners are critical to our operations. We work with our hospital partners to enhance their reputation and market our services to referring physicians, an important source of hospital admissions, within the communities served by those hospitals. In addition, a majority of our physicians maintain regular hospital privileges, as well as trauma privileges where available, to ensure best in class is available to our patients and the community. Under our contracts with hospitals, we are responsible for billing patients and third-party payors for services rendered by our physicians separately from other related charges billed by the hospital or other physicians within the hospital to the same payors.
Third-Party Payors
Our relationships with government-sponsored plans, including Medicare and TRICARE, managed care organizations and commercial health insurance payors are vital to our business. We seek to maintain professional working relationships with our third-party payors, streamline the administrative process of billing and collection, and assist our patients and their families in understanding their health insurance coverage and any balances due for co-payments, co-insurance, deductibles or out-of-network benefit limitations. In addition, through our quality initiatives and continuing research and education efforts, we have sought to enhance clinical care provided to patients, which we believe benefits third-party payors by contributing to improved patient outcomes and reduced long-term health system costs.
We receive compensation for professional services provided by our physicians to patients based upon rates for specific services provided, principally from third-party payors. Our billed charges are substantially the same for all parties in a particular geographic area, regardless of the party responsible for paying the bill for our services. Approximately one-third of our net patient service revenue is received from government-sponsored plans, principally Medicare and TRICARE programs.
Medicare is a health insurance program primarily for individuals 65 years of age and older, certain younger people with disabilities and people with end-stage renal disease. The program is provided without regard to income or assets and offers beneficiaries different ways to obtain their medical benefits. The most common option selected today by Medicare beneficiaries is the traditional fee-for-service payment system. The other options include managed care, preferred provider organizations, private fee-for-service and specialty plans. TRICARE is the healthcare program for U.S. military service members (active, Guard/Reserve and retired) and their families around the world. TRICARE is managed by the Defense Health Agency under leadership of the Assistant Secretary of Defense. Both Medicare and TRICARE compensation rates are generally lower in comparison to commercial health plans. In order to participate in government programs, our center of medical excellence must comply with stringent and often complex enrollment and reimbursement requirements.
We also receive compensation pursuant to contracts with commercial payors that offer a wide variety of health insurance products, such as health maintenance organizations, preferred provider organizations and exclusive provider organizations that are subject to various state laws and regulations, as well as self-insured organizations subject to federal Employee Retirement Income Security Act (“ERISA”) requirements. We seek to secure mutually agreeable contracts with payors that enable our physicians to be listed as in-network participants within the payors’ provider networks
If we do not have a contractual relationship with a health insurance payor, we generally bill the payor our full billed charges. If payment is less than billed charges, we bill the balance to the patient, subject to state and federal laws regulating such billing. Although we maintain standard billing and collections procedures, we also provide discounts and/or payment option plans in certain hardship situations where patients and their families do not have financial resources necessary to pay the amount due at the time services are rendered. Any amounts written-off related to private-pay patients are based on the specific facts and circumstances related to each individual patient account.
Referring Physicians and Practice Groups
Our relationships with our referring physicians and referring practice groups are critical to our success. Our physicians seek to establish and maintain long-term professional relationships with referring physicians in the communities where we practice. We believe that our community presence, through our hospital coverage and medical centers of excellence, assists referring physicians with further enhancing their practices by providing well-coordinated and highly responsive care to their patients who require our musculoskeletal services, diagnostic services and rehabilitative care.
Government Regulation
The healthcare industry is governed by a framework of federal and state laws, rules and regulations that are extensive and complex and for which, in many cases, the industry has the benefit of only limited judicial and regulatory interpretation. If one of our physicians or physician practices is found to have violated these laws, rules or regulations, our business, financial condition and results of operations could be materially adversely affected. Moreover, the Affordable Care Act signed into law in March 2010 contains numerous provisions that are reshaping the United States healthcare delivery system, and healthcare reform continues to attract significant legislative interest, regulatory activity, new approaches, legal challenges and public attention that create uncertainty and the potential for additional changes. Healthcare reform implementation, additional legislation or regulations, and other changes in government policy or regulation may affect our reimbursement, restrict our existing operations, limit the expansion of our business or impose additional compliance requirements and costs, any of which could have a material adverse effect on our business, financial condition, results of operations, cash flows and the trading price of our common stock. See Item 1A. Risk Factors —“General Risks Relating to Our Business—The healthcare regulatory and political framework is uncertain and evolving.”
Fraud and Abuse Provisions
Existing federal laws governing Medicare, TRICARE and other federal healthcare programs (the “FHC Programs”), as well as similar state laws, impose a variety of fraud and abuse prohibitions on healthcare companies like us. These laws are interpreted broadly and enforced aggressively by multiple government agencies, including the Office of Inspector General of the Department of Health and Human Services, the Department of Justice (the “DOJ”) and various state authorities.
The fraud and abuse laws include extensive federal and state regulations applicable to our financial relationships with hospitals, referring physicians and other healthcare entities. In particular, the federal anti-kickback statute prohibits the offer, payment, solicitation or receipt of any remuneration in return for either referring Medicare, TRICARE or other FHC Program business, or purchasing, leasing, ordering or arranging for or recommending any service or item for which payment may be made by an FHC Program. In addition, federal physician self-referral legislation, commonly known as the “Stark Law,” prohibits a physician from ordering certain designated health services reimbursable by Medicare from an entity with which the physician has a prohibited financial relationship. These laws are broadly worded and, in the case of the anti-kickback statute, have been broadly interpreted by federal courts, and potentially subject many healthcare business arrangements to government investigation and prosecution, which can be costly and time consuming. See Item 1A.Risk Factors —“General Risks Relating to Our Business—Stark Law prohibition on physician referrals may be interpreted so as to limit our prospects.”
Violations of these laws are punishable by substantial penalties, including monetary fines, civil penalties, administrative remedies, criminal sanctions (in the case of the anti-kickback statute), exclusion from participation in FHC Programs and forfeiture of amounts collected in violation of such laws, any of which could have an adverse effect on our business and results of operations. Many of the states in which we operate also have anti-kickback and self-referral laws which are applicable to our government and non-government business and which also authorize substantial penalties for violations.
There are a variety of other types of federal and state fraud and abuse laws, including laws authorizing the imposition of criminal, civil and administrative penalties for filing false or fraudulent claims for reimbursement with government healthcare programs. These laws include the civil False Claims Act (“FCA”), which prohibits the submitting of or causing to be submitted false claims to the federal government or federal government programs, including Medicare, the TRICARE program for military dependents and retirees, and the Federal Employees Health Benefits Program. Substantial civil fines and multiple damages, along with other remedies, can be imposed for violating the FCA. Furthermore, proving a violation of the FCA requires only that the government show that the individual or company that submitted or caused to be submitted an allegedly false claim acted in “reckless disregard” of the truth or falsity of the claim, notwithstanding that there may have been no intent to defraud the government program and no actual knowledge that the claim was false (which typically are required to be shown to sustain a criminal conviction). The FCA also applies to the improper retention of known overpayments and includes “whistleblower” provisions that permit private citizens to sue a claimant on behalf of the government and thereby share in the amounts recovered under the law and to receive additional remedies. In recent years, many cases have been brought against healthcare companies by such “whistleblowers,” which have resulted in judgments or, more often, settlements involving substantial payments to the government by the companies involved. It is anticipated that the number of such actions against healthcare companies will continue to increase with the enactment of a growing number of state false claims acts and certain amendments to the FCA recently enacted by Congress and enhanced government enforcement.
In addition, federal and state agencies that administer healthcare programs have at their disposal statutes, commonly known as “civil money penalty laws,” that authorize substantial administrative fines and exclusion from government programs in cases where an individual or company that filed a false claim, or caused a false claim to be filed, knew or should have known that the claim was false or fraudulent. As under the FCA, it often is not necessary for the agency to show that the claimant had actual knowledge that the claim was false or fraudulent in order to impose these penalties.
The civil and administrative false claims statutes are being applied in an increasingly broader range of circumstances. For example, government authorities have asserted that claiming reimbursement for services that fail to meet applicable quality standards may, under certain circumstances, violate these statutes. Government authorities also often take the position, now with support from recent amendments to the FCA, that claims for services that were induced by kickbacks, Stark Law violations or other illicit marketing schemes are fraudulent and, therefore, violate the false claims statutes. Many of the laws and regulations referenced above can be used in conjunction with each other.
If we were excluded from any government-sponsored healthcare programs, not only would we be prohibited from submitting claims for reimbursement under such programs, but we also would be unable to contract with other healthcare providers, such as hospitals, to provide services to them. It could also adversely affect our ability to contract with, or to obtain payment from, non-governmental payors.
Although we diligently conduct our business in compliance with all applicable federal and state fraud and abuse laws, many of the laws and regulations applicable to us, including those relating to billing and those relating to relationships with referring physicians and hospitals, are broadly worded and may be interpreted or applied by prosecutorial, regulatory or judicial authorities in ways that we cannot predict. Accordingly, we cannot assure you that our arrangements or business practices will not be subject to government scrutiny or be alleged or found to violate applicable fraud and abuse laws. Moreover, the standards of business conduct expected of healthcare companies under these laws and regulations have become more stringent in recent years, even in instances where there has been no change in statutory or regulatory language. If there is a determination by government authorities that we have not complied with any of these laws and regulations, our business, financial condition and results of operations could be materially adversely affected. See “Government Investigations.”
Government Reimbursement Requirements
In order to participate in the Medicare program, we must comply with stringent and often complex enrollment and reimbursement requirements. While our compliance program requires that we adhere to the laws and regulations applicable to the government programs in which we participate, our failure to comply with these laws and regulations could negatively affect our business, financial condition and results of operations. See “Government Regulation—Fraud and Abuse Provisions,” “Government Regulation—Compliance Program,” “Government Investigations” and “Other Legal Proceedings,” and Item 1A. Risk Factors—“General Risks Relating to Our Business—The healthcare industry is highly regulated, and government authorities may determine that we have failed to comply with applicable laws or regulation;” “Federal and state laws that protect the privacy and security of protected health information may increase our costs and limit our ability to collect and use that information and subject us to penalties if we are unable to fully comply with such laws;” and “Changes in the rates or methods of third-party reimbursements for medical services could result in reduced demand for our services or create downward pricing pressure, which would result in a decline in our revenues and harm to our financial position.”
In addition, Medicare, TRICARE and other government healthcare programs are subject to statutory and regulatory changes, administrative rulings, interpretations and determinations, requirements for utilization review and new governmental funding restrictions, all of which may materially increase or decrease program payments as well as affect the cost of providing services and the timing of payments to providers. Moreover, because these programs generally provide for reimbursement on a fee-schedule basis rather than on a charge-related basis, we generally cannot increase our revenue by increasing the amount we charge for our services. To the extent our costs increase, we may not be able to recover our increased costs from these programs, and cost containment measures and market changes in non-governmental insurance plans have generally restricted our ability to recover, or shift to non-governmental payors, these increased costs. In attempts to limit federal and state spending, there have been, and we expect that there will continue to be, a number of proposals to limit or reduce Medicare reimbursement for various services. Our business may be significantly and adversely affected by any such changes in reimbursement policies and other legislative initiatives aimed at reducing healthcare costs associated with Medicare, TRICARE and other government healthcare programs.
Our business also could be adversely affected by reductions in or limitations of reimbursement amounts or rates under these government programs, reductions in funding of these programs or elimination of coverage for certain individuals or treatments under these programs.
Antitrust
The healthcare industry is subject to close antitrust scrutiny. In recent years, the Federal Trade Commission (the “FTC”), the Department of Justice (“DOJ”) and state Attorney General have increasingly taken steps to review and, in some cases, taken enforcement action against business conduct and acquisitions in the healthcare industry. Violations of antitrust laws may be punishable by substantial penalties, including significant monetary fines, civil penalties, criminal sanctions, consent decrees and injunctions prohibiting certain activities or requiring divestiture or discontinuance of business operations. Any of these penalties could have a material adverse effect on our business, financial condition and results of operations. We consider the antitrust laws in connection with the acquisition of physician practices and the operation of our business, and we believe our operations are in compliance with applicable laws.
HIPAA and Other Privacy Laws
Numerous federal and state laws, rules and regulations govern the collection, dissemination, use and confidentiality of protected health information, including the federal Health Insurance Portability and Accountability Act of 1996, as amended (“HIPAA”), and its implementing regulations, violations of which are punishable by monetary fines, civil penalties and, in some cases, criminal sanctions. As part of our medical record keeping, third-party billing, research and other services, we and our affiliated practices collect and maintain protected health information on the patients that we serve.
Pursuant to HIPAA, the U.S. Department of Health and Human Services (“HHS”) has adopted standards to protect the privacy and security of individually identifiable health information, known as the Privacy Standards and Security Standards. HHS’s Privacy Standards apply to medical records and other individually identifiable health information in any form, whether electronic, paper or oral, that is used or disclosed by healthcare providers, hospitals, health plans and healthcare clearinghouses, which are known as “Covered Entities.” We have implemented privacy policies and procedures, including training programs, designed to be compliant with the HIPAA Privacy Standards.
HHS’s Security Standards require healthcare providers to implement administrative, physical and technical safeguards to protect the integrity, confidentiality and availability of individually identifiable health information that is electronically received, maintained or transmitted (including between us and our affiliated practices). We have implemented security policies, procedures and systems designed to facilitate compliance with the HIPAA Security Standards.
In February 2009, Congress enacted the Health Information Technology for Economic and Clinical Health Act (“HITECH”) as part of the American Recovery and Reinvestment Act (“ARRA”). Among other changes to the law governing protected health information, HITECH strengthens and expands HIPAA, increases penalties for violations, gives patients new rights to restrict uses and disclosures of their health information, and imposes a number of privacy and security requirements directly on our “Business Associates,” which are third-parties that perform functions or services for us or on our behalf. Specifically, HITECH requires that Covered Entities and Business Associates alike report any unauthorized use or disclosure of individually identifiable health information that meets the definition of a breach, to the affected individuals, HHS and, depending on the number of affected individuals, the media for the affected market. HITECH also authorizes state Attorneys General to bring civil actions in response to violations of HIPAA that threaten the privacy of state residents. As a result, we have made revisions to our privacy policies and procedures so that we are compliant with HITECH requirements.
In addition to the federal HIPAA and HITECH requirements, numerous other state and certain other federal laws protect the confidentiality of patient information, including state medical privacy laws, state social security number protection laws, human subjects research laws and federal and state consumer protection laws. In some cases, state laws are more stringent than HIPAA and therefore, are not preempted by HIPAA.
Environmental Regulations
Our healthcare operations generate medical waste that must be disposed of in compliance with federal, state and local environmental laws, rules and regulations. Our office-based operations are subject to compliance with various other environmental laws, rules and regulations. Such compliance does not, and we anticipate that such compliance will not, materially affect our capital expenditures, financial position or results of operations.
Compliance Program
We maintain a compliance program that reflects our commitment to complying with all laws, rules and regulations applicable to our business and that meets our ethical obligations in conducting our business (the “Compliance Program”). We believe our Compliance Program provides a solid framework to meet this commitment and our obligations as a provider of health care services, including:
| • | a Compliance Committee consisting of our senior executives; |
| • | ourCode of Ethics, which is applicable to our employees, officers and directors; |
| • | a disclosure program that includes a mechanism to enable individuals to disclose on a confidential or anonymous basis to our Chief Executive Officer, or any person who is not in the disclosing individual’s chain of command, issues or questions believed by the individual to be a potential violation of criminal, civil, or administrative laws; |
| • | an organizational structure designed to integrate our compliance objectives into our corporate offices and centers of medical excellence; and |
| • | education, monitoring and corrective action programs, including a disclosure policy designed to establish methods to promote the understanding of our Compliance Program and adherence to its requirements. |
The foundation of our Compliance Program is ourCode of Ethics which is intended to be a comprehensive statement of the ethical and legal standards governing the daily activities of our employees, affiliated professionals, independent contractors, officers and directors. All our personnel are required to abide by, and are given thorough education regarding, ourCode of Ethics. In addition, all employees are expected to report incidents that they believe in good faith may be in violation of ourCode of Ethics.
Government Investigations
We expect that audits, inquiries and investigations from government authorities, agencies, contractors and payors will occur in the ordinary course of business. Such audits, inquiries and investigations and their ultimate resolutions, individually or in the aggregate, could have a material adverse effect on our business, financial condition, results of operations, cash flows and the trading price of our common stock. To the best of our knowledge, as of this time, our health care business is not the subject of any pending audit, inquiry or investigation by any governmental authority.
Other Legal Proceedings
In the ordinary course of our business, we may become involved in pending and threatened legal actions and proceedings, most of which might involve claims of medical malpractice related to medical services provided by our physicians. Our contracts with hospitals generally require us to indemnify them and their affiliates for losses resulting from the negligence of our physicians. We may also become subject to other lawsuits that could involve large claims and significant defense costs. We believe, based upon a review of pending actions and proceedings, that the outcome of such legal actions and proceedings will not have a material adverse effect on our business, financial condition or results of operations. The outcome of such actions and proceedings, however, cannot be predicted with certainty and an unfavorable resolution of one or more of them could have a material adverse effect on our business, financial condition, results of operations, cash flows and the trading price of our common stock.
Although we currently maintain liability insurance coverage intended to cover professional liability and certain other claims, we cannot assure that our insurance coverage will be adequate to cover liabilities arising out of claims asserted against us in the future where the outcomes of such claims are unfavorable to us. Liabilities in excess of our insurance coverage, including coverage for professional liability and certain other claims, could have a material adverse effect on our business, financial condition and results of operations. See “Professional and General Liability Coverage.”
Professional and General Liability Coverage
We maintain professional and general liability insurance policies with third-party insurers on a claims-made basis, subject to deductibles, self-insured retention limits, policy aggregates, exclusions, and other restrictions, in accordance with standard industry practice. We believe that our insurance coverage is appropriate based upon our claims experience and the nature and risks of our business. However, we cannot assure that any pending or future claim will not be successful or if successful will not exceed the limits of available insurance coverage.
FCID Medical, Inc.
FCID Medical, Inc. (FCID) is our wholly-owned subsidiary under which our present center of excellence is owned and operated and future centers of excellence will be owned and operated. FCID managed First Choice Medical Group of Brevard, LLC from November 2011 until we acquired the Company in April 2012. Since acquiring the practice, we have succeeded in increasing monthly patient visits, improving management of account payables/receivables, and expanding the number of physicians and care specialists on staff.
Based in Melbourne, Florida, FCMG is our flagship multi-specialty medical center of excellence that specializes in the delivery of musculoskeletal medicine, diagnostic services and rehabilitative care with multiple quality-focused goals centered on enriching its patients’ care experience. Our physicians and care specialists are recruited and retained with an emphasis on best practices and attitude: that being committed to meeting and exceeding the needs of patients and their families. We currently employ eight best in class physicians who represent what FCHS believes rank as the best clinicians in their respective medical disciplines in Brevard County, Florida. Moreover, all employees of FCMG, from the receptionists to the doctors, are considered caregivers whoput the patient first. All caregivers cooperate with one another through a common focus on the best interests and personal goals of each patient. Moreover, families and friends of each patient are considered vital components of the care team.
Care is focused on each patient’s full continuum of care, which requires a more ‘personalized’ approach to treatment. Care is customized to ensure that each patient’s needs, values and choices are always considered, which squarely aligns with FCHS’s slogan of “transforming healthcare delivery, one patient at a time.”
Diagram 2. First Choice Medical Group’s Patient-Centric Care Delivery Model

We strive every day to ensure that our patients are never kept waiting to see our physicians. Based upon FCMG’s patient exit polling results collected in 2013, our patient wait time has remained consistently below the industry average of approximately 23 minutes (source: Vitals.com).
Care providers listen to and honor patients and family perspectives and choices. Moreover, our caregivers intend to continue to communicate and share complete and unbiased information with patients and families in ways that are affirming and useful in decision-making processes. Our care delivery practices exemplify the very definition of patient-centric care, explicitly recognizing the importance of human interaction in terms of personalized care, kindness and being ‘present’ with patients.
FCMG’s patient-centric culture strives to include providing an inviting, easily accessible, peaceful, healing environment that is aesthetically pleasing and designed specifically to allay patient fear, anxiety and discomfort. The design and décor of FCMG’s lobby and diagnostic and treatment areas are intended to define and reinforce a strong and relevant brand image of quality, patient-centered care. Capitalizing on sweeping views of the Indian River, FCMG’s spa-like decor provides a seamless connection to nature and promotes a palpable sense of good health and wellness.
FCMG also engages the most advanced diagnostic technologies coupled with the latest in individualized care, including trigger point injections and pharmacological, physical, neurological, orthopedic, chiropractic and massage therapy treatments. Our care facilities house both a digital GE X-Ray system and a GE 450 MRI Gem Suite system, which is physically positioned to capitalize on the expansive waterfront view of the Indian River, promoting patient relaxation and soothing fear and anxiety.
Our physicians currently have hospital and surgical privileges at several hospitals serving Brevard County, Florida, and include:
| · | Health First, Inc. – an integrated healthcare delivery system comprising: |
| o | Holmes Regional Medical Center; |
| o | Cape Canaveral Hospital; |
| · | Melbourne Same-Day Surgery Center; |
| · | Merritt Island Surgery Center; |
| · | Crane Creek Surgery Center; and |
| · | Wuestoff Medical Centers in Rockledge and Melbourne. |
Geographic Service Region
Currently, 100% of our revenues are generated from our business interests operating in Melbourne, located in Brevard County, Florida along the coast of the Atlantic Ocean. As of the 2010 Census, the population of Brevard was 543,376, making it the ninth most populous county in the state. Influenced by the presence of the John F. Kennedy Space Center, Brevard County is also known as the “Space Coast.” Military installations in Brevard County include Patrick Air Force Base, Cape Canaveral Air Force Station and the U.S. Air Force Malabar Test Facility. In addition, the U.S. Navy maintains a Trident turning basin at Port Canaveral for ballistic missile submarines.
Real Estate
Marina Towers, LLC
Marina Towers, LLC is our subsidiary which owns and operates Marina Towers, a Class A 78,000 square foot, six-story building located on the Indian River in Melbourne, Florida. The address is 709 South Harbor City Boulevard, Melbourne, Florida 32901. In addition to housing our corporate headquarters and First Choice Medical Group, the building, which averages 95% annual occupancy, also leases commercial office space to tenants that include UBS Financial, Support Systems and Modus Operandi.
Our wholly owned subsidiary FCID Holdings, Inc. holds a 99% ownership stake in Marina Towers, LLC; and our wholly owned subsidiary MTMC of Melbourne, Inc. holds the remaining 1% ownership.
Our Headquarters
Our corporate headquarters is located on the shore of the Indian River at 709 S. Harbor City Boulevard, Suite 250, Melbourne, Florida 32901 in Marina Towers, which is owned by Marina Towers, LLC, a subsidiary owned by FCID Holdings, Inc. and MTMC of Melbourne, Inc., both wholly owned subsidiaries of the Company.
Employees
As of December 31, 2013, we employed approximately 40 employees, which included eight physicians and two physician assistants.
Merger, Re-Incorporation and Name Change
We were incorporated in the State of Colorado on May 30, 2007 to act as a holding corporation for I.V. Services Ltd., Inc. (“IVS”), a Florida corporation engaged in providing billing services to providers of medical services. IVS was incorporated in the State of Florida on September 28, 1987, and on June 30, 2007, 2,429,000 common shares were issued to Mr. Michael West and other IVS shareholders in exchange for 100% of the capital stock of IVS. In the second quarter of 2011, we disposed of IVS, which, at the time, was an inactive, wholly-owned subsidiary of the Company. The consideration for the disposition was the net liability assumption by the purchaser.
On December 29, 2010, we entered into a Share Exchange Agreement (the “Share Exchange Agreement”) with FCID Medical, Inc., a Florida corporation (“FCID Medical”) and FCID Holdings, Inc., a Florida corporation (“FCID Holdings)”, which together will be referred to herein with FCID Medical as “FCID”, and the shareholders of FCID (the “FCID Shareholders”). Pursuant to the terms of the Share Exchange Agreement, the FCID Shareholders exchanged 100% of the outstanding common stock of FCID for a total of 10,000,000 common shares of the Company, resulting in FCID Medical and FCID Holdings being 100% owned subsidiaries of the Company (the “Share Exchange”).
On or about February 13, 2012, we obtained stockholder consent for (i) the approval of an agreement and plan of merger (the “Merger Agreement”) with First Choice Healthcare Solutions, Inc., (“FCHS Delaware”), a Delaware corporation formed exclusively for the purpose of merging with the Company, pursuant to which (a) the Company’s state of incorporation changed from Colorado to Delaware (the “Reincorporation”) (b) the Company’s name changed from Medical Billing Assistance, Inc. to First Choice Healthcare Solutions, Inc. (the “Name Change”), (c) every four shares of Company’s common stock was exchanged for one share of FCHS Delaware common stock (effectively resulting in a four-to-one reverse split of the Company’s common stock) (the “Reverse Split”), and (d) FCHS Delaware inherited the rights and property of the Company and assumed the liabilities of the Company and (ii) the approval of the Medical Billing Assistance, Inc. 2011 Incentive Stock Plan. The effective date for the Reincorporation and the Reverse Split was April 4, 2012. The Company changed its name to be more closely aligned with its target market.
Our address is 709 S. Harbor City Blvd., Suite 250, Melbourne, Florida, 32901 and our phone number is (321) 725-0090. Our website address is www.myfchs.com. Information contained in our website is not incorporated by reference herein.
Where You Can Find Additional Information
The Company is subject to the reporting requirements under the Exchange Act. The Company files with, or furnishes to, the SEC quarterly reports on Form 10-Q, current reports on Form 8-K, and amendments to those reports and will furnish its proxy statement. These filings are available free of charge on the Company’s website, www.myfchs.com, shortly after they are filed with, or furnished to, the SEC. The SEC maintains an Internet website,www.sec.gov, which contains reports and information statements and other information regarding issuers.
ITEM 1A. RISK FACTORS
The risk factors discussed below could cause our actual results to differ materially from those expressed in any forward-looking statements. Although we have attempted to list comprehensively these important factors, we caution you that other factors may in the future prove to be important in affecting our results of operations. New factors emerge from time to time and it is not possible for us to predict all of these factors, nor can we assess the impact of each such factor on the business or the extent to which any factor, or combination of factors, may cause actual results to differ materially from those contained in any forward-looking statement.
The risks described below set forth what we believe to be the most material risks associated with the purchase of our common stock. Before you invest in our common stock, you should carefully consider these risk factors, as well as the other information contained in this prospectus.
General Risks Regarding Our Business
We have a limited operating history that impedes our ability to evaluate our potential future performance and strategy.
Our Company implemented its unique business model in 2012 and we continue to enhance the strategy of the business plan. Our limited operating history in our present format makes it difficult for us to evaluate our future business prospects and make decisions based on estimates of our future performance. To address these risks and uncertainties, we must do the following:
| · | Successfully execute our business strategy; |
| · | Respond to competitive developments; |
| · | Effectively and efficiently integrate new acquisitions; and |
| · | Attract, integrate, retain and motivate qualified personnel. |
We cannot be certain that our business strategy will be successful or that we will successfully address these risks. In the event that we do not successfully address these risks, our business, prospects, financial condition and results of operations may be materially and adversely affected.
We are implementing a strategy to grow our business, which is expensive and may not generate income.
We intend to grow our business, and we plan to incur expenses associated with our growth and expansion. Although we are taking steps to raise funds through equity offerings to implement our growth strategy, these funds may not be adequate to offset all of the expenses we incur in expanding our business. We will need to generate revenues to offset expenses associated with our growth, and we may be unsuccessful in achieving sufficient revenues, despite our attempts to grow our business. If our growth strategies do not result in sufficient revenues and income, we may have to abandon our plans for further growth and/or cease operations, which could have a material and adverse effect on our business, prospects and financial condition.
We may need to raise additional capital. If we are unable to raise additional capital, our business may fail.
If we require additional capital, we may need to borrow money or sell more securities. Under these circumstances, we may be unable to secure additional financing on favorable terms or at all.
Selling additional stock, either privately or publicly, would dilute the equity interests of our stockholders. If we borrow money, we will have to pay interest and may also have to agree to restrictions that limit our operating flexibility. If we are unable to obtain required capital for operations or growth, we may have to curtail business operations which would have a material negative effect on operating results and most likely result in a lower stock price.
Adverse changes in general domestic and worldwide economic conditions and instability and disruption of credit markets could adversely affect our operating results, financial condition, or liquidity.
We are subject to risks arising from adverse changes in general domestic and global economic conditions, including recession or economic slowdown and disruption of credit markets. Recent global market and economic conditions have been unprecedented and challenging with tighter credit conditions and recession in most major economies. Continued concerns about the systemic impact of potential long-term and wide-spread recession, inflation, energy costs, geopolitical issues, the availability and cost of credit, the United States mortgage market and a declining real estate market in the United States have contributed to increased market volatility and diminished expectations for the United States economy. Added concerns fueled by the United States government financial assistance to certain companies and other federal government’s interventions in the United States financial system has led to increased market uncertainty and instability in both United States and international capital and credit markets. These conditions, combined with volatile oil prices, declining business and consumer confidence, increased unemployment, increased tax rates and governmental budget deficits and debt levels have contributed to volatility of unprecedented levels. We believe our healthcare clinics may be impacted by unemployment rates, the number of under-insured or uninsured patients and other conditions arising from the global economic conditions described above. At this time, it is unclear what impact this might have on our future revenues or business.
As a result of these market conditions, the cost and availability of credit has been and may continue to be adversely affected by illiquid credit markets and wider credit spreads. Concern about the stability of the markets generally and the strength of counterparties specifically has led many lenders and institutional investors to reduce, and in some cases, cease to provide funding to borrowers.
Continued turbulence in the United States and international markets and economies may adversely affect our liquidity and financial condition, and the liquidity and financial condition of our patients. If these market conditions continue, they may limit our ability, and the ability of our patients, to timely replace maturing liabilities, and access the capital markets to meet liquidity needs, resulting in material and adverse effects on our business, prospects, financial condition and results of operations.
While the majority of the cost of medical care is typically reimbursed by third-party payers such as commercial healthcare insurance companies or government programs, including Medicare and TRICARE, the consumer pays a portion of health care costs and we are affected by changes in the consumer’s disposal revenue.
After payments by commercial healthcare insurance companies or government programs, including Medicare and TRICARE, the remaining portion of the cost of medical care is paid by the patient. Accordingly, our operating results may vary based upon the impact of changes in the disposable income of consumers interested in healthcare, among other economic factors. A significant decrease in consumer disposable income in a weak economy may result in a decrease in the number of medical procedures performed and a decline in our revenues and profitability. In addition, weak economic conditions may cause some of our patients to experience financial distress or declare bankruptcy, which may negatively impact our accounts receivable collection experience.
Since a significant percentage of our operating expenses are fixed, a relatively small decrease in revenues could have a significant negative impact on our financial results.
A significant percentage of our expenses will be fixed - meaning they do not vary significantly with the increase or decrease in revenues. Such expenses include, but will not be limited to, debt service and capital lease payments, rent and operating lease payments, salaries, maintenance and insurance. As a result, a small reduction in the prices we charge for our services or procedure volume could have a disproportionately negative effect on our financial results.
Loss of key executives, limited experience in operating a public company and failure to attract qualified managers and sales persons could limit our growth and negatively impact our operations.
We depend upon our management team to a substantial extent. In particular, we depend upon Christian Charles Romandetti, our President and Chief Executive Officer for his skills, experience and knowledge of our Company and industry contacts. The loss of Mr. Romandetti or other members of our management team could have a material adverse effect on our business, results of operations or financial condition.
Our limited experience in dealing with the increasingly complex laws pertaining to public companies could be a significant disadvantage to us in that it is likely that an increasing amount of management’s time will be devoted to these activities which will result in less time being devoted to the management and growth of our company. It is possible that we will be required to expand our employee base and hire additional employees to support our operations as a public company which will increase our operating costs in future periods.
We require medical clinic managers, medical professionals and marketing persons with experience in our industry to operate and market our medical clinic services. It is impossible to predict the availability of qualified persons or the compensation levels that will be required to hire them. The loss of the services of any member of our senior management or our inability to hire qualified persons at economically reasonable compensation levels could adversely affect our ability to operate and grow our business.
We may have difficulties managing growth which could lead to higher losses.
Rapid growth could strain our human and capital resources, potentially leading to higher operating losses. Our ability to manage operations and control growth will be dependent upon our ability to raise and spend capital to successfully attract, train, motivate, retain and manage new employees and continue to update and improve our management and operational systems, infrastructure and other resources, financial and management controls, and reporting systems and procedures. Should we be unsuccessful in accomplishing any of these essential aspects of our growth in an efficient and timely manner, then management may receive inadequate information necessary to manage our operations, possibly causing additional expenditures and inefficient use of existing human and capital resources or we otherwise may be forced to grow at a slower pace that could slow or eliminate our ability to achieve and sustain profitability. Such slower than expected growth may require us to restrict or cease our operations and go out of business.
We may not receive payment from some of our healthcare patients because of their financial circumstances.
Some of our healthcare provider patients may not have significant financial resources, liquidity or access to capital. If these patients experience financial difficulties they may be unable to pay for the healthcare services that we will provide. A significant deterioration in general or local economic conditions could have a material adverse effect on the financial health of our healthcare provider patients. As a result, this may adversely affect our financial condition and results of operations.
We may be subject to medical professional liability risks, which could be costly and could negatively impact our business and financial results.
We may be subject to professional liability claims. Although there currently are no known hazards associated with any of our procedures or technologies when performed or used properly, hazards may be discovered in the future. For example: there is a risk of harm to a patient during an MRI if the patient has certain types of metal implants or cardiac pacemakers within his or her body. Although patients are screened to safeguard against this risk, screening may nevertheless fail to identify the hazard. There also is potential risk to patients treated with therapy equipment secondary to inadvertent or excessive over- or under- exposure to radiation — a topic on which the U.S. House of Representatives Committee on Energy and Commerce Subcommittee on Health held a hearing on February 26, 2010. We maintain professional liability insurance with coverage that we believe is consistent with industry practice and appropriate in light of the risks attendant to our business. However, any claim made against us could be costly to defend against, resulting in a substantial damage award against us and divert the attention of our management team from our operations, which could have an adverse effect on our financial performance.
We may not be able to achieve the expected benefits from future acquisitions, which would adversely affect our financial condition and results.
We plan to rely on acquisitions as a method of expanding our business. If we do not successfully integrate acquisitions, we may not realize anticipated operating advantages and cost savings. The integration of companies that have previously operated separately involves a number of risks, including:
| · | Demands on management related to the increase in our size after an acquisition; |
| · | The diversion of management’s attention from the management of daily operations to the integration of operations; |
| · | Difficulties in the assimilation and retention of employees; |
| · | Potential adverse effects on operating results; and |
| · | Challenges in retaining patients. |
We may not be able to maintain the levels of operating efficiency acquired companies have achieved or might achieve separately. Successful integration of each of their operations will depend upon our ability to manage those operations and to eliminate redundant and excess costs. Difficulties in combining operations may not be able to achieve the cost savings and other size-related benefits that we hoped to achieve from these acquisitions, which would harm our financial condition and operating results.
The healthcare regulatory and political framework is uncertain and evolving.
Healthcare laws and regulations may change significantly in the future which could adversely affect our financial condition and results of operations. We continuously monitor these developments and modify our operations from time to time as the legislative and regulatory environment changes.
In March 2010, President Barack Obama signed one of the most significant health care reform measures in decades providing healthcare insurance for approximately 30 million more Americans. The Patient Protection and Affordable Care Act, as amended by the Health Care and Education Affordability Reconciliation Act (collectively, the “PPACA”), substantially changes the way health care is financed by both governmental and private insurers, including several payment reforms that establish payments to hospitals and physicians based in part on quality measures, and may significantly impact our industry. The PPACA requires, among other things, payment rates for services using imaging equipment that costs over $1 million to be calculated using revised equipment usage assumptions and reduced payment rates for imaging services paid under the Medicare Part B fee schedule. We are unable to predict what effect the PPACA or other healthcare reform measures that may be adopted in the future will have on our business.
The healthcare industry is highly regulated, and government authorities may determine that we have failed to comply with applicable laws or regulations.
The healthcare industry and physicians’ medical practices, including the healthcare and other services that we and our affiliated physicians provide, are subject to extensive and complex federal, state and local laws and regulations, compliance with which imposes substantial costs on us. Of particular importance are the provisions summarized as follows:
| · | federal laws (including the federal False Claims Act) that prohibit entities and individuals from knowingly or recklessly making claims to Medicare and other government programs that contain false or fraudulent information or from improperly retaining known overpayments; |
| · | a provision of the Social Security Act, commonly referred to as the “anti-kickback” law, that prohibits the knowing and willful offer, payment, solicitation or receipt of any bribe, kickback, rebate or other remuneration, in cash or in kind, in return for the referral or recommendation of patients for items and services covered, in whole or in part, by federal healthcare programs, such as Medicare; |
| · | a provision of the Social Security Act, commonly referred to as the Stark Law, that, subject to limited exceptions, prohibits physicians from referring Medicare patients to an entity for the provision of certain “designated health services” if the physician or a member of such physician’s immediate family has a direct or indirect financial relationship (including a compensation arrangement) with the entity; |
| · | similar state law provisions pertaining to anti-kickback, fee splitting, self-referral and false claims issues, which typically are not limited to relationships involving federal payors; |
| · | provisions of HIPAA that prohibit knowingly and willfully executing a scheme or artifice to defraud a healthcare benefit program or falsifying, concealing or covering up a material fact or making any material false, fictitious or fraudulent statement in connection with the delivery of or payment for healthcare benefits, items or services; |
| · | state laws that prohibit general business corporations from practicing medicine, controlling physicians’ medical decisions or engaging in certain practices, such as splitting fees with physicians; |
| · | federal and state laws that prohibit providers from billing and receiving payment from Medicare and TRICARE for services unless the services are medically necessary, adequately and accurately documented and billed using codes that accurately reflect the type and level of services rendered; |
| · | federal and state laws pertaining to the provision of services by non-physician practitioners, such as advanced nurse practitioners, physician assistants and other clinical professionals, physician supervision of such services and reimbursement requirements that may be dependent on the manner in which the services are provided and documented; and |
| · | federal laws that impose civil administrative sanctions for, among other violations, inappropriate billing of services to federally funded healthcare programs, inappropriately reducing hospital care lengths of stay for such patients, or employing individuals who are excluded from participation in federally funded healthcare programs. |
In addition, we believe that our business will continue to be subject to increasing regulation, the scope and effect of which we cannot predict. See Item 1. Business—“Government Regulation.”
We may in the future become the subject of regulatory or other investigations or proceedings, and our interpretations of applicable laws, rules and regulations may be challenged.
Regulatory authorities or other parties may assert that our arrangements with our affiliated professional contractors constitute fee splitting or the corporate practice of medicine and seek to invalidate these arrangements, which could have a material adverse effect on our business, financial condition, results of operations, cash flows and the trading price of our common stock. See Item 1. Business—“Government Regulation—Fee Splitting; Corporate Practice of Medicine.” Regulatory authorities or other parties also could assert that our relationships, including fee arrangements, among our affiliated professional contractors, hospital clients or referring physicians violate the anti-kickback, fee splitting or self-referral laws and regulations or that we have submitted false claims or otherwise failed to comply with government program reimbursement requirements. See Item 1. Business—“Government Regulation—Fraud and Abuse Provisions” and “—Government Reimbursement Requirements.” Such investigations, proceedings and challenges could result in substantial defense costs to us and a diversion of management’s time and attention. In addition, violations of these laws are punishable by monetary fines, civil and criminal penalties, exclusion from participation in government-sponsored healthcare programs, and forfeiture of amounts collected in violation of such laws and regulations, any of which could have a material adverse effect on our business, financial condition, results of operations, cash flows and the trading price of our common stock.
Federal and state laws that protect the privacy and security of protected health information may increase our costs and limit our ability to collect and use that information and subject us to penalties if we are unable to fully comply with such laws.
Numerous federal and state laws and regulations govern the collection, dissemination, use, security and confidentiality of individually identifiable health information. These laws include:
| · | Provisions of HIPAA that limit how healthcare providers may use and disclose individually identifiable health information, provide certain rights to individuals with respect to that information and impose certain security requirements; |
| · | HITECH, which strengthens and expands the HIPAA Privacy Standards and Security Standards; |
| · | Other federal and state laws restricting the use and protecting the privacy and security of protected information, many of which are not preempted by HIPAA; |
| · | Federal and state consumer protection laws; and |
| · | Federal and state laws regulating the conduct of research with human subjects. |
As part of our medical record keeping, third-party billing, research and other services, we collect and maintain protected health information in paper and electronic format. New protected health information standards, whether implemented pursuant to HIPAA, HITECH, congressional action or otherwise, could have a significant effect on the manner in which we handle healthcare-related data and communicate with payors, and compliance with these standards could impose significant costs on us or limit our ability to offer services, thereby negatively impacting the business opportunities available to us.
If we do not comply with existing or new laws and regulations related to protected health information we could be subject to remedies that include monetary fines, civil or administrative penalties or criminal sanctions.
Changes in the rates or methods of third-party reimbursements for medical services could result in reduced demand for our services or create downward pricing pressure, which would result in a decline in our revenues and harm to our financial position.
Third-party payors such as Medicare, TRICARE and commercial health insurance companies, may change the rates or methods of reimbursement for the services we plan to provide and could have a significant negative impact on those revenues. At this time, we cannot predict the impact of rate reductions will have on our future revenues or business. Moreover, patients on whom we will depend for the majority of our medical clinic revenues generally rely on reimbursement from third-party payors. If our patients receive decreased reimbursement, this could result in a reduced demand for our services or downward pricing pressures, which could have a material impact on our financial position.
Future requirements limiting access to or payment for medical services may negatively impact our future revenues or business. If legislation substantially changes the way healthcare is reimbursed by both governmental and commercial insurance carriers, it may negatively impact payment rates for certain medical services. We cannot predict at this time whether or the extent to which other proposed changes will be adopted, if any, or how these or future changes will affect the demand for our services.
Managed care organizations may prevent their members from using our services which would cause us to lose current and prospective patients.
Healthcare providers participating as providers under managed care plans may be required to refer medical services to specific medical clinics depending on the plan in which each covered patient is enrolled. These requirements may inhibit their members from using our medical services in some cases. The proliferation of managed care may prevent an increasing number of their members from using our services in the future which would cause our revenues to decline.
Stark Law prohibition on physician referrals may be interpreted so as to limit our prospects.
The Ethics in Patient Referral Act of 1989, as amended (the "Stark Law"), is a civil statute that generally (i) prohibits physicians from making referrals for designated health services to entities in which the physicians have a direct or indirect financial relationship and (ii) prohibits entities from presenting or causing to be presented claims or bills to any individual, third party payer, or other entity for designated health services furnished pursuant to a prohibited referral. Under the Stark Law, a physician may not refer patients for certain designated health services to entities with which the physician has a direct or indirect financial relationship, unless allowed under an enumerated exception. Under the Stark Law, there are numerous statutory and regulatory exceptions for certain otherwise prohibited financial relationships. A transaction must fall entirely within an exception to be lawful under the Stark Law.
The Stark Law contains significant civil sanctions for violations, including denial of payment, refunds of amounts collected in violation of the Stark Law and exclusion from Medicare programs. In addition, OIG may impose a penalty of $10,000 for submitting an illegal claim or not refunding such a claim on a timely basis and a civil monetary penalty of up to $100,000 for each circumvention arrangement or scheme.
We believe that any referrals between or among the company, the physicians providing services and the facilities where procedures are performed will be for services compliant under the Stark Law. If these arrangements are found to violate the Stark Law, we may be required to restructure such services or be subject to civil or criminal fines and penalties, including the exclusion of our Company, the physicians, and the facilities from the Medicare programs, any of which events could have a material adverse effect on our business, financial condition and results of operations.
Some states have enacted statutes, similar to the federal Anti-Kickback Statute and Stark Law, applicable to our operations because they cover all referrals of patients regardless of the payer or type of healthcare service provided. These state laws vary significantly in their scope and penalties for violations. Although we have endeavored to structure our business operations to be in material compliance with such state laws, authorities in those states could determine that our business practices are in violation of their laws. This could have a material adverse effect on our business, financial condition and results of operations.
Advertising restrictions may be interpreted so as to limit our prospects.
Our healthcare clinic business will be dependent on advertising, which is subject to regulation by the Federal Trade Commission ("FTC"). We believe that we have structured our advertising practices to be in material compliance with FTC regulations and guidance. However, we cannot be certain that the FTC will not determine that our advertising practices are in violation of such laws and guidance.
In addition, the laws of many states restrict certain advertising practices by and on behalf of physicians. Many states do not offer clear guidance on the bounds of acceptable advertising practices or on the limits of advertising provided by management companies on behalf of physicians. Although we have endeavored to structure our advertising practices to be in material compliance with such state laws, authorities in those states could determine that our advertising practices are in violation of those laws.
Fee-splitting prohibitions in some states may be interpreted so as to limit our prospects.
Many states prohibit medical professionals from paying a portion of a professional fee to another individual unless that individual is an employee or partner in the same professional practice. If we violate a state's fee-splitting prohibition, we may be subject to civil or criminal fines, and the physician participating in such arrangements may lose his or her licensing privileges. Many states do not offer clear guidance on what relationships constitute fee-splitting, particularly in the context of providing management services for doctors. We have endeavored to structure our business operations in material compliance with these laws. However, state authorities could find that fee-splitting prohibitions apply to our business practices in their states. If any aspect of our operations were found to violate fee-splitting laws or regulations, this could have a material adverse effect on our business, financial condition, results of operations and cash flows.
Facility licensure requirements in some states may be costly and time-consuming, limiting or delaying our operations.
State Departments of Health may require us to obtain licenses in the various states in which we have our medical multi-specialty centers of excellence or other business operations. We intend to obtain the necessary material licensure in states where licensure is required. However, not all of the regulations governing the need for licensure are clear and there is limited guidance available regarding certain interpretative issues. Therefore, it is possible that a state regulatory authority could determine that we are improperly conducting business operations without a license in that state. This could subject us to significant fines or penalties, result in our being required to cease operations in that state or otherwise have a material adverse effect on our business, financial condition and results of operations. Although we currently have no reason to believe that we will be unable to obtain the necessary licenses without unreasonable expense or delay, there can be no assurance that we will be able to obtain any required licensure.
Health Insurance Portability and Accountability Act compliance is critically import to our continuing operations.
In December 2000, the U.S. Department of Health and Human Services ("DHHS") released final health privacy regulations implementing portions of the Administrative Simplification Provisions of the Health Insurance Portability and Accountability Act of 1996 ("HIPAA"). These final health privacy regulations were effective in April 2003, for providers that engage in certain electronic transactions, including the submission of claims for payment. Additionally, DHHS published final standards to protect the security of health-related information in February 2003. Finally, in August 2009 DHHS published interim final breach notification regulations implementing section 13402 of the Health Information Technology for Economic and Clinical Health ("HITECH") Act. The HIPAA privacy and security regulations and the HITECH Act extensively regulate the use and disclosure of individually identifiable health-related information. Our physicians and the Company are covered entities under HIPAA if those entities provide services that are reimbursable under Medicare or other third-party payers (e.g., orthopedic services). Although the covered health care providers themselves are primarily liable for HIPAA compliance, as a "business associate" to these covered entities we are bound indirectly to comply with the HIPAA privacy regulations, and we are directly bound to comply with certain of the HIPAA security regulations. Although we cannot predict the total financial or other impact of these privacy and security regulations on our business, compliance with these regulations could require us to incur substantial expenses, which could have a material adverse effect on our business, financial condition and results of operations. In addition, we will continue to remain subject to any state laws that are more restrictive than the privacy regulations issued under the Administrative Simplification Provisions.
Our medical business may be reliant upon direct-to-patient marketing.
The effectiveness of our marketing programs and messages to patients can have a significant impact on our financial performance. The effectiveness of marketing may fluctuate, resulting in changes in the cost of marketing per procedure, and variations in our margins. Less effective marketing programs could materially and adversely affect our business, financial condition and results of operations.
If we are unable to attract and retain qualified medical professionals, our ability to maintain operations at existing medical centers, to attract patients or to open new medical multi-specialty centers of excellence could be negatively affected.
We generate our revenues through physicians and medical professionals who work for us to perform medical services and procedures. The retention of those physicians and medical professionals is a critical factor in the success of our medical multi-specialty centers, and the hiring of qualified physicians and medical professionals is a critical factor in our ability to launch new multi-specialty medical centers of excellence successfully. However, at times it may be difficult for us to retain or hire qualified physicians and medical professionals. If we are unable consistently to hire and retain qualified physicians and medical professionals, our ability to open new centers, maintain operations at existing medical multi-specialty centers, and attract patients could be materially and adversely affected.
If technological changes occur rendering our equipment or services obsolete, or increase our cost structure, we may need to make significant capital expenditures or modify our business model, which could cause our revenues or results of operations to decline.
Industry competitive or clinical factors, among others, may require us to introduce alternate medical technology for the services and procedures we offer than those that may currently be in use in our medical multi-specialty centers. Introducing such technology could require significant capital investment or force us to modify our business model in such a way as to make our revenues or results of operations decline. An increase in costs could reduce our ability to maintain our margins. An increase in prices could adversely affect our ability to attract new patients. If we are unable to obtain or maintain state of the art equipment that is essential to the professional medical services provided by our clinics, our business, prospects, results of operations and financial condition could be materially and adversely affected.
We rely significantly on information technology and any failure, inadequacy, interruption or security lapse of that technology, including any cybersecurity incidents, could harm our ability to operate our business effectively.
Our internal computer systems and those of third parties with which we contract may be vulnerable to damage from cyber-attacks, computer viruses, unauthorized access, natural disasters, terrorism, war and telecommunication and electrical failures despite the implementation of security measures. System failures, accidents or security breaches could cause interruptions in our operations, and could result in a material disruption of our business operations, in addition to possibly requiring substantial expenditures of resources to remedy. To the extent that any disruption or security breach were to result in a loss of, or damage to, our data or applications, or inappropriate disclosure of confidential or proprietary information, we could incur liability and our collections from third-party payors could be delayed.
If we are forced to lower our procedure prices in order to compete with a better-financed or lower-cost provider of medical healthcare services, our medical revenues and results of operations could decline.
Our multispecialty medical centers of excellence will compete with medical clinics and other technologies currently under development. Competition comes from other clinics and from hospitals, hospital-affiliated group entities and physician group practices.
Some of our current competitors, or other companies which may choose to enter the industry in the future, may have substantially greater financial, technical, managerial, marketing or other resources and experience than we do and may be able to compete more effectively. Similarly, competition could increase if the market for healthcare services does not experience growth, and existing providers compete for market share. Additional competition may develop, particularly if the price for services or reimbursement decreases. Our management, operations, strategy and marketing plans may not be successful in meeting this competition.
If more competitors offer healthcare services in our geographic markets, we might find it necessary to reduce the prices we charge, particularly if competitors offer the services at lower prices than we do. If that were to happen or we were not successful in cost effectively acquiring patients for our procedures, we may not be able to make up for the reduced gross profit margin by increasing the number of procedures that we perform, and our business, financial condition and results from operations could be adversely affected.
Risks Related To Our Real Estate Assets and Operations.
Our performance and value are subject to risks associated with our real estate assets and with the real estate industry.
Since a significant source of our current revenue is our real estate asset, we are subject to the risk that if our property does not generate revenues sufficient to meet our operating expenses, including debt service and capital expenditures, and the costs associated with our growth, our ability to operate and grow will be materially and adversely affected, which will materially and adversely affect our business, results of operations and financial condition and we may have to reduce or cease operations. The following factors, among others, may adversely affect the revenues generated by our property:
| · | Competition from other office and commercial properties; |
| · | Local real estate market conditions, such as oversupply or reduction in demand for office or other commercial space; |
| · | Costs to comply with new local, state and federal laws; |
| · | Changes in interest rates and availability of financing; |
| · | Vacancies, changes in market rental rates and the need to periodically repair, renovate and re-let space; |
| · | Increased operating costs, including insurance expense, utilities, real estate taxes, state and local taxes and heightened security costs; |
| · | Civil disturbances, hurricanes and other natural disasters, or terrorist acts or acts of war which may result in uninsured or underinsured losses; and |
| · | Declines in the financial condition of our tenants and our ability to collect rents from our tenants. |
We may face risks associated with the use of debt, including refinancing risk.
We are subject to the risks normally associated with debt financing, including the risk that our cash flow will be insufficient to meet required payments of principal and interest. We anticipate that only a small portion of the principal of our debt will be repaid prior to maturity. Therefore, we are likely to need to refinance at least a portion of our outstanding debt as it matures. There is a risk that we may not be able to refinance existing debt or that the terms of any refinancing will not be as favorable as the terms of our existing debt. If principal payments due at maturity cannot be refinanced, extended or repaid with proceeds from other sources, such as new equity capital, our cash flow may not be sufficient to repay all maturing debt when a significant "balloon" payment come due. There is a risk that we may be unable to refinance on favorable terms or at all. This risk is currently heightened because of tightened underwriting standards and increased credit risk premiums. These conditions, which may increase the cost and reduce the availability of debt, may continue or worsen in the future.
The risks associated with the physical effects of weather could have a material adverse effect on our property.
The physical effects of weather could have a material adverse effect on our property, operations and business. For example, our property is located on the riverfront in Brevard County Florida. To the extent weather patterns change, our market could experience increases in storm intensity or rising sea-levels that would make the property less desirable to tenants. Over time, these conditions could result in declining demand for office space in our building or the inability of us to operate the building at all. These conditions may also have indirect effects on our business by increasing the cost of (or making unavailable) property insurance on terms we find acceptable, increasing the cost of energy and increasing the cost of snow removal at our properties. There can be no assurance that weather will not have a material adverse effect on our properties, operations or business.
Risks Related to Our Common Stock.
Because our stock is quoted on the OTCQB, it has a limited public trading market.As a result, it may be difficult or impossible for you to liquidate your investment.
While our common stock currently is quoted on the OTCQB under the trading symbol “FCHS,” the trading volume is limited. We cannot assure that such a market will improve in the future. The OTCQB requires that we be a reporting company under the Securities Exchange Act of 1934. Further, we cannot assure that an investor will be able to liquidate his investment without considerable delay, if at all. If a more active market does develop, the price may be highly volatile. Our limited operating history, lack of profitability, negligible stock liquidity, potential extreme price and volume fluctuations, and regulatory burdens may have a significant impact on the market price of the common stock. It is also possible that the relatively low price of our common stock may keep many brokerage firms from engaging in transactions in our common stock.
Our common stock is subject to the “penny stock” rules of the SEC and the trading market in our securities is limited, which makes transactions in our common stock cumbersome and may reduce the value of an investment in our common stock.
The SEC has adopted Rule 3a51-1 which establishes the definition of a “penny stock,” for the purposes relevant to us, as any equity security that (i) has a market price of less than $5.00 per share or with an exercise price of less than $5.00 per share, or (ii) is not registered on a national securities exchange or listed on an automated quotation system sponsored by a national securities exchange. For any transaction involving a penny stock, unless exempt, Rule 15g-9 of the Exchange Act requires:
| · | that a broker or dealer approve a person’s account for transactions in penny stocks; and |
| · | the broker or dealer receive from the investor a written agreement to the transaction, setting forth the identity and quantity of the penny stock to be purchased. |
In order to approve a person’s account for transactions in penny stocks, the broker or dealer must:
| · | obtain financial information and investment experience objectives of the person; and |
| · | make a reasonable determination that the transactions in penny stocks are suitable for that person and the person has sufficient knowledge and experience in financial matters to be capable of evaluating the risks of transactions in penny stocks. |
The broker or dealer must also deliver, prior to any transaction in a penny stock, a disclosure schedule prescribed by the SEC relating to the penny stock market, which, in highlight form:
| · | sets forth the basis on which the broker or dealer made the suitability determination; and |
| · | attests that the broker or dealer received a signed, written agreement from the investor prior to the transaction. |
Disclosure also has to be made about the risks of investing in penny stocks in both public offerings and in secondary trading, and about the commissions payable to both the broker-dealer and the registered representative. Current quotations for the securities and the rights and remedies and to be available to an investor in cases of fraud in penny stock transactions. Finally, monthly statements have to be sent disclosing recent price information for the penny stock held in the account and information on the limited market in penny stocks. Generally, brokers may be less willing to execute transactions in securities subject to the “penny stock” rules. This may make it more difficult
If we raise additional capital by selling equity or equity-linked securities, the equity interests of our stockholders will be diluted.
Selling additional common stock or equity-linked securities, either privately or publicly, may be necessary to source sufficient capital to fund our operations or growth. Such issuances of securities will dilute the equity interests of our stockholders.
We do not expect to pay dividends in the foreseeable future.
We have not paid dividends on our common stock and do not anticipate paying dividends on our common stock in the foreseeable future. We currently plan to use all funds generated by operations for reinvestment in our operating activities. Investors should not count on dividends in evaluating an investment in our common stock.
Our largest shareholder has significant control over our common stock and may be able to control our Company indefinitely.
Our largest shareholder currently has beneficial ownership of approximately 43.5% of our outstanding common stock. This significant stockholder therefore has considerable influence over the outcome of all matters submitted to our stockholders for approval, including the election of directors and the approval of significant corporate transactions.
If an active, liquid trading market for our common stock does not develop, you may not be able to sell your shares quickly or at or above the price you paid for it.
Although our common stock is quoted on the OTCQB, a consistently active and liquid trading market for our common stock has not yet and may not ever develop or be sustained. You may not be able to sell your shares quickly or at or above the price you paid for our stock if trading in our stock is not active.
We cannot offer any assurance that an active trading market for our common stock will develop on the OTCQB or any stock exchange, should we decide to list our stock on a national securities exchange, or how liquid that market may be. As a result, relatively small trades may have a disproportionate impact on the price of our common stock, which may contribute to the price volatility of our common stock and could limit your ability to sell your shares.
Possible volatility in our stock price could negatively affect us and our stockholders.
The market price of our common stock could also be subject to wide fluctuations in response to many risk factors described in this section and other matters, including:
| · | changes by securities analysts in financial estimates of our operating results and the operating results of our competitors; |
| · | publications of research reports by securities analysts about us, our competitors or our industry; |
| · | fluctuations in the valuation of companies perceived by investors to be comparable to us; |
| · | actual or anticipated fluctuations in our quarterly or annual operating results; |
| · | retention and departures of key personnel; |
| · | our failure or the failure of our competitors to meet analysts' projections or guidance that we or our competitors may give to the market; |
| · | strategic decisions by us or our competitors, such as acquisitions, divestitures, spin-offs, joint ventures, strategic investments or changes in business strategy; |
| · | the passage of legislation or other regulatory developments affecting us or our industry; |
| · | speculation in the press or investment community; and |
| · | natural disasters, terrorist acts, acts of war or periods of widespread civil unrest. |
Furthermore, the stock markets have experienced extreme price and volume fluctuations that have affected and continue to affect the market prices of equity securities of many companies. These fluctuations often have been unrelated or disproportionate to the operating performance of those companies. These broad market and industry fluctuations, as well as general economic, political and market conditions, may negatively affect the market price of our common stock. As a result, the market price of our common stock is likely to be similarly volatile and investors in our common stock may experience a decrease, which could be substantial, in the value of their stock. In the past, many companies that have experienced volatility in the market price of their stock have been subject to securities class action litigation. We may be the target of this type of litigation in the future. Securities litigation against us could result in substantial costs and divert our management's attention from other business concerns, which could have a material adverse effect on our business.
The exercise of existing warrants and conversion of existing convertible debt may have a dilutive impact on our existing stockholders.
In financing our operations, we have issued convertible debt and warrants, including warrants to purchase up to 1,875,000 shares of our Common Stock at an exercise price of $3.60 and warrants to purchase up to 2,320,000 shares of our Common Stock at an exercise price of $1.35 per share. Further, if we choose not to repay a convertible debenture in cash, the holder may convert such debt at $1.00 per share. If these warrants were exercised and convertible debt converted into our Common Stock, it could reduce the percentage ownership of our existing stockholders.
Failure to achieve and maintain internal controls in accordance with Sections 302 and 404 of the Sarbanes-Oxley Act of 2002 could have a material adverse effect on our business and stock price.
If we fail to maintain adequate internal controls or fail to implement required new or improved controls, as we grow or as such control standards are modified, supplemented or amended from time to time; we may not be able to assert that we can conclude on an ongoing basis that we have effective internal controls over financial reporting. Effective internal controls are necessary for us to produce reliable financial reports and are important in the prevention of financial fraud. If we cannot produce reliable financial reports or prevent fraud, our business and operating results could be harmed, investors could lose confidence in our reported financial information, and there could be a material adverse effect on our stock price.
| Item 1B. | Unresolved Staff Comments |
Not applicable.
Our corporate headquarters is located at 709 S. Harbor City Blvd., Suite 250, Melbourne, FL 32901 in Marina Towers, a 78,000 square foot Class A six-story office building, which is owned by Marina Towers, LLC. There is an existing mortgage note payable of $7,550,000 secured by land and the building along with first priority assignment of leases and rents.
The building operates with an average 95% tenant occupancy and a rent roll that is supported by approximately 75% non-affiliate, high quality, commercial tenants. The building generates revenue and income for the Company that is intended to be available to fund the expansion of our operating businesses. Our wholly owned subsidiary FCID Holdings, Inc. holds a 99% ownership stake in Marina Towers, LLC; and our wholly owned subsidiary MTMC of Melbourne, Inc. holds the remaining 1% ownership.
We believe that our present facilities will be suitable for the operation of our business for the foreseeable future and should we need to expand, we expect that suitable additional space will be available on commercially reasonable terms, although no assurance can be made in this regard. We also believe our property is adequately covered by insurance.
There are no legal proceedings pending, and we are not aware of any material proceeding contemplated by a governmental authority, to which we are a party or any of our property is subject.
| Item 4. | Mine Safety Disclosure |
Not applicable.
PART II
ITEM 5. MARKET FOR REGISTRANT’S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES
Our Common Stock is quoted on the OTCQB under the symbol “FCHS.”
The following table sets forth, for the period indicated, the quarterly high and low per share bid prices (adjusted for a reverse stock split effective April 4, 2012) for the common stock for each quarter during our last two fiscal years:
| 2013 | | High | | | Low | |
| First Quarter | | $ | 2.20 | | | $ | 1.00 | |
| Second Quarter | | $ | 1.75 | | | $ | 0.05 | |
| Third Quarter | | $ | 1.35 | | | $ | 0.40 | |
| Fourth Quarter | | $ | 2.10 | | | $ | 1.00 | |
| 2012 | | | | | | | | |
| First Quarter* | | $ | 4.04 | | | $ | 2.60 | |
| Second Quarter | | $ | 3.00 | | | $ | 2.70 | |
| Third Quarter | | $ | 2.95 | | | $ | 2.25 | |
| Fourth Quarter | | $ | 2.38 | | | $ | 1.50 | |
The above information was obtained from NASDAQ.com. Because these are over-the-counter market quotations, these quotations reflect inter-dealer prices, without retail mark-up, markdown or commissions and may not represent actual transactions. There is currently no public trading market for our preferred stock.
As of March 27, 2014, we had approximately 228 individual shareholders of record of our common stock, and the closing sales price on that date for our common stock was $2.59 per share. We believe that the number of beneficial owners of our common stock is greater than the number of record holders, because a number of shares of our common stock is held through brokerage firms in “street name.”
Dividend Policy
The Company has never declared or paid any cash dividends on its common stock. We have never paid cash dividends on our common stock. Under Delaware law, we may declare and pay dividends on our capital stock either out of our surplus, as defined in the relevant Delaware statutes, or if there is no such surplus, out of our net profits for the fiscal year in which the dividend is declared and/or the preceding fiscal year. If, however, the capital of our company, computed in accordance with the relevant Delaware statutes, has been diminished by depreciation in the value of our property, or by losses, or otherwise, to an amount less than the aggregate amount of the capital represented by the issued and outstanding stock of all classes having a preference upon the distribution of assets, we are prohibited from declaring and paying out of such net profits and dividends upon any shares of our capital stock until the deficiency in the amount of capital represented by the issued and outstanding stock of all classes having a preference upon the distribution of assets shall have been repaired. The Company does not intend to declare or pay any cash dividends on its common stock in the foreseeable future. The holders of the Company’s common stock are entitled to receive only such dividends (cash or otherwise) as may be declared by the Company’s Board of Directors.
Recent Sales of Unregistered Securities
CCR of Melbourne – Conversion of Debt to Equity
On February 1, 2012, the Company opened a $500,000 unsecured, revolving line of credit loan with CCR of Melbourne, Inc., an entity jointly owned and controlled at that time by Christian “Chris” Romandetti, the Company's Chief Executive Officer, and Carmen Charles Romandetti, our CEO’s father. The revolving line of credit loan was to mature on October 1, 2015 with interest at a per annum rate of 8.5% beginning March 1, 2012. Advances on the line of credit were at the sole discretion of CCR of Melbourne, Inc. On November 8, 2013, CCR converted the then outstanding balance of $142,483.52, representing all of the outstanding related party principal and interest amount on the loan, into shares of the Company’s common stock at a price equal to $0.45 per share for a total of 316,631 shares issued in reliance upon the exemption from registration under Section 4(a)(2) (formerly Section 4(2)) of the Securities Act. On November 8, 2013, Chris Romandetti relinquished all rights, title to and ownership in CCR to Carmen Romandetti in consideration of repayment of a personal loan made to Chris Romandetti by Carmen Romandetti.
MTI Capital – Conversion of Debt to Equity
On May 1, 2013, the Company entered into a loan commitment whereby MTI Capital LLC (“MTI”) provided a line of credit up to $2,000,000 in the form of a convertible loan with interest at 12% per annum, payable monthly with principal due two years from the effective date of the loan. On August 28, 2013, the Company amended the loan agreement to change the conversion rate from $0.75 per share to $0.45 per share.
On November 8, 2013, MTI converted the then outstanding balance of $624,000 principal and interest amount on the loan, into restricted shares of the Company’s common stock, in reliance upon the exemption from registration under Section 4(a)(2), at a price equal to $0.45 per share for a total of 1,386,667 shares issued. Our transfer agent reported to us that MTI redistributed the majority of its shares in our Company to unaffiliated third parties.
CT Capital, Ltd. – Modification of Line of Credit Involving Equity Consideration
On June 13, 2013, we entered into a Loan and Security Agreement (the “Loan Agreement”) with CT Capital, Ltd., d/b/a CT Capital, LP, a Florida limited liability partnership (the “Lender”). Under the Loan Agreement, the Lender committed to make an accounts receivable line of credit in the maximum aggregate amount of $1,500,000 to the Company with an interest rate of 12% per annum (the “Loan”). The maturity date of the Loan is December 31, 2016 (the “Maturity Date”). Interest shall be due and payable monthly. Upon default, the interest may be adjusted to the highest rate permissible by law. The Loan is secured by the accounts receivable and assets of the Company. The assets constituted the collateral for the repayment of the Loan. The Loan Agreement also included covenants, representations, warranties, indemnities and events of default that are customary for facilities of this type. The advance rate was defined as: 80% of all receivables to be 120 days or less at the true collection rate of approximately 27% of total billings, excluding patient billings and collections. Additionally, allowable accounts also included 50% of all accounts protected by Legal Letters of Protection. At any time up until December 31, 2016, the Lender may convert all or any portion of the outstanding principal amount or interest on the Loan into the common stock of the Company at a price equal to $0.75 per share.
On November 8, 2013, in consideration for a fee of 100,000 shares of the Company’s common stock, issued in reliance upon the exemption from registration under Section 4(a)(2) (formerly Section 4(2)) of the Securities Act, CT Capital agreed to modify the line of credit to the Company’s subsidiary, First Choice Medical Group of Brevard, LLC. Under the loan modification agreement, the annual rate of interest was reduced from 12% per annum to 6% per annum and will remain at 6% until November 1, 2015. All other terms under the June 13, 2013 Loan and Security Agreement will remain the same.
Convertible Notes
On December 14, 2012, February 19, 2013, and August 14, 2013, the Company entered into Securities Purchase Agreements for the sale of 8% convertible notes in the original principal amounts of $203,500, $103,500 and $153,500, respectively, with a lender in reliance upon the exemption from registration under Section 4(a)(2) (formerly Section 4(2)) of the Securities Act of 1933, as amended (the “Securities Act”). During the year ended December 31, 2013, the Company paid off each of these notes payable in cash.
Acquisition of Patent
On September 7, 2013, the Company acquired a patent, US 7,789,842 B2, for an orthopedic adjustable arm sling from Donald A. Bittar, the inventor and the Company’s Chief Financial Officer. Based on the independent, third party evaluation of Professional Business Brokers, Inc., the patent was valued at $286,500. The Company issued, in reliance upon the exemption from registration under Section 4(a)(2) (formerly Section 4(2)) of the Securities Act, to Mr. Bittar 636,666 shares of its common stock, valued at $286,500, or $0.45 per share, which was estimated to approximate the fair value of the patent acquired and did not materially differ from the fair value of the common stock at the time of issuance.
Hanover|Elite – Equity Compensation for Services
On October 2, 2013, the Company entered into a cancelable 12-month agreement to engage the services of Elite Financial Communications Group, LLC, d/b/a Hanover|Elite. The terms of the agreement provide for a monthly cash retainer; and 300,000 restricted shares of the Company’s common stock, which shall be earned and issued quarterly as follows: 37,500 shares on January 3, 2014, April 3, 2014, and July 3, 2014; and 187,500 shares on October 3, 2014. The shares will be issued in reliance upon the exemption from registration under Section 4(a)(2) (formerly Section 4(2)) of the Securities Act
Hillair Capital Investments, L.P. – Convertible Debenture
On November 8, 2013, the Company entered into a Securities Purchase Agreement (the “Securities Purchase Agreement”) with Hillair Capital Investments L.P. ("Hillair") whereby the Company received $2,000,000 in gross proceeds from Hillair in exchange for (i) a $2,320,000, 8% Original Issue Discount Convertible Debenture due December 28, 2013, subject to an extension through November 1, 2015 (the “Debenture”), and (ii) a Common Stock Purchase Warrant (the “Warrant”) to purchase up to 2,320,000 shares of the Company’s common stock (the “Common Stock”) at an exercise price of $1.35 per share, which may be exercised on a cashless basis, until November 8, 2018.
The Company issued to Hillair the Debenture with the Warrant, pursuant to Section 4(a)(2) of the Securities Act, for the net purchase price of $2,000,000 (reflecting the $320,000 original issue discount). Until the Debenture is no longer outstanding, the Debenture shall be convertible, in whole or in part at the option of Hillair, into shares of Common Stock, subject to certain conversion limitations set forth in the Debenture. The Company, however, has reserved the right to pay the Debenture in cash. The conversion price for the Debenture is $1.00 per share, subject to adjustment for stock splits, stock dividends, sales of securities for less than $1.00 per share of common stock or other distributions by the Company. As a result of the Company achieving certain milestones, however, the conversion price shall not be reduced to less than $1.00 per share as a result of any subsequent sales of securities for less than $1.00 per share of common stock.
The Company will be obligated to redeem $580,000 of principal on February 1, 2015, May 1, 2015, August 1, 2015 and November 1, 2015, plus accrued but unpaid interest and any other amounts that may be owed to the holder of the Debenture on those dates. Interest on the Debenture accrues at the rate of 8% annually and is payable quarterly on August 1, November 1, February 1, and May 1, beginning on August 1, 2014. Interest is payable in cash or at the Company’s option in shares of the Company’s common stock; provided certain conditions are met.
On or after May 8, 2014, the Company may elect to prepay any portion of the principal amount of the Debenture, subject to providing advance notice to the holder of the Debenture, at 120% of the then outstanding principal amount of the Debenture, plus accrued but unpaid interest and any other amounts then owed to the holder of the Debenture as further set forth therein, subject to certain conditions set forth in the Debenture.
To secure the Company’s obligations under the Debenture, the Company granted Hillair a security interest in certain of its and its subsidiaries’ assets in the Company as described in the Security Agreement. In addition, certain of the Company’s subsidiaries agreed to guarantee the Company’s obligations pursuant to the subsidiary guarantees.
A summary of the use of net proceeds received by the Company in the Hillair transaction is as follows:
| GROSS PROCEEDS FROM HILLAIR TRANSACTION | | $ | 2,000,000.00 | |
| Legal and Diligence Fees Associated with Hillair Transaction | | $ | 140,883.20 | |
| NET PROCEEDS | | $ | 1,859,116.80 | |
| Payment in Full from Escrow of Balance Due on Note with HS Real Company | | $ | 300,000.00 | |
| Payment in Full from Escrow of Balance Due on Accredited Investor Loan | | $ | 188,850.00 | |
| Expansion and Working Capital | | $ | 1,370,266.80 | |
Purchases by Issuer and Its Affiliates
None.
ITEM 6. Selected Financial Data
This item is not required for Smaller Reporting Companies.
ITEM 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations
The following discussion highlights the principal factors that have affected our financial condition and results of operations as well as our liquidity and capital resources for the periods described. This discussion should be read in conjunction with our Consolidated Financial Statements and the related notes included in Item 8 of this Form 10-K. This discussion contains forward-looking statements. Please see the explanatory note concerning “Forward-Looking Statements” in Part I of this Annual Report on Form 10-K and Item 1A. Risk Factors for a discussion of the uncertainties, risks and assumptions associated with these forward-looking statements. The operating results for the periods presented were not significantly affected by inflation.
Overview
FCHS’s mission is to transform, via acquisition and restructuring, multi-specialty clinics or physician-owned practices in the southeastern United States into world class, state-of-the-art medical centers of excellence; thereby establishing and extending ‘First Choice Healthcare Solutions’ brand and reputation as a profitable, well-managed enterprise committed to improving the quality of lives of the caregivers it employs and the health and wellness of the patients and families it serves.
The Company operates in two segments, healthcare services and real estate, through five wholly-owned subsidiaries:
| · | FCID Medical, Inc., which is the subsidiary under which our present center of excellence is owned and operated and future centers of excellence will be owned and operated; |
| · | First Choice Medical Group of Brevard, LLC, which is the Company’s flagship medical center of excellence located in Melbourne, Florida wholly-owned and operated by FCID Medical, Inc.; |
| · | FCID Holdings, Inc. which operates the Company’s real estate interests, and owns a 99% interest in Marina Towers, LLC; |
| · | MTMC of Melbourne, Inc., which owns a 1% ownership stake in Marina Towers, LLC; and |
| · | Marina Towers, LLC, which owns and operates Marina Towers, a Class A 78,000 square foot, six-story building located on the Indian River in Melbourne, Florida. |
By distinguishing our medical centers of excellence as premier destinations for clinically superior, patient-centric care that is coordinated across a patient’s care continuum, we expect to deliver more meaningful and collaborative doctor-patient experiences, accurate diagnoses, effective treatment plans, faster recoveries and materially reduced costs. Currently, our strategic focus is to grow in the southeastern United States through selective employment of physicians and/or the acquisition of physician practices that fit our defined acquisition criteria, including the following:
| · | presents the opportunity for FCHS to introduce additional ancillary revenue channels (i.e. on-site Magnetic Resonance Imaging (MRI), X-ray, Physical Therapy, diagnostic equipment, synergistic medical disciplines, durable medical equipment (DME), related health and wellness products, etc.) that will support and promote enhanced, well-coordinated, patient-centric care while supporting and promoting profitable business operations; |
| · | due diligence supporting economies of scale in billing, collections, purchasing, advertising and compliance that can be fully leveraged to reduce expenses and fuel income growth; and |
| · | creates the opportunity to increase awareness of FCHS’s brand; and aligns with and materially complements our Company’s inherent value proposition to patients, referring physicians and medical institutions, insurers, employers and other healthcare stakeholders in the local markets we serve. |
Model for Medical Centers of Excellence
FCHS’s model for each medical center of excellence is strictly defined to ensure that our high standards for patient care and attention can be fostered and preserved. Ideally, a center will:
| · | employ, on average, ten specialty physicians – all of whom are subject to a rigorous qualification and hiring process; |
| · | provide for the combination of synergistic medical disciplines and supported by related in-house ancillary diagnostic services and technologies, i.e. orthopedics/neurology/interventional pain medicine; |
| · | be capable of generating $16-$20 million when operating at optimal economic capacity; and |
| · | be housed in a commercial building, in close geographic proximity to a primary hospital(s), and allows for 12,000-16,000 square feet of usable space for build-out consideration. |
Because FCHS’s leadership view themselves as guardians of their ideals relating to optimal patient experience of care, we continually reinforce the importance of hiring, training, evaluating, compensating and supporting a workforce committed to patient-centered care. Just as vital, we engage our employees in all aspects of process design and treat them with the same dignity and respect that they are expected to show patients and family members. Central to the success of our Company’s long term growth strategy is attracting and recruiting top tier physicians and care specialists that rank in the top percentile of performance in the local markets we serve; and creating a work environment and corporate culture that serves to engage, motivate and retain them.
Due to sweeping healthcare reform, increased regulatory and reimbursement mandates and the financial challenges each of these impose, remaining in private practice is quickly losing its appeal for many physicians. In fact, according to a nationwide survey published in 2013 by recruiting firm Jackson Healthcare, one-third of U.S. physicians plan to leave private medical practice within the next ten years in favor of employment by hospitals and multi-specialty medical groups. Thus, the opportunity for our Company to attract key medical talent has never been more robust.
Our systems of operation unburden the Company’s physicians from productivity-driven, assembly line medicine, and materially diminish the cognitive overload and exhaustion that makes medical care anything but caring or patient-centered. More specifically, the many advantages and benefits of choosing employment by FCHS are being enabled to focus exclusively on delivering excellent patient care; higher income potential; freedom from day-to-day practice administration, including marketing and generating new patient leads; access to state-of-the-art technology, diagnostics and services; and camaraderie and collaboration with a cadre of first rate caregivers dedicated to common, patient-centered goals and objectives. The requirements for running the day-to-day business functions of the centers are the sole responsibility of our management team – and not the physicians. Simply put, doctors get to be doctors.
Currently, we are actively engaged in identifying and pursuing discussions with prospective acquisitions in key target markets – with those being largely in the southeastern U.S. We anticipate investing $4-$6 million to acquire and/or develop one or more medical centers of excellence during the next 12 months, each center may require up to 6-12 months to achieve optimal economic capacity, depending on the number of physicians and physician assistants to be employed, the medical service mix and the type of diagnostic and ancillary services to be offered.
Payor Mix
We bill third-party payors for professional services provided by our physicians to our patients based upon rates for specific services provided. Our billed charges are substantially the same for all parties regardless of the party responsible for paying the bill for our services. We determine our net patient service revenue based upon the difference between our gross fees for services and our estimated ultimate collections from payors. Net patient service revenue differs from gross fees due to (i) managed care payments at contracted rates, (ii) government-sponsored healthcare program reimbursements at government-established rates, (iii) various reimbursement plans and negotiated reimbursements from other third-parties, and (iv) discounted and uncollectible accounts of private-pay patients.
Our payor mix is composed of contracted managed care, government, principally Medicare and TRICARE, other third-parties, including workers compensation and Legal Letters of Protection work, and private-pay patients. We currently do not accept Medicaid patients.
The following is a summary of our payor mix, expressed as a percentage of net patient service revenue, exclusive of administrative fees, for the periods indicated:
| Payor Mix | | Average % | |
| Insurance - Third Party Payors | | | 48 | % |
| Gov't - Medicare & TRICARE | | | 38 | % |
| Workman's Compensation | | | 6 | % |
| Legal Letters of Protection | | | 5 | % |
| Other | | | 3 | % |
| Total | | | 100 | % |
Critical Accounting Policies
Basis of Accounting
The financial statements of the Company are prepared in conformity with accounting principles generally accepted in the United States of America (“GAAP”). The preparation of these financial statements requires our management to make estimates and assumptions about future events that affect the amounts reported in the financial statements and related notes. Future events and their effects cannot be determined with absolute certainty. Therefore, the determination of estimates requires the exercise of judgment. We believe the following critical accounting policies affect its more significant judgments and estimates used in the preparation of financial statements.
Revenue Recognition
The Company recognizes revenue in accordance with Accounting Standards Codification subtopic 605-10, Revenue Recognition (“ASC 605-10”) which requires that four basic criteria must be met before revenue can be recognized: (1) persuasive evidence of an arrangement exists; (2) delivery has occurred; (3) the selling price is fixed and determinable; and (4) collectability is reasonably assured. Determination of criteria (3) and (4) are based on management's judgments regarding the fixed nature of the selling prices of the products delivered and the collectability of those amounts. Provisions for discounts and rebates to customers, estimated returns and allowances, and other adjustments are provided for in the same period the related sales are recorded.
ASC 605-10 incorporates Accounting Standards Codification subtopic 605-25, Multiple-Element Arraignments (“ASC 605-25”). ASC 605-25 addresses accounting for arrangements that may involve the delivery or performance of multiple products, services and/or rights to use assets. The effect of implementing 605-25 on the Company's financial position and results of operations was not significant.
Derivative Financial Instruments
Accounting Standards Codification subtopic 815-40, Derivatives and Hedging, Contracts in Entity’s own Equity (“ASC 815-40”) became effective for the Company on October 1, 2009. The Company’s convertible debt has conversion provisions based on a discount the market price of the Company’s common stock.
Stock-Based Compensation
Share-based compensation issued to employees is measured at the grant date, based on the fair value of the award, and is recognized as an expense over the requisite service period. The Company measures the fair value of the share-based compensation issued to non-employees using the stock price observed in the arms-length private placement transaction nearest the measurement date (for stock transactions) or the fair value of the award (for non-stock transactions), which were considered to be more reliably determinable measures of fair value than the value of the services being rendered. The measurement date is the earlier of (1) the date at which commitment for performance by the counterparty to earn the equity instruments is reached, or (2) the date at which the counterparty’s performance is complete.
Income Tax
The Company accounts for income taxes pursuant to Accounting Standards Codified 740 (“ASC 740”). Under ASC 740 deferred taxes are provided on a liability method whereby deferred tax assets are recognized for deductible temporary differences and operating loss carry forwards and deferred tax liabilities are recognized for taxable temporary differences. Temporary differences are the differences between the reported amounts of assets and liabilities and their tax bases. Deferred tax assets are reduced by a valuation allowance when, in the opinion of management, it is more likely than not that some portion or all of the deferred tax assets will not be realized. Deferred tax assets and liabilities are adjusted for the effects of changes in tax laws and rates on the date of enactment.
Results of Operations
Year Ended December 31, 2013 as Compared to Year Ended December 31, 2012
Results of Operations
The following is a discussion of the results of operations for the year ended December 31, 2013 compared to the year ended December 31, 2012.
Revenues
Total revenues rose 71% to $6,507,842 for the year ended December 31, 2013, compared to revenue of $3,805,347 for the year ended December 31, 2012. The increase in revenue is primarily due to the increase in net patient service revenue to $5,459,373 for the year ended December 31, 2013 compared to $2,645,310 for the year ended December 31, 2012. The increase in net patient service revenue is attributable to the full-year results from the acquisition of First Choice Medical Group of Brevard, LLC completed in April 2012, and the growth of the medical practice.
Operating Expenses
Operating expenses include the following:
| | | Year Ended 12/31/2013 | | | Year Ended 12/31/2012 | |
| Salaries and Benefits | | $ | 3,096,285 | | | $ | 1,593,245 | |
| Other operating expenses | | | 1,715,942 | | | | 865,641 | |
| General and administrative | | | 1,705,154 | | | | 1,314,302 | |
| Impairment of investment | | | 450,000 | | | | - | |
| Depreciation and amortization | | | 518,611 | | | | 309,899 | |
| Total operating expenses | | $ | 7,485,992 | | | $ | 4,083,087 | |
The major components of operating expenses include practice salaries and benefits, practice supplies and other operating costs, write down of doubtful accounts totaling $361,284, depreciation and general and administrative expenses, which included legal, accounting and professional fees associated with being a public entity.
Salaries and benefits increased 94% to $3,096,285 for the year ended December 31, 2013 compared to $1,593,245 for the year ended December 31, 2012. The increase is attributable to the full-year results from acquisition of First Choice Medical Group of Brevard, LLC completed in April 2012, coupled with the hiring of five additional physicians and their support staff during 2013. For the same reason, other operating expenses increased 98% to $1,715,942 from $865,641.
General and administrative expenses for the year ended December 31, 2013 increased 30% to $1,705,154 compared to $1,314,302, an increase attributable to expenses related to our growth and capital restructuring. We believe that each additional sale or service and corresponding gross profit of such sale or service has minimal incremental offsetting operating expenses. Thus, additional sales could contribute to profit at a higher rate of return on sales as a result of not needing to expand operating expenses at the same pace as sales.
At December 31, 2013, the Company’s management performed an evaluation of its investment in MedTech for purposes of determining the implied fair value of the asset at December 31, 2013. The test indicated that the recorded remaining book value of its investment exceeded its fair value for the year ended December 31, 2013. As a result, upon completion of the assessment, management recorded a non-cash impairment charge of $450,000, net of tax, or $0.03 per share during the year ended December 31, 2013, to reduce the carrying value of the investment to $0.
Depreciation and amortization increased from $367,247 for the year ended December 31, 2012 to $575,959 for the year ended December 31, 2013. The increase is a direct result of the full year of depreciation and amortization of assets acquired in April 2012 from First Choice Medical Group of Brevard, LLC, as well as the addition of new equipment in 2013. This compared to only nine months of depreciation and amortization in 2012.
Net Income (Loss) on Operations
The loss from operations for the year ended December 31, 2013 increased to $978,150, which compared to a loss from operations of $277,740 for the prior year. Notwithstanding non-cash expenses totaling $1,575,400 for the 12 months in 2013, which included stock-based compensation, impairment of investment, depreciation and amortization, income from operations totaled $597,250, which compared to income from operations of $89,507 after factoring $367,247 in non-cash depreciation and amortization recorded for the full year 2012.
Interest Expense
Interest expense was $3,704,086 for the year ended December 31, 2013 compared to $563,391 for the year ended December 31, 2012. Historically, interest expense was primarily attributable to our mortgage interest on our building. The increase in interest expense, however, was a result of corporate interest expense of $2,970,243 for the year ended December 31, 2013 compared to $19,381 for the year ended December 31, 2012. In the second half of 2013, we increased our borrowings to grow our medical business and restructured our debt and, as a result, incurred additional non-cash interest expense.
On November 8, 2013, we entered into a securities purchase agreement with Hillair Capital Investments L.P. ("Hillair") whereby the Company issued Hillair (i) a $2,320,000, 8% original issue discount convertible debenture due initially due December 28, 2013, subsequently extended through November 1, 2015 and (ii) a common stock purchase warrant to purchase up to 2,320,000 shares of the Company’s common stock. We issued detachable warrants granting the holder the right to acquire an aggregate of 2,320,000 shares of the Company’s common stock at $1.35 per share on a cashless basis. During the year ended December 31, 2013, the Company amortized $1,871,117 of the debt discount associated with the debenture and the warrant as interest expense.
Further, during the years ended December 31, 2013 and 2012, the Company amortized and wrote off $2,706,869 and $10,457 of debt discount as non-cash interest expense for convertible notes.
Net Loss
As a result of all the above, we had a net loss of $4,704,303 for the year ended December 31, 2013 compared to net loss of $873,363 for the year ended December 31, 2012.
Segment Results
The Company reports segment information based on the “management” approach. The management approach designates the internal reporting used by management for making decisions and assessing performance as the source of the Company’s reportable segments. The following are the revenues, operating expenses and net income (loss) by segment for the years ended December 31, 2013 and December 31, 2012. The significant fluctuations in the line items are described above.
For the year ended December 31, 2013
| | | Marina | | | FCID | | | | | | Intercompany | | | | |
| | | Towers | | | Medical | | | Corporate | | | Eliminations | | | Total | |
| Revenue: | | | | | | | | | | | | | | | | | | | | |
| Net patient service revenue | | $ | - | | | $ | 5,459,373 | | | $ | - | | | $ | - | | | $ | 5,459,373 | |
| Rental revenue | | | 1,473,048 | | | | - | | | | - | | | | (424,579 | ) | | | 1,048,469 | |
| Total revenue | | | 1,473,048 | | | | 5,459,373 | | | | - | | | | (424,579 | ) | | | 6,507,842 | |
| Total operating expenses | | | 644,782 | | | | 5,314,808 | | | | 1,950,981 | | | | (424,579 | ) | | | 7,485,992 | |
| Net income (loss) from operations: | | $ | 828,266 | | | $ | 144,565 | | | $ | (1,950,981 | ) | | $ | - | | | $ | (978,150 | ) |
For the year ended December 31, 2012
| | | Marina | | | FCID | | | | | | Intercompany | | | | |
| | | Towers | | | Medical | | | Corporate | | | Eliminations | | | Total | |
| Revenue: | | | | | | | | | | | | | | | | | | | | |
Net patient service revenue | | $ | - | | | $ | 2,645,310 | | | $ | - | | | $ | - | | | $ | 2,645,310 | |
| Rental revenue | | | 1,459,092 | | | | - | | | | - | | | | (299,055 | ) | | | 1,160,037 | |
| Total Revenue | | | 1,459,092 | | | | 2,645,310 | | | | - | | | | (299,055 | ) | | | 3,805,347 | |
| Total operating expenses | | | 619,210 | | | | 2,800,812 | | | | 962,120 | | | | (299,055 | ) | | | 4,083,087 | |
| Net income (loss) from operations: | | $ | 839,882 | | | $ | (155,502 | ) | | $ | (962,120 | ) | | $ | - | | | $ | (277,740 | ) |
Liquidity and Capital Resources
We incurred various non-recurring expenses in 2012 in connection with operating startup costs relating to the acquisition of a medical practice. Management believes the positive year-end earnings before interest, taxes, depreciation and amortization and the continuing trend of positive growth before interest, taxes, depreciation and amortization through 2014 will support improved liquidity. Moreover, we issued and sold to Hillair Capital Investments, L.P. a $2,320,000 8% Original Issue Discount Convertible Debenture, raising net proceeds of $2,000,000 less customary legal and due diligence fees. We then paid off or converted to equity a total of $1,238,480 in debt and modified the $1.5 million line of credit with CT Capital, providing for the reduction of the annual interest rate from 12% per annum to 6% per annum in exchange for the issuance of 100,000 restricted shares of our common stock. As of December 31, 2013, we used $800,000 of the available CT Capital line of credit, leaving an available balance of $700,000.
The Marina Towers building is 95% occupied. We believe that ongoing operations of Marina Towers, LLC, the current positive cash balance along with continued execution of Marina Tower’s business development plan will allow us to further improve its working capital; and that it will have sufficient capital resources to meet projected cash flow requirements through the date that is one year plus a day from the filing date of this report. However, there can be no assurance that we will be successful in fully executing its business development plan.
We significantly increased our cash and current assets during the year ended December 31, 2013 due to cash flows provided by financing activities. As of December 31, 2013, we had cash or cash equivalents, restricted cash and total current assets of $739,158; $256,246 and $2,465,487, respectively, compared to cash or cash equivalents and total current assets of $67,045; $221,148 and $934,378, respectively, as of December 31, 2012.
Net cash used in operating activities was $(1,264,058) for the year ended December 31, 2013, compared to cash used in operating activities of $(788,853) for the same period last year. The increase in cash used was a result of a $3,830,940 higher net loss partially offset by non-cash items that affected the net loss, including $2,706,869 for the amortization of debt discount, $361,284 for the write down of doubtful accounts, $450,000 for the impairment of an investment, $549,441 for stock-based compensation and $518,611 in depreciation. Cash used in operations was also impacted by the use of cash associated with the increase of accounts receivable, which increased to $1,272,155 as of December 31, 2013, compared to $527,867 as of December 31, 2012.
Net cash flows used in investing activities was $(372,186) for the year ended December 31, 2013, compared to $(2,852,259) used in investing activities for the year ended December 31, 2012. The increased level of cash used in investing activities during the year ended December 31, 2012 was the result of $2,773,450 in equipment purchases in 2012, as we acquired First Choice Medical Group of Brevard, LLC, compared with $397,688 in equipment purchases in 2013.
Cash flows provided by financing activities was $2,308,357 for year ended December 31, 2013, compared to net cash provided by financing activities of $3,179,854 for the year ended December 31, 2012. The cash flows provided by financing activities were the result of:
| | | Year ended 12/31/2013 | | | Year ended 12/31/2012 | |
| Net (payments) proceeds from related party line of credit | | $ | (10,846 | ) | | $ | 190,000 | |
| Proceeds from convertible note payable | | | 2,128,117 | | | | 203,500 | |
| Proceeds from lines of credit | | | 1,373,208 | | | | - | |
| Proceeds from issuance of notes payable, net of financing costs | | | 152,659 | | | | 2,871,058 | |
| Proceeds from common stock subscription | | | - | | | | 100,000 | |
| Net payments on notes payable | | | (1,334,781 | ) | | | (184,704 | ) |
| Net cash provided by financing activities | | $ | 2,308,357 | | | $ | 3,179,854 | |
On June 13 2013, we entered into a Loan and Security Agreement (the “Loan Agreement”) with CT Capital. Ltd., d/b/a CT Capital, LP, a Florida limited liability partnership (the “Lender”). Under the Loan Agreement, the Lender has committed to make an accounts receivable line of credit in the maximum aggregate amount of $1,500,000 to the Borrower with an interest rate of 12% per annum (the “Loan”). The maturity date of the Loan is December 31, 2016 (the “Maturity Date”). Interest shall be due and payable monthly. Upon default, the interest may be adjusted to the highest rate permissible by law. The Loan is secured by the accounts receivable, among other assets of the Borrower, and our assets. The assets constitute the collateral for the repayment of the Loan. The Loan Agreement also includes covenants, representations, warranties, indemnities and events of default that are customary for facilities of this type. The advance rate is defined as: 80% of all receivables to be 120 days or less at the true collection rate of approximately 27% of total billings, excluding patient billings and collections. Additionally, allowable accounts will also include 50% of all accounts protected by Legal Letters of Protection. At any time, the Lender may convert all or any portion of the outstanding principal amount or interest on the Loan into our common stock at a price equal to $0.75 per share.
On November 8, 2013, in consideration for a fee of 100,000 shares of our common stock, restricted pursuant to Rule 144, CT Capital agreed to modify the line of credit to our subsidiary, First Choice Medical Group of Brevard, LLC. Under the loan modification agreement, the annual rate of interest was reduced from 12% per annum to 6% per annum and will remain at 6% until November 1, 2015. All other terms under the June 13, 2013 Loan and Security Agreement will remain the same.
On November 8, 2013, we entered into a Securities Purchase Agreement (the “Securities Purchase Agreement”) with Hillair Capital Investments L.P. ("Hillair") whereby we issued Hillair (i) a $2,320,000, 8% original issue discount convertible debenture that was initially due December 28, 2013, but subsequently extended through November 1, 2015 and (ii) a common stock purchase warrant to purchase up to 2,320,000 shares of our common stock. The closing of the debenture and warrant transaction occurred on November 8, 2013.
Currently, we are actively engaged in identifying and pursuing discussions with prospective acquisitions in key target markets – with those being largely in the southeastern U.S. Over the next 12 months, we expect to incur significant capital costs to further develop and expand operations. We plan to add another medical center of excellence and purchase additional diagnostic equipment for our operations. We expect to need additional capital of approximately $4-6 million to fund the development and expansion of our operations in 2014. However, there can be no assurance that we will be able to negotiate acceptable terms for, or find suitable candidates for, such acquisition.
There can be no assurance that our cash flow will increase in the near future from anticipated new business activities, or that revenues generated from our existing operations will be sufficient to allow us to continue to pursue new customer programs or profitable ventures.
Contractual Obligations
At December 31, 2013, we had certain obligations and commitments under our loans and capital leases totaling approximately $9,679,261 as follows:
| | | Total | | | 2014 | | | 2015 | | | 2016 | | | 2017 | | | 2018 and Later | |
| Leases | | $ | 1,924,387 | | | $ | 406,670 | | | $ | 447,897 | | | $ | 485,433 | | | $ | 519,892 | | | $ | 64,495 | |
| Loans | | | 7,754,874 | | | | 337,117 | | | | 267,188 | | | | 7,146,853 | | | | 3,716 | | | | | |
| Total | | $ | 9,679,261 | | | $ | 743,787 | | | $ | 715,085 | | | $ | 7,632,286 | | | $ | 523,608 | | | $ | 64,495 | |
Inflation
Our opinion is that inflation has not had, and is not expected to have, a material effect on our operations.
Climate Change
Our opinion is that neither climate change, nor governmental regulations related to climate change, have had, or are expected to have, any material effect on our operations.
Off-Balance Sheet Arrangements
At December 31, 2013, we did not have any off-balance sheet arrangements that have or are reasonably likely to have a current or future effect on our financial condition, changes in financial condition, revenue or expenses, results of operations, liquidity, capital expenditures or capital resources.
New Accounting Pronouncements
There were various updates recently issued, most of which represented technical corrections to the accounting literature or application to specific industries and are not expected to a have a material impact on the Company’s condensed consolidated financial position, results of operations or cash flows.
ITEM 7A. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK
This Item is not required for a Smaller Reporting Company.
ITEM 8. FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA
Our financial statements are contained in pages F-1 through F-26, which appear at the end of this Annual Report on Form 10-K.
ITEM 9. CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE
None.
ITEM 9A. CONTROLS AND PROCEDURES
Evaluation of Disclosure and Control Procedures
The Company’s Chief Executive Officer and the Company’s Chief Financial Officer evaluated the effectiveness of the Company’s disclosure controls and procedures as of December 31, 2013 and had concluded that the Company’s disclosure controls and procedures are effective. The termdisclosure controls and proceduresmeans controls and other procedures that are designed to ensure that information required to be disclosed by the Company in the reports that it files or submits under the Securities Exchange Act of 1934, as amended, is recorded, processed, summarized and reported, within the time periods specified in the SEC’s rules and forms. Disclosure controls and procedures include, without limitation, controls and procedures designed to ensure that information required to be disclosed by the Company in the reports that it files or submits under the Securities Exchange Act of 1934 is accumulated and communicated to the Company’s management, including its principal executive and principal financial officers, or persons performing similar functions, as appropriate to allow timely decisions regarding required disclosure.
Management’s Report on Internal Control over Financial Reporting
The Company’s management is responsible for establishing and maintaining an adequate system of internal control over financial reporting, as defined in Rule 13a-15(f) under the Exchange Act. The Company’s internal control over financial reporting is designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements in accordance with Generally Accepted Accounting Principles (“GAAP”).
Because of its inherent limitations, a system of internal control over financial reporting can provide only reasonable assurance of such reliability and may not prevent or detect misstatements. Also, projection of any evaluation of effectiveness to future periods is subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Management has conducted, with the participation of our Chief Executive Officer and our Chief Financial Officer, an assessment of the effectiveness of our internal control over financial reporting as of December 31, 2013. Management’s assessment of internal control over financial reporting used the criteria set forth in SEC Release 33-8810 based on the framework established by the Committee of Sponsoring Organizations of the Treadway Commission (“COSO”) inInternal Control over Financial Reporting – Guidance for Smaller Public Companies. Based on this evaluation, Management concluded that our system of internal control over financial reporting was effective as of December 31, 2013, based on these criteria.
This Annual Report on Form 10-K does not include an attestation report of our independent registered public accounting firm regarding internal control over financial reporting. As a smaller reporting company, our management's report was not subject to attestation by our registered public accounting firm pursuant to rules of the Securities and Exchange Commission that permit us to provide only the management's report.
Changes in Internal Control over Financial Reporting
There were no changes in our internal control over financial reporting, as defined in Rules 13a-15(f) and 15d-15(f) under the Exchange Act, during the fourth quarter of the year ended December 31, 2013 that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
Item 9B. Other Information
None.
PART III
ITEM 10. DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE
The following table and biographical summaries set forth information, including principal occupation and business experience about our directors and executive officers:
| Name | | Age | | Position | | Officer and/or
Director Since |
| | | | | | | |
| Christian C. Romandetti | | 53 | | President, Chief Executive Officer and Director | | December 2010 |
| Donald A. Bittar | | 72 | | Chief Financial Officer, Treasurer, Secretary and Director | | December 2010 |
| Colin Halpern | | 76 | | Director | | November 2012 |
Christian “Chris” Romandetti – President and Chief Executive Officer
A serial entrepreneur and proven senior executive with experience in a broad range of industries, Mr. Romandetti has served as First Choice Healthcare Solution’s Chairman, President and CEO since December 2010. In this role, he is responsible for articulating the Company’s vision and executing strategies that place clinically superior, patient-centric care and improved clinical outcomes at the core of FCHS’s corporate mission.
Since 2003 through to the present, Mr. Romandetti has been the Managing Member of Marina Towers, LLC, which is now a wholly owned subsidiary of FCHS; and the Managing Member of C&K, LLC, a property holding company. Since 2007, he has also lent his business building expertise to medical practices and MRI centers as a professional business consultant to the healthcare industry. Previously, he was a founding director of Sunrise Bank, a community bank serving local businesses in Florida’s Space Coast and served as an executive officer for numerous companies in the real estate, marine, automotive and construction products industries.
Donald A. Bittar – Chief Financial Officer and Director
In December 2010, Mr. Bittar was appointed as the Company’s CFO, Treasurer and Secretary and a member of the Board of Directors. He brings First Choice Healthcare Solutions more than 30 years’ experience working with companies as an officer, board member and consultant. Before joining the FCHS leadership team, Mr. Bittar served as President and Chairman of Associated Mortgage of North America and President of DA Bittar and Associates, Inc., a management and technology consulting firm that he founded in 1980. From 1969 to 1980, he was Chairman, President and CEO of Marine Telephone, Inc. Since 1969, he has also taught finance, management and information technology at several leading undergraduate and graduate schools. Currently, Mr. Bittar is an Adjunct Professor at Florida Institute of Technology, College of Business, where he was honored as Teacher of the Year in 2013.
In addition to authoringGetting Under the Hood of an Annual Report and Knowing What is Inside, Mr. Bittar invented and was granted a U.S. patent for an adjustable sling that can be used to hold a patient’s arm, wrist and hand in multiple positions while eliminating stress to the neck and shoulder. He has been a frequent speaker at the National Association of Mortgage Bankers, National Council of Savings Institutions, Council of Presidents, New England Bankers Association and National Corporate Cash Managers Association. Donald received a Master of Business Administration degree from Long Island University.
Colin Halpern, Director
Mr. Halpern was appointed as a Director of the Company in November 2012. A highly accomplished multi-national business executive, entrepreneur and real estate developer, he currently serves as the Non-Executive Chairman of Domino’s Pizza Group UK and IRL PLC, the holder of the Domino’s Pizza Master Franchise Rights for the United Kingdom and Republic of Ireland. Mr. Halpern acquired the exclusive rights to own, operate and franchise Domino’s Pizza in 1993 through International Franchise Systems, Inc. In November 1999, with him as Chairman, the Company was taken public and listed on the London Stock Exchange, and now is a constituent of the FTSE 250 Index with 2012 sales of approximately US$390 Million and 20,000 employees worldwide.
Colin also serves as the Managing Director of HS Real Company, LLC; Chairman of Calumet Holdings, LLC; Chairman of Dayenn Limited; President and CEO of NPS Technologies Group; and Chairman of Universal Services Group, among many others.
Board of Directors’ Term of Office
Directors are elected at our annual meeting of shareholders and serve for one year until the next annual meeting of shareholders or until their successors are elected and qualified.
Family Relationships
There are no family relationships among the officers and directors, nor are there any arrangements or understanding between any of the Directors or Officers of our Company or any other person pursuant to which any Officer or Director was or is to be selected as an officer or director.
Involvement in Certain Legal Proceedings
During the last ten years, none of our officers, directors, promoters or control persons have been involved in any legal proceedings as described in Item 401(f) of Regulation S-K.
Board Meetings; Committee Meetings; and Annual Meeting Attendance
During 2013, the Board of Directors held 7 meetings. Each meeting was attended by all of the members of the Board.
Committees of the Board of Directors
There are no committees of the Board of Directors.
Changes in Nominating Process
There are no material changes to the procedures by which security holders may recommend nominees to our Board of Directors.
Shareholder Recommendations for Board Nominees
The Board does not have a Governance or Nominating Committee that is tasked with identifying individuals qualified to become Board members and recommending to the Board the director nominees for the next annual meeting of shareholders. Until such committee is formed, the shareholder recommendations for Board nominees would be directed to the entire Board, who will consider the qualifications of the person recommended based on a variety of factors, including:
| • | the appropriate size and the diversity of our Board; |
| • | our needs with respect to the particular talents and experience of our directors; |
| • | the knowledge, skills and experience of nominees, including experience in technology, business, finance, administration or public service, in light of prevailing business conditions and the knowledge, skills and experience already possessed by other members of the Board; |
| • | experience with accounting rules and practices; |
| • | whether such person qualifies as an “audit committee financial expert” pursuant to the SEC Rules; |
| • | appreciation of the relationship of our business to the changing needs of society; and |
| • | the desire to balance the considerable benefit of continuity with the periodic injection of the fresh perspective provided by new members. |
Compliance with Section 16(A) of the Exchange Act
Section 16(a) of the Exchange Act requires the Company’s directors, officers and stockholders who beneficially own more than 10% of any class of equity securities of the Company registered pursuant to Section 12 of the Exchange Act, collectively referred to herein as the “Reporting Persons,” to file initial statements of beneficial ownership of securities and statements of changes in beneficial ownership of securities with respect to the Company’s equity securities with the SEC. All Reporting Persons are required by SEC regulation to furnish us with copies of all reports that such Reporting Persons file with the SEC pursuant to Section 16(a). Based solely on our review of the copies of such reports and upon written representations of the Reporting Persons received by us, we believe that all Section 16(a) filing requirements applicable to such Reporting Persons have been timely met, except that Mr. Bittar and Mr. Romandetti inadvertently each did not file a Form 3 for share issuances from the Company but filed a Form 5 to report such issuances on March 27, 2014 and Mr. Halpern inadvertently did not file a Form 3 for two share issuances from the Company.
Code of Ethics
The Company has adopted a Code of Ethics for adherence by its Chief Executive Officer and Chief Financial Officer to ensure honest and ethical conduct; full, fair and proper disclosure of financial information in the Company's periodic reports filed pursuant to the Securities Exchange Act of 1934; and compliance with applicable laws, rules, and regulations. Any person may obtain a copy of our Code of Ethics, without charge, by mailing a request to the Company at the address appearing on the front page of this Annual Report on Form 10-K or by viewing it on our website found at www.myfchs.com.
Item 11. Executive Compensation
The following table sets forth compensation information for services rendered by certain of our executive officers in all capacities during the last two completed fiscal years. The following information includes the dollar value of base salaries and certain other compensation, if any, whether paid or deferred. The executive officers of the company did not receive any stock award, option award, non-equity incentive plan compensation, or nonqualified deferred compensation earnings during the last two completed years.
Summary Compensation Table
| Name and Position(s) | | Year | | | Salary
($) | | | Bonus
($) | | | Stock
Awards
($) | | | Other
($)(1) | | | Total
Compensation
($) | |
| Christian C. Romandetti | | | 2013 | | | | 240,000 | | | | 23,750 | | | | 33,000 | | | | 36,347 | | | | 333,097 | |
| President, CEO and Director | | | 2012 | | | | 168,000 | | | | 9,000 | | | | - | | | | 60,108 | | | | 237,108 | |
| | | | | | | | | | | | | | | | | | | | | | | | | |
| Donald A. Bittar, CFO, | | | 2013 | | | | 26,500 | | | | | | | | 33,000 | | | | | | | | 59,500 | |
| Secretary, Treasurer and Director | | | 2012 | | | | 12,350 | | | | - | | | | - | | | | | | | | 12,350 | |
(1) Consists of provision of an automobile, computer equipment and reimbursement of business expenses.
Employment Agreements
The Company entered a formal five-year employment agreement (the “Employment Agreement”) with Christian “Chris” Romandetti, dated March 20, 2014 and effective January 1, 2014, to serve as the Company’s President and Chief Executive Officer. Pursuant to the terms and conditions set forth in the Employment Agreement, Mr. Romandetti is entitled to receive an annual base salary of $250,000, which shall increase no less than 5% per annum for the term of the Employment Agreement. Mr. Romandetti is entitled to (i) five weeks of vacation per year that if not used in any given one year will accrue and (ii) participate in all benefit plans the Company provides to its senior executives and the Company will pay 100% of all costs associated with such plans and will reimburse Mr. Romandetti for all reasonable out-of-pocket expenses and $1,000 per month for auto expenses.
Mr. Romandetti, upon successfully achieving annual revenue milestones, is entitled to receive a bonus equal to 10% of his salary when $7.1 million in total annual revenue is reported in a fiscal year scaling up to a bonus equal to 800% of his salary if and when $100 million in total annual revenue is reported in a fiscal year. If the Company is unable to pay any portion of the bonus compensation when due because of insufficient liquidity or applicable restrictions under prevailing debt financing agreements, then, as an accommodation to the Company, Mr. Romandetti shall be able to convert bonus compensation into shares of the Company’s common stock at a 30% discount to the average closing price during the first calendar month after the end of the fiscal year. Mr. Romandetti will also be entitled to receive a strategic bonus of $100,000, payable in cash, on the sixth month anniversary of opening each new center of excellence.
Pursuant to the Company achieving specific financial performance benchmarks established by the Board of Directors, Mr. Romandetti will also be entitled to receive a cashless option to purchase up to 1 million shares of common stock per year. The exercise price of the options will be the fair market value of the average closing price of the stock during the first calendar month after the end of the fiscal year. Mr. Romandetti shall have up to five years from the date of the annual option grant to exercise the option. In addition to the above compensation consideration, Mr. Romandetti will be entitled to receive annual restricted stock compensation equal to 100% of the total base salary and bonus compensation. The fair market value of the restricted stock grant shall be determined using the average closing price of the common stock during the first calendar month after the end of the fiscal year.
Upon the expiration of the initial five-year term, the Employment Agreement shall automatically be extended for additional terms of one year each unless either party gives 90 day prior written notice of non-renewal. In addition, Mr. Romandetti’s Employment Agreement provides that, upon Mr. Romandetti’s death, disability, termination for any reason other than “Cause” (as such term is defined in the Employment Agreement) or resignation for “Good Reason” (as such term is defined in the Employment Agreement), the Company will pay to Mr. Romandetti 12 months of his annual base salary at the time of separation in accordance with the Corporation’s usual payroll practices and in case of disability additionally the payment on a prorated basis of any bonus or other payments earned in connection with the Company’s then-existing bonus plan in place at the time of such termination. Finally, Mr. Romandetti is subject to standard non-compete and non-solicit covenants during the course of his employment and for a period of 12 months after the date that he is no longer employed by the Company.
Compensation of Directors
The following table sets forth the compensation paid our Board of Directors in fiscal 2013:
| Name | | Shares (#) | | | Shares ($) | |
| Donald A. Bittar | | | 60,000 | | | $ | 33,000 | |
| Colin Halpern | | | 75,000 | | | | 77,250 | |
| Mel Lazar | | | 30,000 | | | | 52,500 | |
| Christian C. Romandetti | | | 60,000 | | | | 33,000 | |
| Totals | | | 225,000 | | | $ | 195,750 | |
In February 2013, the Company issued 60,000 shares of its common stock to members of its Board of Directors for services rendered. The shares of common stock were valued at $105,000 which was estimated to be approximate the fair value of the Company’s common shares during the period covered by the service provided.
In September 2013, the Company issued 165,000 shares of its common stock to members of its Board of Directors for services rendered. The shares of common stock were valued at $90,750, which was estimated to be approximate the fair value of the Company’s common shares during the period covered by the service provided.
Effective March 20, 2013, Mr. Lazar resigned as a director of the Company. His resignation expressed that the reason was personal and not by reason of any disagreement with the Company, financial or otherwise.
Outstanding Equity Awards at 2013 Fiscal Year-End
The Company had no outstanding equity awards as of December 31, 2013.
Potential Payments upon Termination or Change in Control
We do not have any contract, agreement, plan or arrangement that provides for any payment to any of our Named Executive Officers at, following, or in connection with a termination of the employment of such Named Executive Officer, a change in control of the Company or a change in such Named Executive Officer’s responsibilities.
Item 12. Security Ownership of Certain Beneficial Owners and Management
The following table sets forth information as of March 27, 2014 based on information obtained from the persons named below, with respect to the beneficial ownership of our common and preferred stock by (i) each person (including groups) known to us to be the beneficial owner of more than five percent (5%) of our common stock, or (ii) each Director and Officer, and (iii) all Directors and Officers of the Company, as a group. Except as otherwise indicated, all stockholders have sole voting and investment power with respect to the shares listed as beneficially owned by them, subject to the rights of spouses under applicable community property laws.
| Name and Address of Beneficial Owner | | Number of Shares of
Common Stock (1) (2) | | | Percent of Class | |
| Christian C. Romandetti (3) (9) | | | 7,610,000 | | | | 45.3 | % |
| GIRT FT, LLC (4) (9) | | | 5,750,000 | | | | 34.2 | % |
| MedTRX Provider Network, LLC (5) (9) | | | 1,875,000 | | | | 10.0 | % |
| Marina Towers Holdings, LLC (6) (9) | | | 1,800,000 | | | | 10.7 | % |
| Donald A. Bittar (7) (9) | | | 696,666 | | | | 4.1 | % |
| Colin Halpern (9) | | | 75,000 | | | | * | |
| All Executive Officers and Directors as a Group (3 Individuals) | | | 8,381,666 | | | | 44.9 | % |
| Hillair Capital Investments L.P. (8)(10) | | | 2,320,000 | | | | 12.1 | % |
(1) Except as otherwise indicated, we believe that the beneficial owners of the common stock listed above, based on information furnished by such owners, have sole investment and voting power with respect to such shares, subject to community property laws where applicable. Beneficial ownership is determined in accordance with the rules of the SEC and generally includes voting or investment power with respect to securities. Shares of common stock subject to options or warrants currently exercisable, or exercisable within 60 days, are deemed outstanding for purposes of computing the percentage ownership of the person holding such option or warrants, but are not deemed outstanding for purposes of computing the percentage ownership of any other person.
(2) Based on 16,793,248 shares of common stock issued and outstanding as of March 27, 2014.
(3) Mr. Romandetti’s beneficial ownership is primarily through GIRTFT LLC and Marina Towers Holdings, LLC.
(4) GIRTFT LLC is a limited liability company for which Mr. Romandetti is the Managing Member.
(5) Comprised of a warrant to purchase 1,875,000 shares of Common Stock that may be exercised on or prior to the close of business on December 31, 2016 at an exercise price of $3.60 per share
(6) Marina Towers Holdings, LLC is a limited liability company for which Mr. Romandetti is the Managing Member.
(7) Includes 360,000 shares of Common Stock owned by Mr. Bittar’s wife.
(8) Comprised of a warrant to purchase 2,320,000 shares of Common Stock that may be exercised on or prior to the close of business on November 8, 2018 at an exercise price of $1.35 per share.
(9) c/o 709 S. Harbor City Blvd., Suite 250, Melbourne, FL 32901.
(10) 330 Primrose Road, Suite 660, Burlingame, CA 94010. Hillair Capital Management LLC serves as the investment manager of Hillair Capital Investments LP and, as such, Hillair Capital Management LLC has the voting and dispositive power with respect to the securities held by Hillair Capital Investments LP. As manager of Hillair Capital Management LLC, each of Sean McAvoy, Scott Kaufman and Neal Kaufman also shares voting and investment power on behalf of Hillair Capital Investments LP.
Equity Compensation Plans
The following table sets forth information as of December 31, 2013 with respect to compensation plans under which we are authorized to issue shares of our common stock, aggregated as follows:
| · | All compensation plans previously approved by security holders; and |
| · | All compensation plans not previously approved by security holders. |
| | | Equity Compensation Plan Information | |
| Plan Category | | Number of securities
to be issued upon
exercise of
outstanding options,
warrants and rights | | | Weighted-average
exercise price of
outstanding options,
warrants and rights | | | Number of securities
remaining available for
future issuance under
equity compensation plans | |
| | | (a) | | | (b) | | | (c) | |
| Equity compensation plans approved by security holders | | | 0 | | | $ | 0.00 | | | | 500,000 | |
| | | | | | | | | | | | | |
| Equity compensation plans not approved by security holders | | | 0 | | | $ | 0.00 | | | | 0 | |
| | | | | | | | | | | | | |
| Total | | | 0 | | | $ | 0.00 | | | | 500,000 | |
On March 14, 2012, we adopted our2011 Incentive Stock Plan (the “2011 Plan”), pursuant to which 500,000 shares of our common stock are reserved for issuance as awards to employees, directors, officers, consultants, and other service providers of the Company and its subsidiaries (an “Optionee”). The term of the 2011 Plan is ten years from January 6, 2012, its effective date. No grants have been made to date under the 2011 Plan.
Terms and Conditions of Options Pursuant to the 2011 Incentive Stock Plan
Options granted under the Plan shall be subject to the following conditions and shall contain such additional terms and conditions, not inconsistent with the terms of the Plan, as the Plan committee shall deem desirable:
| · | Option Price. The purchase price of each share of Stock purchasable under an incentive option shall be determined by the Plan committee at the time of grant, but shall not be less than 100% of the Fair Market Value (as defined below) of such share of Stock on the date the option is granted; provided , however , that with respect to an Optionee who, at the time such incentive option is granted, owns (within the meaning of Section 424(d) of the United States Internal Revenue Code of 1986 (the “Code)) more than 10% of the total combined voting power of all classes of stock of the Company or of any subsidiary, the purchase price per share of Stock shall be at least 110% of the Fair Market Value per share of Stock on the date of grant. The purchase price of each share of Stock purchasable under a nonqualified option shall not be less than 100% of the Fair Market Value of such share of Stock on the date the option is granted. The exercise price for each option shall be subject to adjustment as provided in the Plan. “Fair Market Value” means the fair market value of the Company’s issued and outstanding Stock as determined in good faith by the Plan committee. In no event shall the purchase price of a share of Stock be less than the minimum price permitted under the rules and policies of any national securities exchange on which the shares of Stock are listed. |
| · | Option Term. The term of each option shall be fixed by the Plan committee, but no option shall be exercisable more than ten years after the date such option is granted and in the case of an Incentive Option granted to an Optionee who, at the time such incentive option is granted, owns (within the meaning of Section 424(d) of the Code) more than 10% of the total combined voting power of all classes of stock of the Company or of any subsidiary, no such incentive option shall be exercisable more than five years after the date such incentive option is granted. |
| · | Exercisability. Options shall be exercisable at such time or times and subject to such terms and conditions as shall be determined by the Plan committee at the time of grant;provided ,however , that in the absence of any option vesting periods designated by the Plan committee at the time of grant, options shall vest and become exercisable as to one-tenth of the total number of shares subject to the option on each of the three month anniversary of the date of grant; and provided further that no options shall be exercisable until such time as any vesting limitation required by Section 16 of the Exchange Act, and related rules, shall be satisfied if such limitation shall be required for continued validity of the exemption provided under Rule 16b-3(d)(3). |
Upon the occurrence of a “Change in Control” (as hereinafter defined), the Plan committee may accelerate the vesting and exercisability of outstanding options, in whole or in part, as determined by the Plan committee in its sole discretion. In its sole discretion, the Plan committee may also determine that, upon the occurrence of a Change in Control, each outstanding option shall terminate within a specified number of days after notice to an Optionee thereunder, and each such Optionee shall receive, with respect to each share of Company Stock subject to such option, an amount equal to the excess of the Fair Market Value of such shares immediately prior to such Change in Control over the exercise price per share of such option; such amount shall be payable in cash, in one or more kinds of property (including the property, if any, payable in the transaction) or a combination thereof, as the Plan committee shall determine in its sole discretion.
For purposes of the Plan, unless otherwise defined in an employment or consulting agreement between the Company and the relevant Optionee, a Change in Control shall be deemed to have occurred if:
| · | a tender offer (or series of related offers) shall be made and consummated for the ownership of 50% or more of the outstanding voting securities of the Company, unless as a result of such tender offer more than 50% of the outstanding voting securities of the surviving or resulting corporation shall be owned in the aggregate by the stockholders of the Company (as of the time immediately prior to the commencement of such offer), any employee benefit plan of the Company or its subsidiaries, and their affiliates; |
| · | the Company shall be merged or consolidated with another corporation, unless as a result of such merger or consolidation more than 50% of the outstanding voting securities of the surviving or resulting corporation shall be owned in the aggregate by the stockholders of the Company (as of the time immediately prior to such transaction), any employee benefit plan of the Company or its subsidiaries, and their affiliates; |
| · | the Company shall sell substantially all of its assets to another corporation that is not wholly owned by the Company, unless as a result of such sale more than 50% of such assets shall be owned in the aggregate by the stockholders of the Company (as of the time immediately prior to such transaction), any employee benefit plan of the Company or its subsidiaries and their affiliates; or |
| · | a Person (as defined below) shall acquire 50% or more of the outstanding voting securities of the Company (whether directly, indirectly, beneficially or of record), unless as a result of such acquisition more than 50% of the outstanding voting securities of the surviving or resulting corporation shall be owned in the aggregate by the stockholders of the Company (as of the time immediately prior to the first acquisition of such securities by such Person), any employee benefit plan of the Company or its subsidiaries, and their affiliates. |
Notwithstanding the foregoing, if Change of Control is defined in an employment or consulting agreement between the Company and the relevant Optionee, then, with respect to such Optionee, Change of Control shall have the meaning ascribed to it in such employment agreement.
Ownership of voting securities shall take into account and shall include ownership as determined by applying the provisions of Rule 13d-3(d)(I)(i) (as in effect on the date hereof) under the Exchange Act. In addition, for such purposes, “Person” shall have the meaning given in Section 3(a)(9) of the Exchange Act, as modified and used in Sections 13(d) and 14(d) thereof; provided , however , that a Person shall not include (A) the Company or any of its subsidiaries; (B) a trustee or other fiduciary holding securities under an employee benefit plan of the Company or any of its subsidiaries; (C) an underwriter temporarily holding securities pursuant to an offering of such securities; or (D) a corporation owned, directly or indirectly, by the stockholders of the Company in substantially the same proportion as their ownership of stock of the Company.
Description of Securities
First Choice Healthcare Solutions has 100,000,000 Common Stock, par value $0.001 per share, authorized for issuance and 1,000,000 Preferred Stock, par value $0.10 per share, authorized for issuance. As of March 14, 2014, there were 16,793,248 shares of Common Stock issued and outstanding. There were zero (0) shares of Preferred Stock that are issued and outstanding.
Item 13. Certain Relationships and Related Transactions; and Director Independence
Guggenheim Life and Annuity Company
On August 12, 2011 Marina Towers, LLC, a Florida limited liability company (“Marina Towers”) an indirect and wholly-owned subsidiary of Medical Billing Assistance, Inc., a Colorado company (the “Company”) entered into a Loan Agreement (the “Loan Agreement”) with Guggenheim Life and Annuity Company, a Delaware life insurance company (“Guggenheim”). The closing and funding of the Loan occurred on August 15, 2011 (the "Closing Date"). Under the Loan Agreement, Guggenheim has committed to make a loan in the aggregate amount of $7,550,000.00 to Marina Towers with an interest rate of 6.10% per annum (the “Loan”). The maturity date of the Loan is September 16, 2016 (the “Maturity Date”). The Loan is evidenced by that certain Consolidated, Amended and Restated Promissory Note, dated August 12, 2011 (the “Note”) and is secured primarily by: (i) that certain first priority Consolidated, Amended and Restated Mortgage and Security Agreement, dated August 12, 2011, encumbering the real and personal property (the “Property”) of Marina Towers (the “Mortgage”); and (ii) that certain first priority Assignment of Leases and Rents, dated August 12, 2011, from Marina Towers, as assignor, to Guggenheim as assignee, pursuant to which Marina Towers assigned to Guggenheim all of Marina Towers’ right, title and interest in and to certain leases and rents as security for the Loan.
The proceeds of the Loan were used to: (i) repay and discharge existing loans relating to the Property; (ii) pay all past-due basic carrying costs, if any, with respect to the Property; (iii) make deposits into the reserve funds, or any escrow accounts established pursuant to the loan documents, on the Closing Date in the amounts set forth in the Loan Agreement; (iv) pay costs and expenses incurred in connection with the closing of the Loan; (v) fund any working capital requirements of the Property; and (vi) distribute the balance, if any, to Marina Towers.
Pursuant to the Loan Agreement, Marina Towers does not have the right to prepay the Loan, in whole or in part, prior to the Maturity Date. After the payment date occurring three months prior to the Maturity Date, Marina Towers may, provided no event of default has occurred and is continuing, at its option and upon thirty days’ prior notice to Guggenheim, prepay the Loan in whole on any date without payment of any prepayment penalty or premiums.
The Loan Agreement is guaranteed by Christian C. Romandetti, the Company’s Chief Executive Officer, pursuant to that certain Guaranty Agreement, dated August 12, 2011, made by Mr. Romandetti for the benefit of Guggenheim (the “Guaranty”). Pursuant to the non-recourse Guaranty, Mr. Romandetti agreed to a limited personal guarantee to Guggenheim of the payments and performance of the obligations of and liabilities of Marina Towers pursuant to the Loan Agreement.
On February 1, 2012, the Company opened a $500,000 unsecured, revolving line of credit loan with CCR of Melbourne, Inc., an entity jointly owned and controlled at that time by Christian “Chris” Romandetti, the Company's Chief Executive Officer and Carmen Charles Romandetti, our CEO’s father. The revolving line of credit loan was to mature on October 1, 2015 with interest at a per annum rate of 8.5% beginning March 1, 2012. Advances on the line of credit were at the sole discretion of CCR of Melbourne, Inc. On November 8, 2013, CCR converted the then outstanding balance of $142,483.52, representing all of the outstanding related party principal and interest amount on the loan, into shares of the Company’s common stock at a price equal to $0.45 per share for a total of 316,631 shares issued. On November 8, 2013, Chris Romandetti relinquished all rights, title to and ownership in CCR to Carmen Romandetti in consideration of a personal loan made to Chris Romandetti by Carmen Romandetti.
The Company entered into an unsecured loan agreement with HS Real Company, LLC (“HSR”) on May 17, 2012 for $100,000 at an interest rate of 12% per annum (the "HSR Note"). On August 5, 2012, HSR increased the principal amount to $250,000, and subsequently HSR advanced an additional $50,000 to the Company, bringing the aggregate principal amount of the HSR Note to $300,000, all of which was due and payable to HSR on December 31, 2012. The Company paid $27,556 and $17,053 as interest on the HSR note for the years ended December 31, 2013 and 2012, respectively. Mr. Colin Halpern is both an affiliate of HSR and a member of the Company’s Board of Directors. On November 8, 2013, the Company paid off the HSR Note, remitting HSR $300,000 for the outstanding principal and interest balance due on the HSR Note.
On September 7, 2013, the Company acquired a patent, US 7,789,842 B2, for an orthopedic adjustable arm sling from Donald A. Bittar, the inventor and the Company’s Chief Financial Officer. Based on the independent, third party evaluation of Professional Business Brokers, Inc., the patent was valued at $286,500. The Company issued Mr. Bittar 636,666 shares of its common stock, valued at $286,500, or $0.45 per share, which was estimated to approximate fair value of the patent acquired and did not materially differ from the fair value of the common stock at the time of issuance.
Director Independence
Currently, none of our directors qualify as independent directors under the NASDAQ listing standards and Rule 10A-3 and Rule 10C-1 of the Exchange Act.
Item 14. Principal Accountant Fees and Services
Audit Fees
Our independent auditor, RBSM LLP, billed an aggregate of $48,000 for the year ended December 31, 2013 audit and the quarterly reviews for the year ended December 31, 2013. RBSM LLP billed $30,137 for the December 31, 2012 audit, quarterly reviews for the year ended December 31, 2012 and audit related fees. In addition, $6,000 and $6,500 were billed for tax services in 2013 and 2012, respectively. Audit Fees and Audit Related Fees consist of fees billed for professional services rendered for auditing our Financial Statements, reviews of interim Financial Statements included in quarterly reports, services performed in connection with other filings with the Securities & Exchange Commission and related comfort letters and other services that are normally provided by our independent auditors in connection with statutory and regulatory filings or engagements. Tax Fees consists of fees billed for professional services for tax compliance, tax advice and tax planning. These services include assistance regarding federal, state and local tax compliance and consultation in connection with various transactions and acquisitions.
| | | 2013 | | | 2012 | |
| Audit Fees | | $ | 48,000 | | | $ | 29,000 | |
| Audit-Related Fees | | | - | | | | 1,137 | |
| Tax Fees | | | 6,000 | | | | 6,500 | |
| All Other Fees | | | - | | | | - | |
| Total | | $ | 54,000 | | | $ | 36,637 | |
PART IV
Item 15. Exhibits, Financial Statement Schedules
| Exhibit No. | | Description | |
| | | | |
| 3.1 | | Articles of Incorporation of Medical Billing Assistance, Inc. (the “Company”) (incorporated by reference to the Company’s Form SB-2 Registration Statement as filed December 20, 2007) | |
| 3.1(a) | | Certificate of Incorporation of First Choice Healthcare Solutions, Inc. (incorporated by reference to Annex B to the Company’s Information Statement on Schedule 14C, filed with the SEC on March 14, 2012) | |
3.1(b) | | Certificate of Merger between First Choice Healthcare Solutions,Inc., a Delaware and surviving corporation and Medical Billing Assistance, Inc., a Colorado corporation. (incorporated by reference to Exhibit 3.1(B) to the Company’s Current Report on Form 8-K, filed with the SEC on April 9, 2012) | |
| 3.2 | | By-laws of the Company (incorporated by reference to the Company’s Form SB-2 Registration Statement as filed December 20, 2007) | |
| 3.2(a) | | By-laws of First Choice Healthcare Solutions, Inc. (incorporated by reference to Annex C to the Company’s Information Statement on Schedule 14C, filed with the SEC on March 14, 2012) | |
| 4.1 | | Medical Billing Assistance, Inc. 2011 Incentive Stock Plan (incorporated by reference to Annex E to the Company’s Information Statement on Schedule 14C, filed with the SEC on March 14, 2012) | |
| 10.1 | | Share Exchange Agreement, dated December 29, 2010, by and between the Company, FCID Medical, Inc., and FCID Holdings, Inc. (incorporated by reference to the Company’s Current Report on Form 8-K filed with the SEC on January 3, 2011) |
| | | |
| 10.5 | | Loan Agreement, dated as of August 12, 2011, between Marina Towers, LLC (“Marina”) and Guggenheim Life and Annuity Company (“Guggenheim”) (incorporated by reference to Exhibit 10.1 to the Company’s Current Report on Form 8-K, filed with the SEC on August 22, 2011) |
| | | |
| 10.6 | | Florida Consolidated, Amended and Restated Promissory Note, dated August 12, 2011, made by Marina to Guggenheim (incorporated by reference to Exhibit 10.2 to the Company’s Current Report on Form 8-K, filed with the SEC on August 22, 2011) |
| | | |
| 10.7 | | Guaranty Agreement, dated as of August 12, 2011, made by Christian C. Romandetti for the benefit of Guggenheim (incorporated by reference to Exhibit 10.3 to the Company’s Current Report on Form 8-K, filed with the SEC on August 22, 2011) |
| | | |
| 10.8 | | Common Stock Warrant, issued December 23, 2011, to MedTrx Provider Network, LLC (incorporated by reference to Exhibit 10.1 to the Company’s Current Report on Form 8-K, filed with the SEC on February 13, 2012) |
| | | |
| 10.9 | | Registration Rights Agreement (incorporated by reference to Exhibit 10.2 to the Company’s Current Report on Form 8-K, filed with the SEC on February 13, 2012) |
| | | |
| 10.10 | | Agreement and Plan of Merger, made as of February 13, 2012, by and between the Company and First Choice Healthcare Solutions, Inc. (incorporated by reference to Appendix A to the Company’s Information Statement on Schedule 14C, filed with the SEC on March 14, 2012) |
| | | |
| 10.11 | | Membership Interest Purchase Closing Agreement between Seller, FCID Medical, Inc. and First Choice Medical Group of Brevard, LLC (incorporated by reference to Exhibit 10.1 to the Company’s Current Report on Form 8-K, filed with the SEC on April 9, 2012) |
| | | |
| 10.12 | | Management Services Agreement between FCID Medical, Inc. and First Choice Medical Group of Brevard, LLC (incorporated by reference to Exhibit 10.2 to the Company’s Current Report on Form 8-K, filed with the SEC on April 9, 2012) |
| | 10.13 | Loan Agreement, dated February 1, 2012, between FCID of Medical, Inc. and CCR of Melbourne, Inc. (incorporated by reference to Exhibit 10.11 to the Company’s Quarterly Report on Form 10-Q, filed with the SEC on May 15, 2012) |
| | | |
| | 10.14 | Revolving Line of Credit Promissory Note, dated February 15, 2012, in the amount of $500,000, issued by FCID Medical, Inc. to CCR of Melbourne, Inc. (incorporated by reference to Exhibit 10.12 to the Company’s Quarterly Report on Form 10-Q, filed with the SEC on May 15, 2012) |
| | | | |
| | 10.15 | Promissory Note, dated as of May 18, 2012, made by First Choice Medical Group of Brevard, LLC to the order of General Electric Capital Corporation, in the amount of $450,000 (incorporated by reference to Exhibit 10.14 to the Company’s Current Report on Form 8-K, filed with the SEC on May 25, 2012) |
| | | | |
| | 10.16 | Master Lease Agreement, dated as of May 10, 2012, between First Choice Medical Group of Brevard, LLC and General Electric Capital Corporation, with schedules (incorporated by reference to Exhibit 10.15 to the Company’s Current Report on Form 8-K, filed with the SEC on May 25, 2012) |
| | | |
| | 10.16(a) | Guaranty, dated May 10, 2012, by Christian Romandetti to General Electric Capital Corporation (incorporated by reference to Exhibit 10.16 to the Company’s Current Report on Form 8-K, filed with the SEC on May 25, 2012) |
| | | |
| | 10.16(b) | Guaranty, dated May 10, 2012, by First Choice Healthcare Solutions, Inc. to General Electric Capital Corporation (incorporated by reference to Exhibit 10.17 to the Company’s Current Report on Form 8-K, filed with the SEC on May 25, 2012) | |
| | | | |
| | 10.17 | Securities Purchase Agreement, made as of December 14, 2012, with note as an exhibit thereto, for the sale of an 8% convertible note in the principal amount of $203,500 + |
| | | | |
| | 10.18 | Securities Purchase Agreement, made as of February 19, 2013, with note as an exhibit thereto, for the sale of an 8% convertible note in the principal amount of $103,500 + |
| | | | |
| | 10.19 | Securities Purchase Agreement, made as of August 14, 2013, for the sale of an 8% convertible note in the principal amount of $153,500, with note as an exhibit thereto. + |
| | | | |
| | 10.20 | Agreement, dated as of May 1, 2013, between MTI Capital LLC and First Choice Healthcare Solutions, Inc.+ |
| | | | |
| | 10.21 | Loan and Security Agreement, dated as of June 13, 2013, by and between CT Capital Ltd and First Choice Medical Group of Brevard, LLC + |
| | | |
| | 10.21(a) | Agreement to Modify Loan Interest Rate and Consent to FCHS Secured Debt Issuance, dated June 13, 2013, by and between CT Capital Ltd and First Choice Medical Group of Brevard, LLc. + |
| | | | |
| | 10.22 | Form of Membership Interest Purchase Agreement, dated August 28, 2013, by and between the Company and the sellers of the membership interests in MedTech Diagnostics LLC + |
| | | | |
| | 10.23 | License Agreement, dater August 28, 2013, by and between Donald Bittar and First Choice Healthcare Solutions, Inc.+ |
| | | | |
| | 10.24 | Amendment to Loan Agreement, dated as of August 28, 2013, by and among MTI Capital LLC and First Choice Healthcare Solutions, Inc.+ |
| | | |
| | 10.25 | Form of Securities Purchase Agreement, dated as of November 8, 2013, between the Company and Hillair Capital Investments, L.P. (incorporated by reference to Exhibit 10.1 to the Company’s Current Report on Form 8-K, filed with the SEC on November 14, 2013) |
| | | | |
| | 10.26 | Form of Common Stock Purchase Warrant, dated as of November 8, 2013, issued to Hillair Capital Investments, L.P (incorporated by reference to Exhibit 4.2 to the Company’s Current Report on Form 8-K, filed with the SEC on November 14, 2013) |
| | 10.27 | Form of Debenture, dated as of November 8, 2013 issued to Hillair Capital Investments, L.P (incorporated by reference to Exhibit 4.1 to the Company’s Current Report on Form 8-K, filed with the SEC on November 14, 2013) |
| | | | |
| | 10.28 | Form of Security Agreement, dated as of November 8, 2013 between Hillair Capital Investments, L.P., the Company and certain of its subsidiaries (incorporated by reference to Exhibit 10.2 to the Company’s Current Report on Form 8-K, filed with the SEC on November 14, 2013) |
| | | |
| | 10.28(a) | Form of Subsidiary Guarantee, dated as of November 8, 2013, to the Securities Purchase Agreement, dated as of November 8, 2013, between the Company and Hillair Capital Investments, L.P. (incorporated by reference to Exhibit 10.3 to the Company’s Current Report on Form 8-K, filed with the SEC on November 14, 2013) |
| | | |
| | 10.29 | Loan Agreement, dated May 17, 2012 between HS Real Company, LLC and First Choice Medical Group of Brevard, LLC |
| | | |
| | 10.29(a) | Promissory Note, dated May 17, 2012, to HS Real Company, LLC |
| | | |
| | 10.29(b) | Amendment to Loan Agreement dated August 5, 2012, with HS REal Company LLC, and First Choice Medical Group of Brevard, LLC |
| | | | |
| | 10.30 | Employment Agreement, dated March 20, 2014, between the Company and Christian Charles Romandetti + |
| | | | |
| | 14 | Code of Ethics, (incorporated by reference to Exhibit 14 to the Company’s Annual Report on Form 10-K, filed with the SEC on March 30, 2012) |
| | | | |
| | 21.1 | List of Subsidiaries + | |
| | | | | | |
| 31.1 | | Certification of CEO pursuant to Sec. 302+ |
| 31.2 | | Certification of CFO pursuant to Sec. 302+ |
| 32.1 | | Certification of CEO pursuant to Sec. 906+ |
| 32.2 | | Certification of CFO pursuant to Sec. 906+ |
| | | |
| EX-101.INS | | XBRL INSTANCE DOCUMENT+ |
| EX-101.SCH | | XBRL TAXONOMY EXTENSION SCHEMA DOCUMENT+ |
| EX-101.CAL | | XBRL TAXONOMY EXTENSION CALCULATION LINKBASE+ |
| EX-101.DEF | | XBRL TAXONOMY EXTENSION DEFINITION LINKBASE+ |
| EX-101.LAB | | XBRL TAXONOMY EXTENSION LABELS LINKBASE+ |
| EX-101.PRE | | XBRL TAXONOMY EXTENSION PRESENTATION LINKBASE+ |
+filed herewith
SIGNATURES
In accordance with Section 13 or 15(d) of the Exchange Act, the registrant caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| | FIRST CHOICE HEALTHCARE SOLUTIONS, INC. |
| | | |
| Dated: March 31, 2014 | By: | /s/ Christian Charles Romandetti |
| | | Christian Charles Romandetti |
| | | President and Chief Executive Officer |
| | | |
| Dated: March 31, 2014 | By: | /s/ Donald A. Bittar |
| | | Donald A. Bittar |
| | | Chief Financial Officer, Secretary and Treasurer |
INDEX TO FINANCIAL STATEMENTS
| CONTENTS | | PAGE NO. |
| | | |
| Reports of Independent Registered Public Accounting Firm | | F-2 |
| | | |
| Consolidated Balance Sheets at December 31, 2013 and 2012 | | F-3 |
| | | |
| Consolidated Statements of Operations for the Years Ended December 31, 2013 and 2012 | | F-4 |
| | | |
| Consolidated Statement of Stockholders’ Deficit for the Two Years Ended December 31, 2013 and 2012 | | F-5 |
| | | |
| Consolidated Statements of Cash Flows for the Years Ended December 31, 2013 and 2012 | | F-6 |
| | | |
| Notes to the Consolidated Financial Statements | | F-7 |
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
Board of Directors and Shareholders
First Choice Healthcare Solutions, Inc.
Melbourne, Florida
We have audited the accompanying balance sheets of First Choice Healthcare Solutions, Inc. (the “Company”), as of December 31, 2013 and 2012, and the related statements of operations, stockholders’ deficit and cash flows for each of the two years in the period ended December 31, 2013. These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements based on our audits.
We have conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States of America). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. Our audits included consideration of internal control over financial reporting as a basis for designing audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion. An audit also includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the financial statements referred to above present fairly, in all material respects, the financial position of First Choice Healthcare Solutions, Inc. as of December 31, 2013 and 2012, and the results of its operations and its cash flows for each of the two years in the period ended December 31, 2013, in conformity with accounting principles generally accepted in the United States of America.
/s/ RBSM LLP
New York, New York
March 28, 2014
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
CONSOLIDATED BALANCE SHEETS
DECEMBER 31, 2013 AND 2012
| | | 2013 | | | 2012 | |
| ASSETS | | | | | | | | |
| Current assets | | | | | | | | |
| Cash | | $ | 739,158 | | | $ | 67,045 | |
| Cash-restricted | | | 256,246 | | | | 221,148 | |
| Accounts receivable | | | 1,272,155 | | | | 527,867 | |
| Prepaid and other current assets | | | 140,580 | | | | 69,970 | |
| Capitalized financing costs, current portion | | | 57,348 | | | | 57,348 | |
| Total current assets | | | 2,465,487 | | | | 943,378 | |
| | | | | | | | | |
| Property, plant and equipment, net of accumulated depreciation of $1,959,127 and $1,465,939 | | | 8,662,057 | | | | 8,756,631 | |
| | | | | | | | | |
| Other assets | | | | | | | | |
| Capitalized financing costs, long term portion | | | 131,540 | | | | 152,911 | |
| Patient list, net of accumulated amortization of $35,000 and $24,391 | | | 265,000 | | | | 275,609 | |
| Patents | | | 286,500 | | | | - | |
| Deposits | | | 2,713 | | | | 2,719 | |
| Total other assets | | | 685,753 | | | | 431,239 | |
| Total assets | | $ | 11,813,297 | | | $ | 10,131,248 | |
| | | | | | | | | |
| LIABILITIES AND STOCKHOLDERS' DEFICIT | | | | | | | | |
| Current liabilities | | | | | | | | |
| Accounts payable and accrued expenses | | $ | 459,000 | | | $ | 576,209 | |
| Stock based payable | | | 166,340 | | | | - | |
| Line of credit, short term | | | 800,000 | | | | - | |
| Notes payable, current portion | | | 743,787 | | | | 690,586 | |
| Note payable, related party | | | - | | | | 300,000 | |
| Convertible note payable, net of unamortized debt discount of $160,543 | | | - | | | | 43,537 | |
| Unearned revenue | | | 74,934 | | | | 39,438 | |
| Total current liabilities | | | 2,244,061 | | | | 1,649,770 | |
| | | | | | | | | |
| Long term debt: | | | | | | | | |
| Deposits held | | | 72,901 | | | | 47,399 | |
| Revolving line of credit, related party | | | - | | | | 153,330 | |
| Convertible note payable, long term portion | | | 2,347,403 | | | | - | |
| Notes payable, long term portion | | | 8,935,473 | | | | 9,410,296 | |
| Derivative liability | | | - | | | | 171,987 | |
| Total long term debt | | | 11,355,777 | | | | 9,783,012 | |
| Total liabilities | | | 13,599,838 | | | | 11,432,782 | |
| Stockholders' deficit | | | | | | | | |
| Preferred stock, $0.01 par value; 1,000,000 shares authorized, Nil issued and outstanding | | | - | | | | - | |
| Common stock, $0.001 par value; 100,000,000 shares authorized, 16,747,248 and 12,706,795 shares issued and outstanding as of December 31, 2013 and 2012, respectively | | | 16,747 | | | | 12,707 | |
| Additional paid in capital | | | 11,560,249 | | | | 7,244,993 | |
| Common stock subscriptions | | | - | | | | 100,000 | |
| Accumulated deficit | | | (13,363,537 | ) | | | (8,659,234 | ) |
| Total stockholders' deficit | | | (1,786,541 | ) | | | (1,301,534 | ) |
| Total liabilities and stockholders' deficit | | $ | 11,813,297 | | | $ | 10,131,248 | |
See the accompanying notes to these consolidated financial statements
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
CONSOLIDATED STATEMENTS OF OPERATIONS
| | | Year ended December 31, | |
| | | 2013 | | | 2012 | |
| Revenues: | | | | | | | | |
| Net patient service revenue | | $ | 5,459,373 | | | $ | 2,645,310 | |
| Rental revenue | | | 1,048,469 | | | | 1,160,037 | |
| Total revenue | | | 6,507,842 | | | | 3,805,347 | |
| | | | | | | | | |
| Operating expenses: | | | | | | | | |
| Salaries and benefits | | | 3,096,285 | | | | 1,593,245 | |
| Other operating expenses | | | 1,715,942 | | | | 865,641 | |
| General and administrative | | | 1,705,154 | | | | 1,314,302 | |
| Impairment of investment | | | 450,000 | | | | - | |
| Depreciation and amortization | | | 518,611 | | | | 309,899 | |
| Total operating expenses | | | 7,485,992 | | | | 4,083,087 | |
| | | | | | | | | |
| Net income (loss) from operations | | | (978,150 | ) | | | (277,740 | ) |
| | | | | | | | | |
| Other income (expense): | | | | | | | | |
| Miscellaneous income | | | 3,063 | | | | 3,000 | |
| Gain (loss) on change in fair value of derivative liability | | | 32,218 | | | | (987 | ) |
| Amortization financing costs | | | (57,348 | ) | | | (57,348 | ) |
| Interest expense, net | | | (3,704,086 | ) | | | (563,391 | ) |
| Total other (expense) | | | (3,726,153 | ) | | | (618,726 | ) |
| | | | | | | | | |
| Net loss before provision for income taxes | | | (4,704,303 | ) | | | (896,466 | ) |
| | | | | | | | | |
| Income taxes (benefit) | | | - | | | | (23,103 | ) |
| | | | | | | | | |
| Net loss | | $ | (4,704,303 | ) | | $ | (873,363 | ) |
| | | | | | | | | |
| Net loss per common share, basic and diluted | | $ | (0.35 | ) | | $ | (0.07 | ) |
| | | | | | | | | |
| Weighted average number of common shares outstanding, basic and diluted | | | 13,529,294 | | | | 12,644,784 | |
See the accompanying notes to these consolidated financial statements
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
CONSOLIDATED STATEMENT OF STOCKHOLDERS' DEFICIT
TWO YEARS ENDED DECEMBER 31, 2013
| | | | | | | | | | | | | | | Additional | | | Common | | | | | | | |
| | | Preferred stock | | | Common stock | | | Paid in | | | Stock | | | Accumulated | | | | |
| | | Shares | | | Amount | | | Shares | | | Amount | | | Capital | | | Subscriptions | | | Deficit | | | Total | |
| Balance, December 31, 2011 | | | - | | | $ | - | | | | 12,462,750 | | | $ | 12,463 | | | $ | 6,747,512 | | | $ | - | | | $ | (7,785,871 | ) | | $ | (1,025,896 | ) |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| Common stock issued to acquire First Choice Medical Group, Inc., net of fair value of 70,529 shares of common stock to be returned from post-acquisition adjustments | | | - | | | | - | | | | 244,045 | | | | 244 | | | | 497,481 | | | | | | | | - | | | | 497,725 | |
| Common stock subscriptions received | | | - | | | | - | | | | - | | | | - | | | | - | | | | 100,000 | | | | - | | | | 100,000 | |
| Net loss | | | - | | | | - | | | | - | | | | - | | | | - | | | | - | | | | (873,363 | ) | | | (873,363 | ) |
| Balance, December 31, 2012 | | | - | | | $ | - | | | | 12,706,795 | | | $ | 12,707 | | | $ | 7,244,993 | | | $ | 100,000 | | | $ | (8,659,234 | ) | | $ | (1,301,534 | ) |
| Common stock issued for services rendered | | | - | | | | - | | | | 533,822 | | | | 534 | | | | 382,567 | | | | - | | | | - | | | | 383,101 | |
| Common stock issued in settlement of line of credit | | | - | | | | - | | | | 1,386,667 | | | | 1,386 | | | | 622,614 | | | | - | | | | - | | | | 624,000 | |
| Common stock issued in settlement of related party line of credit | | | - | | | | - | | | | 316,631 | | | | 317 | | | | 142,167 | | | | - | | | | - | | | | 142,484 | |
| Common stock issued in connection with loan modification | | | - | | | | - | | | | 100,000 | | | | 100 | | | | 95,900 | | | | - | | | | - | | | | 96,000 | |
| Common stock issued for subscription | | | - | | | | - | | | | 66,666 | | | | 66 | | | | 99,934 | | | | (100,000 | ) | | | - | | | | - | |
| Common stock issued to acquire 10% in MedTech Diagnostics, LLC | | | - | | | | - | | | | 1,000,000 | | | | 1,000 | | | | 449,000 | | | | - | | | | - | | | | 450,000 | |
| Common stock issued to acquire patent rights | | | - | | | | - | | | | 636,666 | | | | 637 | | | | 285,863 | | | | - | | | | - | | | | 286,500 | |
| Reclassification of derivative liability to equity upon convertible note payoff | | | - | | | | - | | | | - | | | | - | | | | 366,094 | | | | - | | | | - | | | | 366,094 | |
| Beneficial conversion feature in connection with note payable | | | - | | | | - | | | | - | | | | - | | | | 1,871,117 | | | | - | | | | - | | | | 1,871,117 | |
| Net loss | | | - | | | | - | | | | - | | | | - | | | | - | | | | - | | | | (4,704,303 | ) | | | (4,704,303 | ) |
| Balance, December 31, 2013 | | | - | | | $ | - | | | | 16,747,247 | | | $ | 16,747 | | | $ | 11,560,249 | | | $ | - | | | $ | (13,363,537 | ) | | $ | (1,786,541 | ) |
See the accompanying notes to these consolidated financial statements
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
CONSOLIDATED STATEMENTS OF CASH FLOWS
| | | Year ended December 31, | |
| | | 2013 | | | 2012 | |
| CASH FLOWS FROM OPERATING ACTIVITIES: | | | | | | | | |
| Net Loss | | $ | (4,704,303 | ) | | $ | (873,363 | ) |
| Adjustments to reconcile net loss to cash used in operating activities: | | | | | | | | |
| Depreciation | | | 518,611 | | | | 309,899 | |
| Amortization of financing costs | | | 57,348 | | | | 57,348 | |
| Bad debt expense | | | 361,284 | | | | - | |
| Amortization of debt discount in connection with convertible note | | | 2,706,869 | | | | 10,457 | |
| Stock based compensation | | | 549,441 | | | | - | |
| Common stock issued for loan modification | | | 96,000 | | | | - | |
| Impairment of investment | | | 450,000 | | | | - | |
| Loss on change in fair value of debt derivative | | | (32,218 | ) | | | 987 | |
| Changes in operating assets and liabilities: | | | | | | | | |
| Accounts receivable | | | (1,105,572 | ) | | | (329,375 | ) |
| Accounts receivable-other | | | - | | | | (205,000 | ) |
| Prepaid expenses and other | | | (70,604 | ) | | | (40,265 | ) |
| Restricted funds | | | (35,098 | ) | | | (131,209 | ) |
| Accounts payable and accrued expenses | | | (91,312 | ) | | | 419,417 | |
| Unearned income | | | 35,496 | | | | 15,354 | |
| Deferred income taxes | | | - | | | | (23,103 | ) |
| Net cash provided by operating activities | | | (1,264,058 | ) | | | (788,853 | ) |
| | | | | | | | | |
| CASH FLOWS FROM INVESTING ACTIVITIES: | | | | | | | | |
| Cash received from acquisition | | | - | | | | 48,761 | |
| Cash payments for acquisition | | | - | | | | (143,366 | ) |
| Purchase of equipment | | | (397,688 | ) | | | (2,773,450 | ) |
| Net increase in deposits | | | 25,502 | | | | 15,796 | |
| Net cash used in investing activities | | | (372,186 | ) | | | (2,852,259 | ) |
| | | | | | | | | |
| CASH FLOWS FROM FINANCING ACTIVITIES: | | | | | | | | |
| Net (payments) proceeds from related party line of credit | | | (10,846 | ) | | | 190,000 | |
| Proceeds from convertible note payable | | | 2,128,117 | | | | 203,500 | |
| Proceeds from lines of credit | | | 1,373,208 | | | | - | |
| Proceeds from issuance of notes payable, net of financing costs | | | 152,659 | | | | 2,871,058 | |
| Proceeds from common stock subscription | | | - | | | | 100,000 | |
| Net payments on notes payable | | | (1,334,781 | ) | | | (184,704 | ) |
| Net cash provided by (used in) financing activities | | | 2,308,357 | | | | 3,179,854 | |
| | | | | | | | | |
| Net increase (decrease) in cash and cash equivalents | | | 672,113 | | | | (461,258 | ) |
| Cash and cash equivalents, beginning of period | | | 67,045 | | | | 528,303 | |
| | | | | | | | | |
| Cash and cash equivalents, end of period | | $ | 739,158 | | | $ | 67,045 | |
| | | | | | | | | |
| SUPPLEMENTAL DISCLOSURES OF CASH FLOW INFORMATION: | | | | | | | | |
| Cash paid during the period for interest | | $ | 731,877 | | | $ | 467,670 | |
| Cash paid during the period for taxes | | $ | - | | | $ | - | |
| | | | | | | | | |
| Supplemental Disclosure on non-cash investing and financing activities: | | | | | | | | |
| Common stock issued in connection with acquisition of First Choice Medical Group, Inc. | | $ | - | | | $ | 497,725 | |
| Common stock issued in settlement of note payable | | $ | 624,000 | | | $ | - | |
| Common stock issued in settlement of related party line of credit | | $ | 142,484 | | | $ | - | |
| Common stock issued in connection with acquisition of patent | | $ | 286,500 | | | $ | - | |
| Common stock issued to acquire 10% interest in MedTech Diagnostics, LLC | | $ | 450,000 | | | $ | - | |
| Beneficial conversion feature on convertible note credited to additional paid-in-capital | | $ | 1,871,117 | | | $ | - | |
| Reclassification of derivative liability to additional paid-in-capital | | $ | 366,094 | | | $ | - | |
See the accompanying notes to these consolidated financial statements
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 1 – ORGANIZATION, BUSINESS AND PRINCIPLES OF CONSOLIDATION
A summary of the significant accounting policies applied in the presentation of the accompanying consolidated financial statements follows:
Basis and business presentation
First Choice Healthcare Solutions, Inc., a Delaware corporation (the “Company" or "FCHS”) filed a certificate of merger (the “Certificate of Merger”) of Medical Billing Assistance, Inc., a Colorado corporation incorporated on May 30, 2007 (“Medical Billing”), into the Company. The effective date for the Certificate of Merger was April 4, 2012. Pursuant to the Certificate of Merger, Medical Billing was merged with and into the Company. The effect of the merger was that Medical Billing reincorporated from Colorado to Delaware (the “Reincorporation”). The Company is deemed to be the successor issuer of Medical Billing under Rule 12g-3 of the Securities Exchange Act of 1934, as amended.
Contemporaneously with the Reincorporation, the Company changed its name to First Choice Healthcare Solutions, Inc. to more closely align the company’s name with its target market. Otherwise, the reincorporation does not result in any change in the business, management, fiscal year, accounting, and location of the principal executive offices, assets or liabilities of the Company, formerly known as Medical Billing Assistance, Inc.
On December 29, 2010, First Choice Healthcare Solutions, Inc., formerly known as Medical Billing Assistance, Inc., entered into a share exchange agreement (the "Agreement") with FCID Holdings, Inc. and FCID Medical, Inc., acquiring 100% of the outstanding common stock of FCID Holdings, Inc. and FCID Medical, Inc. through the issuance of 10,000,000 shares of its common stock. The transaction was accounted for as a reverse acquisition as the shareholders of FCID Holdings, Inc. and FCID Medical, Inc. retained the majority of the outstanding common stock of Medical Billing Assistance, Inc. after the share exchange. Effective with the Agreement, First Choice Healthcare Solutions, Inc.’s stockholders' equity was retroactively recapitalized as that of FCID Holdings, Inc. while 100% of the assets and liabilities of First Choice Healthcare Solutions, Inc. valued at $(100,550), consisting of cash $242, investment in subsidiary of $(66,286), accounts payable of $16,677, notes payable of $16,600, interest payable of $1,079, and other liabilities of $150 were recorded as being acquired in the reverse acquisition for its 2,429,000 outstanding common shares on the acquisition date. Subsequent to the December 29, 2010 recapitalization, First Choice Healthcare Solutions, Inc., FCID Holdings, Inc. and FCID Medical, Inc. remain separate legal entities (with First Choice Healthcare Solutions, Inc. as the parent of FCID Holdings, Inc. and FCID Medical, Inc.). All references to the “Company” or “we” or “us” or “our” refer to First Choice Healthcare Solutions, Inc. and its Subsidiaries unless otherwise differentiated. For accounting purposes, FCID Holdings, Inc. and Subsidiaries is treated as the surviving entity and accounting acquirer, although First Choice Healthcare Solutions, Inc. was the legal acquirer. Accordingly, the Company’s historical financial statements are those of FCID Holdings, Inc. and Subsidiaries.
All references to common stock, share and per share amounts have been retroactively restated to reflect the reverse capitalization as if the transaction had taken place as of the beginning of the earliest period presented.
FCID Holdings, Inc. was incorporated in the State of Florida on February 25, 2010. FCID Holdings, Inc. was formed to act as a holding corporation for other business entities as needed, including Marina Towers, LLC, a Florida limited liability company that owns and manages a commercial real estate office building. Marina Towers, LLC was formed in the State of Florida on July 24, 2003. Effective September 30, 2010, in an acquisition classified as a transaction between parties under common control, FCID Holdings, Inc. acquired all the outstanding membership interests of Marina Towers, LLC (12,000,000 FCID Holdings, Inc. common shares were issued for 60 Class A and 40 Class B membership interests of Marina Towers, LLC), making Marina Towers, LLC a wholly owned subsidiary of FCID Holdings, Inc.
The consolidated financial statements include the activity of Marina Towers, LLC from the date of its formation as if the transaction between the parties under common control had taken place as of the beginning of the earliest period presented.
On April 2, 2012, The Company, First Choice Healthcare Solutions, completed its acquisition of First Choice Medical Group of Brevard, LLC (“First Choice – Brevard”), pursuant to the Membership Interest Purchase Closing Agreement (the “Purchase Agreement”), dated the same date. The Company has been managing the practice of First Choice – Brevard since November 1, 2011, pursuant to a Management Services Agreement (the “Management Agreement”).
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 1 – ORGANIZATION, BUSINESS AND PRINCIPLES OF CONSOLIDATION (Continued)
The purchase price for the acquisition was $2,360,848, as adjusted, of which approximately $1.15 million was paid in cash, accounts receivable due the Company of $508,000 and the balance, net of closing adjustments including invoiced service fees, was paid by issuing to the members of First Choice – Brevard 244,045 shares, as adjusted, of the Company’s restricted common stock.
First Choice - Brevard is a multi-specialty medical group including orthopedics (both operative and non-operative), sports medicine, pain management and neurology. The practice is located in Marina Towers, a Class A office building owned by the Company.
A preliminary estimate of the fair values of the assets acquired and liabilities assumed at the date of acquisition are as follows:
| Assets acquired: | | | | |
| Current assets: | | | | |
| Cash | | $ | 48,761 | |
| Accounts receivable | | | 325,300 | |
| Total current assets | | | 374,061 | |
| | | | | |
| Property and equipment | | | 1,731,590 | |
| | | | | |
| Other assets: | | | | |
| Customer list | | | 300,000 | |
| Total acquired assets | | | 2,405,651 | |
| | | | | |
| Liabilities assumed: | | | | |
| Accounts payable | | | 44,802 | |
| | | | | |
| Net assets acquired | | $ | 2,360,849 | |
The consolidated financial statements include the accounts of the Company, including FCID Holdings, Inc., FCID Medical, Inc., First Choice Medical Group of Brevard, LLC and Marina Towers, LLC which are all wholly-owned subsidiaries of FCHS. All significant intercompany balances and transactions have been eliminated in consolidation.
NOTE 2 - SIGNIFICANT ACCOUNTING POLICIES
Use of Estimates
The preparation of the financial statements in conformity with generally accepted accounting principles requires management to make estimates and assumptions that affect certain reported amounts and disclosures. Accordingly, actual results could differ from those estimates.
Revenue Recognition
The Company recognizes revenue in accordance with Accounting Standards Codification subtopic 605-10, Revenue Recognition (“ASC 605-10”) which requires that four basic criteria must be met before revenue can be recognized: (1) persuasive evidence of an arrangement exists; (2) delivery has occurred; (3) the selling price is fixed and determinable; and (4) collectability is reasonably assured. Determination of criteria (3) and (4) are based on management's judgments regarding the fixed nature of the selling prices of the products delivered and the collectability of those amounts. Provisions for discounts and rebates to customers, estimated returns and allowances, and other adjustments are provided for in the same period the related sales are recorded.
ASC 605-10 incorporates Accounting Standards Codification subtopic 605-25, Multiple-Element Arraignments (“ASC 605-25”). ASC 605-25 addresses accounting for arrangements that may involve the delivery or performance of multiple products, services and/or rights to use assets. The effect of implementing 605-25 on the Company's financial position and results of operations was not significant.
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 2 - SIGNIFICANT ACCOUNTING POLICIES (Continued)
Accounts Receivable
Trade receivables are carried at their estimated collectible amounts. Trade credit is generally extended on a short-term basis; thus trade receivables do not bear interest. Trade accounts receivable are periodically evaluated for collectability based on past credit history with customers and their current financial condition. As of December 31, 2013 and 2012, the Company wrote off $361,284 and $-0- and charged to operations respectively.
Capitalized financing costs
Capitalized financing costs represent costs incurred in connection with obtaining the debt financing. These costs are amortized ratably and charged to financing expenses over the term of the related debt. The amortization for the years ended December 31, 2013 and 2012 was $57,348 and $57,348, respectively. Accumulated amortization of deferred financing costs were $133,812 and $76,464 at December 31, 2013 and 2012, respectively.
Concentrations of Credit Risk
The Company’s financial instruments that are exposed to a concentration of credit risk are cash and accounts receivable. Generally, the Company’s cash and cash equivalents in interest-bearing accounts may exceed FDIC insurance limits. The financial stability of these institutions is periodically reviewed by senior management.
Cash and Cash Equivalents
The Company considers cash and cash equivalents to consist of cash on hand and investments having an original maturity of 90 days or less that are readily convertible into cash. As of December 31, 2013, the Company had $739,158 in cash.
Segment Information
Accounting Standards Codification subtopic Segment Reporting 280-10 (“ASC 280-10”) establishes standards for reporting information regarding operating segments in annual financial statements and requires selected information for those segments to be presented in interim financial reports issued to stockholders. ASC 280-10 also establishes standards for related disclosures about products and services and geographic areas. Operating segments are identified as components of an enterprise about which separate discrete financial information is available for evaluation by the chief operating decision maker, or decision-making group, in making decisions how to allocate resources and assess performance. The information disclosed herein materially represents all of the financial information related to the Company’s principal two operating segments (see Note 15).
Patient list
Patient list is comprised of acquired patients in connection with the acquisition of First Choice - Brevard and is amortized ratably over the estimated useful life of 15 years. Amortization for the years ended December 31, 2013 and 2012 was $20,000 and $15,000, respectively. Accumulated amortization of patient list costs were $35,000 and $24,391 at December 31, 2013 and 2012, respectively.
Long-Lived Assets
The Company follows FASB ASC 360-10-15-3, “Impairment or Disposal of Long-lived Assets,” which established a “primary asset” approach to determine the cash flow estimation period for a group of assets and liabilities that represents the unit of accounting for a long-lived asset to be held and used. Long-lived assets to be held and used are reviewed for impairment whenever events or changes in circumstances indicate that the carrying amount of an asset may not be recoverable. The carrying amount of a long-lived asset is not recoverable if it exceeds the sum of the undiscounted cash flows expected to result from the use and eventual disposition of the asset. Long-lived assets to be disposed of are reported at the lower of carrying amount or fair value less cost to sell.
At December 31, 2013, the Company’s management performed an evaluation of its investment in MedTech for purposes of determining the implied fair value of the asset at December 31, 2013. The test indicated that the recorded remaining book value of its investment exceeded its fair value for the year ended December 31, 2013. As a result, upon completion of the assessment, management recorded a non-cash impairment charge of $450,000, net of tax, or $0.03 per share during the year ended December 31, 2013 to reduce the carrying value of the investment to $0. Considerable management judgment is necessary to estimate the fair value. Accordingly, actual results could vary significantly from management’s estimates. (see Note 6).
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 2 - SIGNIFICANT ACCOUNTING POLICIES (Continued)
Property and Equipment
Property and equipment are stated at cost. When retired or otherwise disposed, the related carrying value and accumulated depreciation are removed from the respective accounts and the net difference less any amount realized from disposition, is reflected in earnings. For financial statement purposes, property and equipment are recorded at cost and depreciated using the straight-line method over their estimated useful lives of 20 to 39 years.
Net Loss Per Share
The Company accounts for net loss per share in accordance with Accounting Standards Codification subtopic 260-10, Earnings Per Share (“ASC 260-10”), which requires presentation of basic and diluted earnings per share (“EPS”) on the face of the statement of operations for all entities with complex capital structures and requires a reconciliation of the numerator and denominator of the basic EPS computation to the numerator and denominator of the diluted EPS.
Basic net loss per share is computed by dividing net loss by the weighted average number of shares of common stock outstanding during each period. It excludes the dilutive effects of potentially issuable common shares such as those related to our issued convertible debt, warrants and stock options. Diluted net loss per share for years ending December 31, 2013 and 2012 does not reflect the effects of 3,414,070 and 2,029,686 shares, respectively, potentially issuable upon the conversion of our convertible note payable or the exercise of the Company's stock options and warrants (calculated using the treasury stock method) as of December 31, 2013 and 2012 as including such would be anti-dilutive.
Stock-Based Compensation
Share-based compensation issued to employees is measured at the grant date, based on the fair value of the award, and is recognized as an expense over the requisite service period. The Company measures the fair value of the share-based compensation issued to non-employees using the stock price observed in the arms-length private placement transaction nearest the measurement date (for stock transactions) or the fair value of the award (for non-stock transactions), which were considered to be more reliably determinable measures of fair value than the value of the services being rendered. The measurement date is the earlier of (1) the date at which commitment for performance by the counterparty to earn the equity instruments is reached, or (2) the date at which the counterparty’s performance is complete. As of December 31, 2013, the Company had no non-employee options outstanding to purchase shares of common stock.
Derivative Instrument Liability
The Company accounts for derivative instruments in accordance with ASC 815, which establishes accounting and reporting standards for derivative instruments and hedging activities, including certain derivative instruments embedded in other financial instruments or contracts and requires recognition of all derivatives on the balance sheet at fair value, regardless of hedging relationship designation. Accounting for changes in fair value of the derivative instruments depends on whether the derivatives qualify as hedge relationships and the types of relationships designated are based on the exposures hedged. At December 31, 2013 and 2012, the Company did not have any derivative instruments that were designated as hedges.
Fair Value
Accounting Standards Codification subtopic 825-10, Financial Instruments (“ASC 825-10”) requires disclosure of the fair value of certain financial instruments. The carrying value of cash and cash equivalents, accounts payable and accrued liabilities, and short-term borrowings, as reflected in the balance sheets, approximate fair value because of the short-term maturity of these instruments. All other significant financial assets, financial liabilities and equity instruments of the Company are either recognized or disclosed in the financial statements together with other information relevant for making a reasonable assessment of future cash flows, interest rate risk and credit risk. Where practicable the fair values of financial assets and financial liabilities have been determined and disclosed; otherwise only available information pertinent to fair value has been disclosed.
The company follows Accounting Standards Codification subtopic 820-10, Fair Value Measurements and Disclosures (“ASC 820-10”) and Accounting Standards Codification subtopic 825-10, Financial Instruments (“ASC 825-10”), which permits entities to choose to measure many financial instruments and certain other items at fair value. Neither of these statements had an impact on the Company’s financial position, results of operations nor cash flows.
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 2 - SIGNIFICANT ACCOUNTING POLICIES (Continued)
Patents
Intangible assets with finite lives are amortized over their estimated useful lives. Intangible assets with indefinite lives are not amortized, but are tested for impairment annually. The Company’s intangible assets with finite lives are patent costs, which are amortized over their economic or legal life, whichever is shorter. These patent costs were acquired on September 7, 2013 by the issuance of 636,666 shares of the Company’s common stock to a related party (See Note 12). The shares of common stock were valued at $286,500, which was estimated to be approximately the fair value of the patent acquired and did not materially differ from the fair value of the common stock.
Income Taxes
The Company follows Accounting Standards Codification subtopic 740-10, Income Taxes (“ASC 740-10”) for recording the provision for income taxes. Deferred tax assets and liabilities are computed based upon the difference between the financial statement and income tax basis of assets and liabilities using the enacted marginal tax rate applicable when the related asset or liability is expected to be realized or settled. Deferred income tax expenses or benefits are based on the changes in the asset or liability during each period. If available evidence suggests that it is more likely than not that some portion or all of the deferred tax assets will not be realized, a valuation allowance is required to reduce the deferred tax assets to the amount that is more likely than not to be realized. Future changes in such valuation allowance are included in the provision for deferred income taxes in the period of change. Deferred income taxes may arise from temporary differences resulting from income and expense items reported for financial accounting and tax purposes in different periods. Deferred taxes are classified as current or non-current, depending on the classification of assets and liabilities to which they relate. Deferred taxes arising from temporary differences that are not related to an asset or liability are classified as current or non-current depending on the periods in which the temporary differences are expected to reverse and are considered immaterial.
Recent Accounting Pronouncements
There were various updates recently issued, most of which represented technical corrections to the accounting literature or application to specific industries and are not expected to a have a material impact on the Company’s condensed consolidated financial position, results of operations or cash flows.
NOTE 3 – LIQUIDITY
The Company incurred various non-recurring expenses in 2012 in connection with operating startup costs relating to the acquisition of a medical practice. Management believes the positive year-end earnings before interest, taxes, depreciation and amortization and the continuing trend of positive growth before interest, taxes, depreciation and amortization through 2014 will support improved liquidity. Moreover, the Company issued and sold to Hillair Capital Investments, L.P. a $2,320,000 8% Original Issue Discount Convertible Debenture, raising net proceeds of $2,000,000 less customary legal and due diligence fees. The Company then paid off or converted to equity a total of $1,238,480 in debt and modified its $1.5 million line of credit with CT Capital, providing for the reduction of the annual interest rate from 12% per annum to 6% per annum in exchange for the issuance of 100,000 restricted shares of the Company’s common stock. As of December 31, 2013, the Company has used $800,000 of the available CT Capital line of credit.
The Marina Towers building is fully occupied. The Company believes that ongoing operations of Marina Towers, LLC, the current strong, positive cash balance along with continued execution of its business development plan will allow the Company to further improve its working capital; and that it will have sufficient capital resources to meet projected cash flow requirements through the date that is one year plus a day from the filing date of this report. However, there can be no assurance that the Company will be successful in fully executing its business development plan.
NOTE 4 – CASH - RESTRICTED
Cash-restricted is comprised of funds deposited to and held by the mortgage lender for payments of property taxes, insurance, replacements and major repairs of the Company's commercial building. The majority of the restricted funds are reserved for tenant improvements.
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 5 — PROPERTY, PLANT, AND EQUIPMENT
Property, plant and equipment at December 31, 2013 and 2012 are as follows:
| | | 2013 | | | 2012 | |
| Land | | $ | 1,000,000 | | | $ | 1,000,000 | |
| Building | | | 3,055,168 | | | | 3,055,168 | |
| Building improvements | | | 3,953,846 | | | | 3,806,771 | |
| Automobiles | | | 29,849 | | | | 29,849 | |
| Computer equipment | | | 210,698 | | | | 186,549 | |
| Medical equipment | | | 2,238,639 | | | | 2,039,393 | |
| Office equipment | | | 132,984 | | | | 104,840 | |
| | | | 10,621,184 | | | | 10,222,570 | |
| Less: accumulated depreciation | | | (1,959,127 | ) | | | (1,465,939 | ) |
| | | $ | 8,662,057 | | | $ | 8,756,631 | |
During the year ended December 31, 2013 and 2012, depreciation expense charged to operations was $483,797 and $309,899, respectively.
NOTE 6 — INVESTMENTS
On September 7, 2013, the Company acquired an aggregate 10% membership interest in MedTech Diagnostics, LLC, a Florida distributor of multi-test medical diagnostic equipment. The investment is recorded at an aggregate cost of $450,000, which was determined at the date of the acquisition, and based on the fair value of the underlying issued common shares, or $0.45 per share. More specifically, the Company acquired a 3.75% membership interest for 375,000 shares of its common stock valued at the date of the acquisition of $168,750; and a 6.25% membership interest valued at the date of the acquisition of $281,250. At December 31, 2013, the Company’s management performed an evaluation of its investment in MedTech for purposes of determining the implied fair value of the asset at December 31, 2013. The test indicated that the recorded remaining book value of its investment exceeded its fair value for the year ended December 31, 2013. As a result, upon completion of the assessment, management recorded a non-cash impairment charge of $450,000, net of tax, or $0.03 per share during the year ended December 31, 2013 to reduce the carrying value of the investment to $0. Considerable management judgment is necessary to estimate the fair value. Accordingly, actual results could vary significantly from management’s estimates.
NOTE 7 — LINES OF CREDIT
Line of Credit, CT Capital
On June 13, 2013, the Company’s subsidiary, First Choice Medical Group of Brevard, LLC, entered into a Loan and Security Agreement (the “Loan Agreement”) with CT Capital. Ltd., d/b/a CT Capital, LP, a Florida limited liability partnership (the “Lender”). Under the Loan Agreement, the Lender committed to make an accounts receivable line of credit in the maximum aggregate amount of $1,500,000 to First Choice Medical Group of Brevard, LLC with an interest rate of 12% per annum (the “Loan”). The maturity date of the Loan is December 31, 2016 (the “Maturity Date”). Interest shall be due and payable monthly. Upon default, the interest may be adjusted to the highest rate permissible by law. The Loan is secured by the accounts receivable, and assets of the Company’s subsidiary, First Choice Medical Group of Brevard, LLC. The assets constitute the collateral for the repayment of the Loan. The Loan Agreement also includes covenants, representations, warranties, indemnities and events of default that are customary for facilities of this type. The advance rate is defined as: 80% of all receivables to be 120 days or less at the net collection rate of approximately 27% of total billings, excluding patient billings and collections. Additionally, allowable accounts receivable will also include 50% of all accounts receivable protected by Legal Letters of Protection. At any time, the Lender may convert all or any portion of the outstanding principal amount or interest on the Loan into the common stock of the Company at a price equal to $0.75 per share. The Company did not record an embedded beneficial conversion feature in the note since the fair value of the common stock did not exceed the conversion rate at the date of commitment.
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 7 — LINES OF CREDIT (Continued)
On November 8, 2013, in consideration for a fee of 100,000 shares of the Company’s common stock, restricted pursuant to Rule 144, CT Capital agreed to modify the line of credit to the Company’s subsidiary, First Choice Medical Group of Brevard, LLC. Under the loan modification agreement, the annual rate of interest was reduced from 12% per annum to 6% per annum and will remain at 6% until November 1, 2015. All other terms under the June 13, 2013 Loan and Security Agreement will remain the same.
The obligations of the Company under the Loan Agreement are guaranteed by certain affiliates of the Company, including a personal guarantee issued by the Company’s Chief Executive Officer.
Line of Credit, MTI Capital
On May 1, 2013, the Company entered into a loan commitment whereby MTI Capital LLC provided a line of credit up to $2,000,000 in the form of a convertible loan with interest at 12% per annum, payable monthly with principal due two years from the effective date of the loan. On August 28, 2013, the Company amended the loan agreement to change the conversion rate from $0.75 per share to $0.45 per share.
In the third quarter 2013, the Company did not record an embedded beneficial conversion feature in the note since the fair value of the common stock did not exceed the conversion rate at the date of commitment or amendment.
On November 8, 2013, MTI converted the then outstanding balance of $624,000 principal and interest amount on the loan, into shares of the Company’s common stock at a price equal to $0.45 per share for a total of 1,386,667 shares issued. Our corporate transfer agent reported to us that MTI redistributed the majority of its shares in our Company to unaffiliated third parties.
NOTE 8 — LINE OF CREDIT, RELATED PARTY
On February 1, 2012, the Company opened a $500,000 unsecured, revolving line of credit loan with CCR of Melbourne, Inc., an entity jointly owned and controlled at that time by the Company's Chief Executive Officer and Carmen Romandetti, the Chief Executive Officer’s father. The revolving line of credit loan was to mature on October 1, 2015 with interest at a per annum rate of 8.5% beginning March 1, 2012. Advances on the line of credit were at the sole discretion of CCR of Melbourne, Inc. The Company accrued $11,153 and $6,339 as related party interest for the years ended December 31, 2013 and 2012, respectively.
On November 8, 2013, CCR converted the then outstanding balance of $142,483.52, representing all of the outstanding related party principal and interest amount on the loan, into shares of the Company’s common stock at a price equal to $0.45 per share for a total of 316,631 shares issued.
On November 8, 2013, the Chief Executive Officer relinquished all rights, title to and ownership in CCR to Carmen Romandetti in consideration of a personal loan made to the Chief Executive Officer by Carmen Romandetti.
NOTE 9 — NOTE PAYABLE, RELATED PARTY
The Company entered into an unsecured loan agreement with HS Real Company, LLC (“HSR”) on May 17, 2012 for $100,000 at an interest rate of 12% per annum (the "HSR Note"). On August 5, 2012, HSR increased the principal amount to $250,000, and subsequently HSR advanced an additional $50,000 to the Company, bringing the aggregate principal amount of the HSR Note to $300,000, all of which was due and payable to HSR on December 31, 2012. The Company paid $27,556 and $17,053 as interest on the HSR note for the years ended December 31, 2013 and 2012, respectively.
On November 8, 2013, the Company paid off the HSR Note in full, remitting HSR $300,000 for the outstanding principal and interest balance due on the HSR Note.
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 10 — CONVERTIBLE NOTES PAYABLE
Convertible notes payable at December 31, 2013 and 2012 are as follows:
| | | 2013 | | | 2012 | |
| Note payable, 8% per annum due November 1, 2015, including accrued interest | | $ | 2,347,403 | | | $ | - | |
| Note payable, 8% per annum due September 18, 2013, net of unamortized debt discount of $160,543 including accrued interest | | | - | | | | 43,537 | |
| | | | 2,347,403 | | | | 43,537 | |
| Less: current portion | | | (- | ) | | | (43,537 | ) |
| | | $ | 2,347,403 | | | $ | - | |
Hillair Capital Investments, L.P.
On November 8, 2013, the Company entered into a Securities Purchase Agreement (the “Securities Purchase Agreement”) with Hillair Capital Investments L.P. ("Hillair") whereby the Company received $2,000,000 in gross proceeds from Hillair in exchange for (i) a $2,320,000, 8% Original Issue Discount Convertible Debenture due December 28, 2013, subject to an extension through November 1, 2015 (the “Debenture”), and (ii) a Common Stock Purchase Warrant (the “Warrant”) to purchase up to 2,320,000 shares of the Company’s common stock (the “Common Stock”) at an exercise price of $1.35 per share, which may be exercised on a cashless basis, until November 8, 2018.
The Company issued to Hillair the Debenture with the Warrant for the net purchase price of $2,000,000 (reflecting the $320,000 original issue discount). Until the Debenture is no longer outstanding, the Debenture shall be convertible, in whole or in part at the option of Hillair, into shares of Common Stock, subject to certain conversion limitations set forth in the Debenture. The Company, however, has reserved the right to pay the Debenture in cash. The conversion price for the Debenture is $1.00 per share, subject to adjustment for stock splits, stock dividends, sales of securities for less than $1.00 per share or other distributions by the Company. As a result of the Company achieving certain milestones, however, the conversion price shall not be reduced to less than $1.00 per share as a result of any subsequent sales of securities for less than $1.00 per share of common stock.
The Company will be obligated to redeem $580,000 of principal on February 1, 2015, May 1, 2015, August 1, 2015 and November 1, 2015, plus accrued but unpaid interest and any other amounts that may be owed to the holder of the Debenture on those dates. Interest on the Debenture accrues at the rate of 8% annually and is payable quarterly on August 1, November 1, February 1, and May 1, beginning on August 1, 2014. Interest is payable in cash or at the Company’s option in shares of the Company’s common stock; provided certain conditions are met.
On or after May 8, 2014, the Company may elect to prepay any portion of the principal amount of the Debenture, subject to providing advance notice to the holder of the Debenture, at 120% of the then outstanding principal amount of the Debenture, plus accrued but unpaid interest and any other amounts then owed to the holder of the Debenture as further set forth therein, subject to certain conditions set forth in the Debenture.
To secure the Company’s obligations under the Debenture, the Company granted Hillair a security interest in certain of its and its subsidiaries’ assets in the Company as described in the Security Agreement. In addition, certain of the Company’s subsidiaries agreed to guarantee the Company’s obligations pursuant to the Subsidiary Guarantees.
As described above, in connection with the issuance of the debenture, the Company issued detachable warrants granting the holder the right to acquire an aggregate of 2,320,000 shares of the Company’s common stock at $1.35 per share. In accordance with ASC 470-20, the Company recognized the value attributable to the warrants and the conversion feature in the amount of $1,871,117 to additional paid-in capital and a discount against the notes. The Company valued the warrants in accordance with ASC 470-20 using the Black-Scholes pricing model and the following assumptions: contractual terms of 3.6 years, an average risk free interest rate of 1.42%, a dividend yield of 0%, and volatility of 147.94%. During the year ended December 31, 2013, the Company amortized $1,871,117 of the debt discount to operations as interest expense.
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 10 — CONVERTIBLE NOTES PAYABLE (Continued)
Convertible Notes
On December 14, 2012, February 19, 2013, and August 14, 2013, the Company entered into Securities Purchase Agreements for the sale of 8% convertible notes in the original principal amounts of $203,500, $103,500 and $153,500, respectively, with a lender in reliance upon the exemption from registration under Section 4(a)(2) (formerly Section 4(2)) of the Securities Act of 1933, as amended (the “Securities Act”). During the year ended December 31, 2013, the Company paid off each of these notes payable in cash.
The Company has identified the embedded derivatives related to the above described Notes. These embedded derivatives included certain conversion features and reset provision. The accounting treatment of derivative financial instruments requires that the Company record fair value of the derivatives as of the inception date of Lender’s Note and to fair value as of each subsequent reporting date.
At the inception of the Notes, the Company determined the aggregate fair value of $397,325 of embedded derivatives. The fair value of the embedded derivatives was determined using the Binomial Lattice Option Pricing Model based on the following assumptions: (1) dividend yield of 0%; (2) expected volatility of 98.67 to 119.96%, (3) weighted average risk-free interest rate of 0.12 % to 0.17% (4) expected life of 0.76 years, and (5) estimated fair value of the Company’s common stock of $0.60 to $2.14 per share.
During the year ended December 31, 2013, the Company paid off all outstanding Asher notes. As such, the Company marked to market the fair value of the debt derivative at the date(s) of payoff and reclassified the determined aggregate fair values of $366,094 to equity. The fair values of the embedded derivatives was determined using Binomial Lattice Option Pricing Model based on the following assumptions: (1) dividend yield of 0%, (2) expected volatility of 116.11% to 147.94%, (3) weighted average risk-free interest rate of 0.03% to 09%, (4) expected life of 0.25 to 0.52 year, and (5) estimated fair value of the Company’s common stock of $0.55 to 1.40 per share.
During the years ended December 31, 2013 and 2012, the Company amortized and wrote off $2,706,869 and $10,457 of debt discount to operations as interest expense.
NOTE 11 — NOTES PAYABLE
Notes payable as of December 31, 2013 and 2012 are comprised of the following:
| | | 2013 | | | 2012 | |
| Mortgage payable | | $ | 7,353,398 | | | $ | 7,444,580 | |
| Note payable, GE Capital (construction), MRI | | | 278,287 | | | | 450,604 | |
| Note payable, GE Capital (construction), 2 | | | 100,977 | | | | 153,340 | |
| Note Payable, GE Capital (MRI) | | | 1,592,278 | | | | 1,806,932 | |
| Note Payable, GE Capital (X-ray) | | | 184,001 | | | | 213,126 | |
| Note Payable, GE Arm | | | 114,597 | | | | - | |
| Note payable, Auto | | | 22,211 | | | | 27,300 | |
| Capital lease, Equipment | | | 33,511 | | | | - | |
| Note payable, Dr. Richard Newman | | | - | | | | 5,000 | |
| | | | 9,679,260 | | | | 10,100,882 | |
| Less: current portion | | | (743,787 | ) | | | (690,586 | ) |
| | | $ | 8,935,473 | | | $ | 9,410,296 | |
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 11 — NOTES PAYABLE (Continued)
Mortgage Payable
On August 12, 2011, the Company refinanced its existing mortgage note payable as described below providing additional working capital funds. The aggregate amount of the note of $7,550,000 bears 6.10% interest per annum with monthly payments of $45,752.61 beginning in October 2011 based on a 30 year amortization schedule with all remaining principal and interest due in full on September 16, 2016. The note is secured by land and the building along with first priority assignment of leases and rents. Tenant rents are mailed to lockbox operated by the mortgage service company. In addition, the Company's Chief Executive Officer provided a limited personal guaranty.
In connection with the refinancing of the mortgage note payable, the Company incurred financing costs of $286,723. The capitalized financing costs are amortized ratably over the term of the mortgage note payable.
Note Payable – Equipment Financing
On May 21, 2012, the Company completed a financing with GE Healthcare Financial Services (“GE Capital”) for approximately $2.4 million.
As of September 30, 2012, the Company had drawn down a total of $450,000 against the first construction loan. This construction loan is payable in 35 monthly payments (first three payments are $nil) including interest at 7.38%, beginning the earlier of a) December 2012 or b) total advances have been made in the amount of $450,000.
On September 24, 2012, the Company drew down a total of $150,000 against the second construction loan. This construction loan is payable in 35 monthly payments (first three payments are $nil) including interest at 7.38%, beginning the earlier of a) December 2012 or b) total advances have been made in the amount of $150,000
The Company entered into an aggregate of $2,288,679 equipment finance leases subject to delivery and acceptance. All notes and finance leases have been personally guaranteed by the Company's Chief Executive Officer.
On August 22, 2012, the Company accepted the delivery of X-ray equipment under the equipment finance leases discussed above. As such, the component piece accepted of $212,389 is due over 60 months at $-0- the first three months; $4,300 for the remaining 57 months including interest at 7.9375% per annum. On March 8, 2013, the Company amended the finance lease to interest only payments of $1,384 for three months; $4,575 for the remaining 56 monthly payments.
On September 27, 2012, the Company accepted the delivery of MRI equipment under the equipment finance leases discussed above. As such, the component piece accepted of $1,771,390 is due over 60 months at $-0- the first three months; $38,152 for the remaining 57 months including interest at 7.9375% per annum. On March 8, 2013, the Company amended the finance lease to interest only payments of $11,779 for three months; $38,152 for the remaining 56 monthly payments.
On February 25, 2013, the Company accepted the delivery of C-arm equipment under the equipment finance leases discussed above. As such, the component piece accepted of $117,322 is due over 63 months at $-0- the first three months; $2,388 for the remaining 60 months including interest at 7.39% per annum.
Note Payable – Auto
On May 21, 2012, the Company issued a note payable, in the amount of $29,850, due in monthly installments of $593 including interest of 6.99%, due to mature in June 2017, and secured by related equipment. The outstanding balance on the note payable as of December 31, 2013 was $22,211.
Capital Lease – Equipment
On June 11, 2013, the Company entered into a lease agreement to acquire equipment with 48 monthly payments of $956.45 payable through June 1, 2017 with an effective interest rate of 14.002% per annum. The Company may elect to acquire the leased equipment at a nominal amount at the end of the lease.
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 11 — NOTES PAYABLE (Continued)
Note Payable – Newman
In January 2013, the following note was paid in full.
In connection with the acquisition of First Choice – Brevard as described in Note 1 above, the Company assumed a $45,000 non-interest bearing, unsecured note payable to Dr. Richard Newman at $5,000 per month, matured on January 1, 2013.
Aggregate maturities of long-term debt as of December 31:
| | | Amount | |
| Year ended December 31, 2014 | | $ | 743,787 | |
| Year ended December 31, 2015 | | | 715,085 | |
| Year ended December 31, 2016 | | | 7,632,286 | |
| Year ended December 31, 2017 | | | 523,608 | |
| Year ended December 31, 2018 and thereafter | | | 64,494 | |
| Total | | $ | 9,679,260 | |
NOTE 12 — RELATED PARTY TRANSACTIONS
As more fully described in Note 8 – Line of Credit, Related Party above, CCR of Melbourne, Inc., an entity jointly owned and controlled at that time by the Company's Chief Executive Officer and Carmen Charles Romandetti, the Chief Executive Officer’s father, provided a $500,000 unsecured revolving line of credit to the Company. The Company accrued $11,153 and $6,339 as related party interest for the years ended December 31, 2013 and 2012, respectively. On November 8, 2013, CCR converted the then outstanding balance of $142,483.52, representing all of the outstanding related party principal and interest amount on the loan, into shares of the Company’s common stock at a price equal to $0.45 per share for a total of 316,631 shares issued. On November 8, 2013, the Chief Executive Officer relinquished all rights, title to and ownership in CCR to Carmen Romandetti in consideration of a personal loan made to the Chief Executive Officer by Carmen Romandetti.
As more fully described in Note 9 – Note Payable, Related Party above, the Company entered into an unsecured loan agreement with HS Real Company, LLC (“HSR”) on May 17, 2012 for $100,000 at an interest rate of 12% per annum (the "HSR Note"). On August 5, 2012, HSR increased the principal amount to $250,000, and subsequently HSR advanced an additional $50,000 to the Company, bringing the aggregate principal amount of the HSR Note to $300,000, all of which was due and payable to HSR on December 31, 2012. The Company paid $27,556 and $17,053 as interest on the HSR note for the years ended December 31, 2013 and 2012, respectively. Mr. Colin Halpern is both an Affiliate of HSR and a member of the Board of Directors of First Choice Healthcare Solutions, Inc. On November 8, 2013, the Company paid off the HSR Note, remitting HSR $300,000 for the outstanding principal and interest balance due on the HSR Note.
On September 7, 2013, the Company acquired a patent, US 7,789,842 B2, for an orthopedic adjustable arm sling from Donald A. Bittar, the inventor and the Company’s Chief Financial Officer. Based on the independent, third party evaluation of Professional Business Brokers, Inc., the patent was valued at $286,500. The Company issued Mr. Bittar 636,666 shares of its common stock, valued at $286,500, or $0.45 per share, which was estimated to approximate fair value of the patent acquired and did not materially differ from the fair value of the common stock at the time of issuance.
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 13 — CAPITAL STOCK
Preferred stock
The Company is authorized to issue 1,000,000 shares $0.01 par value preferred stock. As of December 31, 2013 and 2012, none was issued and outstanding.
Common stock
The Company is authorized to issue 100,000,000 shares of $0.001 par value common stock. As of December 31, 2013 and 2012, 16,747,248 and 12,706,795 shares were issued and outstanding, respectively.
On April 4, 2012, the Company affected a four-to-one (4 to 1) reverse stock split of its issued and outstanding shares of common stock, $0.001 par value (whereby every four shares of Company’s common stock will be exchanged for one share of FCHS common stock). All references in the consolidated financial statements and the notes to consolidated financial statements, number of shares, and share amounts have been retroactively restated to reflect the reverse split. The Company has restated from 49,851,000 to 12,462,750 shares of common stock issued and outstanding as of December 31, 2011 to reflect the reverse split.
In April 2012, the Company issued an aggregate of 244,045 shares of its common stock in connection with the acquisition of First Choice Medical Group of Brevard, LLC.
In July 2012, the Company sold 66,666 shares of common stock as part of a stock subscription agreement which expired December 2012. The Company received $100,000 in July 2012. The shares were issued in February 2013.
In December 2011, the Company issued 33,750 shares of its common stock for services rendered. The shares of common stock were valued at $116,100, which was estimated to be approximate the fair value of the Company’s common shares during the period covered by the service provided.
During the year ended December 31, 2013, the Company issued an aggregate of 533,822 shares of its common stock to officers, employees and service providers at an aggregate fair value of $383,101.
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 14 — STOCK OPTIONS AND WARRANTS
Warrants
The following table summarizes the warrants outstanding and the related exercise prices for the underlying shares of the Company's common stock as of December 31, 2013:
| | | | Warrants Outstanding | | | | | | | | Warrants Exercisable | |
| | | | | | | | | Weighted | | | | | | Weighted | |
| Price | | | Outstanding | | | Expiration Date | | Price | | | Exercisable | | | Price | |
| $ | 1.35 | | | | 2,320,000 | | | November 8, 2018 | | $ | 1.35 | | | | 2,320,000 | | | $ | 1.35 | |
| | 3.60 | | | | 1,875,000 | | | December 31, 2016 | | | 3.60 | | | | 1,875,000 | | | | 3.60 | |
| | | | | | 4,195,000 | | | | | $ | 2.36 | | | | 4,195,000 | | | $ | 2.36 | |
The warrant to purchase up to 2,320,000 shares of the Company’s common stock may be exercised on a cashless basis. The warrant to purchase up to 1,875,000 shares of the Company’s common stock may not be exercised on a cashless basis.
Transactions involving stock warrants issued to non-employees are summarized as follows:
| | | Number of
Shares | | | Weighted
Average
Price
Per Share | |
| Outstanding at December 31, 2011: | | | 1,875,000 | | | $ | 3.60 | |
| Granted | | | - | | | | - | |
| Exercised | | | - | | | | - | |
| Expired | | | - | | | | - | |
| Outstanding at December 31, 2012: | | | 1,875,000 | | | | 3.60 | |
| Granted | | | 2,320,000 | | | | 1.35 | |
| Exercised | | | - | | | | - | |
| Expired | | | - | | | | - | |
| Outstanding at December 31, 2013: | | | 4,195,000 | | | $ | 2.36 | |
On November 8, 2013, the Company issued 2,320,000 warrants to purchase the Company’s common stock at $1.35, expiring November 18, 2018, in connection with the securities purchase agreement dated November 8, 2013. See Note 10 above.
As of December 31, 2013, the Company had no outstanding options.
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 15 — SEGMENT REPORTING
The Company reports segment information based on the “management” approach. The management approach designates the internal reporting used by management for making decisions and assessing performance as the source of the Company’s reportable segments. The Company has two reportable segments: Marina Towers, LLC and FCID Medical, Inc.
The Marina Towers, LLC segment derives revenue from the operating leases of its owned building, whereas FCID Medical segment derives revenue for medical services provided to patients.
Information concerning the operations of the Company's reportable segments is as follows:
Summary Statement of Operations for the year ended December 31, 2013:
| | | Marina | | | FCID | | | | | | Intercompany | | | | |
| | | Towers | | | Medical | | | Corporate | | | Eliminations | | | Total | |
| Revenue: | | | | | | | | | | | | | | | | | | | | |
Net patient service revenue | | $ | - | | | $ | 5,459,373 | | | $ | - | | | $ | - | | | $ | 5,459,373 | |
| Rental revenue | | | 1,473,048 | | | | - | | | | - | | | | (424,579 | ) | | | 1,048,469 | |
| Total Revenue | | | 1,473,048 | | | | 5,459,373 | | | | - | | | | (424,579 | ) | | | 6,507,842 | |
| | | | | | | | | | | | | | | | | | | | | |
| Operating expenses: | | | | | | | | | | | | | | | | | | | | |
| Salaries and benefits | | | 12,000 | | | | 2,537,024 | | | | 547,261 | | | | - | | | | 3,096,285 | |
| Other operating expenses | | | 385,712 | | | | 1,754,809 | | | | - | | | | (424,579 | ) | | | 1,715,942 | |
| General and administrative | | | 82,186 | | | | 669,248 | | | | 953,720 | | | | - | | | | 1,705,154 | |
| Impairment of investment | | | - | | | | - | | | | 450,000 | | | | - | | | | 450,000 | |
| Depreciation and amortization | | | 164,884 | | | | 353,727 | | | | - | | | | - | | | | 518,611 | |
| Total operating expenses | | | 644,782 | | | | 5,314,808 | | | | 1,950,981 | | | | (424,579 | ) | | | 7,485,992 | |
| | | | | | | | | | | | | | | | | | | | | |
| Net income (loss) from operations: | | | 828,266 | | | | 144,565 | | | | (1,950,981 | ) | | | - | | | | (978,150 | ) |
| | | | | | | | | | | | | | | | | | | | | |
| Interest expense | | | (464,250 | ) | | | (269,593 | ) | | | (2,970,243 | ) | | | - | | | | (3,704,086 | ) |
| Amortization of financing costs | | | (57,348 | ) | | | - | | | | - | | | | - | | | | (57,348 | ) |
| Gain on change in derivative liability | | | - | | | | - | | | | 32,218 | | | | - | | | | 32,218 | |
| Other income (expense) | | | 3,063 | | | | - | | | | - | | | | - | | | | 3,063 | |
| | | | | | | | | | | | | | | | | | | | | |
| Net Income (loss): | | | 309,731 | | | | (125,028 | ) | | | (4,889,006 | ) | | | - | | | | (4,704,303 | ) |
| | | | | | | | | | | | | | | | | | | | | |
| Income taxes | | | - | | | | - | | | | - | | | | - | | | | - | |
| | | | | | | | | | | | | | | | | | | | | |
| Net income (loss) | | $ | 309,731 | | | $ | (125,028 | ) | | $ | (4,889,006 | ) | | $ | - | | | $ | (4,704,303 | ) |
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 15 — SEGMENT REPORTING (Continued)
Summary Statement of Operations for the year ended December 31, 2012:
| | | Marina | | | FCID | | | | | | Intercompany | | | | |
| | | Towers | | | Medical | | | Corporate | | | Eliminations | | | Total | |
| Revenue: | | | | | | | | | | | | | | | | | | | | |
Net patient service revenue | | $ | - | | | $ | 2,645,310 | | | $ | - | | | $ | - | | | $ | 2,645,310 | |
| Rental revenue | | | 1,459,092 | | | | - | | | | - | | | | (299,055 | ) | | | 1,160,037 | |
| Total Revenue | | | 1,459,092 | | | | 2,645,310 | | | | - | | | | (299,055 | ) | | | 3,805,347 | |
| | | | | | | | | | | | | | | | | | | | | |
| Operating expenses: | | | | | | | | | | | | | | | | | | | | |
| Practice salaries & benefits | | | 12,000 | | | | 1,257,948 | | | | 323,297 | | | | - | | | | 1,593,245 | |
| Practice supplies and other operating expenses | | | - | | | | 1,164,696 | | | | - | | | | (299,055 | ) | | | 865,641 | |
| General and administrative | | | 445,392 | | | | 230,087 | | | | 638,823 | | | | - | | | | 1,314,302 | |
| Depreciation and amortization | | | 161,818 | | | | 148,081 | | | | - | | | | - | | | | 309,899 | |
| Total operating expenses | | | 619,210 | | | | 2,800,812 | | | | 962,120 | | | | (299,055 | ) | | | 4,083,087 | |
| | | | | | | | | | | | | | | | | | | | | |
| Net income (loss) from operations: | | | 839,882 | | | | (155,502 | ) | | | (962,120 | ) | | | - | | | | (277,740 | ) |
| | | | | | | | | | | | | | | | | | | | | |
| Interest expense | | | (463,205 | ) | | | (80,805 | ) | | | (19,381 | ) | | | - | | | | (563,391 | ) |
| Amortization of financing costs | | | (57,348 | ) | | | - | | | | - | | | | - | | | | (57,348 | ) |
| Other income (expense) | | | 3,000 | | | | - | | | | (987 | ) | | | - | | | | 2,013 | |
| | | | | | | | | | | | | | | | | | | | | |
| Net Income (loss): | | | 322,329 | | | | (236,307 | ) | | | (982,488 | ) | | | - | | | | (896,466 | ) |
| | | | | | | | | | | | | | | | | | | | | |
| Income taxes | | | (8,307 | ) | | | 6,090 | | | | 25,320 | | | | - | | | | 23,103 | |
| | | | | | | | | | | | | | | | | | | | | |
| Net income (loss) | | $ | 314,022 | | | $ | (230,217 | ) | | $ | (957,168 | ) | | $ | - | | | $ | (873,363 | ) |
| | | Marina | | | FCID | | | | | | Intercompany | | | | |
| | | Towers | | | Medical | | | Corporate | | | Eliminations | | | Total | |
| Assets: | | | | | | | | | | | | | | | | | | | | |
| At December 31, 2013: | | $ | 6,873,839 | | | $ | 4,178,091 | | | $ | 761,367 | | | $ | - | | | $ | 11,813,297 | |
| At December 31, 2012: | | $ | 4,938,954 | | | $ | 5,183,592 | | | $ | 8,702 | | | $ | - | | | $ | 10,131,248 | |
| | | | | | | | | | | | | | | | | | | | | |
| Assets acquired | | | | | | | | | | | | | | | | | | | | |
| Year ended December 31, 2013: | | $ | 221,902 | | | $ | 175,786 | | | $ | - | | | $ | - | | | $ | 397,688 | |
| Year ended December 31, 2012: | | $ | 29,263 | | | $ | 2,753,578 | | | $ | - | | | $ | - | | | $ | 2,773,450 | |
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 16 - COMMITMENTS AND CONTINGENCIES
Service contracts
The Company carries various service contracts on its office building for repairs, maintenance and inspections. Certain contracts are long term and non-cancellable. The Company’s future minimum payments under no cancellable service contracts by year from December 31, 2013 forward are approximately: 2014: $8,411; 2015: $16,835: total: $25,246.
Employment and Consulting Agreements
Subsequent to the end of 2013, the Company entered a formal five-year employment agreement (the “Agreement”) with Christian “Chris” Romandetti, dated March 20, 2014 and effective January 1, 2014, to serve as the Company’s President and Chief Executive Officer. See Note 19 – Subsequent Events for a description of the terms of the employment agreement.
Hanover|Elite
On October 2, 2013, the Company entered into a cancelable 12-month agreement to engage the services of Elite Financial Communications Group, LLC, d/b/a Hanover|Elite. The terms of the agreement provide for a monthly retainer of $6,000 for the first six months of services, which shall increase to $10,000 per month in months 7-12; and 300,000 shares of the Company’s common stock, subject to SEC Rule 144 restrictions, which shall be earned and issued quarterly as follows: 37,500 shares on January 3, 2014; 37,500 shares on April 3, 2014; 37,500 shares on July 3, 2014; and 187,500 shares on October 3, 2014.
As the Company’s investor and public relations counsel of record, Hanover|Elite will collaborate with management on developing, implementing and supporting a fully integrated corporate and shareholder communications platform; and generating meaningful awareness among and measurable support from the retail and institutional investment banking community for the Company, its compelling business plan and promising future growth potential. Jim Hock, Co-Managing Partner of Hanover|Elite and Co-Chairman of the National Investment Banking Association, will lead the IR/PR effort for the Company.
The Company has other consulting agreements with outside contractors, certain of whom are also Company stockholders. The Agreements are generally expire one year or less.
Litigation
From time to time, we may become involved in various lawsuits and legal proceedings which arise in the ordinary course of business. However, litigation is subject to inherent uncertainties, and an adverse result in these or other matters may arise from time to time that may harm our business. We are not aware of any such legal proceedings that we believe will have, individually or in the aggregate, a material adverse effect on our business, financial condition or operating results.
NOTE 17 – (LOSS) INCOME PER SHARE
The following table presents the computation of basic and diluted loss per share:
| | | 2013 | | | 2012 | |
| Net loss available for common shareholders | | $ | (4,704,303 | ) | | $ | (873,363 | |
| Basic net loss per share | | $ | (0.35 | ) | | $ | (0.07 | ) |
| Weighted average common shares outstanding-basic | | | 13,529,294 | | | | 12,644,784 | |
| Diluted net loss share | | $ | (0.35 | ) | | | (0.07 | ) |
| Weighted average common shares outstanding-Diluted | | | 13,529,294 | | | | 12,644,784 | |
During the year ended December 31, 2013 and 2012, common stock equivalents are not considered in the calculation of the weighted average number of common shares outstanding because they would be anti-dilutive, thereby decreasing the net loss per common share.
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 18 - INCOME TAXES
The Company has adopted Accounting Standards Codification subtopic 740-10, Income Taxes (“ASC 740-10”) which requires the recognition of deferred tax liabilities and assets for the expected future tax consequences of events that have been included in the financial statement or tax returns. Under this method, deferred tax liabilities and assets are determined based on the difference between financial statements and tax bases of assets and liabilities using enacted tax rates in effect for the year in which the differences are expected to reverse. Temporary differences primarily include stock compensation and other equity-related non-cash charges, capitalized financing costs, the basis difference of derivative liabilities and certain accruals.
Due to the reverse acquisition of First Choice Healthcare Solutions, Inc. by FCID Holdings, Inc. on December 29, 2010, the net operating loss carry forwards of First Choice Healthcare Solutions, Inc. incurred prior to that date may not be useable for income tax purposes. As through September 30, 2010 FCID Holdings, Inc. was inactive, and FCID Holdings, Inc.’s active subsidiary is a limited liability company and through September 30, 2010 passed no income through to FCID Holdings, Inc. for federal and state income tax purposes, FCID Holdings, Inc. through September 30, 2010 incurred no income tax at the corporate level.
At December 31, 2013, the Company has available for federal income tax purposes a net operating loss carry forward of approximately $1,400,000 that may be used to offset future taxable income. Components of deferred tax assets as of December 31, 2013 are comprised primarily of stock based compensation and debt discounts in connection with convertible notes. No income taxes were recorded on the earnings in 2013 and 2012 as a result of the utilization of any carry forwards.
Deferred net tax assets consist of the following at December 31, 2013 and 2012:
| | | 2013 | | | 2012 | |
| Deferred tax asset | | $ | 490,000 | | | $ | - | |
| Less valuation allowance | | | (490,000 | ) | | | (- | ) |
| Net deferred tax asset | | $ | 0 | | | $ | 0 | |
The provision for income taxes consists of the following:
| | | 2013 | | | 2012 | |
| Current tax (benefit) | | $ | - | | | $ | - | |
| Adjustment for prior year accrual | | | - | | | | (23,103 | ) |
| Net provision (benefit) | | $ | - | | | $ | (23,103 | ) |
The provision for Federal taxes differs from that computed by applying Federal statutory rates to the loss before any Federal income tax (benefit), as indicated in the following:
| | | 2013 | | | 2012 | |
| Federal statutory rate | | | 35.0 | % | | | 35.0 | % |
| State income taxes net of Federal benefit | | | - | | | | - | |
| | | | 35.0 | % | | | 35.0 | % |
The Company files income tax returns in the U.S. Federal jurisdiction, and various state jurisdictions. The Company is no longer subject to U.S. Federal, state and local, or non-U.S. income tax examinations by tax authorities for years before 2010.
The Company follows the provision of uncertain tax positions as addressed in FASB Accounting Standards Codification 740-10-65-1. The Company recognized no increase in the liability for unrecognized tax benefits. The Company has no tax position for which the ultimate deductibility is highly certain but for which there is uncertainty about the timing of such deductibility. The Company recognizes interest accrued related to unrecognized tax benefits in interest expense and penalties in operating expenses. No such interest or penalties were recognized during the periods presented. The Company had no accruals for interest and penalties at December 31, 2013 and 2012.
FIRST CHOICE HEALTHCARE SOLUTIONS, INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 19 - SUBSEQUENT EVENTS
Employment Agreement with Christian Romandetti
The Company entered a formal five-year employment agreement (the “Employment Agreement”) with Christian “Chris” Romandetti, dated March 20, 2014 and effective January 1, 2014, to serve as the Company’s President and Chief Executive Officer. Pursuant to the terms and conditions set forth in the Employment Agreement, Mr. Romandetti is entitled to receive an annual base salary of $250,000, which shall increase no less than 5% per annum for the term of the Employment Agreement.
Mr. Romandetti, upon successfully achieving annual revenue milestones, is entitled to receive a bonus equal to 10% of his salary when $7.1 million in total annual revenue is reported in a fiscal year scaling up to a bonus equal to 800% of his salary if and when $100 million in total annual revenue is reported in a fiscal year. If the Company is unable to pay any portion of the bonus compensation when due because of insufficient liquidity or applicable restrictions under prevailing debt financing agreements, then, as an accommodation to the Company, Mr. Romandetti shall be able to convert bonus compensation into shares of the Company’s common stock at a 30% discount to the average closing price during the first calendar month after the end of the fiscal year. Mr. Romandetti will also be entitled to receive a strategic bonus of $100,000, payable in cash, on the sixth month anniversary of opening each new center of excellence.
Pursuant to the Company achieving specific financial performance benchmarks established by the Board of Directors, Mr. Romandetti will also be entitled to receive a cashless option to purchase up to 1 million shares of common stock per year. The exercise price of the options will be the fair market value of the average closing price of the stock during the first calendar month after the end of the fiscal year. Mr. Romandetti shall have up to five years from the date of the annual option grant to exercise the option. In addition to the above compensation consideration, Mr. Romandetti will be entitled to receive annual restricted stock compensation equal to 100% of the total base salary and bonus compensation. The fair market value of the restricted stock grant shall be determined using the average closing price of the common stock during the first calendar month after the end of the fiscal year.
In addition, Mr. Romandetti’s Employment Agreement provides that, upon Mr. Romandetti’s death, disability, termination for any reason other than “Cause” (as such term is defined in the Employment Agreement) or resignation for “Good Reason” (as such term is defined in the Employment Agreement), the Company will pay to Mr. Romandetti twelve months of his annual base salary at the time of separation in accordance with the Corporation’s usual payroll practices.