Exhibit 3.62
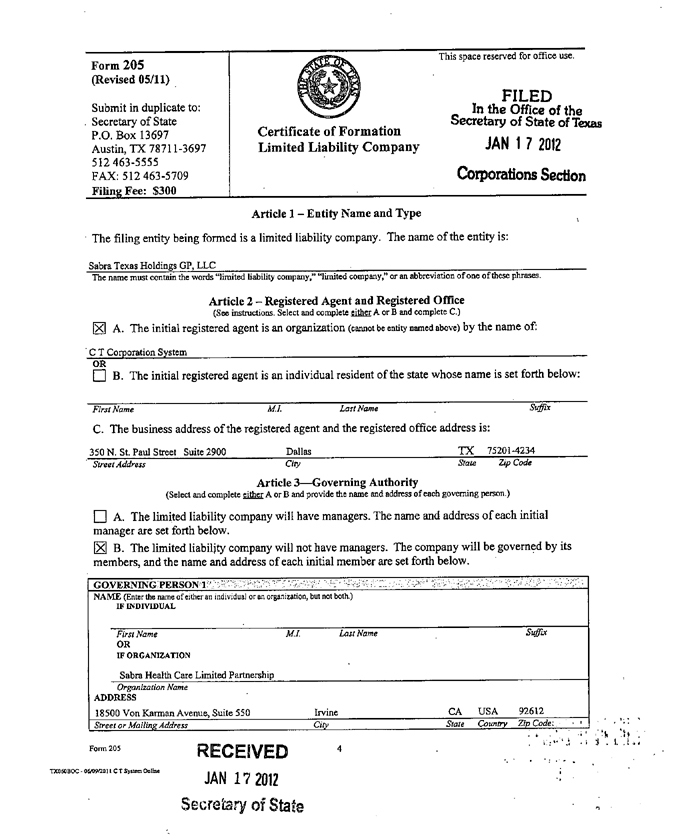
Form 205 This space reserved for office use.
(Revised 05/11)
Submit in duplicate to: FILED
In the Office of the
Secretary of State Certificate of Formation Secretary of State of Texas
P.O. Box 13697
Austin, TX 78711-3697 Limited Liability Company JAN 1 7 2012
512 463-5555 Corporations Section
FAX: 512 463-5709
Filing Fee: $300
Article 1—Entity Name and Type The filing entity being formed is a limited liability company. The name of the entity is:
Sabra Texas Holdings GP, LLC
The name must contain the words “limited liability company,” “limited company,” or an abbreviation of one of these phrases.
Article 2—Registered Agent and Registered Office
(See instructions. Select and complete either A or B and complete C.)
[Xl A. The initial registered agent is an organization (cannot be entity named above) by the name of:
C T Corporation System
OR
[ ] B. The initial registered agent is an individual resident of the state whose name is set forth below:
First Name M.1. Last Name Suffix
C. The business address of the registered agent and the registered office address is:
350 N. St. Paul Street Suite 2900 Dallas TX 75201-4234
Street Address City State Zip Code
Article 3—Governing Authority
(Select and complete either A or B and provide the name and address of each governing person.)
[ ] A. The limited liability company will have managers. The name and address of each initial manager are set forth below.
[X] B. The limited liability company will not have managers. The company will be governed by its members, and the name and address of each initial member are set forth below.
GOVERNING PERSON 1
NAME (Enter the name of cither an individual or an organization, but not both.) IF INDIVIDUAL
First Name M.I. Last Name OR
IF ORGANIZATION Suffix
Sabra Health Care Limited Partnership
Organization Name ADDRESS
18500 Von Karman Avenue, Suite 550 Irvine CA USA 92612
Street or Mailing Address City Slate Country Zip Code:
RECEIVED
TX060BOC • 06/09/2011 C T System Online JAN 17 2012
Secretary of State
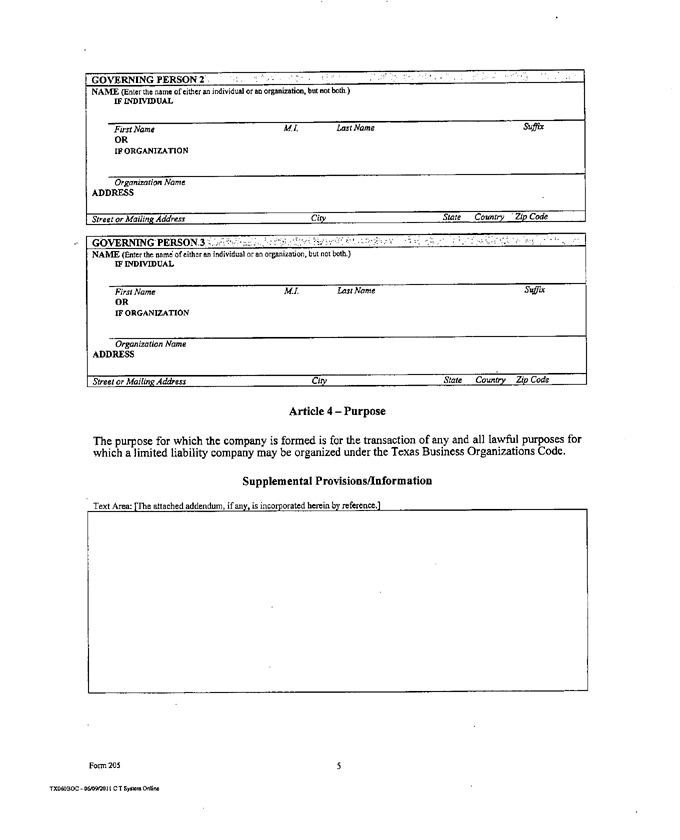
GOVERNING PERSON 2
NAME (Enter the name of either an individual or an organization but not both.)
IF INDIVIDUAL
First Name M.I. last Name Suffix
OR
IP ORGANIZATION
Organization Name
ADDRESS
Street or Mailing Address City State Country Zip Code
GOVERNING PERSON 3
NAME (Enter the name of either an individual or an organization but not both.)
IF INDIVIDUAL
First Name M.I. Last Name Suffix
OR
IF ORGANIZATION
Organization Name
ADDRESS
Street or Mailing Address City State Country Zip Code
Article 4—Purpose
The purpose for which the company is formed is for the transaction of any and all lawful purposes for which a limited liability company may be organized under the Texas Business Organizations Code.
Supplemental Provisions/Information
Text Area: [The attached addendum, if any, is incorporated herein by reference,]
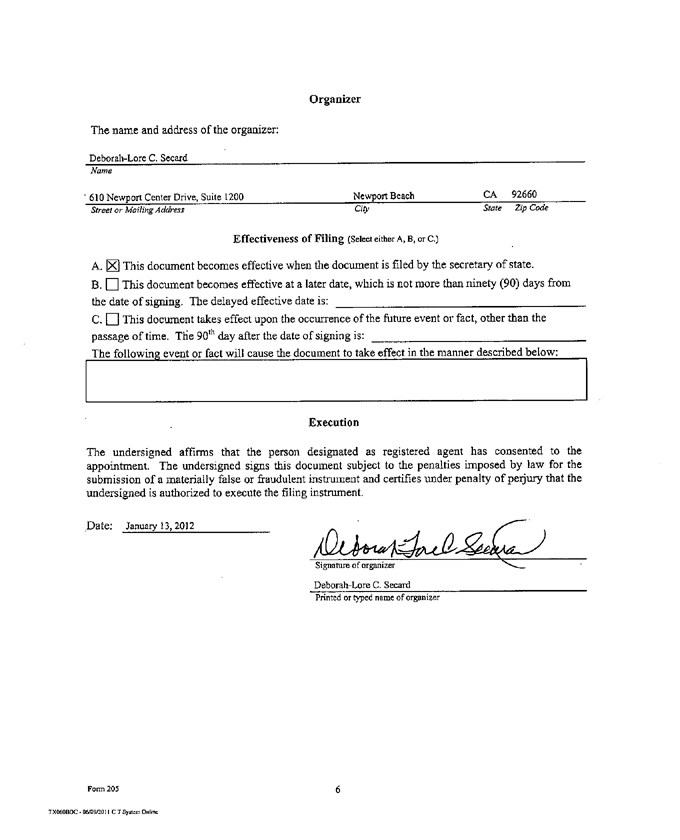
Organizer
The name and address of the organizer:
Deborah-Lore C. Secard
Name
610 Newport Center Drive, Suite 1200 Newport Beach CA 92660
Street or Mailing Address City State Zip Code
Effectiveness Of Filing (Select either A, B, or C.)
A. [X] This document becomes effective when the document is filed by the secretary of state.
B. ? This document becomes effective at a later date, which is not more than ninety (90) days from the date of signing. The delayed effective date is:
C. [ ] This document takes effect upon the occurrence of the future event or fact, other than the
passage of time. The 90th day after the date of signing is:
The following event or fact will cause the document to take effect in the manner described below:
Execution
The undersigned affirms that the person designated as registered agent has consented to the appointment. The undersigned signs this document subject to the penalties imposed by law for the submission of a materially false or fraudulent instrument and certifies under penalty of perjury that the undersigned is authorized to execute the filing instrument.
Date: January 13,2012
Signature of organizer
Deborah-Lore C. Secard
Printed or typed name of organizer