Table of Contents
As filed with the Securities and Exchange Commission on February 6, 2019
RegistrationNo. 333-229097
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
AMENDMENT NO. 2
to
FORMF-1
REGISTRATION STATEMENT
UNDER
THE SECURITIES ACT OF 1933
STEALTH BIOTHERAPEUTICS CORP
(Exact name of registrant as specified in its charter)
N/A
(Translation of Registrant’s Name into English)
| Cayman Islands | 2834 | Not Applicable | ||
(State or other jurisdiction of incorporation or organization) | (Primary Standard Industrial Classification Code Number) | (I.R.S. Employer Identification No.) |
Stealth BioTherapeutics Corp
c/o Intertrust Corporate Services (Cayman) Limited
190 Elgin Avenue, George Town
Grand Cayman
KY1-9005 Cayman Islands
(Address, including zip code, and telephone number, including
area code, of registrant’s principal executive offices)
Stealth BioTherapeutics Inc.
275 Grove Street, Suite3-107
Newton, MA 02466
(617)600-6888
(Name, address, including zip code, and telephone number,
including area code, of agent for service)
Copies to:
Steven D. Singer, Esq. Rosemary G. Reilly, Esq. Christopher D. Barnstable-Brown, Esq. Wilmer Cutler Pickering Hale and Dorr LLP 60 State Street Boston, MA 02109 Telephone:(617) 526-6000 | Brent B. Siler, Esq. Divakar Gupta, Esq. Richard C. Segal, Esq. Cooley LLP 1114 Avenue of the Americas New York, NY 10036 Telephone: (212)479-6000 |
Approximate date of commencement of proposed sale to the public:
As soon as practicable after this Registration Statement is declared effective.
If any of the securities being registered on this form are to be offered on a delayed or continuous basis pursuant to Rule 415 under the Securities Act of 1933, check the following box. ☐
If this form is filed to register additional securities for an offering pursuant to Rule 462(b) under the Securities Act, check the following box and list the Securities Act registration statement number of the earlier effective registration statement for the same offering. ☐
If this form is a post-effective amendment filed pursuant to Rule 462(c) under the Securities Act, check the following box and list the Securities Act registration statement number of the earlier effective registration statement for the same offering. ☐
If this form is a post-effective amendment filed pursuant to Rule 462(d) under the Securities Act, check the following box and list the Securities Act registration statement number of the earlier effective registration statement for the same offering. ☐
Indicate by check mark whether the registrant is an emerging growth company as defined in Rule 405 of the Securities Act of 1933.
Emerging Growth Company ☒
If an emerging growth company that prepares its financial statements in accordance with U.S. GAAP, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 7(a)(2)(B) of the Securities Act. ☐
CALCULATION OF REGISTRATION FEE
| ||||
TITLE OF EACH CLASS OF SECURITIES TO BE REGISTERED (1) | PROPOSED MAXIMUM PRICE(2) | AMOUNT OF REGISTRATION FEE(3)(4) | ||
Ordinary shares, $0.0003 par value per share | $99,820,000 | $12,099 | ||
| ||||
| ||||
| (1) | American depositary shares issuable upon deposit of the ordinary shares registered hereby have been registered under a separate registration statement on Form F-6 (Registration No. 333-229509). Each American depositary share represents 12 ordinary shares. |
| (2) | Estimated solely for the purpose of calculating the registration fee pursuant to Rule 457(o) under the Securities Act of 1933, as amended. Includes the aggregate offering price of additional ordinary shares to be delivered in the form of American depositary shares that the underwriters have the option to purchase. |
| (3) | Calculated pursuant to Rule 457(o) under the Securities Act of 1933, as amended, based on an estimate of the proposed maximum aggregate offering price. |
| (4) | The Registrant previously paid $10,453.50 in connection with the original filing of this Registration Statement. |
The Registrant hereby amends this Registration Statement on such date or dates as may be necessary to delay its effective date until the Registrant shall file a further amendment which specifically states that this Registration Statement shall thereafter become effective in accordance with Section 8(a) of the Securities Act of 1933 or until the Registration Statement shall become effective on such date as the Securities and Exchange Commission, acting pursuant to said Section 8(a), may determine.
Table of Contents
The information in this preliminary prospectus is not complete and may be changed. These securities may not be sold until the registration statement filed with the Securities and Exchange Commission is effective. This preliminary prospectus is not an offer to sell nor does it seek an offer to buy these securities in any jurisdiction where the offer or sale is not permitted.
SUBJECT TO COMPLETION, DATED FEBRUARY 6, 2019
PRELIMINARY PROSPECTUS
6,200,000 American Depositary Shares

Representing 74,400,000 Ordinary Shares
We are offering 6,200,000 American Depositary Shares, or ADSs, each representing 12 ordinary shares, $0.0003 par value per share, of Stealth BioTherapeutics Corp. This is our initial public offering, and no public market currently exists for our ADSs or ordinary shares. We expect the public offering price to be between $12.00 and $14.00 per ADS. We have applied to have the ADSs listed on The Nasdaq Global Market under the symbol “MITO.”
We are an “emerging growth company” as defined in Section 2(a) of the Securities Act of 1933, as amended, and will be subject to reduced public company reporting requirements. See “Prospectus Summary—Implications of Being an Emerging Growth Company.”
Investing in the ADSs involves a high degree of risk. See the “Risk Factors” section beginning on page 15 of this prospectus.
Neither the Securities and Exchange Commission nor any state securities commission has approved or disapproved of these securities or determined if this prospectus is truthful or complete. Any representation to the contrary is a criminal offense.
| PER ADS | TOTAL | |||||||
Initial Public Offering Price | $ | $ | ||||||
Underwriting Discounts and Commissions (1) | $ | $ | ||||||
Proceeds to Stealth BioTherapeutics Corp before expenses | $ | $ | ||||||
| (1) | See “Underwriting” beginning on page 194 for additional information regarding underwriting compensation. |
Our existing principal shareholder, Morningside Venture (I) Investments Limited, certain entities associated with it, certain of the holders of our outstanding convertible notes and entities associated with such holders have indicated an interest in purchasing up to an aggregate of approximately $60.0 million of ADSs in this offering at the initial public offering price and on the same terms as the other purchasers in this offering. However, because indications of interest are not binding agreements or commitments to purchase, these persons may determine to purchase fewer ADSs than they indicate an interest in purchasing or not to purchase any ADSs in this offering. It is also possible that these persons could purchase more ADSs in this offering. In addition, the underwriters could determine to sell fewer ADSs to any of these persons than they indicate an interest in purchasing or not to sell any ADSs to such persons. The underwriters will receive the same underwriting discount and commissions on these ADSs as they will on any other ADSs sold to the public in this offering.
Delivery of the ADSs is expected to be made on or about February , 2019. We have granted the underwriters an option for a period of 30 days from the date of this prospectus to purchase an additional 930,000 ADSs. If the underwriters exercise the option in full, the total underwriting discounts and commissions payable by us will be $ million, and the total proceeds to us, before expenses, will be $ million.
Joint Book-Running Managers
| Jefferies | Evercore ISI | BMO Capital Markets | ||
Lead Manager
Nomura
Prospectus dated February , 2019.
Table of Contents
| 1 | ||||
| 15 | ||||
SPECIAL NOTE REGARDING FORWARD-LOOKING STATEMENTS AND INDUSTRY DATA | 63 | |||
| 64 | ||||
| 66 | ||||
| 67 | ||||
| 69 | ||||
| 72 | ||||
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS | 74 | |||
| 89 | ||||
| 149 | ||||
| 162 | ||||
| 164 | ||||
| 166 | ||||
| 177 | ||||
| 187 | ||||
| 189 | ||||
| 194 | ||||
| 202 | ||||
| 203 | ||||
| 203 | ||||
| 203 | ||||
| 204 |
Through and including , 2019 (25 days after the date of this prospectus), all dealers that effect transactions in these securities, whether or not participating in this offering, may be required to deliver a prospectus. This delivery is in addition to a dealer’s obligation to deliver a prospectus when acting as an underwriter and with respect to an unsold allotment or subscription.
Neither we nor any of the underwriters have authorized anyone to provide any information or to make any representations other than those contained in this prospectus or in any free writing prospectuses we have prepared. We take no responsibility for, and can provide no assurance as to the reliability of, any other information that others may give you. We are offering to sell, and seeking offers to buy, ADSs only in jurisdictions where offers and sales are permitted. The information in this prospectus is accurate only as of the date of this prospectus, regardless of the time of delivery of this prospectus or any sale of ADSs. Our business, financial condition, results of operations and prospects may have changed since that date.
For investors outside the United States: Neither we nor any of the underwriters have done anything that would permit this offering or possession or distribution of this prospectus in any jurisdiction where action for that purpose is required, other than in the United States. Persons outside the United States who come into possession of this prospectus must inform themselves about, and observe any restrictions relating to, the offering of the ADSs and the distribution of this prospectus outside of the United States.
We are incorporated under the laws of the Cayman Islands as an exempted company with limited liability, and a majority of our outstanding securities are owned bynon-U.S. residents. Under the rules of the U.S. Securities and Exchange Commission, or the SEC, we are currently eligible for treatment as a “foreign private issuer.” As a foreign private issuer, we will not be required to file periodic reports and financial statements with the SEC as frequently or as promptly as domestic registrants whose securities are registered under the Securities Exchange Act of 1934, as amended, or the Exchange Act.
Table of Contents
This summary highlights selected information contained elsewhere in this prospectus and is qualified in its entirety by the more detailed information and financial statements included elsewhere in this prospectus. It does not contain all of the information that you should consider in making your investment decision. Before investing in the ADSs, you should carefully read this entire prospectus, including our consolidated financial statements and the related notes included elsewhere in this prospectus. You should also consider, among other things, the matters described under “Risk Factors” beginning on page 15. Except as otherwise indicated herein or as the context otherwise requires, references in this prospectus to “Stealth,” “the Company,” “we,” “us” and “our” refer to Stealth BioTherapeutics Corp and its consolidated subsidiaries, or any one or more of them as the context may require.
Overview
We are a clinical-stage biotechnology company focused on the discovery, development and commercialization of novel therapies for diseases involving mitochondrial dysfunction. Mitochondria, found in nearly every cell in the body, are the body’s main source of energy production and are critical for normal organ function. Dysfunctional mitochondria characterize a number of rare genetic diseases, collectively known as primary mitochondrial diseases, and are also involved in many commonage-related diseases. We believe our lead product candidate, elamipretide, has the potential to treat both rare genetic and commonage-related mitochondrial diseases. Our mission is to be the leader in mitochondrial medicine, and we have assembled a highly experienced management team, board of directors and group of scientific advisors to help us achieve this mission.
We are studying elamipretide in the following indications:
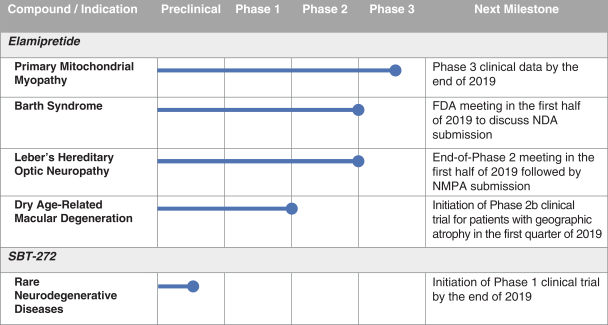
Primary mitochondrial myopathy.Primary mitochondrial myopathy, characterized by debilitating skeletal muscle weakness, exercise intolerance and fatigue, which we believe affects an estimated 40,000 diagnosed individuals in the United States. There are no therapies approved by the U.S. Food and Drug Administration, or the FDA, the European Medicines Agency, or the EMA, or the National Medical Products Association of China, or the NMPA, for the treatment of this indication. We have received Fast Track and Orphan Drug designations from the FDA for the development of elamipretide in this indication. We are conducting a Phase 3 pivotal trial in North America and Europe and expect to have data from that trial by the end of 2019.
Barth.Barth syndrome, or Barth, characterized by heart muscle weakness, or cardiomyopathy, neutropenia, or low white blood cell count (which may lead to an increased risk for infections), skeletal muscle weakness, delayed growth, fatigue and varying degrees of physical disability, is estimated to affect between one in 300,000 to one in 400,000 births in the United States and there are estimated to be less than 200 known living patients worldwide with Barth. There are no therapies approved by the FDA, EMA or NMPA for the treatment of Barth. We have received Fast Track and Orphan Drug designations from the FDA for the development of elamipretide in this indication. In December 2018, we completed the placebo-controlled portion of a Phase 2/3 clinical trial in patients with Barth. While the trial did not reach its primary endpoints, we observed trends toward improvement in the subset of patients with lower ratios of monolysocardiolipin to tetralinoleylcardiolipin, which we believe are the patients most likely to respond to therapy. We plan to meet with the FDA during the first half of 2019 to discuss a potential new drug application, or NDA, submission.
LHON. Leber’s hereditary optic neuropathy, or LHON, is characterized by central vision loss. We estimate that LHON affects approximately 10,000 individuals in the United States, of whom an estimated 70% have the genetic mutation, G11778A, that we are studying. There are no therapies approved by the FDA or NMPA for the treatment of LHON, and there is only oneEMA-approved therapy. We have received Fast Track and Orphan Drug designations from the FDA for the development of elamipretide in this indication. We completed the placebo-controlled portion of a Phase 2 clinical trial during the first half of 2018, and continue to follow patients in open-label extension. While the trial did not reach its primary endpoint of change in best corrected
1
Table of Contents
visual acuity, we observed trends favoring elamipretide across a number of endpoints, and we are continuing to observe improvements in an ongoing open-label extension. We plan to meet with the FDA for an end-of-Phase 2 meeting during the first half of 2019. Following that meeting, we plan to submit a clinical trial application to the NMPA for inclusion of clinical trial sites in China in a potential Phase 3 clinical trial.
Dry AMD. Dry acute macular degeneration, or dry AMD, characterized by symptoms such as distorted vision, reduction in low light visual acuity, reduced overall visual acuity and blurred vision, is estimated to affect over 10 million individuals in the United States and is the leading cause of blindness among older adults in the developed world. There are no therapies approved by the FDA, EMA or NMPA for the treatment of dry AMD. We completed a Phase 1 trial in patients with drusen, an early form of dry AMD, and geographic atrophy, an advanced form of dry AMD, in which we observed statistically significant improvement over baseline in various parameters of visual function in both the drusen and geographic atrophy cohorts. We received Fast Track designation from the FDA for the development of elamipretide for patients with dry AMD with geographic atrophy in November 2018. We plan to launch a Phase 2b clinical trial for the treatment of patients with geographic atrophy in the first quarter of 2019.
In addition to our clinical development programs for elamipretide, we plan to evaluateSBT-20, our second clinical-stage product candidate, for rare disease indications, such as peripheral neuropathies. We are developingSBT-272, a preclinical-stage product candidate, for rare neurodegenerative diseases. In addition, our internal discovery platform has generated a library of over 100 proprietary, differentiated compounds which could have clinical benefit for diseases related to mitochondrial dysfunction and from which we plan to designate potential product candidates. We may also utilize certain of these compounds as part of our “carrier platform,” in which they could serve as scaffolds to deliver other beneficial compounds to the mitochondria.
2
Table of Contents
Our Pipeline
The following table summarizes our development pipeline, including preclinical studies and ongoing and planned clinical trials of our product candidates we have advanced, or expect to advance in the next year, to clinical development.
We previously completed a Phase 1/2 clinical trial for the evaluation of SBT-20 in subjects with early-stage Huntington’s disease and a Phase 1 healthy volunteer study. We are currently evaluating preclinical disease models for the selection of an indication ahead of planning for a Phase 2 clinical trial.
Our Product Candidates
Elamipretide
Elamipretide is a small peptide that targets and binds reversibly to cardiolipin, stabilizing mitochondrial structure and function under conditions of oxidative stress. Elamipretide has been generally well-tolerated in over 900 people exposed to it systemically and 53 subjects exposed to it topically as of December 31, 2018.
We are evaluating elamipretide in primary mitochondrial diseases where there is a genetic basis for the underlying mitochondrial dysfunction and where we have the potential for expedited regulatory review, including primary mitochondrial myopathy, Barth and LHON. We also believe that elamipretide and our pipeline compounds may be able to address the significant unmet medical needs of larger populations affected by common diseases associated with aging. We are progressing our development of elamipretide for dry AMD, and we plan to evaluate clinical trials for other commonage-related disease indications in conjunction with our pipeline compounds.
SBT-20
SBT-20 is a small peptide that, like elamipretide, targets and binds reversibly to cardiolipin, stabilizing mitochondrial structure and function under conditions of oxidative stress.SBT-20 has been generally well-tolerated in 75 people exposed to it systemically as of December 31, 2018. Based on preclinical studies, we believe thatSBT-20 readily penetrates cell membranes and targets and binds reversibly to the inner membrane of mitochondria, or IMM. We plan to evaluateSBT-20 for rare peripheral neuropathies.
3
Table of Contents
SBT-272
SBT-272, our lead discovery pipeline compound, is among our novel peptides and peptidomimetics, which target the mitochondria and potentially improve mitochondrial function relative to our current product candidates as observed in non-clinical experiments. We are evaluating SBT-272 for rare neurodegenerative diseases, such as amyotrophic lateral sclerosis, or ALS.
Background on Mitochondrial Diseases
Mitochondria, found in almost all human cells, are the “powerhouse of the cell.” Normal mitochondrial function is essential for human life and for the proper functioning of many systems in our bodies. Mitochondria have their own DNA, called mitochondrial DNA, or mtDNA, which is inherited only from our mothers and is separate and distinct from nuclear DNA. Mitochondrial diseases arising from inherited genetic defects, called primary mitochondrial diseases, are typically rare diseases which can impact multiple organ systems within the body and may lead to reduced lifespan. Symptoms of primary mitochondrial disease, including chronic pain, vision problems, cardiovascular problems and kidney problems, may be compared to “accelerated aging” as described by individuals with the disease and their caregivers.
Although mtDNA is originally inherited from our mothers, it is replicated within cells as mitochondria reproduce and is highly susceptible to mutation within specific cells and organ systems as we age. Mitochondrial diseases arising from these spontaneous mutations in our mtDNA, called secondary mitochondrial diseases, include senescence, neurodegenerative diseases (such as Alzheimer’s disease, Parkinson’s disease and ALS), heart disease (such as heart failure and atherosclerosis), diabetes, ophthalmic conditions (such as AMD, glaucoma, diabetic retinopathy and diabetic macular edema), cancer, diabetes, skeletal muscle dysfunction (such as sarcopenia) and kidney diseases.
Mitochondrial dysfunction, whether inherited or acquired, often impacts high energy-demanding organs such as the skeletal muscle, cardiac, renal, visual, neurological, central nervous, circulatory or endocrine systems.
Our approach
Our product candidates target cardiolipin in the IMM, stabilizing it under conditions of oxidative stress. Cardiolipin is a conically shaped phospholipid that plays an important role in establishing the cristae architecture within the IMM and optimizing the function of the electron transport chain. Reduced and damaged cardiolipin content has been observed in many diseases, and a deficiency of normal cardiolipin is thought to be centrally involved in mitochondrial dysfunction.
Our lead product candidate, elamipretide, along with several of our pipeline compounds, target and bind reversibly to cardiolipin, stabilizing it under conditions of oxidative stress, thereby preserving the curved architecture of the IMM. We have focused our development efforts on diseases and conditions that affect the organs in the body that generate significant energy because of the high mitochondrial content found in the cells comprising these organs.
Our Strategy
We aim to continue the development of mitochondrial medicine to improve the lives of patients with unmet medical needs. There are no treatments approved by the FDA, the EMA or the NMPA for primary mitochondrial myopathy, Barth or dry AMD, and there are no FDA or NMPA approved treatments for LHON. We are pioneering the development of treatments for these diseases with unmet medical needs and believe we are well-positioned to be among the first to address these largely untapped markets in the United States, Europe and China. Although our initial development focus is on rare primary mitochondrial diseases, we believe that over the longer term there could be significant opportunities with regard to commonage-related diseases, including dry AMD. To achieve our objective, we intend to:
4
Table of Contents
Rapidly advance the clinical development of elamipretide in rare mitochondrial diseases
We are developing elamipretide for rare mitochondrial diseases, including primary mitochondrial myopathy, Barth and LHON. We have received Fast Track and Orphan Drug designations in the United States for each of these indications. We are enrolling subjects into our ongoing Phase 3 clinical trial for the treatment of primary mitochondrial myopathy, which we expect to have fully enrolled during the first half of 2019. We have completed the placebo-controlled portion of a Phase 2/3 clinical trial for the treatment of Barth and are continuing to evaluate efficacy endpoints during an open-label extension, in which all subjects are eligible to continue receiving elamipretide. Eight subjects are continuing in the open-label extension phase. We plan to meet with the FDA regarding this program during the first half of 2019 to discuss a potential NDA submission. We have completed the placebo-controlled portion of a Phase 2 clinical trial for the treatment of LHON and are continuing to evaluate efficacy endpoints during an open-label extension trial, in which all subjects are eligible to continue receiving the study drug. We plan to meet with the FDA for an end-of-Phase 2 meeting regarding this program during the first half of 2019.Following that meeting, we plan to submit a clinical trial application to the NMPA for inclusion of clinical sites in China in a potential Phase 3 clinical trial, which we believe may help expedite clinical trial enrollment. We will continue to evaluate development of elamipretide for additional rare disease indications.
Accelerate the clinical development of elamipretide for dry AMD
We are advancing development of elamipretide for dry AMD, anage-related disease, which is the leading cause of blindness in older adults. Dry AMD is estimated to impact approximately 10 million individuals in the United States and is the leading cause of blindness among older adults in the developed world. We received Fast Track designation in the United States for dry AMD with geographic atrophy in November 2018. Dry AMD would provide a significantly larger potential market size than our rare disease indications if we are able to successfully develop and commercialize elamipretide or one of our pipeline compounds for this indication. In our Phase 1 clinical trial of elamipretide, we observed evidence of clinical benefit for patients with dry AMD. We plan to initiate a Phase 2b placebo-controlled clinical trial for the treatment of patients with geographic atrophy, an advanced form of dry AMD, in the first quarter of 2019.
Expand clinical development efforts in China under new regulatory pathways
The prevalence of primary mitochondrial diseases, such as primary mitochondrial myopathy, Barth and LHON, is thought to be comparable in China to that in the United States because evidence suggests that prevalence does not vary by race or ethnicity for mitochondrial diseases. China has recently implemented policies to expedite regulatory pathways for rare diseases, including publication of a list of rare diseases that includes mitochondrial related diseases such as LHON. For primary mitochondrial myopathy, with respect to which we are currently conducting a pivotal trial in the United States and Europe, and Barth, we may apply to the NMPA for clinical trial waivers and expedited approval if and when we receive FDA approval for these indications. For LHON, we plan to submit a clinical trial application to the NMPA for the inclusion of Chinese clinical sites in our subsequent clinical trials, which may be used to support FDA approval. We believe that inclusion of Chinese sites may help expedite enrollment of clinical trials in rare diseases, as well as progress potential commercial collaboration opportunities for the China market for our product candidates, if approved.
Advance the development of pipeline mitochondrial medicines in rare diseases
We believe that our mitochondrial targeted product candidates may be beneficial in rare diseases involving mitochondrial dysfunction and hope to nominate compounds from our pipeline for select rare disease indications. We plan to evaluate our second clinical product candidate,SBT-20, for which we have completed two Phase 1 clinical safety trials in healthy volunteers, for rare peripheral neuropathies. We are evaluating our lead pipeline compound,SBT-272, for rare neurodegenerative diseases, such as ALS. We expect to initiate a Phase 1 clinical safety trial forSBT-272 by the end of 2019.
5
Table of Contents
Advance the development of pipeline mitochondrial medicines in commonage-related diseases
We believe that mitochondrial medicine may be a promising approach for many commonage-related diseases beyond AMD, including neurodegenerative diseases. We believe that the United States, Europe and China are important markets for the clinical development ofage-related diseases, and we are evaluating further development of our product candidates and pipeline compounds forage-related indications in these markets.
Expand our carrier platform
We have extensive experience in optimizing delivery of our compounds to the mitochondria, which has been a challenge for other drug delivery technologies. We have demonstrated capability to deliver beneficial “payloads” to mitochondria by conjugating them with our proprietary compounds, which serve as vectors or carriers to the mitochondria, conferring organelle specificity to promising therapies. These payloads could include small molecules, proteins, oligonucleotides and complex formulations, such as DNA, siRNA and miRNA, nanoparticles and liposomes. This delivery platform, which we call our carrier platform, could enable delivery of missing proteins or even gene therapy to address inherited mitochondrial disorders.
Explore potential strategic partnerships and alliances to maximize the value of our development programs
We hold worldwide exclusive licenses from the Cornell Research Foundation, Inc. and the Institut de recherches cliniques de Montréal for our two clinical-stage assets, elamipretide andSBT-20. We have full ownership of our preclinical compound library, includingSBT-272. We may explore select strategic partnerships and alliances to support our drug development programs, while preserving significant development and commercialization rights, if we believe that such alliances may allow us to leverage the financial support and therapeutic area expertise and resources of a strategic partner to accelerate the development and commercialization of our drug candidates, particularly in common disease indications. We plan to retain rights to lead the development and commercialization of elamipretide for primary mitochondrial myopathy, Barth, LHON and dry AMD in the United States but will consider collaborating in Europe and China.
Expand our intellectual property portfolio in the field of mitochondrial medicine
We continue to invest in our mitochondrial medicine discovery platform to identify new approaches to improve absorption, distribution, metabolism and excretion of active mitochondrial compounds. We have an active discovery and development program focused on novel compounds targeting mitochondria. We believe the differentiated mitochondrial targeting characteristics of our compounds, our development of proprietary assays to screen new compounds for mitochondrial targeting and activity characteristics, and our experience working with various models of mitochondrial dysfunction position us to be a leader in next generation development of mitochondrial product candidates that are improved relative to elamipretide and SBT-20. We intend to use our insight into mitochondrial biology to continue developing additional intellectual property as we pursue additional novel compounds that target mitochondrial disease. As of December 31, 2018, our intellectual property portfolio included 374 issued patents and 298 patent applications relating to mitochondrial medicine, either wholly-owned orin-licensed, in select commercially relevant jurisdictions, including the United States, key European countries, China, Japan and Canada.
Recent Developments
As of December 31, 2018, we had cash and cash equivalents of $10.9 million.
The information above is based on preliminary unaudited information and management estimates for the year ended December 31, 2018, is not a comprehensive statement of our financial results, and is subject to completion of our financial closing procedures. Our independent registered public accounting firm has not conducted an audit or review of, and does not express an opinion or any other form of assurance with respect to, this preliminary estimate.
6
Table of Contents
Risks Associated with Our Business
Our business is subject to a number of risks of which you should be aware before making an investment decision. These risks are discussed more fully in the “Risk Factors” section of this prospectus immediately following this prospectus summary. These risks include the following:
| ∎ | We have incurred significant losses since inception. We expect to incur losses for the foreseeable future and may never achieve or maintain profitability. As of September 30, 2018, we had an accumulated deficit of $399.7 million. |
| ∎ | We will need substantial additional funding. If we are unable to raise capital when needed, we would be forced to delay, reduce or eliminate our research and drug development programs or commercialization efforts. If we do raise additional capital, it may cause dilution to our shareholders. |
| ∎ | We depend heavily on the success of elamipretide, our lead product candidate, and we cannot be certain that we will receive regulatory approval for elamipretide or if we will successfully commercialize elamipretide even if we receive such regulatory approval. |
| ∎ | Our approach to the discovery and development of product candidates that target mitochondria is unproven, and we do not know whether we will be able to develop any drugs of commercial value. |
| ∎ | If clinical trials of our product candidates fail to demonstrate safety and efficacy to the satisfaction of regulatory authorities or do not otherwise produce positive results, we may incur additional costs or experience delays in completing, or ultimately be unable to complete, the development and commercialization of our product candidates. |
| ∎ | We expect to depend on third parties for the development, marketing and/or commercialization of our product candidates in some cases. If those collaborations are not successful, we may not be able to capitalize on the market potential of our product candidates. |
| ∎ | We hold exclusive licenses from Cornell Research Foundation and the Institut de recherches cliniques de Montréal for both of our clinical-stage product candidates, elamipretide andSBT-20. If these third parties terminate their agreements with us, our competitive position and our market share, will be harmed. For example, under our license agreement with Cornell, if we fail to commercialize a product by December 31, 2020, Cornell may terminate our license, subject to specified exceptions for causes due to scientific and regulatory events that are common in drug development, such as institutional review board delays, clinical trial recruitment, clinical trial results and regulatory delays, and other events over which we cannot exert direct control. |
| ∎ | Following completion of this offering, Morningside Venture (I) Investments Limited will beneficially own approximately 65.1% of our ordinary shares (or 63.3% if the underwriters exercise their option to purchase additional ADSs in full), without giving effect to any ADSs that may be purchased by it in this offering, assuming that we sell the number of ADSs set forth on the cover page of this prospectus, and will therefore continue to have substantial control over us after this offering, which could limit your ability to influence the outcome of key decisions and transactions involving us, including a change of control. |
| ∎ | Based on our cash balances, recurring losses and our projected spending in 2018, and without giving effect to the proceeds of this offering, there is a substantial doubt about our ability to continue as a going concern. |
| ∎ | As a foreign private issuer, we are exempt from a number of rules under the U.S. securities laws and Nasdaq Stock Market, or Nasdaq, corporate governance rules and are permitted to file less information with the Securities and Exchange Commission, or the SEC, than U.S. companies. This may limit the information available to holders of the ADSs. |
Corporate Information
Our registered office is located at c/o Intertrust Corporate Services (Cayman) Limited, 190 Elgin Avenue, George Town, Grand Cayman,KY1-9005 Cayman Islands. We have three wholly-owned subsidiaries: Stealth BioTherapeutics, Inc., a Delaware company, which we refer to as Stealth Delaware; Stealth BioTherapeutics
7
Table of Contents
(HK) Limited, a company incorporated with limited liability under the laws of Hong Kong; and Stealth BioTherapeutics (Shanghai) Limited, a limited liability company established in the People’s Republic of China. Our agent for service of process in the United States is Stealth Delaware, and the executive offices of Stealth Delaware are located at 275 Grove Street, Suite3-107, Newton, MA 02466, and the telephone number there is (617)600-6888. Our website address iswww.stealthbt.com. We have included our website address in this prospectus as an inactive textual reference only. The information contained in, or accessible through, our website does not constitute part of this prospectus.
Stealth BioTherapeutics Corp is a Cayman Islands company and we conduct our operations in the United States through Stealth Delaware. All of our employees are employed by Stealth Delaware.
“Stealth BioTherapeutics,” the Stealth BioTherapeutics logo and other trademarks or service marks of Stealth BioTherapeutics Corp appearing in this prospectus are the property of Stealth BioTherapeutics or our subsidiaries. This prospectus contains additional trade names, trademarks and service marks of others, which are the property of their respective owners. Solely for convenience, trademarks and trade names referred to in this prospectus may appear without the® or™ symbols.
Implications of Being an Emerging Growth Company
As a company with less than $1.07 billion in revenue during our last fiscal year, we qualify as an “emerging growth company” as defined in the Jumpstart Our Business Startups Act of 2012, or the JOBS Act. As an emerging growth company, we may take advantage of specified reduced disclosure and other requirements that are otherwise applicable generally to public companies. These provisions include:
| ∎ | only two years of audited financial statements, in addition to any required unaudited interim financial statements, with correspondingly reduced “Management’s Discussion and Analysis of Financial Condition and Results of Operations” disclosure; |
| ∎ | reduced disclosure about our executive compensation arrangements; |
| ∎ | exemption from thenon-binding advisory votes on executive compensation, including golden parachute arrangements; and |
| ∎ | exemption from the auditor attestation requirement in the assessment of our internal controls over financial reporting. |
Generally, we may take advantage of these exemptions for up to five years or such earlier time that we are no longer an emerging growth company. We would cease to be an emerging growth company if we have more than $1.07 billion in annual revenue, we have more than $700.0 million in market value of our shares held bynon-affiliates or we issue more than $1.0 billion ofnon-convertible debt over a three-year period. We may choose to take advantage of some, but not all, of the available exemptions. We have taken advantage of certain reduced reporting burdens in this prospectus. Accordingly, the information contained herein may be different than the information you receive from other public companies in which you hold securities.
In addition, the JOBS Act provides that an emerging growth company can take advantage of an extended transition period for complying with new or revised accounting standards. This allows an emerging growth company to delay the adoption of certain accounting standards until those standards would otherwise apply to private companies. We have elected to avail ourselves of this exemption from new or revised accounting standards and, therefore, we will not be subject to the same new or revised accounting standards as other public companies.
Implications of Being a Foreign Private Issuer
Our status as a foreign private issuer also exempts us from compliance with certain laws and regulations of the SEC and certain regulations of The Nasdaq Stock Market. Consequently, we are not subject to all of the disclosure requirements applicable to companies organized within the United States. For example, we are exempt from certain rules under the Exchange Act that regulate disclosure obligations and procedural requirements related to the solicitation of proxies, consents or authorizations applicable to a security registered
8
Table of Contents
under the Exchange Act. In addition, our senior management and supervisory board members are exempt from the reporting and “short-swing” profit recovery provisions of Section 16 of the Exchange Act and related rules with respect to their purchases and sales of our securities. Moreover, we are not required to file periodic reports and financial statements with the SEC as frequently or as promptly as U.S. public companies. Accordingly, there may be less publicly available information concerning our company than there is for U.S. public companies.
In addition, foreign private issuers are not required to file their annual report on Form20-F until 120 days after the end of each fiscal year, while U.S. domestic issuers that are accelerated filers are required to file their annual report on Form10-K within 75 days after the end of each fiscal year. Foreign private issuers are also exempt from the Regulation Fair Disclosure, aimed at preventing issuers from making selective disclosures of material information.
We may take advantage of these exemptions until such time as we no longer qualify as a foreign private issuer. In order to maintain our current status as a foreign private issuer, either a majority of our shares must be directly or indirectly owned of record bynon-residents of the United States, or a majority of our executive officers or directors may not be United States citizens or residents, more than 50% of our assets cannot be located in the United States and our business must be administered principally outside the United States.
9
Table of Contents
The Offering
ADSs offered by us | 6,200,000 ADSs |
ADSs to be outstanding following this offering | 6,200,000 ADSs (with each ADS representing 12 ordinary shares) |
Ordinary shares to be outstanding following this offering | 396,220,998 ordinary shares, or 407,380,998 ordinary shares if the underwriters exercise their option to purchase additional ADSs in full (including, in each case, ordinary shares represented by the ADSs offered by this prospectus) |
Option to purchase additional ADSs | The underwriters have an option for a period of 30 days from the date of this prospectus to purchase up to 930,000 additional ADSs. |
The ADSs | Each ADS represents 12 ordinary shares, par value $0.0003 per share. You will have the rights of an ADS holder or beneficial owner (as applicable) as provided in the deposit agreement among us, the depositary and holders and beneficial owners of ADSs from time to time. To better understand the terms of our ADSs, see “Description of American Depositary Shares.” We also encourage you to read the deposit agreement, the form of which is filed as an exhibit to the registration statement of which this prospectus forms a part. |
Depositary | Citibank, N.A. |
Use of proceeds | We intend to use the net proceeds from this offering, together with our existing cash and cash equivalents, to fund the continued development of elamipretide, to fund continued clinical development of discovery compounds, including SBT-272, and for working capital and other general corporate purposes. See “Use of Proceeds” for a more complete description of the intended use of proceeds from this offering. |
Risk factors | You should read the “Risk Factors” section of this prospectus for a discussion of factors to consider carefully before deciding to invest in the ADSs. |
Concentration of Ownership | Following the completion of this offering and without giving effect to any ADSs that may be purchased by it in the offering, Morningside Venture (I) Investments Limited will own 65.1% of our ordinary shares (or 63.3% if the underwriters exercise their option to purchase additional ADSs in full), assuming that we sell the number of ADSs set forth on the cover page of this prospectus. |
Proposed Nasdaq Global Market symbol | MITO |
The number of ordinary shares to be outstanding after this offering is based on 321,820,998 ordinary shares issued and outstanding as of December 31, 2018, giving effect to (i) the conversion of all outstanding Series A convertible preferred shares into 91,600,398 ordinary shares and (ii) the issuance of 161,732,652 ordinary shares upon the conversion of our outstanding convertible notes in an aggregate principal amount of
10
Table of Contents
$132.4 million, or the 2018 Notes, assuming an initial public offering price of $13.00 per ADS (the midpoint of the estimated price range set forth on the cover page of this prospectus), both of which will occur automatically upon the closing of this offering, and excluding:
| ∎ | 15,871,229 ordinary shares issuable upon exercise of share options outstanding as of December 31, 2018, at a weighted-average exercise price of $1.06 per share; |
| ∎ | 9,631,519 ordinary shares available for future issuance as of December 31, 2018 under our 2006 share incentive plan, which shares will cease to be available for issuance following the closing of this offering; |
| ∎ | 47,692,934 ordinary shares reserved for issuance, in connection with this offering, under our 2019 share incentive plan, which plan includes provisions that automatically increase the number of ordinary shares reserved for issuance thereunder each year; |
| ∎ | 3,972,565 ordinary shares reserved for issuance, in connection with this offering, under our 2019 employee share purchase plan, which plan includes provisions that automatically increase the number of ordinary shares reserved for issuance thereunder each year; and |
| ∎ | 461,538 ordinary shares issuable upon exercise of an outstanding warrant with an exercise price equal to $1.08 per share (based upon the assumed initial public offering price of $13.00 per ADS in this offering and reflected on an implied per ordinary share basis). |
Unless otherwise indicated, this prospectus reflects and assumes the following:
| ∎ | a one-for-three reverse share split that became effective on December 28, 2018 |
| ∎ | the conversion of all outstanding Series A convertible preferred shares into an aggregate of 91,600,398 ordinary shares; |
| ∎ | conversion of the 2018 Notes; |
| ∎ | no exercise of the outstanding options or warrant described above; |
| ∎ | no exercise by the underwriters of their option to purchase additional ADSs; and |
| ∎ | no purchases of ADSs by our existing shareholders in this offering. |
Upon the closing of this offering, the number of shares issued upon conversion of the 2018 Notes will be based upon the initial public offering price per ADS. Based upon an assumed initial public offering price of $13.00 per ADS (the midpoint of the estimated price range set forth on the cover page of this prospectus), assuming accrual of interest through February 20, 2019, the 2018 Notes will convert into an aggregate of 161,732,652 ordinary shares upon the closing of this offering. For illustrative purposes only, the table below shows the number of ordinary shares that would be issuable upon conversion of the 2018 Notes at various initial public offering prices per ADS and the resulting total number of outstanding ordinary shares, assuming accrual of interest through February 20, 2019.
Assumed Initial Public | Ordinary Shares Issuable upon Conversion of 2018 Notes | Total Ordinary Shares Outstanding After this Offering | ||
| $11.00 | 191,138,589 | 425,626,935 | ||
| $12.00 | 175,210,373 | 409,698,719 | ||
| $13.00 | 161,732,652 | 396,220,998 | ||
| $14.00 | 150,180,320 | 384,668,666 | ||
| $15.00 | 140,168,298 | 374,656,644 |
Our existing principal shareholder, Morningside Venture (I) Investments Limited, certain entities associated with it, certain of the holders of our outstanding convertible notes and entities associated with such holders have indicated an interest in purchasing up to an aggregate of approximately $60.0 million of ADSs in this offering at the initial public offering price and on the same terms as the other purchasers in this offering. Assuming an initial public offering price of $13.00 per ADS, these persons would purchase an aggregate of 4,615,385 of the 6,200,000
11
Table of Contents
ADSs offered in this offering based on these indications of interest. However, because indications of interest are not binding agreements or commitments to purchase, these persons may determine to purchase fewer ADSs than they indicate an interest in purchasing or not to purchase any ADSs in this offering. It is also possible that these persons could purchase more ADSs in this offering. In addition, the underwriters could determine to sell fewer ADSs to any of these persons than they indicate an interest in purchasing or not to sell any ADSs to such persons. The underwriters will receive the same underwriting discount and commissions on these ADSs as they will on any other ADSs sold to the public in this offering.
12
Table of Contents
Summary Consolidated Financial Information
We have derived the following summary of consolidated statement of operations data for the years ended December 31, 2016 and 2017 and the summary consolidated balance sheet data as of December 31, 2017 from our audited consolidated financial statements appearing elsewhere in this prospectus. We have derived the following consolidated statements of operations data for the nine months ended September 30, 2017 and 2018 and the consolidated balance sheet data as of September 30, 2018 from unaudited condensed consolidated financial statements included elsewhere in this prospectus. In the opinion of management, the unaudited condensed consolidated financial statements reflect all adjustments, which include normal recurring adjustments, necessary for a fair presentation of the consolidated financial statements. Historical results are not necessarily indicative of the results that may be expected in the future, and the results for the nine months ended September 30, 2018 are not necessarily indicative of the results that may be expected for the full fiscal year or any other period. The summary consolidated financial data set forth below should be read together with our consolidated financial statements and the related notes to those statements, as well as the sections of this prospectus captioned “Selected Consolidated Financial Data” and “Management’s Discussion and Analysis of Financial Condition and Results of Operations.”
| YEAR ENDED DECEMBER 31, | NINE MONTHS ENDED SEPTEMBER 30, | |||||||||||||||
| 2016 | 2017 | 2017 | 2018 | |||||||||||||
| (in thousands, except share and per share data) | ||||||||||||||||
Consolidated Statement of Operations Data: | ||||||||||||||||
Operating expenses: | ||||||||||||||||
Research and development | $ | 48,445 | $ | 63,220 | $ | 46,212 | $ | 41,758 | ||||||||
General and administrative | 13,403 | 16,500 | 12,937 | 12,541 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Total operating expenses | 61,848 | 79,720 | 59,149 | 54,299 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Loss from operations | (61,848 | ) | (79,720 | ) | (59,149 | ) | (54,299 | ) | ||||||||
Other income (expense), net | 799 | (3,190 | ) | (1,691 | ) | (15,824 | ) | |||||||||
|
|
|
|
|
|
|
| |||||||||
Net loss attributable to ordinary shareholders | $ | (61,049 | ) | $ | (82,910 | ) | $ | (60,840 | ) | $ | (70,123 | ) | ||||
|
|
|
|
|
|
|
| |||||||||
Net loss per share attributable to ordinary shareholders—basic and diluted (1) | $ | (0.90 | ) | $ | (1.21 | ) | $ | (0.89 | ) | $ | (1.02 | ) | ||||
|
|
|
|
|
|
|
| |||||||||
Weighted-average ordinary shares used in net loss per share attributable to ordinary shareholders—basic and diluted(1) | 68,165,325 | 68,472,262 | 68,471,469 | 68,474,614 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Pro forma net loss per share attributable to ordinary shareholders—basic and diluted (1) | $ | (0.43 | ) | $ | (0.24 | ) | ||||||||||
|
|
|
| |||||||||||||
Pro forma weighted-average ordinary shares used in net loss per share attributable to ordinary shareholders—basic and diluted (1) | 188,261,368 | 238,105,715 | ||||||||||||||
|
|
|
| |||||||||||||
| (1) | See Notes 2 and 15 to our audited consolidated financial statements and notes 2 and 13 to our unaudited interim condensed consolidated financial statements appearing elsewhere in this prospectus for further details on the calculation of basic and diluted net loss per share attributable to ordinary shareholders and pro forma basic and diluted net loss per share attributable to ordinary shareholders. |
13
Table of Contents
The following table sets forth summary consolidated balance sheet data as of September 30, 2018:
| ∎ | on an actual basis; |
| ∎ | on a pro forma basis to give effect to the conversion of all outstanding Series A convertible preferred shares into 91,600,398 ordinary shares; and |
| ∎ | on a pro forma as adjusted basis to give further effect to (i) the issuance of 161,732,652 ordinary shares upon the conversion of our outstanding convertible notes in an aggregate principal amount of $132.4 million, assuming an initial public offering price of $13.00 per ADS (the midpoint of the estimated price range set forth on the cover page of this prospectus), both of which will occur automatically upon the closing of this offering and (ii) our issuance and sale of 6,200,000 ADSs in this offering at an assumed initial public offering price of $13.00 per ADS, which is the midpoint of the range set forth on the cover page of this prospectus, after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us. |
| AS OF SEPTEMBER 30, 2018 | ||||||||||||
| ACTUAL | PRO FORMA | PRO FORMA AS ADJUSTED (1) | ||||||||||
| (in thousands) | ||||||||||||
Consolidated Balance Sheet Data: | ||||||||||||
Cash and cash equivalents | $ | 4,078 | $ | 4,078 | $ | 77,038 | ||||||
Working capital | (31,027 | ) | (31,027 | ) | 46,323 | |||||||
Net assets | (149,076 | ) | (149,076 | ) | 40,069 | |||||||
Total assets | 11,630 | 11,630 | 84,590 | |||||||||
Total Series A convertible preferred shares | 211,377 | — | — | |||||||||
Total accumulated deficit | (399,680 | ) | (399,680 | ) | (399,680 | ) | ||||||
Total shareholders’ (deficit) equity | (360,453 | ) | (149,076 | ) | 40,069 | |||||||
| (1) | The pro forma as adjusted information provided above is illustrative only and will depend on the actual initial public offering price and other terms of our initial public offering determined in connection with the pricing of this offering. Each $1.00 increase (decrease) in the assumed initial public offering price of $13.00 per ADS, which is the midpoint of the range set forth on the cover page of this prospectus, would increase (decrease) the pro forma as adjusted amount of each of cash and cash equivalents, working capital, total assets and total shareholders’ (deficit) equity by $5.8 million, assuming that the number of ADSs offered by us, as set forth on the cover page of this prospectus, remains the same and after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us. Each increase (decrease) of 1.0 million ADSs in the number of ADSs offered by us, as set forth on the cover page of this prospectus, would increase (decrease) the pro forma as adjusted amount of each of cash and cash equivalents, working capital, total assets and total shareholders’ (deficit) equity by $12.1 million, assuming no change in the assumed initial public offering price per ADS and after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us. |
14
Table of Contents
Investing in the ADSs involves a high degree of risk. Before you decide to invest in the ADSs, you should consider carefully the risks described below, together with the other information contained in this prospectus, including our consolidated financial statements and the related notes appearing at the end of this prospectus. We believe the risks described below are the risks that are material to us as of the date of this prospectus. If any of the following risks occur, our business, financial condition, results of operations and future growth prospects could be materially and adversely affected. In these circumstances, the market price of the ADSs could decline, and you may lose all or part of your investment.
Risks Related to Our Financial Position and Need for Additional Capital
We have incurred significant losses since inception and expect to incur significant and increasing losses for at least the next several years. We may never achieve or maintain profitability.
We have incurred significant annual net operating losses in every year since our inception. Our net losses were $61.0 million, $82.9 million and $70.1 million for the years ended December 31, 2016 and 2017 and nine months ended September 30, 2018, respectively. As of September 30, 2018, we had an accumulated deficit of $399.7 million. We expect to continue to incur significant and increasing operating losses for the foreseeable future, and we do not know whether or when we will become profitable. We have not generated any revenues from product sales, have not completed the development of any product candidates and may never have a product candidate approved for commercialization. We have financed our operations to date through the issuance of our ordinary shares and Series A convertible preferred shares and debt financings and have devoted substantially all of our financial resources and efforts to research and development, including preclinical studies and clinical development programs. Our net losses may fluctuate significantly from quarter to quarter and year to year. Net losses and negative cash flows have had, and will continue to have, an adverse effect on our shareholders’ deficit and working capital.
We anticipate that our expenses will increase substantially if and as we:
| ∎ | continue to develop and conduct clinical trials with respect to our lead product candidate, elamipretide, including our ongoing Phase 2 and 3 clinical trials, for the treatment of primary mitochondrial myopathy, Barth, LHON, and dry AMD and any future clinical trials; |
| ∎ | initiate and continue research and preclinical and clinical development efforts for our other product candidates, including SBT-20 andSBT-272; |
| ∎ | seek to identify and develop additional product candidates; |
| ∎ | seek regulatory and marketing approvals for our product candidates that successfully complete clinical trials, if any; |
| ∎ | establish sales, marketing, distribution and other commercial infrastructure in the future to commercialize various products for which we may obtain marketing approval, if any; |
| ∎ | require the manufacture of larger quantities of product candidates for clinical development and potentially commercialization; |
| ∎ | maintain, expand and protect our intellectual property portfolio; |
| ∎ | hire and retain additional personnel, such as clinical, quality control and scientific personnel; |
| ∎ | add operational, financial, management information systems and commercial personnel, including personnel to support our product development and help us comply with our obligations as a public company; and |
| ∎ | add property, equipment and physical infrastructure to support our research and development programs in the United States, Europe and China. |
Our ability to become and remain profitable depends on our ability to generate revenue. We do not expect to generate significant revenue unless and until we are, or any future collaborator is, able to obtain marketing approval for, and successfully commercialize, one or more of our product candidates. This will require our, or any of our future collaborators’, success in a range of challenging activities, including completing clinical trials of our product candidates, obtaining marketing approval for these product candidates, manufacturing, marketing and selling those
15
Table of Contents
products for which we, or any of our future collaborators, may obtain marketing approval, satisfying any post-marketing requirements and obtaining reimbursement for our products from private insurance or government payors. Because of the uncertainties and risks associated with these activities, we are unable to accurately predict the timing and amount of increased expenses, and if or when we might achieve profitability. We and any future collaborators may never succeed in these activities and, even if we do, or any future collaborators do, we may never generate revenues that are large enough for us to achieve profitability. Even if we do achieve profitability, we may not be able to sustain or increase profitability on a quarterly or annual basis. Our failure to become and remain profitable would decrease the value of our company and could impair our ability to raise capital, expand our business, maintain our research and development efforts, diversify our pipeline of product candidates or continue our operations. A decline in the value of our company could cause you to lose all or part of your investment.
We will need substantial additional funding. If we are unable to raise capital when needed, we may be forced to delay, reduce or eliminate our product development programs or commercialization efforts.
Developing pharmaceutical products, including conducting preclinical studies and clinical trials, is a very time-consuming, expensive and uncertain process that takes years to complete. We expect our expenses to increase in connection with our ongoing activities, particularly as we initiate new clinical trials of, initiate new research and preclinical development efforts for and seek marketing approval for our product candidates. In addition, if we obtain marketing approval for any of our product candidates, we may incur significant commercialization expenses related to product sales, marketing, manufacturing and distribution to the extent that such sales, marketing, manufacturing and distribution are not the responsibility of a future collaborator. Furthermore, following the completion of this offering, we expect to incur significant additional costs associated with operating as a public company. Accordingly, we will need to obtain substantial additional funding in connection with our continuing operations. If we are unable to raise capital when needed and on attractive terms, we may be forced to delay, reduce or eliminate our research and development programs or any future commercialization efforts.
We plan to use the net proceeds of this offering primarily to fund our ongoing research and development efforts, including our clinical development of elamipretide for rare disease indications and for dry AMD. We will be required to expend significant funds in order to advance the development of elamipretide, as well as any other product candidates we may develop in the future. In addition, while we may seek one or more collaborators for future development of our product candidates, and, in particular, may conduct any large Phase 3 clinical trials of elamipretide, such as those we would likely be required to conduct for common diseases such as dry AMD, in collaboration with one or more partners that would finance most of the associated costs, we may not be able to enter into a collaboration for any of our product candidates on suitable terms, or at all. In any event, the net proceeds of this offering and our existing cash and cash equivalents will not be sufficient to fund all of the efforts that we plan to undertake or to fund the completion of development of any of our product candidates. Accordingly, we will be required to obtain further funding through public or private equity offerings, debt financings, collaborations and licensing arrangements or other sources. Adequate additional financing may not be available to us on acceptable terms, or at all. Our failure to raise capital as and when needed would have a negative impact on our financial condition and our ability to pursue our business strategy.
We believe that the net proceeds from this offering, together with our existing cash and cash equivalents, will enable us to fund our operating expenses and capital expenditure requirements for the next 12 months. Our estimate as to how long we expect the net proceeds from this offering, together with our existing cash and cash equivalents, to be able to fund our operations is based on assumptions that may prove to be wrong, and we could use our available capital resources sooner than we currently expect. Further, changing circumstances, some of which may be beyond our control, could cause us to consume capital significantly faster than we currently anticipate, and we may need to seek additional funds sooner than planned. Our future funding requirements, both short-term and long-term, will depend on many factors, including:
| ∎ | scope, progress, timing, costs and results of our current and future clinical trials; |
| ∎ | research and preclinical development efforts for any future product candidates that we may develop; |
| ∎ | our ability to enter into and the terms and timing of any collaborations, licensing agreements or other arrangements; |
| ∎ | number of future product candidates that we pursue and their development requirements; |
16
Table of Contents
| ∎ | outcome, timing and costs of seeking regulatory approvals; |
| ∎ | costs of commercialization activities for any of our product candidates that receive marketing approval to the extent such costs are not the responsibility of any future collaborators, including the costs and timing of establishing product sales, marketing, distribution and manufacturing capabilities; |
| ∎ | subject to receipt of marketing approval, revenue, if any, received from commercial sales of our current and future product candidates; |
| ∎ | our headcount growth and associated costs as we expand our research and development and establish a commercial infrastructure; |
| ∎ | costs of preparing, filing and prosecuting patent applications, maintaining and protecting our intellectual property rights and defending against intellectual property related claims; and |
| ∎ | costs of operating as a public company. |
We have no history of commercializing pharmaceutical products, which may make it difficult to evaluate the prospects for our future viability.
We began operations in 2006 and initiated our first clinical trial in 2010. Our operations to date have been limited to financing and staffing our company and developing our technology and conducting preclinical research and clinical trials for our product candidates. We have not demonstrated an ability to obtain marketing approvals, manufacture a commercial scale product, or arrange for a third-party to do so on our behalf, or conduct sales and marketing activities necessary for successful product commercialization. Accordingly, you should consider our prospects in light of the costs, uncertainties, delays and difficulties frequently encountered by companies in the early stages of development, especially clinical-stage biopharmaceutical companies such as ours. Predictions about our future success or viability may not be as accurate as they could be if we had a longer operating history or a history of successfully developing and commercializing pharmaceutical products.
Our recurring losses and negative cash flows have raised substantial doubt regarding our ability to continue as a going concern.
Based on our cash balances, recurring losses and our projected spending, there is a substantial doubt about our ability to continue as a going concern. If we are unable to obtain sufficient capital in this offering, our business, financial condition and results of operations will be materially and adversely affected, and we will need to obtain alternative financing or significantly modify our operational plans to continue as a going concern. If we are unable to continue as a going concern, we might have to liquidate our assets and, the values we receive for our assets in liquidation or dissolution could be significantly lower than the values reflected in our consolidated financial statements. Further, even if we successfully complete and receive net proceeds from this offering, given our planned expenditures for the next several years, including, without limitation, expenditures in connection with our clinical trials of elamipretide,SBT-20 and other new compounds, we may conclude, in connection with the issuance of our consolidated financial statements for the year ending December 31, 2018 or any other subsequent period, that there is substantial doubt regarding our ability to continue as a going concern. In addition, our lack of cash resources and our potential inability to continue as a going concern may materially adversely affect the price of the ADSs and our ability to raise new capital or to enter into critical contractual relations with third parties.
Raising additional capital may cause dilution to our shareholders, including purchasers of ADSs in this offering, restrict our operations or require us to relinquish rights to our technologies or product candidates.
We expect that significant additional capital will be needed in the future to continue our planned operations. To the extent that we raise additional capital through the sale of ordinary shares, ADSs, convertible securities or other equity securities, our existing shareholders’ ownership interest may be substantially diluted, and the terms of these securities could include liquidation or other preferences and anti-dilution protections that could adversely affect your rights as a holder of ADSs. Additional debt financing, if available, would result in increased fixed payment obligations and may involve agreements that include restrictive covenants that limit our ability to take specific actions, such as incurring additional debt, making capital expenditures, creating liens, redeeming shares or declaring dividends, that could adversely impact our ability to conduct our business. For example, in connection with our term loan facility with Hercules Capital, Inc., or Hercules, we granted a security interest on all of our assets, excluding our intellectual property, and agreed to a negative pledge on our intellectual property. The term loan facility also contains restrictive covenants including, subject to certain exceptions, covenants that prohibit us from incurring additional indebtedness, creating any lien on our property, making investments, paying dividends or
17
Table of Contents
redeeming shares, transferring any material portion of our assets, merging with or acquiring another entity, entering into a transaction that will result in a change of control and making certain other corporate changes. Future debt securities or other financing arrangements could contain similar or more restrictive negative covenants. In addition, securing financing could require a substantial amount of time and attention from our management and may divert a disproportionate amount of their attention away fromday-to-day activities, which may adversely affect our management’s ability to oversee the development of our product candidates.
If we raise additional funds through collaborations or marketing, distribution or licensing arrangements with third parties, we may have to relinquish valuable rights to our technologies, future revenue streams or product candidates or grant licenses on terms that may not be favorable to us. If we are unable to raise additional funds when needed, we may be required to delay, limit, reduce or terminate our product development or future commercialization efforts or grant rights to develop and market product candidates that we would otherwise prefer to develop and market ourselves.
We have a significant amount of debt, which may affect our ability to operate our business and secure additional financing in the future.
As of September 30, 2018, we had $20.0 million of outstanding principal under our term loan facility with Hercules and an additional $20.0 million of available borrowings, subject to achievement of specified milestones. Beginning in December 2018, we are required to repay principal and interest on these borrowings in monthly installments through January 2021. Subject to the restrictions in this existing facility, we could incur additional indebtedness beyond our borrowings from Hercules.
Our outstanding indebtedness, including any additional indebtedness beyond our borrowings from Hercules, combined with our other financial obligations and contractual commitments, could have significant adverse consequences, including:
| ∎ | requiring us to dedicate a portion of our cash resources to the payment of interest and principal, reducing money available to fund working capital, capital expenditures, product development and other general corporate purposes; |
| ∎ | increasing our vulnerability to adverse changes in general economic, industry and market conditions; |
| ∎ | subjecting us to restrictive covenants that may reduce our ability to take certain corporate actions or obtain further debt or equity financing; |
| ∎ | limiting our flexibility in planning for, or reacting to, changes in our business and the industry in which we compete; and |
| ∎ | placing us at a competitive disadvantage compared to our competitors that have less debt or better debt servicing options. |
We may not have sufficient funds and may be unable to arrange for additional financing to pay the amounts due under our existing debt instruments. Failure to make payments or comply with other covenants under our existing debt instruments could result in an event of default and acceleration of amounts due. Additionally, under our loan and security agreement with Hercules, an occurrence that has a material adverse effect on our business, operations, properties, assets or financial condition, on the collateral, liens or priority of such liens or on our ability to perform under the terms of the loan or associated agreements is an event of default. If an event of default occurs and the lenders accelerate the amounts due, we may not be able to make accelerated payments, and the lenders could seek to enforce security interests in the collateral securing such indebtedness, which includes substantially all of our assets other than our intellectual property. In addition, the covenants under our credit facility, the pledge of our assets as collateral and the negative pledge with respect to our intellectual property could limit our ability to obtain additional debt financing.
Risks Related to the Discovery, Development and Commercialization of Our Product Candidates
Our approach to the discovery and development of product candidates and the development of therapies targeting mitochondria generally are unproven, and we do not know whether we will be able to develop any products of commercial value.
We are focused on discovering and developing therapies for diseases involving mitochondrial dysfunction, particularly by developing therapies that target mitochondria in order to normalize the function of dysfunctional
18
Table of Contents
mitochondria. While we believe that our approach may ultimately enable drug research and clinical development for mitochondrial diseases across a wide range of therapeutic areas, this approach is unproven. We have not yet succeeded and may never succeed in demonstrating efficacy and safety for any of our product candidates in later stage clinical trials or in obtaining marketing approval thereafter. For example, although we have conducted Phase 1 and Phase 2 clinical trials, we have not yet completed a Phase 3 clinical trial.
In addition, there are over 250 genetic mutations underlying numerous rare diseases collectively known as primary mitochondrial diseases. Our clinical trials for the treatment of primary mitochondrial myopathy required that subjects have genetic confirmation of primary mitochondrial disease. Participants in our ongoing Phase 3 clinical trial may have a different mix of genotypes than the subjects of our prior clinical trials, which could have an impact on the results of our Phase 3 clinical trial. However, we have agreed with the FDA that we will stratify patients in our ongoing Phase 3 clinical trial according to certain categories of genetic mutation, so that patients within the agreed categories of mutations will be evenly balanced as between elamipretide and placebo treatment. Furthermore, no products or therapies targeting mitochondrial dysfunction have ever obtained marketing approval from the FDA or the NMPA, and the EMA has approved one therapy to treat LHON (Raxone, or idebenone, made by Santhera Pharmaceuticals), which is the only approved therapy to treat any primary mitochondrial disease.
If we are unable to successfully discover and develop product candidates, our business prospects will be substantially harmed.
We are dependent on the success of elamipretide, our lead product candidate. If we are unable to complete the clinical development of, obtain marketing approval for or successfully commercialize this product candidate, either alone or with a collaborator, or if we experience significant delays in doing so, our business could be substantially harmed.
We have no products approved for sale and are investing a significant portion of our efforts and financial resources in the development of elamipretide for the treatment of rare primary mitochondrial diseases. Our prospects are substantially dependent on our ability, or the ability of any future collaborator, to develop, obtain marketing approval for and successfully commercialize elamipretide.
The success of elamipretide will depend on several factors, including the following:
| ∎ | successful recruitment of subjects, enrollment in and completion of our ongoing clinical trials; |
| ∎ | initiation and successful recruitment of subjects, enrollment in and completion of additional clinical trials; |
| ∎ | safety, tolerability and efficacy profiles that are satisfactory to the FDA or any comparable foreign regulatory authority for marketing approval; |
| ∎ | our ability to identify success criteria and endpoints for our clinical trials such that the FDA and other regulatory authorities will be able to determine the clinical efficacy and safety profile of any product candidates we may develop; |
| ∎ | timely receipt of marketing approvals from applicable regulatory authorities; |
| ∎ | the performance of our future collaborators, if any; |
| ∎ | the extent of any required post-marketing approval commitments to applicable regulatory authorities; |
| ∎ | establishment of supply arrangements with third-party raw materials suppliers and manufacturers; |
| ∎ | establishment of arrangements with third-party manufacturers to obtain finished drug products that are appropriately packaged for sale; |
| ∎ | obtaining and maintaining patent, trade secret protection and regulatory exclusivity, both in the United States and internationally; |
| ∎ | protection of our rights in our intellectual property portfolio; |
| ∎ | successful launch of commercial sales following any marketing approval; |
| ∎ | a continued acceptable safety profile following any marketing approval; |
| ∎ | accuracy of the estimates of the current and future number of patients with mitochondrial associated or inherited mitochondrial diseases; |
| ∎ | commercial acceptance by patients, the medical community and third-party payors following any marketing approval; and |
| ∎ | our ability to compete with other therapies targeting inherited mitochondrial diseases. |
19
Table of Contents
Many of these factors—including with respect to clinical development, the regulatory submission process, potential threats to our intellectual property rights and the manufacturing, marketing and sales efforts of any future collaborator—are beyond our control, and clinical development of product candidates is inherently risky and uncertain. For example, although we observed trends towards improvement in a certain subset of patients, our Phase 2/3 clinical trial in Barth failed to reach its primary efficacy endpoints. If we are unable to develop, receive marketing approval for and successfully commercialize elamipretide, on our own or with any future collaborator, or experience delays as a result of any of these factors or otherwise, our business could be substantially harmed.
Additionally, we are developing elamipretide for certain indications of the eye, including LHON and dry AMD. Our clinical trial for the treatment of LHON involved administration of elamipretide by use of topical drops, and our clinical trial for the treatment of dry AMD involved administration of elamipretide by subcutaneous injection. We are cognizant of the challenges of targeting back of eye diseases with topical drops. The human eye has evolved to protect itself by washing foreign substances such as eye drops from the surface, with tears capable of removing as much as 95% of an eye drop. The vitreous in the interior of the eye also poses a barrier to delivery of therapies from the front of the eye to the retina. Based on the results of our Phase 2 clinical trial of elamipretide for the treatment of LHON, which did not meet its primary endpoint of change in best corrected visual acuity over the 12-month double-blind portion of the trial, we will still consider topical drops for back of eye indications and may need to conduct additional studies to determine the appropriate dose.
We may not be successful in our efforts to identify or discover and develop additional potential product candidates.
A significant portion of the research that we are conducting involves the development of new therapeutic compounds targeting the mitochondria. The results we obtain in preclinical testing and early clinical trials may not be predictive of results that are obtained in later studies, and we may suffer significant setbacks in advanced clinical trials, even after seeing promising results in earlier studies. The drug discovery that we are conducting may not be successful in identifying compounds that have commercial value or therapeutic utility. Our discovery platform may initially show promise in identifying potential product candidates, yet fail to yield viable product candidates for clinical development or commercialization for a number of reasons, including:
| ∎ | compounds we develop may not demonstrate improved efficacy, safety or tolerability; |
| ∎ | potential product candidates may, on further study, be shown to have harmful side effects or other characteristics that indicate that they are unlikely to receive marketing approval and achieve market acceptance; |
| ∎ | competitors may develop alternative therapies that render our potential product candidatesnon-competitive or less attractive; or |
| ∎ | a potential product candidate may not be capable of being produced at an acceptable cost. |
Our research programs to identify new product candidates will require substantial technical, financial and human resources, and we may be unsuccessful in our efforts to identify new product candidates. If we are unable to identify suitable additional compounds for preclinical and clinical development, our ability to develop product candidates and obtain product revenues in future periods could be compromised, which could result in significant harm to our financial position and adversely impact the price of the ADSs.
We have never obtained marketing approval for a product candidate and we may be unable to obtain, or may be delayed in obtaining, marketing approval for any of our product candidates.
We have never obtained marketing approval for a product candidate. It is possible that the FDA may refuse to accept for substantive review any new drug applications, or NDAs, that we submit for our product candidates or may conclude after review of our data that our application is insufficient to obtain marketing approval of our product candidates. If the FDA does not accept or approve our NDAs for either of our most advanced product candidates, it may require that we conduct additional clinical, nonclinical or manufacturing validation studies and submit that data before it will reconsider our applications. Depending on the extent of these or any otherFDA-required studies, approval of any NDA or application that we submit may be delayed by several years, or may require us to expend more resources than we have available. It is also possible that additional studies, if performed and completed, may not be considered sufficient by the FDA to approve our NDAs.
Any delay in obtaining, or an inability to obtain, any marketing approvals would prevent us from commercializing our product candidates, generating revenues and achieving and sustaining profitability. If any of these outcomes occur,
20
Table of Contents
we may be forced to abandon our development efforts for our product candidates, which could significantly and materially harm our business.
Results of preclinical studies and early clinical trials may not be predictive of results of future clinical trials.
The outcome of preclinical studies and early clinical trials may not be predictive of the success of later clinical trials, and interim results of clinical trials do not necessarily predict success in future clinical trials. Many companies in the pharmaceutical and biotechnology industries have suffered significant setbacks in late-stage clinical trials after achieving positive results in earlier development, and we cannot be certain that we will not face similar setbacks. The design of a clinical trial can determine whether its results will support approval of a product and flaws in the design of a clinical trial may not become apparent until the clinical trial is well advanced. If our trial designs are not sufficient, our ophthalmic programs may be delayed or we may decide to terminate one or more of such programs.
We have limited experience in designing clinical trials and may be unable to design and execute a clinical trial to support marketing approval. In addition, preclinical and clinical data are often susceptible to varying interpretations and analyses. During the regulatory review process, we will need to identify success criteria and endpoints at the time of the initiation of the trial such that the FDA or other regulatory authorities will be able to determine the clinical efficacy and safety profile of any product candidates we may develop, and the resulting clinical data and results may be difficult to analyze. Even if the FDA or other regulatory authorities were to find our success criteria to be sufficiently validated and clinically meaningful, we may not achieve thepre-specified endpoints to a degree of statistical significance. Many companies that believed that their product candidates had performed satisfactorily in preclinical studies and clinical trials nonetheless failed to obtain marketing approval of their product candidates. Even if we, or any future collaborators, believe that the results of clinical trials for our product candidates warrant marketing approval, the FDA or comparable foreign regulatory authorities may disagree and may not grant marketing approval of our product candidates.
In some instances, there can be significant variability in safety or efficacy results between different clinical trials of the same product candidate due to numerous factors, including changes in trial procedures set forth in protocols, differences in the size and type of the patient populations, changes in and adherence to the dosing regimen and other clinical trial protocols and the rate of dropout among clinical trial participants. Specifically, the clinical trials we have completed to date have enrolled only small numbers of subjects, we have experienced dropout among participants and we have not always successfully achieved ourpre-specified clinical trial endpoints to a degree of statistical significance.
To date, we have conducted small Phase 1 and Phase 2 clinical trials, many of which have been undertaken to help inform our clinical strategy and develop later stage clinical trials intended to assess efficacy. While the endpoints and populations for these later stage clinical trials, including Phase 3 clinical trials that we are planning, are derived from results of our earlier trials and medical literature, in our prior clinical trials we did not demonstrate a statistically significant effect in the population and on the efficacy endpoints prospectively described in the clinical trial protocol. The lack of statistical significance could be attributed to various factors, including the lack of power to demonstrate significance, the design of the studies or the lack of a treatment benefit from our product candidate. In some cases, we conducted post hoc, retrospective analyses of data subsets and have designed, and expect to design planned, later clinical trials based on the results of such post hoc analyses. For example, in our Phase 2 clinical trial for the treatment of primary mitochondrial myopathy, in the elamipretide-treated group, we observed an improvement on the primary endpoint of improvement in distance walked in six minutes (the six minute walk test, or 6MWT) relative to the placebo-treated group, which was not statistically significant, and our Phase 1/2 clinical trial for the treatment of primary mitochondrial myopathy did not demonstrate statistically significant changes in the high-dose versus placebo comparison of 6MWT results at day five pursuant to the primary statistical analysis model specified in the statistical analysis plan. We conducted an exploratory post hoc analysis of the results from this Phase 1/2 clinical trial primarily to assess, among other things, whether there was a potentially confounding cohort effect in the placebo group, which could occur if subjects randomized to placebo within higher-dose cohorts performed better due to the placebo effect of knowing they were randomized within a higher-dose cohort. This post hoc analysis showed a significant mean improvement from baseline insix-minute walk distance after five days of treatment, as adjusted for gender and baseline distance, for individuals treated with the high dose of elamipretide compared to placebo-treated individuals. The design of our Phase 3 clinical trial for the treatment of mitochondrial myopathy was informed, in part, by the results of this post hoc analysis.
21
Table of Contents
If we fail to receive positive results in clinical trials of our product candidates and do not achieve statistical significance for the prospectively specified primary endpoints in our planned Phase 3 clinical trials, the development timeline and regulatory approval and commercialization prospects for our most advanced product candidates, and, correspondingly, our business and financial prospects, would be negatively impacted.
Because we are developing elamipretide for the treatment of several indications for which regulatory authorities have not issued definitive guidance as to how to measure and demonstrate efficacy, there is substantial risk that the design or outcomes of our clinical trials will not be satisfactory to support marketing approval.
We are developing elamipretide for several indications for which there is currently no approved therapy in the United States, China or the European Union, including primary mitochondrial myopathy, Barth, and dry AMD. We are developing elamipretide for LHON, for which there are no currently approved therapies in the United States or China and only one therapy approved in Europe. Furthermore, there has been limited historical clinical trial experience for the development of drugs to treat many of these indications. As a result, the design and conduct of clinical trials for these indications is subject to substantial risk. In particular, regulatory authorities in the United States and in other jurisdictions, including Europe and China, have not issued definitive guidance as to how to measure and demonstrate efficacy for primary mitochondrial myopathy, Barth, LHON or dry AMD and, as a result, there is substantial risk that the design or outcomes of our clinical trials will not be satisfactory to support marketing approval. For example, the endpoints in our Phase 2/3 clinical trial of elamipretide for the treatment of Barth syndrome included change insix-minute walk distance and change in a total fatigue scale, or BTHSA Total Fatigue, from the Barth symptom assessment, or BTHSA, a newly developed patient reported outcome measure, which has not been utilized in prior trials and may not be accepted by regulators as a basis for approval. Even if this type of novel endpoint is accepted as a basis for approval in the United States, we cannot be certain that regulators outside of the United States will accept such endpoints or will not require us to conduct additional validation studies to support the suitability of such endpoints for approval in these jurisdictions.
We may expend our limited resources to pursue a particular product candidate or indication and fail to capitalize on product candidates or indications that may be more profitable or for which there is a greater likelihood of success.
Because we have limited financial and managerial resources, we intend to focus on developing product candidates for specific indications that we identify as most likely to succeed, in terms of both their potential for marketing approval and commercialization. As a result, we may forego or delay pursuit of opportunities with other product candidates or for other indications that may prove to have greater commercial potential.
Our resource allocation decisions may cause us to fail to capitalize on viable commercial products or profitable market opportunities. Our spending on current and future research and development programs and product candidates for specific indications may not yield any commercially viable product candidates. If we do not accurately evaluate the commercial potential or target market for a particular product candidate, we may relinquish valuable rights to that product candidate through collaboration, licensing or other royalty arrangements in cases in which it would have been more advantageous for us to retain sole development and commercialization rights to the product candidate.
Clinical drug development involves a lengthy and expensive process with an uncertain outcome.
Clinical testing is expensive, time-consuming and uncertain as to outcome. We cannot guarantee that any clinical trials will be conducted as planned or completed on schedule, or at all. The clinical development of our product candidates is susceptible to the risk of failure at any stage of drug development, including failure to demonstrate efficacy in a clinical trial or across a broad population of patients, the occurrence of adverse events that are severe or medically or commercially unacceptable, failure to comply with protocols or applicable regulatory requirements and determination by the FDA or any comparable foreign regulatory authority that a product candidate may not continue development or is not approvable. For example, Phase 3 clinical trials for common diseases associated with aging, such as dry AMD, would likely require a large number of subjects to be enrolled, which would cause any such trial to be very expensive. Moreover, it is possible that even if one or more of our product candidates has a beneficial effect, that effect will not be detected during clinical evaluation as a result of one or more of a variety of factors, including the size, duration, design, measurements, conduct or analysis of our clinical trials. Conversely, as a result of the same factors, our clinical trials may indicate an apparent positive effect of a product candidate that is greater than the actual positive effect, if any. Similarly, in our clinical trials we may fail to detect toxicity of or intolerability caused by our product candidates, or mistakenly believe that our product candidates are toxic or not well tolerated when that is not in fact the case. Many companies in the pharmaceutical and biotechnology industries have suffered
22
Table of Contents
significant setbacks in late-stage clinical trials after achieving positive results in earlier development, and we cannot be certain that we will not face additional setbacks. It is possible that any of our development programs may be placed on full or partial clinical hold by regulatory authorities at any point, which would delay and possibly prevent further development of our product candidates.
If clinical trials of our product candidates fail to satisfactorily demonstrate safety and efficacy to the FDA and other comparable foreign regulators, we, or any future collaborators, may incur additional costs or experience delays in completing, or ultimately be unable to complete, the development and commercialization of these product candidates.
We, and any future collaborators, are not permitted to commercialize, market, promote or sell any product candidate in the United States without obtaining marketing approval from the FDA. Comparable foreign regulatory authorities impose similar restrictions. We, and any future collaborators, may never receive such approvals. We, and any future collaborators, must complete extensive preclinical development and clinical trials to demonstrate the safety and efficacy of our product candidates in humans before we, or they, will be able to obtain these approvals.
Clinical testing is expensive, difficult to design and implement, can take many years to complete and is inherently uncertain as to outcome. We have not previously submitted an NDA to the FDA or similar drug approval filings to comparable foreign regulatory authorities for any of our product candidates. Any inability to complete preclinical and clinical development successfully could result in additional costs to us, or any future collaborators, and impair our ability to generate revenues from product sales, regulatory and commercialization milestones and royalties. Moreover, if (i) we, or any future collaborators, are required to conduct additional clinical trials or other testing of our product candidates beyond the trials and testing that we or they contemplate, (ii) we, or any future collaborators, are unable to successfully complete clinical trials of our product candidates or other testing, (iii) the results of these trials or tests are unfavorable, uncertain or are only modestly favorable, or (iv) there are unacceptable safety concerns associated with our product candidates, we, or any future collaborators, may:
| ∎ | be delayed in obtaining marketing approval for our product candidates; |
| ∎ | not obtain marketing approval at all; |
| ∎ | obtain approval for indications or patient populations that are not as broad as intended or desired; |
| ∎ | obtain approval with labeling that includes significant use or distribution restrictions or significant safety warnings, including boxed warnings; |
| ∎ | be subject to additional post-marketing testing or other requirements; or |
| ∎ | be required to remove the product from the market after obtaining marketing approval. |
Adverse events or undesirable side effects caused by, or other unexpected properties of, any of our product candidates may be identified during development that could delay or prevent their marketing approval or limit their use.
Adverse events or undesirable side effects caused by, or other unexpected properties of, our product candidates could cause us, any future collaborators, an institutional review board or regulatory authorities to interrupt, delay or halt clinical trials of one or more of our product candidates and could result in a more restrictive label or the delay or denial of marketing approval by the FDA or comparable regulatory authorities. If any of our product candidates is associated with adverse events or undesirable side effects or has properties that are unexpected, we, or any future collaborators, may need to abandon development or limit development of that product candidate to certain uses or subpopulations in which the undesirable side effects or other characteristics are less prevalent, less severe or more acceptable from a risk-benefit perspective. For example, subjects in certain of our clinical trials have reported adverse events arising from reaction at the injection site and some subjects have withdrawn as a result. Moreover, laboratory findings have demonstrated mild to moderate elevations in eosinophils beginning at approximately three to four weeks after initiation of elamipretide treatment, although these have not been reported to be associated with any systemic clinical manifestations of eosinophilia and in general were demonstrated to have returned to within normal range or to baseline levels after withdrawal of elamipretide therapy and, in most subjects, to decrease to within normal range after approximately 16 weeks of elamipretide therapy (and without withdrawal of therapy). In addition, we observed a mean increase in certain liver enzymes in subjects who received the highest dose ofSBT-20 in our Phase 1 clinical trial, although the principal investigator determined that no individual increases in such liver enzymes were clinically significant and although similar increases were not observed in the highest dose cohort of a prior Phase 1/2 clinical trial of SBT-20. Many compounds that initially showed promise in clinical or earlier stage testing have later been found to cause undesirable or unexpected side effects that prevented further development of
23
Table of Contents
the compound. If we, or any future collaborators, experience any of a number of possible unforeseen events in connection with clinical trials of our product candidates, potential marketing approval or commercialization of our product candidates could be delayed or prevented.
We, or any future collaborators, may experience numerous unforeseen events during, or as a result of, clinical trials that could delay or prevent marketing approval or commercialization of our product candidates, including:
| ∎ | clinical trials of our product candidates may produce unfavorable or inconclusive results; |
| ∎ | we, or any future collaborators, may decide, or regulators may require us or them, to conduct additional clinical trials or abandon product development programs; |
| ∎ | the number of subjects required for clinical trials of our product candidates may be larger than we, or any future collaborators, anticipate, subject enrollment in these clinical trials may be slower than we, or any future collaborators, anticipate or participants may drop out of these clinical trials at a higher rate than we, or any future collaborators, anticipate; |
| ∎ | the cost of planned clinical trials of our product candidates may be greater than we anticipate; |
| ∎ | our third-party contractors or those of any future collaborators, including those manufacturing our product candidates or components or ingredients thereof or conducting clinical trials on our behalf or on behalf of any future collaborators, may fail to comply with regulatory requirements or meet their contractual obligations to us or any future collaborators in a timely manner, or at all; |
| ∎ | regulators or institutional review boards may not authorize us, any future collaborators or our or their investigators to commence a clinical trial or conduct a clinical trial at a prospective trial site; |
| ∎ | we, or any future collaborators, may have delays in reaching or fail to reach agreement on acceptable clinical trial contracts or clinical trial protocols with prospective trial sites; |
| ∎ | subjects that enroll in a clinical trial may misrepresent their eligibility to do so or may otherwise not comply with the clinical trial protocol, resulting in the need to drop the subjects from the clinical trial, increase the needed enrollment size for the clinical trial or extend the clinical trial’s duration; |
| ∎ | we, or any future collaborators, may have to delay, suspend or terminate clinical trials of our product candidates for various reasons, including a finding that the participants are being exposed to unacceptable health risks, undesirable side effects or other unexpected characteristics of the product candidate; |
| ∎ | regulators or institutional review boards may require that we, or any future collaborators, or our or their investigators suspend or terminate clinical research for various reasons, including noncompliance with regulatory requirements or their standards of conduct, a finding that the participants are being exposed to unacceptable health risks, undesirable side effects or other unexpected characteristics of the product candidate or findings of undesirable effects caused by a chemically or mechanistically similar drug or drug candidate; |
| ∎ | the FDA or comparable regulatory authorities may disagree with our, or any future collaborators’, clinical trial designs or our or their interpretation of data from preclinical studies and clinical trials; |
| ∎ | the FDA or comparable regulatory authorities may fail to approve or subsequently find fault with the manufacturing processes or facilities of third-party manufacturers with which we, or any future collaborators, enter into agreements for clinical and commercial supplies; |
| ∎ | the supply or quality of raw materials or manufactured product candidates or other materials necessary to conduct clinical trials of our product candidates may be insufficient, inadequate or not available at an acceptable cost, or we may experience interruptions in supply; and |
| ∎ | the approval policies or regulations of the FDA or comparable regulatory authorities may significantly change in a manner rendering our clinical data insufficient to obtain marketing approval. |
Product development costs for us, or any future collaborators, will increase if we, or they, experience delays in testing or pursuing marketing approvals and we, or they, may be required to obtain additional funds to complete clinical trials and prepare for possible commercialization of our product candidates. We do not know whether any preclinical tests or clinical trials will begin as planned, will need to be restructured, or will be completed on schedule, or at all. Significant preclinical or clinical trial delays also could shorten any periods during which we, or any future collaborators, may have the exclusive right to commercialize our product candidates or allow our
24
Table of Contents
competitors, or the competitors of any future collaborators, to bring products to market before we, or any future collaborators, do and impair our ability, or the ability of any future collaborators, to successfully commercialize our product candidates and may harm our business and results of operations. In addition, many of the factors that lead to clinical trial delays may ultimately lead to the denial of marketing approval of any of our product candidates.
If we, or any future collaborators, experience delays or difficulties in the enrollment of subjects in clinical trials, our or their receipt of necessary regulatory approvals could be delayed or prevented.
We, or any future collaborators, may not be able to initiate or continue clinical trials for any of our product candidates if we, or they, are unable to locate and enroll a sufficient number of eligible subjects to participate in clinical trials as required by the FDA or comparable regulatory authorities. For example, we are developing elamipretide for the treatment of several rare diseases with small patient populations, such as Barth. Enrollment is a significant factor in the timing of clinical trials, and is affected by many factors, including:
| ∎ | the size and nature of the patient population; |
| ∎ | the severity of the disease under investigation; |
| ∎ | the proximity of subjects to clinical sites; |
| ∎ | the eligibility criteria for the trial; |
| ∎ | the design of the clinical trial; |
| ∎ | efforts to facilitate timely enrollment; |
| ∎ | competing clinical trials; and |
| ∎ | clinician and patient perception as to the potential advantages and risks of the drug being studied in relation to other available therapies, including any new drugs that may be approved for the indications we are investigating. |
Our inability, or the inability of any future collaborators, to enroll a sufficient number of subjects for our, or their, clinical trials could result in significant delays or may require us or them to abandon one or more clinical trials altogether. For example, our Phase 2a clinical trial of elamipretide in subjects pre-treated prior to a renal angioplasty was terminated early due to recruitment challenges after enrolling only 14 subjects of the 28 originally planned. In our Phase 3 clinical trial of elamipretide for the treatment of primary mitachondrial myopathy, we aim to enroll 200 subjects, all of whom were required to be enrolled in our pre-trial registry. Of the over 400 subjects in the pre-trial registry, 69 are located in Italy, where we are in discussions with regulators for authorization to use our pen injector in the Phase 3 clinical trial. If we are unable to obtain such authorization, the enrollment in our Phase 3 clinical trial may be delayed or otherwise adversely impacted. Enrollment delays in clinical trials may result in increased development costs for our product candidates, delay or halt the development of and approval processes for our product candidates and jeopardize our, or any future collaborators’, ability to commence sales of and generate revenues from our product candidates, which could cause the value of our company to decline.
If any of our product candidates receives marketing approval and we, or others, later discover that the drug is less effective than previously believed or causes undesirable side effects that were not previously identified, our ability, or that of any future collaborators, to market the drug could be compromised.
Clinical trials of our product candidates are conducted in carefully defined subsets of subjects who have agreed to enter into clinical trials. Consequently, it is possible that our clinical trials, or those of any future collaborator, may indicate an apparent positive effect of a product candidate that is greater than the actual positive effect, if any, or alternatively fail to identify undesirable side effects. In particular, because our product candidates will require chronic dosing over the lifetime of the patient, there may be undesirable side effects as a result of long-term exposure to the drug that were not observed in our clinical trials. If, following approval of a product candidate, we, or others, discover that the drug is less effective than previously believed or causes undesirable side effects that were not previously identified, any of the following adverse events could occur:
| ∎ | regulatory authorities may withdraw their approval of the drug or seize the drug; |
| ∎ | we, or any future collaborators, may be required to recall the drug, change the way the drug is administered or conduct additional clinical trials; |
| ∎ | additional restrictions may be imposed on the marketing of, or the manufacturing processes for, the particular drug; |
25
Table of Contents
| ∎ | we may be subject to fines, injunctions or the imposition of civil or criminal penalties; |
| ∎ | regulatory authorities may require the addition of labeling statements, such as a “black box” warning or a contraindication; |
| ∎ | we, or any future collaborators, may be required to create a medication guide outlining the risks of the previously unidentified side effects for distribution to patients; |
| ∎ | we, or any future collaborators, could be sued and held liable for harm caused to patients; |
| ∎ | the drug may become less competitive; and |
| ∎ | our reputation may suffer. |
Any of these events could have a material and adverse effect on our operations and business and could adversely impact the price of the ADSs.
Even if one of our product candidates receives marketing approval, it may fail to achieve the degree of market acceptance by physicians, patients, third-party payors and others in the medical community necessary for commercial success and the market opportunity for the product candidate may be smaller than we estimate.
We have never commercialized a product. Even if one of our product candidates is approved by the appropriate regulatory authorities for marketing and sale, it may nonetheless fail to gain sufficient market acceptance by physicians, patients, third-party payors and others in the medical community. For example, physicians are often reluctant to switch their patients from existing therapies even when new and potentially more effective or convenient treatments enter the market. Further, patients often acclimate to the therapy that they are currently taking and do not want to switch unless their physicians recommend switching products or they are required to switch therapies due to lack of reimbursement for existing therapies.
Efforts to inform the medical community and third-party payors on the benefits of our product candidates may require significant resources and may not be successful. If any of our product candidates is approved but does not achieve an adequate level of market acceptance, we may not generate significant revenues and we may not become profitable. The degree of market acceptance of our product candidates, if approved for commercial sale, will depend on a number of factors, including:
| ∎ | the efficacy and safety of the product; |
| ∎ | the potential advantages of the product compared to alternative treatments; |
| ∎ | the prevalence and severity of any side effects; |
| ∎ | the clinical indications for which the product is approved; |
| ∎ | whether the product is designated under physician treatment guidelines as a first-line therapy or as a second- or third-line therapy; |
| ∎ | limitations or warnings, including distribution or use restrictions, contained in the product’s approved labeling; |
| ∎ | our ability, or the ability of any future collaborators, to offer the product for sale at competitive prices; |
| ∎ | the product’s convenience and ease of administration compared to alternative treatments; |
| ∎ | the willingness of the target patient population to try, and of physicians to prescribe, the product; |
| ∎ | the strength of sales, marketing and distribution support; |
| ∎ | the approval of other new products for the same indications; |
| ∎ | changes in the standard of care for the targeted indications for the product; |
| ∎ | the timing of market introduction of our approved products as well as competitive products; |
| ∎ | availability of coverage and the adequacy of reimbursement from government payors, managed care plans and other third-party payors; |
| ∎ | adverse publicity about the product or favorable publicity about competitive products; and |
| ∎ | potential product liability claims. |
The potential market opportunities for our product candidates are difficult to estimate precisely. Our estimates of the potential market opportunities are predicated on many assumptions, including industry knowledge and publications, third-party research reports and other surveys. While we believe that our internal assumptions are reasonable, these
26
Table of Contents
assumptions involve the exercise of significant judgment on the part of our management, are inherently uncertain and the reasonableness of these assumptions has not been assessed by an independent source. If any of the assumptions proves to be inaccurate, the actual markets for our product candidates could be smaller than our estimates of the potential market opportunities.
If we are unable to establish sales, marketing and distribution capabilities or enter into sales, marketing and distribution arrangements with third parties, we may not be successful in commercializing any product candidates that we develop if and when those product candidates are approved.
We do not have a sales, marketing or distribution infrastructure and have no experience in the sale, marketing or distribution of pharmaceutical products. To achieve commercial success for any approved product, we must either develop a sales and marketing organization or outsource these functions to third parties. We plan to use a combination of focusedin-house sales and marketing capabilities and third-party collaboration, licensing and distribution arrangements to sell any of our products that receive marketing approval.
We generally plan to retain rights to participate in commercialization in the United States, particularly for products that we can commercialize with a specialized sales force and by building a focused sales and marketing organization in the United States to sell our products. The development of sales, marketing and distribution capabilities will require substantial resources, will be time-consuming and could delay any product launch. If the commercial launch of a product for which we recruit a sales force and establish marketing and distribution capabilities is delayed or does not occur for any reason, we could have prematurely or unnecessarily incurred these commercialization costs. This may be costly, and our investment could be lost if we cannot retain or reposition our sales and marketing personnel. In addition, we may not be able to hire or retain a sales force that is sufficient in size or has adequate expertise in the medical markets that we plan to target. If we are unable to establish or retain a sales force and marketing and distribution capabilities, our operating results may be adversely affected. If a potential partner has development or commercialization expertise that we believe is particularly relevant to one of our products, then we may seek to collaborate with that potential partner even if we believe we could otherwise develop and commercialize the product independently.
We hope to collaborate with third parties for commercialization in the United States of any products that require a large sales, marketing and product distribution infrastructure. We plan to commercialize our products outside the United States through collaboration, licensing and distribution arrangements with third parties. As a result of entering into arrangements with third parties to perform sales, marketing and distribution services, our product revenues or the profitability of these product revenues may be lower, perhaps substantially lower, than if we were to directly market and sell products in those markets. Furthermore, we may be unsuccessful in entering into the necessary arrangements with third parties or may be unable to do so on terms that are favorable to us. In addition, we may have little or no control over such third parties, and any of them may fail to devote the necessary resources and attention to sell and market our products effectively.
If we do not establish sales, marketing and distribution capabilities, either on our own or in collaboration with third parties, we will not be successful in commercializing any of our product candidates that receive marketing approval.
We have recently modified our manufacturing processes so that we will be able to produce sufficient quantities of elamipretide for commercial distribution. Interruptions in this process could delay anticipated marketing authorization applications.
Solid-phase peptide synthesis was previously used to produce elamipretide acetate batches for all completed and certain ongoing preclinical and clinical trials. Due to a lack of scalability, we deemed this process undesirable for production of commercial quantities of elamipretide and have implemented a new solution-phase process. It is typical during the years prior to gaining approval for new drugs to continue to develop manufacturing processes to achieve larger scale production with a typical goal of implementing essentially the commercial process prior to supplying pivotal clinical trials. However, our transition to a solution-phase process is recent, and any interruption in continued production of supply needed to meet potential commercial demands could delay anticipated marketing authorization applications, including NDAs, and/ or significantly impact the anticipated cost of commercial production, if our product candidates are approved for sale.
27
Table of Contents
To simplify the daily injection of elamipretide for patients, we have recently developed a multi-dose cartridge suitable for use in a pen injector, but we are still evaluating whether the cartridge will meet performance specifications.
For Phase 1/2 clinical trials, we developed aready-to-use sterile solution drug product suitable for subcutaneous administration. Thisready-to-use solution drug product consists of 1.5 mL of a simple sterile solution of elamipretide acetate containing sodium chloride for tonicity, packaged in asingle-use5-mL vial. This product has been administered clinically using a disposable needle and syringe. To simplify the daily injection of elamipretide for patients with primary mitochondrial myopathy, a multi-dose cartridge, suitable for use in a pen injector, has been developed for use in the most recent clinical trials, including the pivotal clinical trial for primary mitochondrial myopathy, and for commercial distribution, if elamipretide is approved for sale for this indication. Development of this multi-dose cartridge has necessitated that a preservative be added to the formulation to inhibit bacterial growth during thefive-dayintended-use period, and a buffer has been added to maintain a pH suitable for injection; these formulation changes also apply to themulti-use vial which will be supplied to Barth patients if elamipretide is approved for sale for Barth. The preservative and buffer salt are common in similar types of formulations administered by subcutaneous injection. The specific preservative and the level contained in the drug products have been the subject of meetings seeking scientific advice from EU competent authorities and anend-of-Phase 2 meeting with FDA. No issues were raised in either case that would prevent us from continuing as planned with the commercialization of the formulation.
In addition, we have limited experience with the cartridge as a primary container for the drug product and have not demonstrated that the packaged product is stable for extended periods or that the cartridge meets the performance specifications in the pen injector after prolonged storage. Failure in any of these key stability measures could limit the shelf-life of elamipretide. The pen injector has not been submitted for approval in the United States or certain other markets that are key to the projected commercial value of the product, if it is approved for sale. However, we have discussed the pen injector with the FDA and other regulatory authorities and we have received authorization to utilize the pen injector andmulti-use cartridge in our Phase 3 clinical trial in countries including the United States, Canada, Denmark, Hungary and the United Kingdom. We are continuing discussions with regulators in Italy, which does not have a clear path for utilizing a device such as our pen injector in clinical trials. It is possible that we will not receive approval to utilize the device at our Italian sites, which account for 69 of the 407 subjects enrolled in our pre-trial registry. With respect to FDA, the comments received to date have been primarily to address human factors testing (ease of use), which we have addressed in our responses.
We face substantial competition from other pharmaceutical and biotechnology companies, and our operating results may suffer if we fail to compete effectively.
The development and commercialization of new drug products is highly competitive. We expect that we, and any future collaborators, will face significant competition from major pharmaceutical companies, specialty pharmaceutical companies and biotechnology companies worldwide with respect to any of our product candidates that we, or they, may seek to develop or commercialize in the future. Specifically, there are a number of large pharmaceutical and biotechnology companies that currently market and sell products or are pursuing the development of product candidates for the treatment of the key indications of our most advanced programs.
We are initially developing elamipretide for the treatment of rare primary mitochondrial diseases and common diseases of aging in which mitochondrial function is impaired. There are several companies developing treatments that target mitochondria or mitochondria-associated diseases. The majority of these efforts is in preclinical development, is focused on gene therapy or is proposing the use of generic compounds. To our knowledge, none of these is focused on cardiolipin remodeling. Our competitors include: NeuroVive Pharmaceutical AB, Reata Pharmaceuticals, Inc., BioElectron Technology Corporation (formerly Edison Pharmaceuticals Inc.), LumiThera, Inc. and Santhera Pharmaceuticals Holding. In addition to competition from competitors who are developing treatments that seek to improve mitochondrial function or otherwise target the mitochondria, we also face competition from therapies that target the indications we are studying, particularly for diseases of aging such as dry AMD. Such competitors who are developing or who have developed competing therapies include Allegro Ophthalmics, LLC, Apellis Pharmaceuticals, Astellas Pharma Inc., Hemera Biosciences Inc., Ionis Pharmaceuticals, Inc. and Ophthotech Corporation.
28
Table of Contents
Our competitors may succeed in developing, acquiring or licensing technologies and drug products that are more effective, have fewer or more tolerable side effects or are less costly than any product candidates that we are currently developing or that we may develop, which could render our product candidates obsolete and noncompetitive.
Our commercial opportunity could be reduced or eliminated if our competitors develop and commercialize products that are safer, more effective, have fewer or less severe side effects, are more convenient or are less expensive than any products that we, or any future collaborators, may develop. Our competitors also may obtain FDA or other marketing approval for their products before we, or any future collaborators, are able to obtain approval for ours, which could result in our competitors establishing a strong market position before we, or any future collaborators, are able to enter the market.
Many of our existing and potential future competitors have significantly greater financial resources and expertise in research and development, manufacturing, preclinical testing, conducting clinical trials, obtaining marketing approvals and marketing approved products than we do. Mergers and acquisitions in the pharmaceutical and biotechnology industries may result in even more resources being concentrated among a smaller number of our competitors. Smaller or early stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies. These competitors also compete with us in recruiting and retaining qualified scientific and management personnel and establishing clinical trial sites and patient registration for clinical trials, as well as in acquiring technologies complementary to, or necessary for, our programs.
If the FDA or comparable regulatory authorities approve generic versions of any of our products that receive marketing approval, or such authorities do not grant our products appropriate periods of data exclusivity before approving generic versions of our products, the sales of our products could be adversely affected.
Once an NDA is approved, the product covered thereby becomes a “reference-listed drug” in the FDA’s publication, “Approved Drug Products with Therapeutic Equivalence Evaluations.” Manufacturers may seek approval of generic versions of reference-listed drugs through submission of abbreviated new drug applications, or ANDAs, in the United States. In support of an ANDA, a generic manufacturer need not conduct clinical studies. Rather, the applicant generally must show that its product has the same active ingredient(s), dosage form, strength, route of administration and conditions of use or labeling as the reference-listed drug and that the generic version is bioequivalent to the reference-listed drug, meaning it is absorbed in the body at the same rate and to the same extent. Generic products may be significantly less costly to bring to market than the reference-listed drug and companies that produce generic products are generally able to offer them at lower prices. Thus, following the introduction of a generic drug, a significant percentage of the sales of any branded product or reference-listed drug may be typically lost to the generic product.
The FDA may not approve an ANDA for a generic product until any applicable period ofnon-patent exclusivity for the reference-listed drug has expired. The Federal Food, Drug, and Cosmetic Act, or FDCA, provides a period of five years ofnon-patent exclusivity for a new drug containing a new chemical entity, or NCE. Specifically, in cases where such exclusivity has been granted, an ANDA may not be filed with the FDA until the expiration of five years unless the submission is accompanied by a Paragraph IV certification that a patent covering the reference-listed drug is either invalid or will not be infringed by the generic product, in which case the applicant may submit its application four years following approval of the reference-listed drug. We have an issued composition of matter patent on elamipretide. As such, the active ingredient will be treated as an NCE and any products containing elamipretide will be granted exclusivity based on that patent expiry date and other contributing factors. It is unclear whether the FDA will treat the active ingredients in our other product candidates as NCEs and, therefore, afford them five years of NCE data exclusivity if they are approved. If any product we develop does not receive five years of NCE exclusivity, the FDA may approve generic versions of such product three years after its date of approval. Manufacturers may seek to launch these generic products following the expiration of the applicable marketing exclusivity period, even if we still have patent protection for our product.
Competition that our products, if any, may face from generic versions of our products could materially and adversely impact our future revenue, profitability and cash flows and substantially limit our ability to obtain a return on the investments we have made in those product candidates.
29
Table of Contents
Even if we, or any future collaborators, are able to commercialize any product candidate that we, or they, develop, the product may become subject to unfavorable pricing regulations, third-party payor reimbursement practices or healthcare reform initiatives that could harm our business.
The commercial success of our product candidates in key potential markets will depend substantially on the extent to which the costs of our product candidates will be paid by third-party payors, including government health administration authorities and private health coverage insurers. If coverage and reimbursement is not available, or reimbursement is available only to limited levels, we, or any future collaborators, may not be able to successfully commercialize our product candidates. Even if coverage is provided, the approved reimbursement amount may not be high enough to allow us, or any future collaborators, to establish or maintain pricing sufficient to realize a sufficient return on our or their investments.
There is significant uncertainty related to third-party payor coverage and reimbursement of newly approved drugs. Marketing approvals, pricing and reimbursement for new drug products vary widely from country to country. Some countries require approval of the sale price of a drug before it can be marketed. In many countries, the pricing review period begins after marketing or product licensing approval is granted. In some foreign markets, prescription pharmaceutical pricing remains subject to continuing governmental control even after initial approval is granted. As a result, we, or any future collaborators, might obtain marketing approval for a product in a particular country, but then be subject to price regulations that delay commercial launch of the product, possibly for lengthy time periods, which may negatively impact the revenues we are able to generate from the sale of the product in that country. Adverse pricing limitations may hinder our ability or the ability of any future collaborators to recoup our or their investment in one or more product candidates, even if our product candidates obtain marketing approval. Moreover, in the United States, no uniform policy of coverage and reimbursement for products exists among third-party payors. Third-party payors often rely upon Medicare coverage policy and payment limitations in setting their reimbursement rates, but also have their own methods and approval process apart from Medicare determinations. Therefore, coverage and reimbursement for products in the United States can differ significantly from payor to payor.
Patients who are provided medical treatment for their conditions generally rely on third-party payors to reimburse all or part of the costs associated with their treatment. Therefore, our ability, and the ability of any future collaborators, to commercialize any of our product candidates will depend in part on the extent to which coverage and reimbursement for these products and related treatments will be available from third-party payors. Third-party payors decide which medications they will cover and establish reimbursement levels. The healthcare industry is acutely focused on cost containment, both in the United States and worldwide. Government authorities and other third-party payors have attempted to control costs by limiting coverage and the amount of reimbursement for particular medications, which could affect our ability or that of any future collaborators to sell our product candidates profitably. These payors may not view our products, if any, as cost-effective, and coverage and reimbursement may not be available to our customers, or those of any future collaborators, or may not be sufficient to allow our products, if any, to be marketed on a competitive basis. Cost-control initiatives could cause us, or any future collaborators, to decrease the price we, or they, might establish for products, which could result in lower than anticipated product revenues. If the prices for our products, if any, decrease or if governmental and other third-party payors do not provide coverage or adequate reimbursement, our prospects for revenue and profitability will suffer.
There may also be delays in obtaining coverage and reimbursement for newly approved drugs, and coverage may be more limited than the indications for which the drug is approved by the FDA or comparable regulatory authorities. Moreover, eligibility for reimbursement does not imply that any drug will be paid for in all cases or at a rate that covers our costs, including research, development, manufacture, sale and distribution. Reimbursement rates may vary, by way of example, according to the use of the drug and the clinical setting in which it is used. Reimbursement rates may also be based on reimbursement levels already set for lower cost drugs or may be incorporated into existing payments for other services.
In addition, increasingly, third-party payors are requiring higher levels of evidence of the benefits and clinical outcomes of new technologies and are challenging the prices charged. We cannot be sure that coverage will be available for any product candidate that we, or any future collaborator, commercialize and, if available, that the reimbursement rates will be adequate. Further, the net reimbursement for drug products may be subject to additional reductions if there are changes to laws that presently restrict imports of drugs from countries where they
30
Table of Contents
may be sold at lower prices than in the United States. An inability to promptly obtain coverage and adequate payment rates from both government-funded and private payors for any of our product candidates for which we, or any future collaborator, obtain marketing approval could significantly harm our operating results, our ability to raise capital needed to commercialize products and our overall financial condition.
Product liability lawsuits against us could divert our resources, cause us to incur substantial liabilities and limit commercialization of any products that we may develop.
We face an inherent risk of product liability claims as a result of the clinical testing of our product candidates despite obtaining appropriate informed consents from our clinical trial participants. We will face an even greater risk if we or any future collaborators commercially sell any product that we or they may develop. For example, we may be sued if any product we develop allegedly causes injury or is found to be otherwise unsuitable during clinical testing, manufacturing, marketing or sale. Any such product liability claims may include allegations of defects in manufacturing, defects in design, a failure to warn of dangers inherent in the product, negligence, strict liability or a breach of warranties. Claims could also be asserted under state consumer protection acts. If we cannot successfully defend ourselves against product liability claims, we may incur substantial liabilities or be required to limit commercialization of our product candidates. Regardless of the merits or eventual outcome, liability claims may result in:
| ∎ | decreased demand for our product candidates or products that we may develop; |
| ∎ | injury to our reputation and significant negative media attention; |
| ∎ | withdrawal of clinical trial subjects; |
| ∎ | significant costs to defend resulting litigation; |
| ∎ | substantial monetary awards to trial subjects or patients; |
| ∎ | loss of revenue; |
| ∎ | reduced resources of our management to pursue our business strategy; and |
| ∎ | the inability to commercialize any products that we may develop. |
Although we believe we maintain adequate general and clinical trial liability insurance for a company at our stage, this insurance may not fully cover potential liabilities that we may incur. The cost of any product liability litigation or other proceeding, even if resolved in our favor, could be substantial. We will need to increase our insurance coverage if and when we begin selling any product candidate that receives marketing approval. In addition, insurance coverage is becoming increasingly expensive. If we are unable to obtain or maintain sufficient insurance coverage at an acceptable cost or to otherwise protect against potential product liability claims, it could prevent or inhibit the development and commercial production and sale of our product candidates, which could adversely affect our business, financial condition, results of operations and prospects.
Risks Related to Our Dependence on Third Parties
We expect to seek to establish collaborations and, if we are not able to establish them on commercially reasonable terms, we may have to alter our development and commercialization plans.
Our drug development programs and the potential commercialization of our product candidates will require substantial additional cash to fund expenses. We expect to continue to seek one or more collaborators for the development and commercialization of one or more of our product candidates. For example, we hold worldwide rights for elamipretide andSBT-20 and we own our new pipeline compounds, including SBT-272. We expect to retain rights to control the commercialization of elamipretide in rare primary mitochondrial conditions in the United States, and we may explore partnerships for development of elamipretide,SBT-20 and one or more of our pipeline compounds, including SBT-272, in selected other indications and territories. Likely collaborators may include large andmid-size pharmaceutical companies, regional and national pharmaceutical companies and biotechnology companies. In addition, if we are able to obtain marketing approval for any of our product candidates from foreign regulatory authorities, we intend to enter into strategic relationships with international biotechnology or pharmaceutical companies for the commercialization of such product candidates outside of the United States.
We face significant competition in seeking appropriate collaborators. Whether we reach a definitive agreement for a collaboration will depend, among other things, upon our assessment of the collaborator’s resources and expertise,
31
Table of Contents
the terms and conditions of the proposed collaboration and the proposed collaborator’s evaluation of a number of factors. Those factors may include the potential differentiation of our product candidate from competing product candidates, design or results of clinical trials, the likelihood of approval by the FDA or comparable foreign regulatory authorities and the regulatory pathway for any such approval, the potential market for the product candidate, the costs and complexities of manufacturing and delivering the product to patients and the potential of competing products. The collaborator may also consider alternative product candidates or technologies for similar indications that may be available for collaboration and whether such collaboration could be more attractive than the one with us for our product candidate.
Collaborations are complex and time-consuming to negotiate and document. Further, there have been a significant number of recent business combinations among large pharmaceutical companies that have resulted in a reduced number of potential future collaborators.
We may not be able to negotiate collaborations on a timely basis, on acceptable terms, or at all. If we are unable to do so, we may have to curtail the development of the product candidate for which we are seeking to collaborate, reduce or delay its development program or one or more of our other development programs, delay its potential commercialization or reduce the scope of any sales or marketing activities, or increase our expenditures and undertake development or commercialization activities at our own expense. If we elect to increase our expenditures to fund development or commercialization activities on our own, we may need to obtain additional capital, which may not be available to us on acceptable terms, or at all. If we do not have sufficient funds, we may not be able to further develop our product candidates or bring them to market and generate product revenue.
If we enter into collaborations with third parties for the development and commercialization of our product candidates, our prospects with respect to those product candidates will depend in significant part on the success of those collaborations.
We may enter into collaborations for the development and commercialization of certain of our product candidates. If we enter into such collaborations, we will have limited control over the amount and timing of resources that our collaborators will dedicate to the development or commercialization of our product candidates. Our ability to generate revenues from these arrangements will depend on any future collaborators’ abilities to successfully perform the functions assigned to them in these arrangements. In addition, any future collaborators may have the right to abandon research or development projects and terminate applicable agreements, including funding obligations, prior to or upon the expiration of the agreed upon terms.
Collaborations involving our product candidates pose a number of risks, including the following:
| ∎ | collaborators have significant discretion in determining the efforts and resources that they will apply to these collaborations; |
| ∎ | collaborators may not perform their obligations as expected; |
| ∎ | collaborators may not pursue development and commercialization of our product candidates or may elect not to continue or renew development or commercialization programs, based on clinical trial results, changes in the collaborators’ strategic focus or available funding or external factors, such as an acquisition, that divert resources or create competing priorities; |
| ∎ | collaborators may delay clinical trials, provide insufficient funding for a clinical trial, stop a clinical trial or abandon a product candidate, repeat or conduct new clinical trials or require a new formulation of a product candidate for clinical testing; |
| ∎ | a collaborator with marketing and distribution rights to one or more products may not commit sufficient resources to the marketing and distribution of such product or products; |
| ∎ | disagreements with collaborators, including disagreements over proprietary rights, contract interpretation or the preferred course of development, might cause delays or termination of the research, development or commercialization of product candidates, might lead to additional responsibilities for us with respect to product candidates, or might result in litigation or arbitration, any of which would be time-consuming and expensive; |
| ∎ | collaborators may not properly maintain or defend our intellectual property rights or may use our proprietary information in such a way as to invite litigation that could jeopardize or invalidate our intellectual property or proprietary information or expose us to potential litigation; |
32
Table of Contents
| ∎ | collaborators may infringe the intellectual property rights of third parties, which may expose us to litigation and potential liability; and |
| ∎ | collaborations may be terminated and, if terminated, may result in a need for additional capital to pursue further development or commercialization of the applicable product candidates. |
Collaboration agreements may not lead to development or commercialization of product candidates in the most efficient manner, or at all. If any future collaborator of ours is involved in a business combination, it could decide to delay, diminish or terminate the development or commercialization of any product candidate licensed to it by us.
We rely on third parties to conduct our clinical trials. If they do not perform satisfactorily, our business could be significantly harmed.
We do not independently conduct clinical trials of any of our product candidates. We rely on third parties, such as contract research organizations, clinical data management organizations, medical institutions and clinical investigators, to conduct these clinical trials and expect to rely on these third parties to conduct clinical trials of any other product candidate that we develop. Any of these third parties may terminate their engagements with us under certain circumstances. We may not be able to enter into alternative arrangements or do so on commercially reasonable terms. In addition, there is a natural transition period when a new contract research organization begins work. As a result, delays would likely occur, which could materially impact our ability to meet our expected clinical development timelines and harm our business, financial condition and prospects.
Further, our reliance on these third parties for clinical development activities limits our control over these activities, but we remain responsible for ensuring that each of our studies is conducted in accordance with the applicable protocol, legal, regulatory and scientific standards. For example, notwithstanding the obligations of a contract research organization for a trial of one of our product candidates, we remain responsible for ensuring that each of our clinical trials is conducted in accordance with the general investigational plan and protocols for the trial. Moreover, the FDA requires us to comply with standards, commonly referred to as current Good Clinical Practices, or cGCPs, for conducting, recording and reporting the results of clinical trials to assure that data and reported results are credible and accurate and that the rights, integrity and confidentiality of trial participants are protected. The FDA enforces these cGCPs through periodic inspections of trial sponsors, principal investigators, clinical trial sites and institutional review boards. If we or our third-party contractors fail to comply with applicable cGCPs, the clinical data generated in our clinical trials may be deemed unreliable and the FDA may require us to perform additional clinical trials before approving our product candidates, which would delay the marketing approval process. We cannot be certain that, upon inspection, the FDA will determine that any of our clinical trials comply with cGCPs. Similar regulatory requirements apply outside the United States, including the International Council for Harmonization of Technical Requirements for the Registration of Pharmaceuticals for Human Use, or ICH. We are also required to register clinical trials and post the results of completed clinical trials on a government-sponsored database, ClinicalTrials.gov, within certain timeframes. Failure to do so can result in fines, adverse publicity and civil and criminal sanctions.
Furthermore, the third parties conducting clinical trials on our behalf are not our employees, and except for remedies available to us under our agreements with such contractors, we cannot control whether or not they devote sufficient time, skill and resources to our ongoing development programs. These contractors may also have relationships with other commercial entities, including our competitors, for whom they may also be conducting clinical trials or other drug development activities, which could impede their ability to devote appropriate time to our clinical programs. If these third parties do not successfully carry out their contractual duties, meet expected deadlines or conduct our clinical trials in accordance with regulatory requirements or our stated protocols, we may not be able to obtain, or may be delayed in obtaining, marketing approvals for our product candidates. If that occurs, we will not be able to, or may be delayed in our efforts to, successfully commercialize our product candidates. In such an event, our financial results and the commercial prospects for any product candidates that we seek to develop could be harmed, our costs could increase and our ability to generate revenues could be impaired.
We also rely on other third parties to store and distribute drug supplies for our clinical trials. Any performance failure on the part of our distributors could delay clinical development or marketing approval of our product candidates or commercialization of any resulting products, producing additional losses and depriving us of potential product revenue.
33
Table of Contents
We contract with third parties for the manufacture and distribution of our product candidates for clinical trials and expect to continue to do so in connection with our future development and commercialization efforts. This reliance on third parties increases the risk that we will not have sufficient quantities of our product candidates or such quantities at an acceptable cost, which could delay, prevent or impair our development or commercialization efforts.
We currently have no manufacturing facilities and limited personnel with manufacturing experience. We rely on contract manufacturers to produce both drug substance and drug product required for our clinical trials. We plan to continue to rely upon contract manufacturers, and potentially collaboration partners, to manufacture commercial quantities of our product candidates and, if approved, products. Reliance on such third-party contractors entails risks, including:
| ∎ | manufacturing delays if our third-party contractors give greater priority to the supply of other products over our product candidates or otherwise do not satisfactorily perform according to the terms of the agreements between us and them; |
| ∎ | the possible termination or nonrenewal of agreements by our third-party contractors at a time that is costly or inconvenient for us; |
| ∎ | the possible breach by the third-party contractors of our agreements with them; |
| ∎ | the failure of third-party contractors to comply with applicable regulatory requirements; |
| ∎ | the possible mislabeling of clinical supplies, potentially resulting in the wrong dose amounts being supplied or active drug or placebo not being properly identified; |
| ∎ | the possibility of clinical supplies not being delivered to clinical sites on time, leading to clinical trial interruptions, or of drug supplies not being distributed to commercial vendors in a timely manner, resulting in lost sales; and |
| ∎ | the possible misappropriation of our proprietary information, including our trade secrets andknow-how. |
We currently rely, and expect to continue to rely, on third parties for the manufacture of our product candidates for preclinical studies and clinical trials, as well as for commercial manufacture if our product candidates receive marketing approval. To date, we, or our partners on our behalf, have obtained materials for elamipretide andSBT-20 from third party manufacturers. If any of our existing manufacturers should become unavailable to us for any reason, we may incur some delay in identifying or qualifying replacements.
Any manufacturing problem or the loss of a contract manufacturer could be disruptive to our operations, delay our clinical trials and, if our products are approved for sale, result in lost sales. Any reliance on suppliers may involve several risks, including a potential inability to obtain critical materials and reduced control over production costs, delivery schedules, reliability and quality. Any unanticipated disruption to future contract manufacture caused by problems at suppliers could delay shipment of our product candidates, increase our cost of goods sold and result in lost sales.
If any of our product candidates are approved by any regulatory agency, we plan to enter into agreements with third-party contract manufacturers for the commercial production and distribution of those products. It may be difficult for us to reach agreement with a contract manufacturer on satisfactory terms or in a timely manner. In addition, we may face competition for access to manufacturing facilities as there are a limited number of contract manufacturers operating under current good manufacturing practices, or cGMPs, that are capable of manufacturing our product candidates. Consequently, we may not be able to reach agreement with third-party manufacturers on satisfactory terms, which could delay our commercialization efforts.
Third-party manufacturers are required to comply with cGMPs and similar regulatory requirements outside the United States, such as the ICH. Facilities used by our third-party manufacturers must be approved by the FDA after we submit an NDA and before potential approval of the product candidate. Similar regulations apply to manufacturers of our product candidates for use or sale in foreign countries. We do not control the manufacturing process and are completely dependent on our third-party manufacturers for compliance with the applicable regulatory requirements for the manufacture of our product candidates. If our manufacturers cannot successfully manufacture material that conforms to our specifications and the strict regulatory requirements of the FDA, and of any applicable foreign regulatory authority, we will not be able to secure the applicable approval for their manufacturing facilities. If these facilities are not approved for commercial manufacture, we may need to find
34
Table of Contents
alternative manufacturing facilities, which could result in delays in obtaining approval for the applicable product candidate.
In addition, our manufacturers are subject to ongoing periodic inspections by the FDA and corresponding state and foreign agencies for compliance with cGMPs and similar regulatory requirements both prior to and following the receipt of marketing approval for any of our product candidates. Some of these inspections may be unannounced. Failure by any of our manufacturers to comply with applicable cGMPs or other regulatory requirements could result in sanctions being imposed on us, including fines, injunctions, civil penalties, delays, suspensions or withdrawals of approvals, operating restrictions, interruptions in supply and criminal prosecutions, any of which could adversely affect supplies of our product candidates and significantly harm our business, financial condition and results of operations.
Our current and anticipated future dependence upon others for the manufacture of our product candidates may adversely affect our future profit margins and our ability to commercialize any products that receive marketing approval on a timely and competitive basis.
Risks Related to Our Intellectual Property
If we are unable to obtain and maintain sufficient patent protection for our product candidates, or if the scope of the patent protection is not sufficiently broad, our competitors could develop and commercialize products similar or identical to ours, and our ability to commercialize our product candidates successfully may be adversely affected.
Our success depends in large part on our ability to obtain and maintain patent protection in the United States and other countries with respect to our proprietary product candidates. If we do not adequately protect our intellectual property, competitors may be able to erode or negate any competitive advantage we may have, which could harm our business and ability to achieve profitability. To protect our proprietary position, we file patent applications in the United States and abroad related to our novel product candidates that are important to our business. The patent application and approval process is expensive and time-consuming. We may not be able to file and prosecute all necessary or desirable patent applications at a reasonable cost or in a timely manner.
The patent position of biotechnology and pharmaceutical companies generally is highly uncertain. No consistent policy regarding the breadth of claims allowed in biotechnology and pharmaceutical patents has emerged to date in the United States or in many foreign jurisdictions. In addition, the determination of patent rights with respect to pharmaceutical compounds commonly involves complex legal and factual questions, which has in recent years been the subject of much litigation. As a result, the issuance, scope, validity, enforceability, term and commercial value of our patent rights are highly uncertain.
Our pending patent applications cannot be enforced against third parties practicing the technology claimed in such applications unless and until a patent issues from such applications. Assuming the other requirements for patentability are met, currently, the first to file a patent application is generally entitled to the patent. However, prior to March 16, 2013, in the United States, the first to invent was entitled to the patent. Publications of discoveries in the scientific literature often lag behind the actual discoveries, and patent applications in the United States and other jurisdictions are typically not published until 18 months after filing, or in some cases not at all. Therefore, we cannot be certain that we were the first to make the inventions claimed in our patents or pending patent applications, or that we were the first to file for patent protection of such inventions.
Moreover, because the issuance of a patent is not conclusive as to its inventorship, scope, validity, term or enforceability, our patents or pending patent applications may be challenged in the courts or patent offices in the United States and abroad. For example, we may be subject to a third-party preissuance submission of prior art to the U.S. Patent and Trademark Office, or USPTO, or become involved in post-grant review procedures, oppositions, derivations, reexaminations, inter partes review or interference proceedings, in the United States or elsewhere, challenging our patent rights or the patent rights of others. An adverse determination in any such challenges may result in loss of exclusivity or in patent claims being narrowed, invalidated or held unenforceable, in whole or in part, which could limit our ability to stop others from using or commercializing similar or identical technology and products, or limit the duration of the patent protection of our technology and products. Moreover, if the breadth or strength of protection provided by our patents and patent applications is threatened, regardless of the outcome, it
35
Table of Contents
could dissuade companies from collaborating with us to license, develop or commercialize current or future product candidates. In addition, given the amount of time required for the development, testing and regulatory review of new product candidates, patents protecting such candidates might expire before or shortly after such candidates are commercialized. Furthermore, while it is our policy to require our employees and contractors who may be involved in the conception or development of intellectual property to execute agreements assigning such intellectual property to us, we may be unsuccessful in executing such an agreement with each party who, in fact, conceives or develops intellectual property that we regard as our own. As a result, the inventorship or ownership of our intellectual property may be challenged in the future.
Our pending and future patent applications may not result in patents being issued which protect our product candidates, in whole or in part, or which effectively prevent others from commercializing competitive products. Our issued patents or any patents that may issue in the future may be invalidated or interpreted narrowly, such that they fail to provide us with any significant competitive advantage. Changes in either the patent laws or interpretation of the patent laws in the United States and other countries may diminish the value of our patents or narrow the scope of our patent protection. In addition, the laws of foreign countries may not protect our rights to the same extent or in the same manner as the laws of the United States. For example, European patent law restricts the patentability of methods of treatment of the human body more than United States law does.
Even if our patent applications have issued or do issue as patents, they may not issue in a form that will provide us with any meaningful protection, prevent competitors from competing with us or otherwise provide us with any competitive advantage. Our competitors may be able to circumvent our patents by developing similar or alternative technologies or products in anon-infringing manner. Our competitors may also seek approval to market their own products similar to or otherwise competitive with our products. Alternatively, our competitors may seek to market generic versions of any approved products by submitting ANDAs to the FDA in which they claim that patents owned or licensed by us are invalid, unenforceable or not infringed. In these circumstances, we may need to defend or assert our patents, or both, including by filing lawsuits alleging patent infringement. In any of these types of proceedings, a court or other agency with jurisdiction may find our patents invalid or unenforceable, or that our competitors are competing in anon-infringing manner. Thus, even if we have valid and enforceable patents, these patents still may not provide protection against competing products or processes sufficient to achieve our business objectives.
If we are unable to protect the confidentiality of our trade secrets, the value of our technology could be materially adversely affected and our business would be harmed.
While we have obtained composition of matter patents with respect to our clinical-stage product candidates through an application familyin-licensed from Cornell Research Foundation, Inc., a subsidiary of Cornell University, or Cornell, and Institut de recherches cliniques de Montréal, or the IRCM, we also rely on trade secret protection for certain aspects of our discovery platform. We seek to protect these trade secrets, in part, by entering intonon-disclosure and confidentiality agreements with parties who have access to them, such as our employees, consultants, independent contractors, advisors, contract manufacturers, suppliers and other third parties. We also enter into confidentiality and invention or patent assignment agreements with employees, certain consultants, contractors and collaborators. To our knowledge, such agreements have been entered into with all relevant parties; however we cannot be certain that our trade secrets and other confidential proprietary information will not be disclosed or that competitors will not otherwise gain access to our trade secrets or independently develop substantially equivalent information and techniques. Any party with whom we have executed such an agreement may breach that agreement and disclose our proprietary information, including our trade secrets, and we may not be able to obtain adequate remedies for such breaches. Enforcing a claim that a party illegally disclosed or misappropriated a trade secret is difficult, expensive and time-consuming, and the outcome is unpredictable. In addition, if any of our trade secrets were to be lawfully obtained or independently developed by a competitor, we would have no right to prevent such third-party, or those to whom they communicate such technology or information, from using that technology or information to compete with us. If any of our trade secrets were to be misappropriated or disclosed to, or independently developed by, a competitor, our business and competitive position could be harmed.
36
Table of Contents
Certain aspects of our product candidates and technology are protected by patents exclusively licensed from academic institutions. If these third parties terminate their agreements with us or fail to maintain or enforce the underlying patents, or we otherwise lose our rights to these patents, our competitive position and our market share in the markets for any of our approved products will be harmed.
We are a party to license agreements and certain aspects of our business depend on patents and/or patent applications owned by third parties. In particular, we hold exclusive licenses from Cornell and the IRCM for elamipretide andSBT-20 as well as for other compounds and certain methods. We may enter into additional license agreements as part of the development of our business in the future. If we are unable to maintain these patent rights or our license to these patent rights for any reason, or if we are unable to maintain any future material license we may enter into, our ability to develop and commercialize our product candidates could be materially harmed.
Our licensors may not successfully prosecute certain patent applications under which we are licensed and on which our business depends. Even if patents issue from these applications, our licensors may fail to maintain these patents, may decide not to pursue litigation against third party infringers, may fail to prove infringement, or may fail to defend against counterclaims of patent invalidity or unenforceability. For example, under our license agreement with Cornell, we have the first right to enforce the licensed patents against third party infringement. However, our first right to enforce is subject to Cornell’s consent.
Risks with respect to parties from whom we have obtained intellectual property rights may also arise out of circumstances beyond our control. Despite our best efforts, our licensors might conclude that we have materially breached our license agreements and might therefore terminate the license agreements, thereby removing our ability to obtain regulatory approval and to market products covered by these license agreements. For example, under our license agreements with Cornell and the IRCM, if we fail to commercialize a product by December 31, 2020, Cornell may terminate the license, subject to specified exceptions for causes due to scientific and regulatory events that are common in drug development, such as institutional review board delays, clinical trial recruitment, clinical trial results and regulatory delays, and other events over which we cannot exert direct control. If our license agreements are terminated, or if the underlying patents fail to provide the intended market exclusivity, competitors would have the freedom to seek regulatory approval of, and to market, products similar or identical to ours. Moreover, if our license agreements are terminated, our former licensors and/or assignors may be able to prevent us from utilizing the technology covered by the licensed or assigned patents and patent applications. This could have a material adverse effect on our competitive business position and our business prospects.
Our license agreements with Cornell and the IRCM impose, and future license agreements we may enter into may impose, various diligence, milestone payment, royalty and other obligations on us. For example, our license agreements with Cornell and the IRCM include an obligation to pay royalties on the net sales of product candidates or related technologies to the extent they are covered by the agreement. If we fail to comply with our obligations under our license agreement with Cornell and the IRCM or future license agreements, and if no such exceptions apply, our counterparties may have the right to terminate these agreements, in which event we might not be able to develop, manufacture or market any product that is covered by the agreement or face other penalties under the agreement, such as loss of exclusivity. Such an occurrence could materially adversely affect the value of the product candidate being developed under any such agreement. Termination of these agreements or reduction or elimination of our rights under these agreements may result in our having to negotiate new or reinstated agreements with less favorable terms or cause us to lose our rights under these agreements, including our rights to important intellectual property or technology.
Moreover, disputes may arise regarding intellectual property subject to a licensing agreement, including:
| ∎ | the scope of rights granted under the license agreement and other interpretation-related issues; |
| ∎ | the extent to which our product candidates, technology and processes infringe on intellectual property of the licensor that is not subject to the licensing agreement; |
| ∎ | the sublicensing of patent and other rights under our collaborative development relationships; |
| ∎ | our diligence obligations under the license agreement and what activities satisfy those diligence obligations; |
37
Table of Contents
| ∎ | the inventorship and ownership of inventions andknow-how resulting from the joint creation or use of intellectual property by our licensors and us and our partners; and |
| ∎ | the priority of invention of patented technology. |
In addition, the agreements under which we currently license intellectual property or technology from third parties are complex, and certain provisions in such agreements may be susceptible to multiple interpretations. The resolution of any contract interpretation disagreement that may arise could narrow what we believe to be the scope of our rights to the relevant intellectual property or technology, or increase what we believe to be our financial or other obligations under the relevant agreement, either of which could have a material adverse effect on our business, financial condition, results of operations, and prospects. Moreover, if disputes over intellectual property that we have licensed prevent or impair our ability to maintain our current licensing arrangements on commercially acceptable terms, we may be unable to successfully develop and commercialize the affected product candidates, which could have a material adverse effect on our business, financial conditions, results of operations, and prospects.
Some of our intellectual property that was discovered through government-funded programs may be subject to federal regulation such as“march-in” rights, certain reporting requirements, and a preference for United States industry. Compliance with such regulations may limit our exclusive rights, subject us to expenditure of resources with respect to reporting requirements and limit our ability to contract with foreign manufacturers.
Some of our intellectual property with respect to our product candidates has been funded, at least in part, by the U.S. government and, therefore, would be subject to certain federal regulations. As a result, the U.S. government may have certain rights to intellectual property embodied in our current or future product candidates pursuant to the Bayh-Dole Act of 1980, or Bayh-Dole Act. For example, under the“march-in” provisions of the Bayh-Dole Act, the government may have the right under limited circumstances to require the patent owners to grant exclusive, partially exclusive ornon-exclusive rights to third parties for intellectual property discovered through the government-funded program. The government can exercise itsmarch-in rights if it determines that action is necessary because the patent owner fails to achieve practical application of the new invention or because action is necessary to alleviate health concerns or address the safety needs of the public. Intellectual property discovered under the government-funded program is also subject to certain reporting requirements, compliance with which may require us or our licensors to expend substantial resources. Such intellectual property is also subject to a preference for U.S. industry, which may limit our ability to contract with foreign product manufacturers for products covered by such intellectual property. We may apply for additional U.S. government funding, and it is possible that we may discover additional compounds or product candidates as a result of such funding. Intellectual property under such discoveries would be subject to the applicable provisions of the Bayh-Dole Act. Similarly, intellectual property that we license in the future may have been made using government funding and may be subject to the provisions of the Bayh-Dole Act.
We may become involved in lawsuits to protect or enforce our patents or other intellectual property, which could be expensive, time consuming and unsuccessful.
Competitors may infringe our patents, trademarks, copyrights or other intellectual property. We may be required to file infringement claims, which can be expensive and time consuming and divert the time and attention of our management and scientific personnel. Any claims we assert against perceived infringers could provoke these parties to assert counterclaims against us alleging that we infringe their patents, in addition to counterclaims asserting that our patents are invalid or unenforceable, or both. In any patent infringement proceeding, there is a risk that a court will decide that a patent of ours is invalid or unenforceable, in whole or in part, and that we do not have the right to stop the other party from using the invention at issue. There is also a risk that, even if the validity of such patents is upheld, the court will construe the patent’s claims narrowly or decide that we do not have the right to stop the other party from using the invention at issue on the grounds that our patent claims do not cover the invention. An adverse outcome in a litigation or proceeding involving our patents could limit our ability to assert our patents against those parties or other competitors, and may curtail or preclude our ability to exclude third parties from making and selling similar or competitive products. Any of these occurrences could adversely affect our competitive business position, business prospects and financial condition. Similarly, if we assert trademark infringement claims, a court may determine that the marks we have asserted are invalid or unenforceable, or that the party against whom we have asserted trademark infringement has superior rights to the marks in question. In this case, we could ultimately be forced to cease use of such trademarks.
38
Table of Contents
Even if we establish infringement, the court may decide not to grant an injunction against further infringing activity and instead award only monetary damages, which may or may not be an adequate remedy. Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a risk that some of our confidential information could be compromised by disclosure during litigation. There could also be public announcements of the results of hearings, motions or other interim proceedings or developments. If securities analysts or investors perceive these results to be negative, it could have a material adverse effect on the price of the ADSs. Moreover, there can be no assurance that we will have sufficient financial or other resources to file and pursue such infringement claims, which typically last for years before they are concluded. Even if we ultimately prevail in such claims, the monetary cost of such litigation and the diversion of the attention of our management and scientific personnel could outweigh any benefit we receive as a result of the proceedings.
In addition, we may from time to time become involved in disputes, including litigation, with respect to intellectual property. For example, in August 2013, a former vendor commenced an arbitration proceeding against us regarding a disputed license to the vendor’s technology. In July 2014, the vendor commenced a lawsuit against one of our service providers, whom we had previously agreed to indemnify for certain liabilities. In February 2016, we entered into a settlement agreement that provided for mutual releases and dismissal with prejudice of each of the pending arbitration and litigation claims. In connection with the settlement, we paid $725,000 to the vendor and agreed to withdraw and/or not refile certain pending patent applications in satisfaction of all of our obligations under the settlement agreement.
If we are sued for infringing intellectual property rights of third parties, such litigation could be costly and time-consuming and could prevent or delay us from developing or commercializing our product candidates.
Our commercial success depends, in part, on our ability to develop, manufacture, market and sell our product candidates without infringing the intellectual property and other proprietary rights of third parties. Third parties have U.S. andnon-U.S. issued patents and pending patent applications relating to compounds and methods of use for the treatment of key indications for our priority programs, and we may be subject to claims that our research, development and commercialization activities infringe or otherwise violate patents or other intellectual property rights owned or controlled by third parties. If any third-party patents or patent applications are found to cover our product candidates or their methods of use, we may not be free to manufacture or market our product candidates as planned without obtaining a license, which may not be available on commercially reasonable terms, or at all.
There is a substantial amount of intellectual property litigation in the biotechnology and pharmaceutical industries, and we may become party to, or threatened with, litigation or other adversarial proceedings regarding intellectual property rights with respect to our products candidates, including derivation or interference proceedings, post grant andinter partes reviews, opposition proceedings, and the like in the US and in other jurisdictions. Third parties may assert infringement claims against us based on existing or future intellectual property rights. The outcome of intellectual property litigation is subject to uncertainties that cannot be adequately quantified in advance. The pharmaceutical and biotechnology industries have produced a significant number of patents, and it may not always be clear to industry participants, including us, which patents cover various types of products or methods of use. The coverage of patents is subject to interpretation by the courts, and the interpretation is not always uniform. If we were sued for patent infringement, we would need to demonstrate that our product candidates, products or methods either do not infringe the patent claims of the relevant patent or that the patent claims are invalid or unenforceable, and we may not be able to do this. Proving invalidity is difficult. For example, in the United States, proving invalidity requires a showing of clear and convincing evidence to overcome the presumption of validity enjoyed by issued patents. Even if we are successful in these proceedings, we may incur substantial costs and the time and attention of our management and scientific personnel could be diverted in pursuing these proceedings, which could significantly harm our business and operating results. In addition, we may not have sufficient resources to bring these actions to a successful conclusion. Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation or administrative proceedings, there is a risk that some of our confidential information could be compromised by disclosure. In addition, any uncertainties resulting from the initiation and continuation of any litigation could have material adverse effect on our ability to raise additional funds or otherwise have a material adverse effect on our business, results of operations, financial condition and prospects.
If we are found to infringe a third party’s intellectual property rights, we could be forced, including by court order, to cease developing, manufacturing or commercializing the infringing product candidate or product. Alternatively, we
39
Table of Contents
may be required to obtain a license from such third-party in order to use the infringing technology and continue developing, manufacturing or marketing the infringing product candidate. However, we may not be able to obtain any required license on commercially reasonable terms, or at all. Even if we were able to obtain a license, it could benon-exclusive, thereby giving our competitors access to the same technologies licensed to us. In addition, we could be found liable for monetary damages, including treble damages and attorneys’ fees if we are found to have willfully infringed a patent. A finding of infringement could prevent us from commercializing our product candidates or force us to cease some of our business operations, which could materially harm our business. Claims that we have misappropriated the confidential information or trade secrets of third parties could have a similar negative impact on our business.
Changes to the patent law in the United States and other jurisdictions could diminish the value of patents in general, thereby impairing our ability to protect our products.
As is the case with other biopharmaceutical companies, our success is heavily dependent on intellectual property, particularly patents. Obtaining and enforcing patents in the biopharmaceutical industry involves both technological and legal complexity and is therefore costly, time consuming and inherently uncertain. Patent reform legislation in the United States and other countries, including the Leahy-Smith America Invents Act, or the Leahy-Smith Act, signed into law in September 2011, could increase those uncertainties and costs. The Leahy-Smith Act includes a number of significant changes to U.S. patent law. These include provisions that affect the way patent applications are prosecuted, redefine prior art and provide more efficient and cost-effective avenues for competitors to challenge the validity of patents. In addition, the Leahy-Smith Act has transformed the U.S. patent system into a “first to file” system. Thefirst-to-file provisions, however, only became effective in March 2013. Accordingly, it is not yet clear what, if any, impact the Leahy-Smith Act will have on the operation of our business. However, the Leahy-Smith Act and its implementation could make it more difficult to obtain patent protection for our inventions and increase the uncertainties and costs surrounding the prosecution of our or our collaboration partners’ patent applications and the enforcement or defense of our or our collaboration partners’ issued patents, all of which could harm our business, results of operations and financial condition.
The U.S. Supreme Court has ruled on several patent cases in recent years, either narrowing the scope of patent protection available in certain circumstances or weakening the rights of patent owners in certain situations. Additionally, there have been recent proposals for additional changes to the patent laws of the United States and other countries that, if adopted, could impact our ability to enforce our proprietary technology. Depending on future actions by the U.S. Congress, the U.S. courts, the USPTO and the relevantlaw-making bodies in other countries, the laws and regulations governing patents could change in unpredictable ways that would weaken our ability to obtain new patents or to enforce our existing patents and patents that we might obtain in the future.
Obtaining and maintaining our patent protection depends on compliance with various procedural, document submissions, fee payment and other requirements imposed by governmental patent agencies, and our patent protection could be reduced or eliminated fornon-compliance with these requirements.
Periodic maintenance fees on any issued patent are due to be paid to the USPTO and foreign patent agencies in several stages over the lifetime of the patent. The USPTO and various foreign governmental patent agencies require compliance with a number of procedural, documentary, fee payment and other similar provisions during the patent application process. While an inadvertent lapse can in many cases be cured by payment of a late fee or by other means in accordance with the applicable rules, there are situations in which noncompliance can result in abandonment or lapse of the patent or patent application, resulting in partial or complete loss of patent rights in the relevant jurisdiction.Non-compliance events that could result in abandonment or lapse of a patent or patent application include, but are not limited to, failure to respond to official actions within prescribed time limits,non-payment of fees and failure to properly legalize and submit formal documents. If we fail to maintain the patents and patent applications covering our product candidates, our competitive position would be adversely affected.
We may not be able to enforce our intellectual property rights throughout the world.
Filing, prosecuting and defending patents on our product candidates in all countries throughout the world would be prohibitively expensive. The requirements for patentability may differ in certain countries, particularly in developing countries. Competitors may use our technologies in jurisdictions where we have not pursued and obtained patent protection to develop their own products and, further, may export otherwise infringing products to territories where we may obtain patent protection, but where patent enforcement is not as strong as that in the United States. These
40
Table of Contents
products may compete with our products in jurisdictions where we do not have any issued or licensed patents and any future patent claims or other intellectual property rights may not be effective or sufficient to prevent them from so competing.
Moreover, our ability to protect and enforce our intellectual property rights may be adversely affected by unforeseen changes in foreign intellectual property laws. Additionally, laws of some countries outside of the United States and Europe do not afford intellectual property protection to the same extent as the laws of the United States and Europe. Many companies have encountered significant problems in protecting and defending intellectual property rights in certain foreign jurisdictions. The legal systems of some countries, including China, India and other developing countries, do not favor the enforcement of patents and other intellectual property rights. This could make it difficult for us to stop the infringement of our patents or the misappropriation of our other intellectual property rights. For example, many foreign countries have compulsory licensing laws under which a patent owner must grant licenses to third parties. Consequently, we may not be able to prevent third parties from practicing our inventions in certain countries outside the United States and Europe. Competitors may use our technologies in jurisdictions where we have not obtained patent protection to develop their own products and, further, may export otherwise infringing products to territories where we have patent protection, if our ability to enforce our patents to stop infringing activities is inadequate. These products may compete with our products, and our patents or other intellectual property rights may not be effective or sufficient to prevent them from competing.
Proceedings to enforce our patent rights in foreign jurisdictions, whether or not successful, could result in substantial costs and divert our efforts and resources from other aspects of our business. Furthermore, while we intend to protect our intellectual property rights in major markets for our products, we cannot ensure that we will be able to initiate or maintain similar efforts in all jurisdictions in which we may wish to market our products. Accordingly, our efforts to protect our intellectual property rights in such countries may be inadequate.
Patent terms may be inadequate to protect our competitive position on our product candidates for an adequate amount of time.
Patents have a limited lifespan. In the United States, if all maintenance fees are timely paid, the natural expiration of a patent is generally 20 years from its earliest U.S.non-provisional filing date. Various extensions may be available, but the life of a patent, and the protection it affords, is limited. Even if patents covering our product candidates are obtained, once the patent life has expired, we may be open to competition from competitive products, including generics or biosimilars. Given the amount of time required for the development, testing and regulatory review of new product candidates, patents protecting such candidates might expire before or shortly after such candidates are commercialized. As a result, our owned and licensed patent portfolio may not provide us with sufficient rights to exclude others from commercializing products similar or identical to ours.
If we do not obtain patent term extension and data exclusivity for any product candidates we may develop, our business may be materially harmed.
Depending upon the timing, duration and specifics of any FDA marketing approval of any product candidates we may develop, one or more of our U.S. patents may be eligible for limited patent term extension under the Drug Price Competition and Patent Term Restoration Action of 1984, or Hatch-Waxman Amendments. The Hatch-Waxman Amendments permit a patent term extension of up to five years as compensation for patent term lost during the FDA regulatory review process. A patent term extension cannot extend the remaining term of a patent beyond a total of 14 years from the date of product approval, only one patent may be extended and the extension only applies to those claims covering the approved drug, a method for using it, or a method for manufacturing it. However, we may not be granted an extension because of, for example, failing to exercise due diligence during the testing phase or regulatory review process, failing to apply within applicable deadlines, failing to apply prior to expiration of relevant patents, or otherwise failing to satisfy applicable requirements. Moreover, the applicable time period or the scope of patent protection afforded could be less than we request. If we are unable to obtain patent term extension or the term of any such extension is less than we request, our competitors may obtain approval of competing products following our patent expiration, and our business, financial condition, results of operations and prospects could be materially harmed.Furthermore, in the United States, only a single patent can be extended for each qualifying FDA approval, and any patent can be extended only once and only for a single product. Laws governing analogous patent term extensions in foreign jurisdictions vary widely, as do laws governing the ability to obtain multiple patents from a single patent family. Because both elamipretide andSBT-20compositions-of-matter are protected by a single family
41
Table of Contents
of patents and applications, we may not be able to secure patent term extensions for both of these product candidates in all jurisdictions where these product candidates are or may be approved, including the United States.
We may be subject to claims by third parties asserting that our employees or we have misappropriated their intellectual property, or claiming ownership of what we regard as our own intellectual property.
Many of our employees and our licensors’ employees, including our senior management, were previously employed by others, including universities and other biotechnology and pharmaceutical companies, some of which are our competitors or potential competitors. Some of these employees, including each member of our senior management, executed proprietary rights,non-disclosure andnon-competition agreements, or similar agreements, in connection with such previous employment. Although we try to ensure that our employees do not use the proprietary information orknow-how of others in their work for us, we may be subject to claims that we or these employees have used or disclosed intellectual property, including trade secrets or other proprietary information, of any such third party. Litigation may be necessary to defend against such claims. If we fail in defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights or personnel or sustain damages. Such intellectual property rights could be awarded to a third party, and we could be required to obtain a license from such third party to commercialize our technology or products. Such a license may not be available on commercially reasonable terms, or at all. Even if we are successful in defending against such claims, litigation could result in substantial costs and be a distraction to management.
In addition, while we typically require our employees, consultants and contractors who may be involved in the development of intellectual property to execute agreements assigning such intellectual property to us, we may be unsuccessful in executing such an agreement with each party who in fact develops intellectual property that we regard as our own, which may result in claims by or against us related to the ownership of such intellectual property. If we fail in prosecuting or defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights. Even if we are successful in prosecuting or defending against such claims, litigation could result in substantial costs and be a distraction to our senior management and scientific personnel.
Risks Related to Regulatory Approval and Other Legal Compliance Matters
Even if we complete the necessary preclinical and clinical studies, the marketing approval process is expensive, time consuming and uncertain and may prevent us or any future collaborators from obtaining approvals for the commercialization of some or all of our product candidates. As a result, we cannot predict when or if, and in which territories, we, or any future collaborators, will obtain marketing approval to commercialize a product candidate.
The research, testing, manufacturing, labeling, approval, selling, marketing, promotion and distribution of drug products are subject to extensive regulation by the FDA and comparable foreign regulatory authorities, which regulations differ from country to country. We, and any future collaborators, are not permitted to market our product candidates in the United States or in other countries until we, or they, receive approval of an NDA from the FDA or marketing approval from applicable regulatory authorities outside the United States. Our product candidates are in various stages of development and are subject to the risks of failure inherent in drug development. We have not submitted an application for or received marketing approval for any of our product candidates in the United States or in any other jurisdiction. We have limited experience in conducting and managing the clinical trials necessary to obtain marketing approvals, including FDA approval of an NDA.
The process of obtaining marketing approvals, both in the United States and abroad, is lengthy, expensive and uncertain. It may take many years, if approval is obtained at all, and can vary substantially based upon a variety of factors, including the type, complexity and novelty of the product candidates involved.
In addition, changes in marketing approval policies during the development period, changes in or the enactment or promulgation of additional statutes, regulations or guidance or changes in regulatory review for each submitted product application may cause delays in the approval or rejection of an application. Regulatory authorities have substantial discretion in the approval process and may refuse to accept any application or may decide that our data are insufficient for approval and require additional preclinical, clinical or other studies. In addition, varying interpretations of the data obtained from preclinical and clinical testing could delay, limit or prevent marketing approval of a product candidate. Any marketing approval we, or any future collaborators, ultimately obtain may be limited or subject to restrictions or post-approval commitments that render the approved product not commercially viable.
42
Table of Contents
Any delay in obtaining or failure to obtain required approvals could materially adversely affect our ability or that of any future collaborators to generate revenue from the particular product candidate, which likely would result in significant harm to our financial position.
Failure to obtain marketing approval in foreign jurisdictions would prevent our product candidates from being marketed abroad.
In order to market and sell our products in key potential markets, we, and any future collaborators, must obtain separate marketing approvals and comply with numerous and varying regulatory requirements. The approval procedure varies among countries and can involve additional testing. The time required to obtain approval may differ substantially from that required to obtain FDA approval. The marketing approval process outside the United States generally includes all of the risks associated with obtaining FDA approval. In addition, in many countries outside the United States, it is required that the product be approved for reimbursement before the product can be approved for sale in that country. We, and any future collaborators, may not obtain approvals from regulatory authorities outside the United States on a timely basis, if at all. Approval by the FDA does not ensure approval by regulatory authorities in other countries or jurisdictions, and approval by one regulatory authority outside the United States does not ensure approval by regulatory authorities in other countries or jurisdictions or by the FDA.
On June 23, 2016, the electorate in the United Kingdom voted in favor of leaving the European Union, commonly referred to as Brexit. On March 29, 2017, the country formally notified the European Union of its intention to withdraw pursuant to Article 50 of the Lisbon Treaty. Since a significant proportion of the regulatory framework in the United Kingdom is derived from European Union directives and regulations, the referendum could materially impact the regulatory regime with respect to the approval of our product candidates in the United Kingdom or the European Union. Any delay in obtaining, or an inability to obtain, any marketing approvals in the United Kingdom, as a result of Brexit or otherwise, would prevent us from commercializing our product candidates in the United Kingdom and reduce our ability to generate revenue and achieve and sustain profitability. If any of these outcomes occur, we may be forced to restrict or delay efforts to seek regulatory approval in the United Kingdom for our product candidates, which could significantly and materially harm our business.
Furthermore, other European countries may seek to conduct referenda with respect to continuing membership with the European Union. We do not know to what extent Brexit or other comparable initiatives, or any resulting changes, would affect our ability to conduct clinical trials or obtain marketing approval in these jurisdictions, and each could materially impact our ability to conduct clinical trials or obtain marketing approval on a timely basis, or at all.
We have obtained Fast Track designation from the FDA for elamipretide for the treatment of primary mitochondrial myopathy, Barth, LHON and dry AMD with geographic atrophy. However, Fast Track designation may not actually lead to a faster development, regulatory review or approval process.
If a product is intended for the treatment of a serious or life-threatening condition and the product candidate demonstrates the potential to address unmet needs for this condition, the treatment sponsor may apply for FDA Fast Track designation. If the Fast Track designation is obtained, the FDA may initiate review of sections of an NDA, before the application is complete. This “rolling review” is available if the applicant provides, and the FDA approves, a schedule for submission of the individual sections of the application. In December 2015, the FDA notified us that we had obtained Fast Track designation for elamipretide for the treatment of primary mitochondrial myopathy, in November 2017, the FDA notified us that we had obtained Fast Track designation for elamipretide for the treatment of Barth and LHON and in November 2018, the FDA notified us that we had obtained Fast Track designation for elamipretide for the treatment of patients with geographic atrophy, an advanced form of dry AMD. Fast Track designation does not ensure that we will experience a faster development, regulatory review or approval process compared to conventional FDA procedures or that we will ultimately obtain regulatory approval of elamipretide. Additionally, the FDA may withdraw Fast Track designation if it believes that the designation is no longer supported by data from our clinical development program.
We have obtained orphan drug designation from the FDA for elamipretide for the treatment of primary mitochondrial myopathy, Barth and LHON. However, we, or any future collaborators, may not be able to obtain orphan drug designation or orphan drug exclusivity for our other product candidates.
Regulatory authorities in some jurisdictions, including the United States, may designate drugs for relatively small patient populations as orphan drugs. Under the Orphan Drug Act, the FDA may designate a product as an orphan
43
Table of Contents
drug if it is a drug intended to treat a rare disease or condition, which is generally defined as a patient population of fewer than 200,000 individuals annually in the United States, or a patient population greater than 200,000 in the United States where there is no reasonable expectation that the cost of developing the drug will be recovered from sales in the United States. We have received orphan drug designation for elamipretide for primary mitochondrial myopathy, Barth and LHON. We, or any future collaborators, may seek orphan drug designations for other product candidates or in other jurisdictions and may be unable to obtain such designations.
Even for product candidates for which we, or any future collaborators, may obtain orphan drug designation, we, or they, may not be able to obtain orphan drug exclusivity for that product candidate. Generally, if a product candidate with an orphan drug designation receives the first marketing approval for the indication for which it has such designation, the product is entitled to a period of marketing exclusivity, which precludes FDA from approving another marketing application for a product that constitutes the same drug treating the same indication for that marketing exclusivity period, except in limited circumstances. If another sponsor receives such approval before we do (regardless of our orphan drug designation), we will be precluded from receiving marketing approval for our product for the applicable exclusivity period. The applicable period is seven years in the United States. The exclusivity period in the United States can be extended by six months if the sponsor submits pediatric data that fairly respond to a written request from FDA for such data. Orphan drug exclusivity may be revoked if any regulatory agency determines that the request for designation was materially defective or if the manufacturer is unable to assure sufficient quantity of the product to meet the needs of patients with the rare disease or condition.
Even if we, or any future collaborators, obtain orphan drug exclusivity for a product, that exclusivity may not effectively protect the product from competition because different drugs can be approved for the same condition. In the United States, even after an orphan drug is approved, FDA may subsequently approve another drug for the same condition if FDA concludes that the latter drug is not the same drug or is clinically superior in that it is shown to be safer, more effective or makes a major contribution to patient care. In the European Union, marketing authorization may be granted to a similar medicinal product for the same orphan indication if:
| ∎ | the second applicant can establish in its application that its medicinal product, although similar to the orphan medicinal product already authorized, is safer, more effective or otherwise clinically superior; |
| ∎ | the holder of the marketing authorization for the original orphan medicinal product consents to a second orphan medicinal product application; or |
| ∎ | the holder of the marketing authorization for the original orphan medicinal product cannot supply sufficient quantities of orphan medicinal product. |
Even if we, or any future collaborators, obtain marketing approvals for our product candidates, the terms of approvals and ongoing regulation of our products may limit how we, or they, manufacture and market our products, which could materially impair our ability to generate revenue.
Once marketing approval has been granted, an approved product and its manufacturer and marketer are subject to ongoing review and extensive regulation. We, and any future collaborators, must therefore comply with requirements concerning advertising and promotion for any of our product candidates for which we or they obtain marketing approval. Promotional communications with respect to prescription drugs are subject to a variety of legal and regulatory restrictions and must be consistent with the information in the product’s approved labeling. Thus, we and any future collaborators will not be able to promote any products we develop for indications or uses for which they are not approved.
In addition, manufacturers of approved products and those manufacturers’ facilities are required to comply with extensive FDA requirements, including ensuring that quality control and manufacturing procedures conform to cGMPs, which include requirements relating to quality control and quality assurance as well as the corresponding maintenance of records and documentation and reporting requirements. We, our contract manufacturers, any future collaborators and their contract manufacturers could be subject to periodic unannounced inspections by the FDA to monitor and ensure compliance with cGMPs.
Accordingly, assuming we, or any future collaborators, receive marketing approval for one or more of our product candidates, we, and any future collaborators, and our and their contract manufacturers will continue to expend time, money and effort in all areas of regulatory compliance, including manufacturing, production, product surveillance and quality control.
44
Table of Contents
If we, or any of our future collaborators, are not able to comply with post-approval regulatory requirements, we, and any such future collaborators, could have the marketing approvals for our products withdrawn by regulatory authorities and our, or any future collaborators’, ability to market any future products could be limited, which could adversely affect our ability to achieve or sustain profitability. Further, the cost of compliance with post-approval regulations may have a negative effect on our operating results and financial condition.
Any of our product candidates for which we, or any future collaborators, obtain marketing approval in the future could be subject to post-marketing restrictions or withdrawal from the market and we, or any future collaborators, may be subject to substantial penalties if we, or they, fail to comply with regulatory requirements or if we, or they, experience unanticipated problems with our products following approval.
Any of our product candidates for which we, or any future collaborators, obtain marketing approval in the future, as well as the manufacturing processes, post-approval studies and measures, labeling, advertising and promotional activities for such product, among other things, will be subject to continual requirements of and review by the FDA and other regulatory authorities. These requirements include submissions of safety and other post-marketing information and reports, registration and listing requirements, requirements relating to manufacturing, quality control, quality assurance and corresponding maintenance of records and documents, requirements regarding the distribution of samples to physicians and recordkeeping. Even if marketing approval of a product candidate is granted, the approval may be subject to limitations on the indicated uses for which the product may be marketed or to the conditions of approval, including the requirement to implement a Risk Evaluation and Mitigation Strategy.
The FDA may also impose requirements for costly post-marketing studies or clinical trials and surveillance to monitor the safety or efficacy of a product. The FDA and other agencies, including the Department of Justice, closely regulate and monitor the post-approval marketing and promotion of products to ensure that they are manufactured, marketed and distributed only for the approved indications and in accordance with the provisions of the approved labeling. The FDA imposes stringent restrictions on manufacturers’ communications regardingoff-label use and if we, or any future collaborators, do not market any of our product candidates for which we, or they, receive marketing approval for only their approved indications, we, or they, may be subject to warnings or enforcement action foroff-label marketing. Violation of the FDCA and other statutes, including the False Claims Act, relating to the promotion and advertising of prescription drugs may lead to investigations or allegations of violations of federal and state health care fraud and abuse laws and state consumer protection laws, which violations can result in the imposition of significant administrative, civil and criminal penalties.
In addition, later discovery of previously unknown adverse events or other problems with our products or their manufacturers or manufacturing processes, or failure to comply with regulatory requirements, may yield various results, including:
| ∎ | restrictions on such products, manufacturers or manufacturing processes; |
| ∎ | restrictions on the labeling or marketing of a product; |
| ∎ | restrictions on product distribution or use; |
| ∎ | requirements to conduct post-marketing studies or clinical trials; |
| ∎ | warning letters or untitled letters; |
| ∎ | withdrawal of the products from the market; |
| ∎ | refusal to approve pending applications or supplements to approved applications that we submit; |
| ∎ | recall of products; |
| ∎ | restrictions on coverage by third-party payors; |
| ∎ | fines, restitution or disgorgement of profits or revenues; |
| ∎ | suspension or withdrawal of marketing approvals; |
| ∎ | refusal to permit the import or export of products; |
| ∎ | product seizure; or |
| ∎ | injunctions or the imposition of civil or criminal penalties. |
45
Table of Contents
Healthcare legislative reform measures may increase the difficulty and cost for us and any future collaborators to obtain marketing approval of and commercialize our product candidates and affect the prices we, or they, may obtain.
In the United States and some foreign jurisdictions, there have been a number of legislative and regulatory changes and proposed changes regarding the healthcare system that could, among other things, prevent or delay marketing approval of our product candidates, restrict or regulate post-approval activities and affect our ability, or the ability of any future collaborators, to profitably sell any products for which we, or they, obtain marketing approval. We expect that current laws, as well as other healthcare reform measures that will be adopted in the future, may result in more rigorous coverage criteria and in additional downward pressure on the price that we, or any future collaborators, may receive for any approved products.
For example, the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act, or collectively the Affordable Care Act, became law in 2010 and includes the following provisions of potential importance to our product candidates:
| ∎ | an annual,non-deductible fee on any entity that manufactures or imports specified branded prescription drugs and biologic agents; |
| ∎ | an increase in the statutory minimum rebates a manufacturer must pay under the Medicaid Drug Rebate Program; |
| ∎ | a new methodology by which rebates owed by manufacturers under the Medicaid Drug Rebate Program are calculated for certain drugs and biologics that are inhaled, infused, instilled, implanted or injected; |
| ∎ | expansion of federal healthcare fraud and abuse laws, including the False Claims Act and the federal healthcare Anti-Kickback Statute, new government investigative powers and enhanced penalties for noncompliance; |
| ∎ | a new Medicare Part D coverage gap discount program, in which manufacturers must agree to offer 50% (and 70% commencing January 1, 2019)point-of-sale discounts off negotiated prices; |
| ∎ | extension of manufacturers’ Medicaid rebate liability; |
| ∎ | expansion of eligibility criteria for Medicaid programs; |
| ∎ | expansion of the entities eligible for discounts under the Public Health Service pharmaceutical pricing program; |
| ∎ | new requirements to report financial arrangements with physicians and teaching hospitals; |
| ∎ | a new requirement to annually report drug samples that manufacturers and distributors provide to physicians; |
| ∎ | a new Patient-Centered Outcomes Research Institute to oversee, identify priorities in, and conduct comparative clinical effectiveness research, along with funding for such research; |
| ∎ | establishment of a Center for Medicare Innovation at the Centers for Medicare and Medicaid Services, or CMS, to test innovative payment and service delivery models to lower Medicare and Medicaid spending, potentially including prescription drug spending; and |
| ∎ | establishment a licensure framework for follow on biologic products. |
Some of the provisions of the Affordable Care Act have yet to be implemented, and there have been judicial and Congressional challenges to certain aspects of the Affordable Care Act, as well as recent efforts by the Trump administration to repeal or replace certain aspects of the Affordable Care Act. Since January 2017, President Trump has signed two Executive Orders and other directives designed to delay the implementation of certain provisions of the Affordable Care Act or otherwise circumvent some of the requirements for health insurance mandated by the Affordable Care Act. Congress has considered legislation that would repeal or repeal and replace all or part of the Affordable Care Act. While Congress has not passed comprehensive repeal legislation, two bills affecting the implementation of certain taxes under the Affordable Care Act have been signed into law. The Tax Cuts and Jobs Act of 2017, or the Tax Act, includes a provision repealing, effective January 1, 2019, thetax-based shared responsibility payment imposed by the Affordable Care Act on certain individuals who fail to maintain qualifying health coverage for all or part of a year that is commonly referred to as the “individual mandate”. On January 22, 2018, President Trump signed a continuing resolution on appropriations for fiscal year 2018 that delayed the
46
Table of Contents
implementation of certain Affordable CareAct-mandated fees, including theso-called “Cadillac” tax on certain high cost employer-sponsored insurance plans, the annual fee imposed on certain health insurance providers based on market share, and the medical device excise tax onnon-exempt medical devices. The Bipartisan Budget Act of 2018, or the BBA, among other things, amends the Affordable Care Act, effective January 1, 2019, to close the coverage gap in most Medicare drug plans, commonly referred to as the “donut hole”. In July 2018, CMS published a final rule permitting further collections and payments to and from certain Affordable Care Act qualified health plans and health insurance issuers under the Affordable Care Act risk adjustment program in response to the outcome of federal district court litigation regarding the method CMS uses to determine this risk adjustment. On December 14, 2018, a U.S. District Court Judge in the Northern District of Texas ruled that the individual mandate is an inseverable feature of the Affordable Care Act, and therefore, because it was repealed as part of the Tax Act, the remaining provisions of the Affordable Care Act are invalid as well. While the Trump Administration and CMS have both stated that the ruling will have no immediate effect, it is unclear how this decision and subsequent appeals, if any, and other efforts to repeal and replace the Affordable Care Act will impact the Affordable Care Act and our business.
The timing and scope of any potential future legislation to repeal and replace Affordable Care Act provisions is highly uncertain in many respects. Such reforms, if enacted, could have an adverse effect on anticipated revenue from product candidates that we may successfully develop and for which we may obtain marketing approval and may affect our overall financial condition and ability to develop or commercialize product candidates. We expect that the Affordable Care Act, if retained in its current form, as well as other healthcare reform measures that may be adopted in the future, may result in additional reductions in Medicare and other healthcare funding, more rigorous coverage criteria, new payment methodologies and additional downward pressure on the price that we receive for any approved product and/or the level of reimbursement physicians receive for administering any approved product we might bring to market. Reductions in reimbursement levels may negatively impact the prices we receive or the frequency with which our products are prescribed or administered by physicians. Any reduction in reimbursement from Medicare or other government programs may result in a similar reduction in payments from private payors.
In addition, other legislative changes have been proposed and adopted since the Affordable Care Act was enacted. In August 2011, the Budget Control Act of 2011, among other things, created measures for spending reductions by Congress. A Joint Select Committee on Deficit Reduction, tasked with recommending a targeted deficit reduction of at least $1.2 trillion for the years 2013 through 2021, was unable to reach required goals, thereby triggering the legislation’s automatic reduction to several government programs. These changes included aggregate reductions to Medicare payments to providers of up to 2% per fiscal year, which went into effect in April 2013 and due to legislative amendments to the statute, including the BBA, will remain in effect through 2027 unless additional Congressional action is taken. The American Taxpayer Relief Act of 2012, among other things, reduced Medicare payments to several providers and increased the statute of limitations period for the government to recover overpayments to providers from three to five years. These new laws may result in additional reductions in Medicare and other healthcare funding and otherwise affect the prices we may obtain for any of our product candidates for which we may obtain regulatory approval or the frequency with which any such product candidate is prescribed or used.
Moreover, there has been heightened governmental scrutiny recently over pharmaceutical pricing practices in light of the rising cost of prescription drugs and biologics. Such scrutiny has resulted in several recent Congressional inquiries and proposed and enacted federal and state legislation designed to, among other things, bring more transparency to product pricing, review the relationship between pricing and manufacturer patient programs, and reform government program reimbursement methodologies for products. At the federal level, the Trump administration’s budget proposal for fiscal year 2019 contains further drug price control measures that could be enacted during the 2019 budget process or in other future legislation, including, for example, measures to permit Medicare Part D plans to negotiate the price of certain drugs under Medicare Part B, to allow some states to negotiate drug prices under Medicaid, and to eliminate cost sharing for generic drugs forlow-income patients. Further, the Trump administration released a “Blueprint” to lower drug prices and reduce out of pocket costs of drugs that contains additional proposals to increase manufacturer competition, increase the negotiating power of certain federal healthcare programs, incentivize manufacturers to lower the list price of their products and reduce the out of pocket costs of drug products paid by consumers. The U.S. Department of Health and Human Services has already started the process of soliciting feedback
47
Table of Contents
on certain of these measures and, additionally, is immediately implementing others under its existing authority. For example, in September 2018, CMS announced that it will allow Medicare Advantage Plans the option to use step therapy for Part B drugs beginning January 1, 2019, and in October 2018, CMS proposed a new rule that would requiredirect-to-consumer television advertisements of prescription drugs and biological products, for which payment is available through or under Medicare or Medicaid, to include in the advertisement the Wholesale Acquisition Cost, or list price, of that drug or biological product. Although a number of these, and other potential, proposals will require authorization through additional legislation to become effective, Congress and the executive branch have each indicated that it will continue to seek new legislative and/or administrative measures to control drug costs. At the state level, legislatures have increasingly passed legislation and implemented regulations designed to control pharmaceutical and biological product pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access and marketing cost disclosure and transparency measures, and, in some cases, designed to encourage importation from other countries and bulk purchasing.
Additionally, on May 30, 2018, the Trickett Wendler, Frank Mongiello, Jordan McLinn, and Matthew Bellina Right to Try Act of 2017 was signed into law. The law, among other things, provides a federal framework for certain patients to access certain investigational new drug products that have completed a Phase I clinical trial and that are undergoing investigation for FDA approval. Under certain circumstances, eligible patients can seek treatment without enrolling in clinical trials and without obtaining FDA permission under the FDA expanded access program. There is no obligation for a drug manufacturer to make its drug products available to eligible patients as a result of the Right to Try Act.
Legislative and regulatory proposals have also been made to expand post-approval requirements and restrict sales and promotional activities for pharmaceutical products. We cannot be sure whether additional legislative changes will be enacted, or whether the FDA regulations, guidance or interpretations will be changed, or what the impact of such changes on the marketing approvals of our product candidates, if any, may be. In addition, increased scrutiny by the United States Congress of the FDA’s approval process may significantly delay or prevent marketing approval, as well as subject us and any future collaborators to more stringent product labeling and post-marketing testing and other requirements.
Our relationships with customers and third-party payors, among others, will be subject to applicable anti-kickback, fraud and abuse and other healthcare laws and regulations, which could expose us to penalties, including criminal sanctions, civil penalties, contractual damages, reputational harm and diminished profits and future earnings.
Healthcare providers and third-party payors will play a primary role in the recommendation and prescription of any products for which we obtain marketing approval. Our arrangements with third-party payors, healthcare providers and customers, if any, will subject us to broadly applicable fraud and abuse and other healthcare laws and regulations. These laws and regulations may constrain the business or financial arrangements and relationships through which we market, sell and distribute any products for which we obtain marketing approval. These include the following:
Anti-Kickback Statute. The federal healthcare Anti-Kickback Statute prohibits, among other things, persons and entities from knowingly and willfully soliciting, offering, receiving or providing remuneration, directly or indirectly, in cash or in kind, to induce or reward, or in return for, either the referral of an individual for, or the purchase, order or recommendation or arranging of, any good or service, for which payment may be made under a federal healthcare program such as Medicare and Medicaid;
False Claims Laws. The federal civil and criminal false claims laws, including the False Claims Act, and civil monetary penalties laws, whichprovides for civil whistleblower or qui tam actions, prohibit, among other things, individuals and entities from knowingly presenting, or causing to be presented false or fraudulent claims for payment by a federal healthcare program or making a false statement or record material to payment of a false claim or avoiding, decreasing or concealing an obligation to pay money to the federal government;
HIPAA. The federal Health Insurance Portability and Accountability Act of 1996, or HIPAA, imposes criminal and civil liability for, among other things, executing a scheme to defraud any healthcare benefit program or making false statements relating to healthcare matters, and, as amended by the Health Information Technology for Economic and Clinical Health Act and their implementing regulations, also imposes obligations, including mandatory contractual terms and physical, administrative and technical safeguards, with respect to maintaining the privacy, security and transmission of individually identifiable health information;
48
Table of Contents
Transparency Requirements. The federal Physician Payments Sunshine Act requires applicable manufacturers of covered drugs, biologics, devices and supplies to report payments and other transfers of value to physicians and teaching hospitals and ownership and investment interests by physicians; and
Analogous State and Foreign Laws. Analogous state and foreign fraud and abuse laws and regulations, such as state anti-kickback and false claims laws, which may be broader in scope, can apply to our business activities, including sales or marketing arrangements, and claims involving healthcare items or services reimbursed bynon-governmental third party payors, including private insurers, and are generally broad and are enforced by many different federal and state agencies as well as through private actions. Some state laws require pharmaceutical companies to comply with the pharmaceutical industry’s voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government and require drug manufacturers to report information related to payments and other transfers of value to physicians and other healthcare providers or marketing expenditures. Certain state and local laws require the registration of pharmaceutical sales representatives. State and foreign laws also govern the privacy and security of health information in some circumstances, many of which differ from each other in significant ways and often are notpre-empted by HIPAA, thus complicating compliance efforts.
Efforts to ensure that our business arrangements with third parties comply with applicable healthcare laws and regulations involve substantial costs. It is possible that governmental authorities will conclude that our business practices may not comply with current or future statutes, regulations or case law involving applicable fraud and abuse or other healthcare laws and regulations. If our operations are found to be in violation of any of these laws or any other governmental regulations that may apply to us, we may be subject to significant civil, criminal and administrative penalties, damages, fines, disgorgement, individual imprisonment, exclusion of products from government-funded healthcare programs, such as Medicare and Medicaid, additional reporting requirements and oversight if we become subject to a corporate integrity agreement or similar agreement to resolve allegations ofnon-compliance with these laws, and the curtailment or restructuring of our operations. If any of the physicians or other healthcare providers or entities with whom we expect to do business is found to be not in compliance with applicable laws, they may be subject to criminal, civil or administrative sanctions, including exclusions from government-funded healthcare programs.
Regulatory or legislative developments regarding privacy and data security matters could adversely affect our ability to conduct our business.
We are subject to data privacy and security regulation in the jurisdictions in which we conduct our business, particularly in light of increased regulatory scrutiny of and user expectations regarding the processing, collection, use, storage, dissemination, transfer and disposal of user data. The regulatory frameworks regarding privacy issues in many jurisdictions are constantly evolving and can be subject to significant changes from time to time, and therefore we may not be able to comprehensively assess the scope and extent of our compliance responsibility at a global level. In addition, state laws govern the privacy and security of health information in certain circumstances, many of which differ from each other in significant ways, thus complicating compliance efforts. Data privacy concerns may result in increased costs of operations and threats of lawsuits, enforcement actions and related liabilities, including financial penalties.
Our internal computer systems, or those of our collaborators or other contractors or consultants, may fail or suffer security breaches, which could result in a material disruption of our product development programs.
Our internal computer systems and those of our current and any future collaborators and other contractors or consultants are vulnerable to damage from computer viruses, unauthorized access, natural disasters, terrorism, war and telecommunication and electrical failures. Such systems may be vulnerable to service interruptions or to security breaches from inadvertent or intentional actions by our employees, third-party vendors and/or business partners, or from cyber-attacks by malicious third parties. Cyber-attacks are increasing in their frequency, sophistication and intensity, and have become increasingly difficult to detect. Cyber-attacks could include the deployment of harmful malware, ransomware,denial-of-service attacks, social engineering and other means to affect service reliability and threaten the confidentiality, integrity and availability of information. Cyber-attacks also could include phishing attempts ore-mail fraud to cause payments or information to be transmitted to an unintended recipient.
While we have not experienced a system failure, accident, cyber-attack or security breach that has resulted in a material interruption in our operations to date, if such an event were to occur, it could result in a material disruption
49
Table of Contents
of our development programs and our business operations, whether due to a loss of our trade secrets or other proprietary information or other similar disruptions. For example, the loss of clinical trial data from completed or future clinical trials could result in delays in our regulatory approval efforts and significantly increase our costs to recover or reproduce the data.
Additionally, any such event that leads to unauthorized access, use or disclosure of personal information, including personal information regarding our patients or employees, could harm our reputation, cause us not to comply with federal and/or state breach notification laws and foreign law equivalents and otherwise subject us to liability under laws and regulations that protect the privacy and security of personal information. Security breaches and other inappropriate access can be difficult to detect, and any delay in identifying them may lead to increased harm of the type described above. While we have implemented security measures to protect our information technology systems and infrastructure, there can be no assurance that such measures will prevent service interruptions or security breaches that could adversely affect our business and the further development of our product candidates could be delayed.
The collection, use, disclosure, transfer, or other processing of personal data regarding individuals in the EU, including personal health data, is subject to the EU General Data Protection Regulation, or the GDPR, which became effective on May 25, 2018. The GDPR is wide-ranging in scope and imposes numerous requirements on companies that process personal data, including requirements relating to processing health and other sensitive data, obtaining consent of the individuals to whom the personal data relates, providing information to individuals regarding data processing activities, responding to data subject requests, implementing safeguards to protect the security and confidentiality of personal data, providing notification of data breaches, and taking certain measures when engaging third-party processors. The GDPR also imposes strict rules on the transfer of personal data to countries outside the EU, including the United States, and permits data protection authorities to impose large penalties for violations of the GDPR, including potential fines of up to€20.0 million or 4% of annual global revenues, whichever is greater. The GDPR also confers a private right of action on data subjects and consumer associations to lodge complaints with supervisory authorities, seek judicial remedies, and obtain compensation for damages resulting from violations of the GDPR. Compliance with the GDPR will be a rigorous and time-intensive process that may increase our cost of doing business or require us to change our business practices, and despite those efforts, there is a risk that we may be subject to fines and penalties, litigation, and reputational harm in connection with any European activities.
We are subject to U.S. and certain foreign export and import controls, sanctions, embargoes, anticorruption laws, and anti-money laundering laws and regulations. Compliance with these legal standards could impair our ability to compete in domestic and international markets. We can face criminal liability and other serious consequences for violations, which can harm our business.
We are subject to export control and import laws and regulations, including the U.S. Export Administration Regulations, U.S. Customs regulations, various economic and trade sanctions regulations administered by the U.S. Treasury Department’s Office of Foreign Assets Controls, the U.S. Foreign Corrupt Practices Act of 1977, as amended, or FCPA, the U.S. domestic bribery statute contained in 18 U.S.C. § 201, the U.S. Travel Act, the USA PATRIOT Act, and other state and national anti-bribery and anti-money laundering laws in the countries in which we conduct activities. Anti-corruption laws are interpreted broadly and prohibit companies and their employees, agents, contractors, and other collaborators from authorizing, promising, offering, or providing, directly or indirectly, improper payments or anything else of value to recipients in the public or private sector. We may engage third parties to sell our products outside the United States, to conduct clinical trials, and/or to obtain necessary permits, licenses, patent registrations, and other regulatory approvals. We have direct or indirect interactions with officials and employees of government agencies or government-affiliated hospitals, universities, and other organizations. We can be held liable for the corrupt or other illegal activities of our employees, agents, contractors, and other collaborators, even if we do not explicitly authorize or have actual knowledge of such activities. Any violations of the laws and regulations described above may result in substantial civil and criminal fines and penalties, imprisonment, the loss of export or import privileges, debarment, tax reassessments, breach of contract and fraud litigation, reputational harm, and other consequences.
50
Table of Contents
If we fail to comply with environmental, health and safety laws and regulations, we could become subject to fines or penalties or incur costs that could significantly harm our business.
We are subject to numerous environmental, health and safety laws and regulations, including those governing laboratory procedures and the handling, use, storage, treatment and disposal of hazardous materials and wastes. From time to time and in the future, our operations may involve the use of hazardous and flammable materials, including chemicals and biological materials, and may also produce hazardous waste products. Although we contract with third parties for the disposal of these materials and waste products, we cannot completely eliminate the risk of contamination or injury resulting from these materials. In the event of contamination or injury resulting from the use or disposal of our hazardous materials, we could be held liable for any resulting damages, and any liability could exceed our resources. We also could incur significant costs associated with civil or criminal fines and penalties for failure to comply with such laws and regulations.
We maintain workers’ compensation insurance to cover us for costs and expenses we may incur due to injuries to our employees resulting from the use of hazardous materials, but this insurance may not provide adequate coverage against potential liabilities. However, we do not maintain insurance for environmental liability or toxic tort claims that may be asserted against us.
In addition, we may incur substantial costs in order to comply with current or future environmental, health and safety laws and regulations. Current or future environmental laws and regulations may impair our research, development or production efforts, which could adversely affect our business, financial condition, results of operations or prospects. In addition, failure to comply with these laws and regulations may result in substantial fines, penalties or other sanctions.
In the future, if we decide to market our products outside of the United States, such as in the European Union or China, we would need to obtain additional approvals and comply with additional regulatory requirements.
Our primary regulatory strategy is to apply first for approvals in the United States for our rare disease programs. We intend to seek approvals in China commencing in 2019. We may in the future apply for approvals in Europe, or clinical trial waivers in China, following receipt of marketing authorization in the United States. However, as we also plan to consider collaboration for commercialization efforts in Europe and China, we anticipate that potential commercialization partners may have input into regulatory strategies in those jurisdictions. To date, we have focused our regulatory efforts primarily on achieving approvals and marketing authorization in the United States. In order to market any product outside of the United States, we need to comply with numerous and varying regulatory requirements of other countries and jurisdictions regarding quality, safety and efficacy and governing, among other things, clinical trials, marketing authorization, commercial sales and distribution of products. Whether or not we obtain FDA approval for a product, we or our collaborators would need to obtain the necessary approvals by the comparable foreign regulatory authorities before marketing the product in those countries or jurisdictions. We cannot be sure whether and when we would be able to obtain the necessary approvals, which could adversely affect our business and prospects.
Governments outside the United States may impose strict price controls, which may adversely affect our revenues, if any.
In some countries, the pricing of prescription pharmaceuticals is subject to governmental control. In these countries, pricing negotiations with governmental authorities can take considerable time after the receipt of marketing approval for a product. To obtain reimbursement or pricing approval in some countries, we, or any future collaborators, may be required to conduct a clinical trial that compares the cost-effectiveness of our product to other available therapies. If reimbursement of our products is unavailable or limited in scope or amount, or if pricing is set at unsatisfactory levels, our business could be materially harmed.
Our employees may engage in misconduct or other improper activities, includingnon-compliance with regulatory standards and requirements, which could cause significant liability for us and harm our reputation.
We are exposed to the risk of employee fraud or other misconduct, including intentional failures to comply with FDA regulations or similar regulations of comparable regulatory authorities, provide accurate information to the FDA or comparable regulatory authorities, comply with manufacturing standards we have established, comply with federal and state healthcare fraud and abuse laws and regulations and similar laws and regulations established and enforced by comparable regulatory authorities, report financial information or data accurately or disclose unauthorized activities to
51
Table of Contents
us. Employee misconduct could also involve the improper use of information obtained in the course of clinical trials, which could result in regulatory sanctions and serious harm to our reputation. It is not always possible to identify and deter employee misconduct, and the precautions we take to detect and prevent this activity may not be effective in controlling unknown or unmanaged risks or losses or in protecting us from governmental investigations or other actions or lawsuits stemming from a failure to be in compliance with such laws, standards or regulations. If any such actions are instituted against us, and we are not successful in defending ourselves or asserting our rights, those actions could have a significant impact on our business and results of operations, including the imposition of significant civil, criminal and administrative penalties, damages, fines, disgorgement, individual imprisonment, exclusion of products from government-funded healthcare programs, such as Medicare and Medicaid, additional reporting requirements and oversight if subject to a corporate integrity agreement or similar agreement to resolve allegations ofnon-compliance with these laws, and the curtailment or restructuring of our operations.
Risks Related to Employee Matters and Managing Growth
Our future success depends on our ability to retain key executives and to attract, retain and motivate qualified personnel.
We are highly dependent on Reenie McCarthy, our Chief Executive Officer and a Director, as well as the other principal members of our management and scientific teams. Ms. McCarthy is employed “at will,” meaning we or she may terminate the employment relationship at any time. In the future, we may be dependent on other members of our management, scientific and development team. Our ability to compete in the highly competitive biotechnology and pharmaceuticals industries depends upon our ability to attract and retain highly qualified managerial, scientific and medical personnel. Our industry has experienced a high rate of turnover of management personnel in recent years. If we lose one or more of our executive officers or other key employees, our ability to implement our business strategy successfully could be seriously harmed. Furthermore, replacing executive officers or other key employees may be difficult and may take an extended period of time because of the limited number of individuals in our industry with the breadth of skills and experience required to develop, gain marketing approval of and commercialize products successfully. Competition to hire from this limited pool is intense, and we may be unable to hire, train, retain or motivate these additional key employees on acceptable terms given the competition among numerous pharmaceutical and biotechnology companies for similar personnel. We also experience competition for the hiring of scientific and clinical personnel from universities and research institutions.
We rely on consultants and advisors, including scientific and clinical advisors, to assist us in formulating our research and development and commercialization strategy. Our consultants and advisors may be employed by other entities and may have commitments under consulting or advisory contracts with those entities that may limit their availability to us. If we are unable to continue to attract and retain highly qualified personnel, our ability to develop and commercialize our product candidates will be limited.
We expect to grow our organization, and as a result, we may encounter difficulties in managing our growth, which could disrupt our operations.
We expect to experience significant growth in the number of our employees and the scope of our operations, particularly in the areas of drug manufacturing, regulatory affairs and sales, marketing and distribution. To manage these growth activities, we must continue to implement and improve our managerial, operational and financial systems, expand our facilities and continue to recruit and train additional qualified personnel. Our management may need to devote a disproportionate amount of its attention to managing these growth activities. Due to our limited financial resources and the limited experience of our management team in managing a company with such anticipated growth, we may not be able to effectively manage the expansion of our operations or identify, recruit and train additional qualified personnel. Our inability to manage the expansion of our operations effectively may result in weaknesses in our infrastructure, give rise to operational mistakes, loss of business opportunities, loss of employees and reduced productivity among remaining employees. Our expected growth could also require significant capital expenditures and may divert financial resources from other projects, such as the development of additional product candidates. If we are unable to effectively manage our expected growth, our expenses may increase more than expected, our ability to generate revenues could be reduced and we may not be able to implement our business strategy, including the successful commercialization of our product candidates.
52
Table of Contents
Risks Related to this Offering and Ownership of ADSs
After this offering, Morningside Venture (I) Investments Limited will continue to have a controlling ownership interest in our ordinary shares and the ability to determine all matters submitted to shareholders for approval.
Assuming the sale by us of 6,200,000 ADSs (or 7,130,000 ADSs if the underwriters exercise their option to purchase additional ADSs in full), Morningside Venture (I) Investments Limited, or MVIL, will beneficially own 65.1% of our ordinary shares (or 63.3% if the underwriters exercise their option to purchase additional ADSs in full), without giving effect to any ADSs that may be purchased in this offering. As a result, MVIL will be able to control all matters submitted to our shareholders for approval, as well as our management and affairs. For example, MVIL would control the election of directors and approval of any merger, consolidation or sale of all or substantially all of our assets. This concentration of ownership control may:
| ∎ | delay, defer or prevent a change in control; |
| ∎ | entrench our management or the board of directors; or |
| ∎ | impede a merger, consolidation, takeover or other business combination involving us that other shareholders may desire. |
MVIL will own a controlling portion of our ordinary shares after this offering and may have conflicts of interest with us and other shareholders in the future.
MVIL will beneficially own approximately 65.1% of our ordinary shares (or 63.3% if the underwriters exercise their option to purchase additional ADSs in full) following the completion of this offering, without giving effect to any ADSs that may be purchased in this offering. The interests of MVIL may not always be consistent with the interests of our company or of our other shareholders. Accordingly, MVIL could cause us to enter into transactions or agreements of which other holders of our ordinary shares would not approve or make decisions with which such holders would disagree. Gerald L. Chan, one of our directors, is aco-founder of the Morningside group, a private investment group with venture, private equity and property investments. In addition, Reenie McCarthy, our Chief Executive Officer and a director, served as a member of the investment team at the Morningside group from 1993 through 2016, and remains a director of Morningside Technology Advisory, LLC, which provides advisory services to entities associated with the Morningside group.
Although Dr. Chan is not an officer, director or employee of MVIL and has neither voting nor dispositive control over the ordinary shares held by MVIL and does not otherwise beneficially own such shares, as a result of his ongoing relationship with the Morningside group, transactions between us and MVIL may present an actual or perceived conflict of interest. Although Ms. McCarthy is not an officer, director or employee of MVIL, and has neither voting nor dispositive control over our ordinary shares held by MVIL and does not otherwise beneficially own such shares, as a result of her historic relationship with the Morningside group and her ongoing relationship with Morningside Technology Advisory, LLC, transactions between us and MVIL may present an actual or perceived conflict of interest. Any actual or perceived conflicts of interest may lead Dr. Chan and Ms. McCarthy to recuse themselves from actions of our board of directors with respect to transactions involving MVIL and its affiliates. For example, in a situation in which MVIL is adverse to us, such as if it breaches an agreement with us, a conflict could arise. We may not be able to resolve any potential conflicts, and even if we do, the resolution may be less favorable than if we were dealing with an unaffiliated party.
MVIL is in the business of making investments in companies and could from time to time acquire and hold interests in businesses that compete with us. MVIL may also pursue acquisition opportunities that may be complementary to our business, and as a result, desirable acquisitions may not be available to us. So long as MVIL continues to own a significant amount of our equity, it will continue to be able to strongly influence or effectively control our decisions.
Our existing principal shareholder, Morningside Venture (I) Investments Limited, certain entities associated with it, certain of the holders of our outstanding convertible notes and entities associated with such holders have indicated an interest in purchasing up to an aggregate of approximately $60.0 million of ADSs in this offering at the initial public offering price and on the same terms as the other purchasers in this offering. Assuming an initial public offering price of $13.00 per ADS, these persons would purchase an aggregate of 4,615,385 of the 6,200,000 ADSs offered in this offering based on these indications of interest. However, because indications of interest are not binding agreements or commitments to purchase, these persons may determine to purchase fewer ADSs than they
53
Table of Contents
indicate an interest in purchasing or not to purchase any ADSs in this offering. It is also possible that these persons could purchase more ADSs in this offering. In addition, the underwriters could determine to sell fewer ADSs to any of these persons than they indicate an interest in purchasing or not to sell any ADSs to such persons. The foregoing discussion does not reflect any potential purchases by these potential purchasers.
If you purchase ADSs in this offering, you will suffer immediate dilution in the net tangible book value of your investment.
The initial public offering price of the ADSs will be substantially higher than the net tangible book value per ADS. Therefore, if you purchase ADSs in this offering, you will pay a price per ADS that substantially exceeds our net tangible book value per ADS after this offering. Based on an assumed initial public offering price of $13.00 per ADS, which is the midpoint of the price range set forth on the cover page of this prospectus, you will experience immediate dilution of $11.79 per ADS, representing the difference between our pro forma as adjusted net tangible book value per ADS after giving effect to this offering and the assumed initial public offering price. In addition, purchasers of ADSs in this offering will have contributed approximately 17.5% of the aggregate price paid by all purchasers of our shares and will own approximately 18.8% of our ordinary shares outstanding after this offering, excluding any ordinary shares that they may have acquired prior to this offering. Furthermore, if the underwriters exercise their option to purchase additional ADSs or our previously issued options to acquire ordinary shares at prices below the assumed initial public offering price are exercised, you will experience further dilution. For a further description of the dilution that you will experience immediately after this offering, see “Dilution.”
The price of the ADSs is likely to be highly volatile, which could result in substantial losses for purchasers of the ADSs in this offering.
The price of the ADSs is likely to be highly volatile. The stock market in general and the market for smaller pharmaceutical and biotechnology companies in particular have experienced extreme volatility that has often been unrelated to the operating performance of particular companies. As a result of this volatility, you may not be able to sell your ADSs at or above the initial public offering price and you may lose some or all of your investment. The market price for the ADSs may be influenced by many factors, including:
| ∎ | our ability to commercialize or obtain regulatory approval for our product candidates, or delays in commercializing or obtaining regulatory approval; |
| ∎ | announcements relating to our clinical trials, including any periodic updates relating to enrollment of trial subjects, adverse events, site initiation, and timing of release of interim analyses and final trial results; |
| ∎ | commencement or termination of collaborations for our development programs; |
| ∎ | failure or discontinuation of any of our development programs; |
| ∎ | results from, or any delays in, clinical trials relating to our product candidates, including our clinical trials for elamipretide; |
| ∎ | any need to suspend or discontinue clinical trials due to side effects or other safety risks, or any need to conduct studies on the long-term effects associated with the use of our product candidates; |
| ∎ | manufacturing issues related to our product candidates for clinical trials or future products for commercialization; |
| ∎ | commercial success and market acceptance of our product candidates following regulatory approval; |
| ∎ | undesirable side effects caused by product candidates after they have entered the market; |
| ∎ | ability to discover, develop and commercialize additional product candidates; |
| ∎ | announcements relating to collaborations that we may enter into with respect to the development or commercialization of our product candidates; |
| ∎ | success of our competitors in discovering, developing or commercializing products; |
| ∎ | strategic transactions undertaken by us; |
| ∎ | additions or departures of key personnel; |
| ∎ | product liability claims related to our clinical trials or product candidates; |
| ∎ | business disruptions caused by earthquakes or other natural disasters; |
| ∎ | disputes concerning our intellectual property or other proprietary rights; |
| ∎ | FDA, EMA, NMPA or other regulatory actions affecting us or our industry; |
54
Table of Contents
| ∎ | healthcare reform measures in the United States; |
| ∎ | future sales or issuances of equity or debt securities by us; |
| ∎ | fluctuations in our semi-annual operating results; |
| ∎ | the issuance of new or changed securities analysts’ reports or recommendations regarding us; |
| ∎ | announcement or expectation of additional financing efforts; |
| ∎ | sales of our ordinary shares by us, our insiders or other shareholders; |
| ∎ | actual and anticipated variations in our results of operations; |
| ∎ | changes in securities analysts’ estimates or market perception of our financial performance; |
| ∎ | announcements by us of significant acquisitions, disposals, strategic alliances or joint ventures; |
| ∎ | recruitment or loss of key personnel by us or our competitors; |
| ∎ | market developments affecting us or the markets in which we operate; |
| ∎ | regulatory or legal developments, including litigation; |
| ∎ | the operating and share price performance of companies that investors consider to be comparable to us; |
| ∎ | the depth and liquidity of the market for the ADSs; |
| ∎ | the release or expiry oflock-up or other transfer restrictions on our ordinary shares and ADSs; |
| ∎ | general economic, political and stock market conditions in the United States and the countries in which we operate and elsewhere in the world; and |
| ∎ | the other factors described in this “Risk Factors” section. |
Additionally, in the past, securities class action litigation has often been brought against a company following a decline in the market price of its securities. This risk is especially relevant for us in light of the significant stock price volatility pharmaceutical companies have experienced in recent years. If we face such litigation, it could result in substantial costs and a diversion of management’s attention and resources, which could harm our business.
No public market for the ADSs currently exists, and an active trading market for the ADSs may not develop.
Prior to this offering, there has been no public market for the ADSs. The initial public offering price for the ADSs will be determined through negotiations with the underwriters. This price may not reflect the price at which investors in the market will be willing to buy and sell our ADSs following this offering. Although we have applied to have the ADSs listed on The Nasdaq Global Market, an active trading market for the ADSs may never develop or, if developed, be maintained following this offering. If an active market for the ADSs does not develop or is not maintained, it may be difficult for you to sell ADSs you purchase in this offering without depressing the market price for the ADSs, or at all. An inactive trading market may also impair our ability to raise capital to continue to fund operations by selling shares or ADSs and may impair our ability to acquire other companies or technologies by using our shares or ADSs as consideration.
We have broad discretion in the use of the net proceeds from this offering and may not use them effectively.
Our management will have broad discretion in the application of the net proceeds from this offering and could spend the proceeds in ways that do not improve our results of operations or enhance the value of the ADSs. The failure by our management to apply these funds effectively could result in financial losses that could significantly harm our business, cause the price of the ADSs to decline and delay the development of our product candidates. Pending their use, we may invest the net proceeds from this offering in a manner that does not produce income or that loses value.
We are an “emerging growth company,” and the reduced disclosure requirements applicable to emerging growth companies may make the ADSs less attractive to investors.
We are an “emerging growth company,” as defined in the Jumpstart Our Business Startups Act of 2012, or the JOBS Act, and may remain an emerging growth company for up to five years. For so long as we remain an emerging growth company, we are permitted and plan to rely on exemptions from certain disclosure requirements that are applicable to other public companies that are not emerging growth companies. These exemptions include not being required to comply with the auditor attestation requirements of Section 404 of the Sarbanes-Oxley Act of 2002, or SOX Section 404, not being required to comply with any requirement that may be adopted by the Public Company Accounting Oversight Board regarding mandatory audit firm rotation or a supplement to the auditor’s report providing additional information about the audit and the financial statements, reduced disclosure obligations regarding executive compensation and exemptions from the requirements of holding a nonbinding advisory vote on executive
55
Table of Contents
compensation and shareholder approval of any golden parachute payments not previously approved. In this prospectus, we have not included all of the executive compensation related information that would be required if we were not an emerging growth company and a foreign private issuer. We cannot predict whether investors will find the ADSs less attractive if we rely on these exemptions. If some investors find the ADSs less attractive as a result, there may be a less active trading market for the ADSs and the price of the ADSs may be more volatile.
In addition, the JOBS Act provides that an emerging growth company can take advantage of an extended transition period for complying with new or revised accounting standards. This allows an emerging growth company to delay the adoption of certain accounting standards until those standards would otherwise apply to private companies. We have elected to avail ourselves of this exemption from new or revised accounting standards and, therefore, we will not be subject to the same new or revised accounting standards as other public companies. As a result, our financial statements may not be comparable to the financial statements of reporting companies that are required to comply with the effective dates for new or revised accounting standards that are otherwise applicable to public companies.
As a foreign private issuer, we are exempt from a number of rules under the U.S. securities laws and are permitted to file less information with the Securities and Exchange Commission than U.S. companies. This may limit the information available to holders of the ADSs.
We are a “foreign private issuer,” as defined in the rules and regulations of the Securities and Exchange Commission, or the SEC, and, consequently, we are not subject to all of the disclosure requirements applicable to companies organized within the United States. For example, we are exempt from certain rules under the U.S. Exchange Act, that regulate disclosure obligations and procedural requirements related to the solicitation of proxies, consents or authorizations applicable to a security registered under the Exchange Act. In addition, our senior management and supervisory board members are exempt from the reporting and “short-swing” profit recovery provisions of Section 16 of the Exchange Act and related rules with respect to their purchases and sales of our securities. Moreover, we are not required to file periodic reports and financial statements with the SEC as frequently or as promptly as U.S. public companies. Accordingly, there may be less publicly available information concerning our company than there is for U.S. public companies.
In addition, foreign private issuers are not required to file their annual report onForm 20-F until 120 days after the end of each fiscal year, while U.S. domestic issuers that are accelerated filers are required to file their annual report onForm 10-K within 75 days after the end of each fiscal year. Foreign private issuers are also exempt from the Regulation Fair Disclosure, aimed at preventing issuers from making selective disclosures of material information. As a result of the above, you may not have the same protections afforded to shareholders of companies that are not foreign private issuers.
We intend to rely on Nasdaq Stock Market rules that permit us to comply with applicable Cayman Islands corporate governance practices, rather than the corresponding domestic U.S. corporate governance practices, and therefore your rights as a shareholder will differ from the rights you would have as a shareholder of a domestic U.S. issuer.
As a foreign private issuer whose ADSs are listed on The Nasdaq Global Market, we are permitted in certain cases to follow Cayman Islands corporate governance practices instead of the corresponding requirements of the Nasdaq Stock Market rules. A foreign private issuer that elects to follow a home country practice instead of Nasdaq requirements must submit to Nasdaq in advance a written statement from an independent counsel in such issuer’s home country certifying that the issuer’s practices are not prohibited by the home country’s laws. In addition, a foreign private issuer must disclose in its annual reports filed with the SEC each such requirement that it does not follow and describe the home country practice followed instead of any such requirement. In accordance with Cayman Islands law:
| ∎ | we do not require a remuneration committee to have entirely independent directors; |
| ∎ | we do not require an independent director oversight of director nominations; and |
| ∎ | we do not require the board of directors to have regularly scheduled meetings at which only independent directors are present. |
For further information upon the differences between Delaware law and Cayman Islands law, please see “Description of Share Capital and Articles of Association—Differences in Corporate Law.”
56
Table of Contents
We may lose our foreign private issuer status, which would then require us to comply with the Exchange Act’s domestic reporting regime and cause us to incur significant legal, accounting and other expenses.
As discussed above, we are a foreign private issuer, and therefore, we are not required to comply with all of the periodic disclosure and current reporting requirements of the Exchange Act. The determination of foreign private issuer status is made annually on the last business day of an issuer’s most recently completed second fiscal quarter. We would lose our foreign private issuer status if, for example, more than 50% of our ordinary shares are directly or indirectly held by residents of the United States and we fail to meet additional requirements necessary to maintain our foreign private issuer status. If we lose our foreign private issuer status on this date, we will be required to file with the SEC periodic reports and registration statements on U.S. domestic issuer forms, which are more detailed and extensive than the forms available to a foreign private issuer. We will also have to mandatorily comply with U.S. federal proxy requirements, and our officers, directors and principal shareholders will become subject to the short-swing profit disclosure and recovery provisions of Section 16 of the Exchange Act. In addition, we will lose our ability to rely upon exemptions from certain corporate governance requirements under the Nasdaq listing rules. As a U.S. listed public company that is not a foreign private issuer, we will incur significant additional legal, accounting and other expenses that we will not incur as a foreign private issuer, and accounting, reporting and other expenses in order to maintain a listing on a U.S. securities exchange. These rules and regulations could also make it more difficult for us to attract and retain qualified members of our board of directors and more expensive to procure director and officer liability insurance.
We will incur increased costs as a result of operating as a public company, and our management will be required to devote substantial time to new compliance initiatives and corporate governance practices.
As a public company, and particularly after we are no longer an “emerging growth company,” we will incur significant legal, accounting and other expenses that we did not incur as a private company. The Sarbanes-Oxley Act of 2002, the Dodd-Frank Wall Street Reform and Consumer Protection Act, the listing requirements of The Nasdaq Global Market and other applicable securities rules and regulations impose various requirements on public companies, including establishment and maintenance of effective disclosure and financial controls and corporate governance practices. We expect that we will need to hire additional accounting, finance and other personnel in connection with our becoming, and our efforts to comply with the requirements of being, a public company and our management and other personnel will need to devote a substantial amount of time towards maintaining compliance with these requirements. These requirements will increase our legal and financial compliance costs and will make some activities more time-consuming and costly. For example, we expect that the rules and regulations applicable to us as a public company may make it more difficult and more expensive for us to obtain director and officer liability insurance, which could make it more difficult for us to attract and retain qualified members of our board of directors. We are currently evaluating these rules and regulations, and cannot predict or estimate the amount of additional costs we may incur or the timing of such costs. These rules and regulations are often subject to varying interpretations, in many cases due to their lack of specificity, and, as a result, their application in practice may evolve over time as new guidance is provided by regulatory and governing bodies. This could result in continuing uncertainty regarding compliance matters and higher costs necessitated by ongoing revisions to disclosure and governance practices.
Pursuant to SOX Section 404, we will be required to furnish a report by our management on our internal control over financial reporting. However, while we remain an emerging growth company, we will not be required to include an attestation report on internal control over financial reporting issued by our independent registered public accounting firm. To achieve compliance with SOX Section 404 within the prescribed period, we will be engaged in a process to document and evaluate our internal control over financial reporting, which is both costly and challenging. In this regard, we will need to continue to dedicate internal resources, potentially engage outside consultants and adopt a detailed work plan to assess and document the adequacy of internal control over financial reporting, continue steps to improve control processes as appropriate, validate through testing that controls are functioning as documented and implement a continuous reporting and improvement process for internal control over financial reporting. Despite our efforts, there is a risk that we will not be able to conclude, within the prescribed timeframe, or at all, that our internal control over financial reporting is effective as required by SOX Section 404. If we identify one or more material weaknesses, it could result in an adverse reaction in the financial markets due to a loss of confidence in the reliability of our financial statements.
57
Table of Contents
A significant portion of our total outstanding shares is restricted from immediate resale, but may be sold into the market in the near future, which could cause the market price of the ADSs to decline significantly, even if our business is doing well.
Sales of a substantial number of ADSs in the public market could occur at any time. These sales, or the perception in the market that the holders of a large number of ordinary shares intend to sell ADSs, could reduce the market price of the ADSs. After this offering and after giving effect to (i) the issuance of 161,732,652 shares upon the conversion of the 2018 Notes, assuming an initial public offering price of $13.00 per ADS (the midpoint of the estimated price range set forth on the cover page of this prospectus), and (ii) the conversion of all outstanding Series A convertible preferred shares into an aggregate of 91,600,398 ordinary shares, both of which will occur automatically upon the closing of this offering, we will have 396,220,998 ordinary shares outstanding based on the 68,487,948 ordinary shares outstanding as of December 31, 2018 (or 407,380,998 shares if the underwriters exercise their option to purchase additional ADSs in full).
All ADSs we are selling in this offering may be resold in the public market immediately, unless purchased by our affiliates. The remaining ordinary shares are currently restricted under securities laws or as a result oflock-up or other agreements, but will be able to be sold, subject to any applicable volume limitations under federal securities laws with respect to affiliate sales. For additional information on applicable restrictions on sales of ordinary shares and ADSs after this offering, see the “Shares and ADS Eligible For Future Sale” section of this prospectus.
We, each of our directors, officers and holders of substantially all our outstanding equity securities have entered intolock-up agreements with the underwriters under which we and they have agreed, subject to certain exceptions described in the section titled “Underwriting”, not to, directly or indirectly, dispose of or hedge any ordinary shares, ADSs or securities convertible into or exchangeable for ordinary shares during the period from the date of the final prospectus for this offering continuing to and including 180 days after the date of the final prospectus for this offering without the prior written consent of Jefferies LLC and Evercore Group L.L.C. We refer to this period as thelock-up period. Upon the release of the foregoing restrictions, our securityholders subject to alock-up agreement will be able to sell our ADSs in the public market, subject to volume limitations applicable to affiliates. In addition, Jefferies LLC and Evercore Group L.L.C. may, in their sole discretion, release all or some portion of the securities subject tolock-up agreements prior to the expiration of thelock-up period. For a description of thelock-up agreements, see the ‘‘Underwriting’’ section of this prospectus. Sales of a substantial number of such securities upon early release or expiration of thelock-up period or the perception that such sales may occur could cause the market price of ADSs to decline or make it more difficult for you to sell your ADSs at a time and at a price that you deem appropriate. We also plan to register all approximately 67.5 million ordinary shares that we may issue under our equity compensation plans. Once we register these shares, they can be freely sold in the public market upon issuance and once vested, subject to volume limitations applicable to affiliates and thelock-up agreements described above and in the “Underwriting” section of this prospectus.
We do not anticipate paying any cash dividends on the ADSs in the foreseeable future. Accordingly, holders of ADSs must rely on capital appreciation, if any, for any return on their investment.
We have never declared nor paid cash dividends on our share capital. We currently plan to retain all of our future earnings, if any, to finance the operation, development and growth of our business. In addition, the terms of our existing loan and security agreement preclude us from paying cash dividends without the consent of our lender. As a result, capital appreciation, if any, of the ADSs will be your sole source of gain for the foreseeable future. However, if we do pay a cash dividend on our ordinary shares in the future, we may only pay such dividend out of our profits or share premium (subject to applicable solvency requirements) under Cayman Islands law.
If securities or industry analysts do not publish research or publish inaccurate or unfavorable research about our business, our share price and trading volume could decline.
The trading market for the ADSs will likely depend, in part, on the research and reports that securities or industry analysts publish about us or our business. We do not have any control over these analysts. There can be no assurance that analysts will cover us, or provide favorable coverage. If one or more analysts downgrade the ADSs or change their opinion of the ADSs, our share price would likely decline. In addition, if one or more analysts cease coverage of our company or fail to regularly publish reports on us, we could lose visibility in the financial markets, which could cause the price of the ADSs or trading volume to decline.
58
Table of Contents
We may be classified as a passive foreign investment company for any taxable year, which may result in adverse U.S. federal income tax consequence to U.S. holders.
Based on our estimated gross income and average value of our gross assets, taking into account the initial public offering price of the ADSs in this offering and the expected price of the ADSs following this offering, and the nature of our business, we do not believe that we were a “passive foreign investment company,” or PFIC, for U.S. federal income tax purposes for our tax year ended December 31, 2017 and do not expect to be a PFIC during our tax year ending December 31, 2018. A corporation organized outside the United States generally will be classified as a PFIC for U.S. federal income tax purposes in any taxable year in which at least 75% of its gross income is passive income or on average at least 50% of the gross value of its assets is attributable to assets that produce passive income or are held for the production of passive income. Passive income for this purpose generally includes dividends, interest, royalties, rents and gains from commodities and securities transactions. Our status in any taxable year will depend on our assets and activities in each year, and because this is a factual determination made annually after the end of each taxable year, there can be no assurance that we will not be considered a PFIC for the current taxable year or any future taxable year. The market value of our assets may be determined in large part by reference to the market price of the ADSs, which is likely to fluctuate after the offering, and may fluctuate considerably given that market prices of biotechnology companies have been especially volatile. If we were to be treated as a PFIC for any taxable year during which a U.S. holder held the ADSs, however, certain adverse U.S. federal income tax consequences could apply to the U.S. holder. See “Taxation—Material U.S. Federal Income Tax Considerations for U.S. Holders—Passive Foreign Investment Company Rules” in this prospectus.
We may choose to list our ordinary shares on another securities exchange outside of the United States the ADSs following this offering, which may adversely affect the liquidity and value of our ADSs and subject us to additional obligations.
We have in the past considered, and may in the future seek to, list our ordinary shares on another exchange outside of the United States following this offering. If we decide to pursue a cross or dual listing of our ordinary shares, we cannot predict the effect any such listing would have on the value of our ordinary shares and ADSs. However, the cross listing of our ordinary shares and our ADSs may dilute the liquidity of these securities in one or both markets and may adversely affect the development of an active trading market for our ADSs in the United States. The price of our ADSs could also be adversely affected by trading in our ordinary shares on any other exchange. Furthermore, a listing on any other exchange could subject us to additional requirements and/or obligations, including financial and other reporting requirements, and could restrict our ability to undertake certain activities that would be beneficial for our shareholders and holders of our ADSs.
Holders of our ADSs have fewer rights than our shareholders and must act through the depositary to exercise their rights.
Holders of our ADSs do not have the same rights as our shareholders and may only exercise their voting rights with respect to the underlying ordinary shares in accordance with the provisions of the deposit agreement. Holders of the ADSs will appoint the depositary or its nominee as their representative to exercise the voting rights attaching to the ordinary shares represented by the ADSs. When a general meeting is convened, if you hold ADSs, you may not receive sufficient notice of a shareholders’ meeting to permit you to withdraw the ordinary shares underlying your ADSs to allow you to vote directly with respect to any specific matter. We will make all commercially reasonable efforts to cause the depositary to extend voting rights to you in a timely manner, but we cannot assure you that you will receive voting materials in time to instruct the depositary to vote, and it is possible that you, or persons who hold their ADSs through brokers, dealers or other third parties, will not have the opportunity to exercise a right to vote. Furthermore, the depositary will not be liable for any failure to carry out any instructions to vote, for the manner in which any vote is cast or for the effect of any such vote. As a result, you may not be able to exercise your right to vote and you may lack recourse if your ADSs are not voted as you request. In addition, in your capacity as an ADS holder, you will not be able to call a shareholders’ meeting. See “Description of American Depositary Shares.”
Holders of our ADSs may face limitations on transfer and withdrawal of underlying ordinary shares.
Our ADSs, which may be evidenced by American Depositary Receipts, or ADRs, are transferable on the books of the depositary. However, the depositary may close its books at any time or from time to time when it deems expedient in connection with the performance of its duties. The depositary may refuse to deliver, transfer or register transfers of your ADSs generally when our books or the books of the depositary are closed, or at any time if we or the depositary think it is advisable to do so because of any requirement of law, government or governmental body, or under any
59
Table of Contents
provision of the deposit agreement, or for any other reason subject to your right to cancel your ADSs and withdraw the underlying ordinary shares. Temporary delays in the cancellation of your ADSs and withdrawal of the underlying ordinary shares may arise because the depositary has closed its transfer books or we have closed our transfer books, the transfer of ordinary shares is blocked to permit voting at a shareholders’ meeting or we are paying a dividend on our ordinary shares. In addition, you may not be able to cancel your ADSs and withdraw the underlying ordinary shares when you owe money for fees, taxes and similar charges and when it is necessary to prohibit withdrawals in order to comply with any laws or governmental regulations that apply to ADSs or to the withdrawal of ordinary shares or other deposited securities. See “Description of American Depositary Shares.”
ADS holders may not be entitled to a jury trial with respect to claims arising under the deposit agreement, which could result in less favorable outcomes to the plaintiff(s) in any such action.
The deposit agreement governing the ADSs representing our ordinary shares provides that holders and beneficial owners of ADSs irrevocably waive the right to a trial by jury in any legal proceeding arising out of or relating to the deposit agreement or the ADSs, including in respect of claims under federal securities laws, against us or the depositary to the fullest extent permitted by applicable law. If this jury trial waiver provision is prohibited by applicable law, an action could nevertheless proceed under the terms of the deposit agreement with a jury trial. To our knowledge, the enforceability of a jury trial waiver under the federal securities laws has not been finally adjudicated by a federal court. However, we believe that a jury trial waiver provision is generally enforceable under the laws of the State of New York, which govern the deposit agreement, by a court of the State of New York or a federal court, which havenon-exclusive jurisdiction over matters arising under the deposit agreement, applying such law. In determining whether to enforce a jury trial waiver provision, New York courts and federal courts will consider whether the visibility of the jury trial waiver provision within the agreement is sufficiently prominent such that a party has knowingly waived any right to trial by jury. We believe that this is the case with respect to the deposit agreement and the ADSs. In addition, New York courts will not enforce a jury trial waiver provision in order to bar a viable setoff or counterclaim sounding in fraud or one which is based upon a creditor’s negligence in failing to liquidate collateral upon a guarantor’s demand, or in the case of an intentional tort claim (as opposed to a contract dispute), none of which we believe are applicable in the case of the deposit agreement or the ADSs. No condition, stipulation or provision of the deposit agreement or ADSs serves as a waiver by any holder or beneficial owner of ADSs or by us or the depositary of compliance with any provision of the federal securities laws. If you or any other holder or beneficial owner of ADSs brings a claim against us or the depositary in connection with such matters, you or such other holder or beneficial owner may not be entitled to a jury trial with respect to such claims, which may have the effect of limiting and discouraging lawsuits against us and/or the depositary. If a lawsuit is brought against us and/or the depositary under the deposit agreement, it may be heard only by a judge or justice of the applicable trial court, which would be conducted according to different civil procedures and may result in different outcomes than a trial by jury would have had, including results that could be less favorable to the plaintiff(s) in any such action, depending on, among other things, the nature of the claims, the judge or justice hearing such claims, and the venue of the hearing.
You may face difficulties in protecting your interests, and your ability to protect your rights through U.S. courts may be limited, because we are incorporated under Cayman Islands law and many of our directors reside outside of the United States.
We are an exempted company incorporated under the laws of the Cayman Islands. Our corporate affairs shall be governed by our Amended and Restated Memorandum and Articles of Association to be in effect upon the completion of this offering, referred to as our Articles of Association, the Companies Law (2018 Revision) of the Cayman Islands, referred to as the Companies Law, and the common law of the Cayman Islands. The rights of shareholders to take action against the directors, actions by minority shareholders and the fiduciary duties of our directors to us under Cayman Islands law are to a large extent governed by the common law of the Cayman Islands. The common law of the Cayman Islands is derived in part from comparatively limited judicial precedent in the Cayman Islands as well as from the common law of England and Wales, the decisions of whose courts are of persuasive authority, but are not binding, on a court in the Cayman Islands. Similarly, the rights of our shareholders and the fiduciary duties of our directors under Cayman Islands law are not as clearly established as they would be under statutes or judicial precedent in some jurisdictions in the United States. In particular, the Cayman Islands has a less developed body of securities laws than the United States, and some U.S. states, such as Delaware, have more fully developed and judicially interpreted bodies of corporate law than the Cayman Islands. As a Cayman Islands exempted company, we may not have standing to initiate a derivative action in a federal court of the United States.
60
Table of Contents
As a result, you may be limited in your ability to protect your interests if you are harmed in a manner that would otherwise enable you to sue in a United States federal court. In addition, shareholders of Cayman Islands companies may not have standing to initiate a shareholder derivative action in U.S. federal courts.
Shareholders of Cayman Islands exempted companies like us have very limited statutory rights under Cayman Islands law to inspect the corporate records of Cayman Islands exempted companies into which they are invested and have no statutory rights to obtain copies of registers of shareholders of Cayman Islands exempted companies. Although our shareholders may request access to our books and records, our directors have discretion under our Articles of Association to determine whether or not, and under what conditions, certain of our corporate records may be inspected by our shareholders. Under the Companies Law, shareholders are entitled to view our Articles of Association. This may make it more difficult for you to obtain the information needed to establish any facts necessary for a shareholder motion or to solicit proxies from other shareholders in connection with a proxy contest.
Certain corporate governance practices in the Cayman Islands, which is the jurisdiction of our incorporation, differ significantly from requirements for companies incorporated in other jurisdictions such as the United States. To the extent we choose to follow practice in the Cayman Islands with respect to corporate governance matters, our shareholders may be afforded less protection than they otherwise would under rules and regulations applicable to U.S. domestic issuers.
The Cayman Islands has no legislation specifically dedicated to the rights of investors in securities or statutorily defined private causes of action to investors in securities such as those found under the Securities Act of 1933, or the Securities Act, or the Exchange Act. Subject to limited exceptions, under Cayman Islands law, a shareholder is not entitled to bring a derivative action against the board of directors. U.S.-style class action lawsuits are not recognized in the Cayman Islands, but groups of shareholders with identical interests may bring representative proceedings in a similar fashion.
As a result of all of the above, our shareholders may have more difficulty in protecting their interests in the face of actions taken by management, or members of the board of directors than they would as public shareholders of a company incorporated in the United States. For a discussion of significant differences between the provisions of the Companies Law of the Cayman Islands and the laws applicable to companies incorporated in the United States and their shareholders, see “Description of Share Capital and Articles of Association—Material Differences in Corporate Law.”
The rights of our shareholders may differ from the rights typically offered to shareholders of a U.S. corporation.
Our corporate affairs and the rights of holders of ordinary shares are governed by our Articles of Association, the Companies Law, and the common law of the Cayman Islands. Certain rights and responsibilities of our shareholders, ADS holders and members of our board of directors under Cayman Islands law are different from those that apply to a Delaware corporation.
Directors of Cayman Islands exempted companies are required to observe certain fiduciary duties. These fiduciary duties are owed to the Cayman Islands company and include the duty to act in the best interests of the company and the shareholders as a whole. However, the fiduciary duties of a director of a Cayman Islands exempted company may not be the same as the fiduciary duty of a director of a U.S. corporation.
In addition, controlling shareholders of U.S. corporations owe fiduciary duties to minority shareholders, while shareholders (including controlling shareholders) of Cayman Islands companies generally owe no fiduciary duties to the company or other shareholders.
The rights of our shareholders to bring shareholders’ suits against us or our board of directors under Cayman Islands law are much more limited than those of shareholders of a U.S. corporation. For example, under Cayman Islands law, a shareholder who wishes to bring a claim against a director would generally need to obtain permission from the Grand Court of the Cayman Islands, or Cayman Islands Court, to bring a derivative action, in the name of the company, against the director. This is because the director of a Cayman Islands exempted company owes duties to the company and not to individual shareholders. As a result, our shareholders, including holders of ADSs, may have more difficulty protecting their rights in connection with actions taken by our directors than they would as shareholders of a U.S. corporation.
61
Table of Contents
Minority shareholders in a Cayman Islands exempted company have more limited rights than minority shareholders in a U.S. corporation in relation to mergers and similar transactions that the company may carry out. For example, if a merger under the Companies Law involving a Cayman Islands exempted company is approved by the requisite majority of shareholders, a dissenting minority shareholder would have the right to be paid the fair value of their shares (which, if not agreed between the parties, will, following the course of legal proceedings, be determined by the Cayman Islands Court) if the shareholders follow the statutorily prescribed procedure for initiating such proceedings, subject to certain exceptions. Such dissenter rights differ substantially from the appraisal rights, which would ordinarily be available to dissenting shareholders of Delaware corporations. Further, if a takeover offer is made to the shareholders of a Cayman Islands exempted company and accepted by holders of 90% of the shares affected, the offeror may require the holders of the remaining shares to transfer such shares on the terms of the offer. An objection can be made to the Cayman Islands Court, but this is unlikely to succeed in the case of an offer which has been so approved unless there is evidence of fraud, bad faith or collusion. A minority shareholder in this scenario would have no rights comparable to the appraisal rights which would generally be available to a dissenting shareholder of a U.S. corporation in similar circumstances. See the section of this prospectus titled “Description of Share Capital and Articles of Association” for a description of the principal differences between the provisions of Cayman Islands law applicable to us and the U.S. Delaware General Corporate Law relating to shareholders’ rights and protections.
62
Table of Contents
SPECIAL NOTE REGARDING FORWARD-LOOKING STATEMENTS AND INDUSTRY DATA
This prospectus contains forward-looking statements that involve substantial risks and uncertainties. These statements include all matters that are not related to present facts or current conditions or that are not historical facts, including statements regarding our strategy, future operations, future financial position, future revenue, projected costs, prospects, plans, objectives of management and expected market growth. These statements involve known and unknown risks, uncertainties and other important factors that may cause our actual results, performance or achievements to be materially different from any future results, performance or achievements expressed or implied by the forward-looking statements.
The words “anticipate,” “believe,” “estimate,” “expect,” “intend,” “may,” “plan,” “predict,” “project,” “would” and similar expressions are intended to identify forward-looking statements, although not all forward-looking statements contain these identifying words. These forward-looking statements include, among other things, statements regarding:
| ∎ | our plans to develop and commercialize elamipretide,SBT-20 and our other product candidates and to identify additional product candidates; |
| ∎ | ongoing and planned clinical trials and preclinical studies for our product candidates, includingSBT-272, including the timing of initiation of these trials and studies and the timing of the anticipated results; |
| ∎ | our plans to possibly enter into collaborations for the development of product candidates and the potential benefits of any collaboration; |
| ∎ | the timing of anticipated regulatory filings or regulatory approvals and plans and expectations for expedited regulatory review for our product candidates; |
| ∎ | the potentials advantages and clinical utility of our product candidates; |
| ∎ | our commercialization, marketing and manufacturing capabilities and strategy; |
| ∎ | our intellectual property position and strategy; |
| ∎ | our estimates regarding the potential market opportunity for our product candidates; |
| ∎ | our expectations related to the use of proceeds from this offering; and |
| ∎ | our estimates regarding expenses, future revenue, capital requirements, sufficiency of our current cash and cash equivalent and expected proceeds from this offering and our need for and ability to obtain additional funding. |
We may not actually achieve the plans, intentions or expectations disclosed in our forward-looking statements, and you should not place undue reliance on our forward-looking statements. Actual results or events could differ materially from the plans, intentions and expectations disclosed in the forward-looking statements we make. We have included important factors in the cautionary statements included in this prospectus, particularly in the “Risk Factors” section, that could cause actual results or events to differ materially from the forward-looking statements that we make. Except as context otherwise requires, our forward-looking statements do not reflect the potential impact of any future acquisitions, mergers, dispositions, joint ventures or investments that we may make.
You should read this prospectus, the documents that we reference in this prospectus and the documents that we have filed as exhibits to the registration statement of which this prospectus is a part completely and with the understanding that our actual future results may be materially different from what we expect. The forward-looking statements contained in this prospectus are made as of the date of this prospectus and we do not assume any obligation to update any forward-looking statements, whether as a result of new information, future events or otherwise, except as required by applicable law.
This prospectus includes statistical and other industry and market data, which we obtained from our own internal estimates and research, as well as from industry and general publications and research, surveys and studies conducted by third parties. Industry publications, studies and surveys generally state that they have been obtained from sources believed to be reliable, although they do not guarantee the accuracy or completeness of such information. While we believe that each of these studies, reports and publications is reliable, we have not independently verified market and industry data from third-party sources. While we believe our internal company research is reliable and the market definitions are appropriate, neither such research nor these definitions have been verified by any independent source.
63
Table of Contents
We estimate that the net proceeds from this offering will be approximately $73.0 million (or $84.2 million if the underwriters exercise their option to purchase additional ADSs in full), based on an assumed initial public offering price of $13.00 per ADS, which is the midpoint of the range set forth on the cover page of the prospectus, after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us.
Each $1.00 increase (decrease) in the assumed initial public offering price of $13.00 per ADS would increase (decrease) the net proceeds to us from this offering by $5.8 million, assuming the number of ADSs offered by us, as set forth on the cover page of this prospectus, remains the same and after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us. Each increase (decrease) of 1.0 million ADSs in the number of ADSs offered by us, as set forth on the cover page of this prospectus, would increase (decrease) our net proceeds from this offering by $12.1 million, assuming no change in the assumed initial public offering price per ADS and after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us.
As of September 30, 2018, we had cash and cash equivalents of $4.1 million. We currently estimate that we will use the net proceeds from this offering, together with our existing cash and cash equivalents, as follows:
| ∎ | approximately $25.0 million to fund the continued clinical development of elamipretide for the treatment of primary mitochondrial myopathy through pivotal data from a Phase 3 clinical trial; |
| ∎ | approximately $8.0 million to fund the continued clinical development of elamipretide for the treatment of Barth and LHON through anticipated upcoming regulatory interactions; |
| ∎ | approximately $8.0 million to fund the continued clinical development of elamipretide for the treatment of dry AMD through initiation of a Phase 2b clinical trial; |
| ∎ | approximately $6.0 million to fund the continued preclinical development ofSBT-272 throughIND-enabling studies and to fund a Phase 1 safety trial; |
| ∎ | approximately $10.4 million for principal and interest payments that we are obligated to make over the next 12 months under our term loan facility with Hercules; and |
| ∎ | the balance for working capital and other general corporate purposes, including advancement of our pipeline of discovery compounds. |
As of September 30, 2018, we had $20.0 million of outstanding principal under our term loan facility with Hercules and an additional $20.0 million of available borrowings, subject to achievement of specified milestones. Borrowings under the term loan facility bear interest at a floating per annum rate equal to the greater of (i) theWall Street Journal prime rate plus 5.50% or (ii) 9.50%. Beginning in December 2018, we are required to repay principal and interest on these borrowings in monthly installments through the scheduled maturity of January 1, 2021.
This expected use of net proceeds from this offering represents our intentions based upon our current plans and business conditions, which could change in the future as our plans and business conditions evolve. The amounts and timing of our actual expenditures may vary significantly depending on numerous factors, including the progress of our development of product candidates, the status of and results from clinical trials, as well as any collaborations that we may enter into with third parties, and any unforeseen cash needs. As a result, our management will retain broad discretion over the allocation of the net proceeds from this offering.
We anticipate that, assuming our current operating plan, the net proceeds from this offering, together with our existing cash and cash equivalents, will only be sufficient to allow us to complete a Phase 3 clinical trial for elamiptretide for primary mitochondrial myopathy, to initiate but not complete our planned Phase 2b clinical trial for the treatment of dry AMD, and to conduct a Phase 1 trial ofSBT-272. Based on our current operating plan, we will require additional capital to advance elamipretide through pivotal trials for indications other than primary mitochondrial myopathy and to advance our other product candidates through later-stage clinical development, as well as to commercialize any of our product candidates if we receive regulatory approval. We have based these estimates on assumptions that may prove to be wrong, including assumptions regarding the clinical trials necessary
64
Table of Contents
for FDA approval of our product candidates, and we could use our capital resources sooner than we currently expect. Due to the numerous risks and uncertainties associated with product development, including risks and uncertainties with respect to successful enrollment and completion of clinical trials, at this time we cannot reasonably estimate the amount of additional funding that will be necessary to complete the clinical development of any of our product candidates. If we receive regulatory approval for elamipretide,SBT-20 or any of our other product candidates, we expect to incur significant commercialization expenses related to product manufacturing, sales, marketing and distribution. Accordingly, we will be required to obtain further funding through public or private equity offerings, debt financings, collaborations and licensing arrangements or other sources.
Pending use of the proceeds as described above, we intend to invest the net proceeds in short-term, interest-bearing, investment-grade securities.
65
Table of Contents
We have never declared or paid any cash dividends on our share capital. We intend to retain all of our future earnings, if any, to finance the growth and development of our business, and we do not intend to pay cash dividends to the holders of our ordinary shares for the foreseeable future. In addition, the terms of our existing loan and security agreement preclude us from paying cash dividends without the consent of our lender. However, if we do pay a cash dividend on our ordinary shares in the future, we may only pay such dividend out of our profits or share premium (subject to applicable solvency requirements) under Cayman Islands law.
66
Table of Contents
The following table sets forth our cash and cash equivalents and capitalization as of September 30, 2018:
| ∎ | on an actual basis; |
| ∎ | on a pro forma basis giving effect to (i) the conversion of all outstanding Series A convertible preferred shares into 91,600,398 ordinary shares and (ii) the effectiveness of our Amended and Restated Memorandum and Articles of Association upon the completion of this offering; and |
| ∎ | on a pro forma as adjusted basis giving additional effect to (i) the issuance of 161,732,652 ordinary shares upon the conversion of our outstanding 2018 Notes in an aggregate principal amount of $132.4 million, assuming an initial public offering price of $13.00 per ADS (the midpoint of the estimated price range set forth on the cover page of this prospectus) and (ii) the sale of ADSs offered in this offering, assuming an initial public offering price of $13.00 per ADS, which is the midpoint of the range set forth on the cover page of this prospectus, after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us. |
You should read this information in conjunction with our consolidated financial statements and the related notes appearing at the end of this prospectus and the “Management’s Discussion and Analysis of Financial Condition and Results of Operations” section, the “Selected Consolidated Financial Data” section and other financial information contained in this prospectus.
| AS OF SEPTEMBER 30, 2018 | ||||||||||||
| ACTUAL | PRO FORMA | PRO FORMA AS ADJUSTED | ||||||||||
| (in thousands, except share data) | ||||||||||||
Cash and cash equivalents | $ | 4,078 | $ | 4,078 | $ | 77,038 | ||||||
|
|
|
|
|
| |||||||
Convertible notes payable | $ | 102,357 | $ | 102,357 | $ | — | ||||||
Long-term debt, less current portion | 12,467 | 12,467 | 12,467 | |||||||||
Series A convertible preferred shares, $0.0003 par value; 106,666,667 shares authorized, 91,600,398 issued and outstanding, actual; no shares authorized, issued or outstanding, pro forma and pro forma as adjusted | 211,377 | — | — | |||||||||
Shareholders’ (deficit) equity: | ||||||||||||
Ordinary Shares, $0.0003 par value; 203,333,333 shares authorized, 68,474,614 shares issued and outstanding, actual; 750,000,000 shares authorized, 160,075,012 shares issued and outstanding, pro forma; 750,000,000 shares authorized, 396,207,665 shares issued and outstanding, pro forma as adjusted | 21 | 48 | 119 | |||||||||
Additionalpaid-in capital | 39,206 | 250,556 | 439,630 | |||||||||
Accumulated deficit | (399,680 | ) | (399,680 | ) | (399,680 | ) | ||||||
|
|
|
|
|
| |||||||
Total shareholders’ (deficit) equity | (360,453 | ) | (149,076 | ) | 40,069 | |||||||
|
|
|
|
|
| |||||||
Total capitalization | $ | (34,252 | ) | $ | (34,252 | ) | $ | 52,536 | ||||
|
|
|
|
|
| |||||||
Each $1.00 increase (decrease) in the assumed initial public offering price of $13.00 per ADS, which is the midpoint of the range set forth on the cover page of this prospectus, would increase (decrease) the pro forma as adjusted amount of each of cash and cash equivalents, total shareholders’ equity (deficit) and total capitalization by $5.8 million, assuming that the number of ADSs offered by us, as set forth on the cover page of this prospectus, remains the same and after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us. Each increase (decrease) of 1.0 million ADSs in the number of ADSs offered by us at the assumed initial public offering price would increase (decrease) the pro forma as adjusted amount of each of cash and cash equivalents,
67
Table of Contents
total shareholders’ equity (deficit) and total capitalization by $12.1 million, assuming an initial public offering price of $13.00 per ADS, which is the midpoint of the range set forth on the cover page of this prospectus, after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us.
The table above does not include:
| ∎ | 15,550,986 ordinary shares issuable upon exercise of share options outstanding as of September 30, 2018, at a weighted-average exercise price of $1.05 per share; |
| ∎ | 9,965,096 ordinary shares available for future issuance as of September 30, 2018 under our 2006 share incentive plan, which shares will cease to be available for issuance following the closing of this offering; |
| ∎ | 47,692,934 ordinary shares reserved for issuance, in connection with this offering, under our 2019 share incentive plan, which plan includes provisions that automatically increase the number of ordinary shares reserved for issuance thereunder each year; |
| ∎ | 3,972,565 ordinary shares reserved for issuance, in connection with this offering, under our 2019 employee share purchase plan, which plan includes provisions that automatically increase the number of ordinary shares reserved for issuance thereunder each year; and |
| ∎ | 461,538 ordinary shares issuable upon exercise of an outstanding warrant with an exercise price equal to $1.08 per share (based on the assumed initial public offering price of $13.00 per ADS in this offering and reflected on an implied per ordinary share basis). |
68
Table of Contents
If you invest in the ADSs in this offering, your ownership interest will be immediately diluted to the extent of the difference between the initial public offering price per ADS and the pro forma as adjusted net tangible book value per ADS after this offering.
Our historical net tangible book value as of September 30, 2018 was approximately $(149.1) million, or $(2.18) per ordinary share and $(26.13) per ADS. Each ADS represents 12 ordinary shares. Our historical net tangible book value per share represents the amount of our total tangible assets less our total liabilities, divided by the number of ordinary shares outstanding as of September 30, 2018.
Our pro forma net tangible book value as of September 30, 2018 was $(149.1) million, or $(0.93) per ordinary share and $(11.18) per ADS. Pro forma net tangible book value per share represents our total tangible assets less our total liabilities, divided by the number of ordinary shares outstanding after giving effect to the conversion of all outstanding Series A convertible preferred shares into an aggregate of 91,600,398 ordinary shares, which will occur automatically upon the closing of this offering.
After giving further effect to (i) the issuance of 161,732,652 ordinary shares upon the conversion of our outstanding 2018 Notes in an aggregate principal amount of $132.4 million assuming an initial public offering price of $13.00 per ADS (the midpoint of the estimated price range set forth on the cover page of this prospectus) and (ii) the sale of 6,200,000 ADSs in this offering at an assumed initial public offering price of $13.00 per ADS, which is the midpoint of the range set forth on the cover page of this prospectus, after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us, our pro forma as adjusted net tangible book value as of September 30, 2018 would have been $40.1 million, or $0.10 per share and $1.21 per ADS. This amount represents an immediate increase in pro forma net tangible book value of $1.03 per share to our existing shareholders and an immediate dilution in pro forma net tangible book value of $11.79 per ADS to new investors purchasing ADSs in this offering.
The following table illustrates dilution on a per ADS basis:
Assumed initial public offering price per ADS | $ | 13.00 | ||||||
Historical net tangible book value per ADS as of September 30, 2018 | $ | (26.13 | ) | |||||
|
| |||||||
Pro forma net tangible book value per ADS as of September 30, 2018 | (11.18 | ) | ||||||
Increase in pro forma as adjusted net tangible book value attributable to investors purchasing ADSs in this offering | 12.39 | |||||||
|
| |||||||
Pro forma as adjusted net tangible book value per ADS after this offering | 1.21 | |||||||
|
| |||||||
Dilution per ADS to new investors | $ | 11.79 | ||||||
|
|
Each $1.00 increase (decrease) in the assumed initial public offering price of $13.00 per ADS would increase (decrease) the pro forma as adjusted net tangible book value by $5.8 million, the pro forma as adjusted net tangible book value per ADS by $0.17 and the dilution per ADS to investors in this offering by $0.83 per ADS, assuming that the number of ADSs offered by us, as set forth on the cover page of this prospectus, remains the same and after deducting the estimated underwriting discount and offering expenses payable by us. An increase of 1.0 million ADSs in the number of ADSs offered by us, as set forth on the cover page of this prospectus, would increase our pro forma as adjusted net tangible book value per ADS after this offering by $0.32 and decrease the dilution per ADS to investors in this offering by $0.32, assuming no change in the assumed initial public offering price per ADS and after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us. A decrease of 1.0 million ADSs in the number of ADSs offered by us, as set forth on the cover page of this prospectus, would decrease our pro forma as adjusted net tangible book value per ADS after this offering by $0.34 and increase the dilution per ADS to investors in this offering by $0.34, assuming no change in the assumed initial public offering price and after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us.
69
Table of Contents
If the underwriters exercise their option to purchase additional ADSs in full in this offering, the pro forma as adjusted net tangible book value per ADS would be $1.04, the increase in pro forma net tangible book value per ADS to existing shareholders would be $12.22 and the dilution per ADS to new investors would be $11.96, in each case based on an assumed initial public offering price of $13.00 per ADS.
The following table summarizes, on a pro forma as adjusted basis as of September 30, 2018, the differences between the number of shares (including in the form of ADSs) purchased from us, the total consideration in respect of such shares and the average price per share paid by existing shareholders and to be paid by new investors. The calculation below is based on an assumed initial public offering price of $13.00 per ADS, before deducting the underwriting discounts and commissions and estimated offering expenses payable by us.
| ORDINARY SHARES PURCHASED | TOTAL CONSIDERATION | AVERAGE PRICE PER SHARE | ||||||||||||||||||
| NUMBER | PERCENT | AMOUNT | PERCENT | |||||||||||||||||
Existing shareholders | 321,807,665 | 81.2 | % | $ | 381,196,120 | 82.5 | % | $ | 1.18 | |||||||||||
New investors | 74,400,000 | 18.8 | 80,600,000 | 17.5 | 1.08 | |||||||||||||||
|
|
|
|
|
|
|
| |||||||||||||
Total | 396,207,665 | 100 | % | $ | 461,796,120 | 100 | % | 1.17 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||||||
Our existing principal shareholder, Morningside Venture (I) Investments Limited, certain entities associated with it, certain of the holders of our outstanding convertible notes and entities associated with such holders have indicated an interest in purchasing up to an aggregate of approximately $60.0 million of ADSs in this offering at the initial public offering price and on the same terms as the other purchasers in this offering. However, because indications of interest are not binding agreements or commitments to purchase, these persons may determine to purchase fewer ADSs than they indicate an interest in purchasing or not to purchase any ADSs in this offering. It is also possible that these persons could purchase more ADSs in this offering. In addition, the underwriters could determine to sell fewer ADSs to any of these persons than they indicate an interest in purchasing or not to sell any ADSs to such persons. The table above does not reflect any potential purchases by these potential purchasers.
If the underwriters exercise their option to purchase additional ADSs in full:
| ∎ | the percentage of ordinary shares held by existing shareholders will decrease to 79.0% of the total number of ordinary shares outstanding after this offering; and |
| ∎ | the number of shares (including in the form of ADSs) held by new investors will increase to 85,560,000 shares, or 21.0% of the total number of ordinary shares outstanding after this offering. |
The foregoing tables and calculations are based on the number of ordinary shares outstanding as of September 30, 2018, after giving effect to (i) the issuance of 161,732,652 ordinary shares upon the conversion of our outstanding convertible notes in an aggregate principal amount of $132.4 million, assuming an initial public offering price of $13.00 per share (the midpoint of the estimated price range set forth on the cover page of this prospectus), and (ii) the conversion of all outstanding Series A convertible preferred shares into an aggregate of 91,600,398 ordinary shares upon the closing of this offering, and exclude:
| ∎ | 15,550,986 ordinary shares issuable upon exercise of share options outstanding as of September 30, 2018 at a weighted-average exercise price of $1.05 per share; |
| ∎ | 9,965,096 ordinary shares available for future issuance as of September 30, 2018 under our 2006 share incentive plan, which shares will cease to be available for issuance following the closing of this offering; |
| ∎ | 47,692,934 ordinary shares reserved for issuance, in connection with this offering, under our 2019 share incentive plan, which plan includes provisions that automatically increase the number of ordinary shares reserved for issuance thereunder each year; |
70
Table of Contents
| ∎ | 3,972,565 ordinary shares reserved for issuance, in connection with this offering, under our 2019 employee share purchase plan, which plan includes provisions that automatically increase the number of ordinary shares reserved for issuance thereunder each year; and |
| ∎ | 461,538 ordinary shares issuable upon exercise of an outstanding warrant with an exercise price equal to $1.08 per share (based on the assumed initial public offering price of $13.00 per ADS in this offering and reflected on an implied per ordinary share basis). |
71
Table of Contents
SELECTED CONSOLIDATED FINANCIAL DATA
We have derived the following selected of consolidated statement of operations data for the fiscal years ended December 31, 2016 and 2017 and the summary consolidated balance sheet data as of December 31, 2016 and 2017 from our audited consolidated financial statements appearing elsewhere in this prospectus. The consolidated statements of operations data for the nine months ended September 30, 2017 and 2018 and the consolidated balance sheet data as of September 30, 2018 have been derived from our unaudited condensed consolidated financial statements included elsewhere in this prospectus and have been prepared on the same basis as the audited consolidated financial statements. In the opinion of management, the unaudited data reflects all adjustments, consisting only of normal recurring adjustments, necessary for a fair presentation of the financial information contained in those statements. Our historical results are not necessarily indicative of the results that should be expected for any future period. The selected consolidated financial data set forth below should be read together with our consolidated financial statements and the related notes to those statements, as well as the section of this prospectus captioned “Management’s Discussion and Analysis of Financial Condition and Results of Operations.”
| YEAR ENDED DECEMBER 31, | NINE MONTHS ENDED SEPTEMBER 30, | |||||||||||||||
| 2016 | 2017 | 2017 | 2018 | |||||||||||||
| (in thousands, except share and per share data) | ||||||||||||||||
Consolidated Statement of Operations Data: | ||||||||||||||||
Operating expenses: | ||||||||||||||||
Research and development | $ | 48,445 | $ | 63,220 | $ | 46,212 | $ | 41,758 | ||||||||
General and administrative | 13,403 | 16,500 | 12,937 | 12,541 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Total operating expenses | 61,848 | 79,720 | 59,149 | 54,299 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Loss from operations | (61,848 | ) | (79,720 | ) | (59,149 | ) | (54,299 | ) | ||||||||
|
|
|
|
|
|
|
| |||||||||
Other (expense) income, net | 799 | (3,190 | ) | (1,691 | ) | (15,824 | ) | |||||||||
|
|
|
|
|
|
|
| |||||||||
Net loss attributable to ordinary shareholders | $ | (61,049 | ) | $ | (82,910 | ) | $ | (60,840 | ) | $ | (70,123 | ) | ||||
|
|
|
|
|
|
|
| |||||||||
Net loss per share attributable to ordinary shareholders—basic and diluted (1) | $ | 0.90 | $ | 1.21 | $ | 0.89 | $ | 1.02 | ||||||||
|
|
|
|
|
|
|
| |||||||||
Weighted-average ordinary shares used in net loss per share attributable to ordinary shareholders—basic and diluted (1) | 68,165,325 | 68,472,262 | 68,471,469 | 68,474,614 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Pro forma net loss per share attributable to ordinary shareholders—basic and diluted (unaudited)(1) | $ | (0.43 | ) | $ | (0.24 | ) | ||||||||||
|
|
|
| |||||||||||||
Pro forma weighted-average ordinary shares used in net loss per share attributable to ordinary shareholders—basic and diluted (unaudited) (1) | 188,261,368 | 238,105,715 | ||||||||||||||
|
|
|
| |||||||||||||
| (1) | See Notes 2 and 15 to our audited consolidated financial statements and notes 2 and 13 to our unaudited interim condensed consolidated financial statements appearing elsewhere in this prospectus for further details on the calculation of basic and diluted net loss per share attributable to ordinary shareholders and pro forma basic and diluted net loss per share attributable to ordinary shareholders. |
72
Table of Contents
| AS OF DECEMBER 31, | AS OF SEPTEMBER 30, 2018 | |||||||||||
| 2016 | 2017 | |||||||||||
| (in thousands) | ||||||||||||
Consolidated Balance Sheet Data: | ||||||||||||
Cash and cash equivalents | $ | 9,710 | $ | 4,119 | $ | 4,078 | ||||||
Working capital deficit | (338 | ) | (18,675 | ) | (31,027 | ) | ||||||
Net assets | 1,546 | (79,909 | ) | (149,076 | ) | |||||||
Total assets | 13,322 | 7,155 | 11,630 | |||||||||
Total Series A convertible preferred shares | 211,377 | 211,377 | 211,377 | |||||||||
Total accumulated deficit | (246,647 | ) | (329,557 | ) | (399,680 | ) | ||||||
Total shareholders’ deficit | (209,831 | ) | (291,286 | ) | (360,453 | ) | ||||||
73
Table of Contents
MANAGEMENT’S DISCUSSION AND ANALYSIS OF
FINANCIAL CONDITION AND RESULTS OF OPERATIONS
The following discussion and analysis of our financial condition and results of operations should be read together with our consolidated financial statements and related notes and other financial information appearing elsewhere in this prospectus. Some of the information contained in this discussion and analysis or set forth elsewhere in this prospectus, including information with respect to our plans and strategy for our business and related financing, includes forward-looking statements that involve risks and uncertainties. As a result of many factors, including those factors set forth in the “Risk Factors” section of this prospectus, our actual results could differ materially from the results described in or implied by the forward-looking statements contained in the following discussion and analysis.
Overview
We are a clinical-stage biotechnology company focused on the discovery, development and commercialization of novel therapies for diseases involving mitochondrial dysfunction. Mitochondria, found in nearly every cell in the body, are the body’s main source of energy production and are critical for normal organ function. Dysfunctional mitochondria characterize a number of rare genetic diseases, collectively known as primary mitochondrial diseases, and are also involved in many commonage-related diseases. We believe our lead product candidate, elamipretide, has the potential to treat both rare genetic and commonage-related mitochondrial diseases. Our mission is to be the leader in mitochondrial medicine, and we have assembled a highly experienced management team, board of directors and group of scientific advisors to help us achieve this mission.
We are studying elamipretide in the following indications:
Primary mitochondrial myopathy. Primary mitochondrial myopathy, characterized by debilitating skeletal muscle weakness, exercise intolerance and fatigue, which we believe affects an estimated 40,000 diagnosed individuals in the United States. There are no therapies approved by the FDA, the EMA or the NMPA, for the treatment of this indication. We have received Fast Track and Orphan Drug designation from the FDA for the development of elamipretide in this indication. We are conducting a Phase 3 pivotal trial in North America and in Europe and expect to have data from that trial by the end of 2019.
Barth. Barth, characterized by heart muscle weakness, or cardiomyopathy, neutropenia, or low white blood cell count (which may lead to an increased risk for infections), skeletal muscle weakness, delayed growth, fatigue and varying degrees of physical disability, is estimated to affect between one in 300,000 to one in 400,000 births in the United States and there are estimated to be less than 200 known living patients worldwide with Barth. There are no therapies approved by the FDA, EMA or NMPA for the treatment of Barth. We have received Fast Track and Orphan Drug designation from the FDA for the development of elamipretide in this indication. In December 2018, we completed the placebo-controlled portion of a Phase 2/3 clinical trial in patients with Barth. While the trial did not reach its primary endpoints, we observed trends toward improvement in the subset of patients with lower ratios of monolysocardiolipin to tetralinoleylcardiolipin, which we believe are the patients most likely to respond to therapy. We plan to meet with the FDA during the first half of 2019 to discuss a potential NDA submission.
LHON.LHON is characterized by central vision loss. We estimate that LHON affects approximately 10,000 individuals in the United States, of whom an estimated 70% have the genetic mutation, G11778A, that we are studying. There are no therapies approved by the FDA or NMPA for the treatment of LHON, and there is only oneEMA-approved therapy. We have received Fast Track and Orphan Drug designation from the FDA for the development of elamipretide in this indication. We completed the placebo-controlled portion of a Phase 2 clinical trial during the first half of 2018, and continue to follow patients in open-label extension. While the trial did not reach its primary endpoint of change in best corrected visual acuity, we observed trends favoring elamipretide across a number of endpoints, and we are continuing to observe improvements in an ongoing open-label extension. We plan to meet with the FDA for an end-of-Phase 2 meeting during the first half of 2019. Following that meeting, we plan to submit a clinical trial application to the NMPA for inclusion of clinical trial sites in China in a potential Phase 3 clinical trial.
Dry AMD. Dry AMD, characterized by symptoms such as distorted vision, reduction in low light visual acuity, reduced overall visual acuity and blurred vision, is estimated to affect over 10 million individuals in the United States,
74
Table of Contents
representing 90% of all individuals with AMD in the United States, and is the leading cause of blindness among older adults in the developed world. There are no therapies approved by the FDA, EMA or NMPA for the treatment of dry AMD. We completed a Phase 1 trial in patients with drusen, an early form of dry AMD, and geographic atrophy, an advanced form of dry AMD, in which we observed statistically significant improvement over baseline in various parameters of visual function in both the drusen and geographic atrophy cohorts. We received Fast Track designation from the FDA for the development of elamipretide for patients with Dry AMD with geographic atrophy in November 2018. We plan to launch a Phase 2b clinical trial for the treatment of patients with geographic atrophy in the first quarter of 2019.
In addition to our clinical development programs for elamipretide, we plan to evaluateSBT-20, our second clinical-stage product candidate, for rare disease indications, such as peripheral neuropathies. We are developingSBT-272, a preclinical-stage product candidate, for rare neurodegenerative diseases. In addition, our internal discovery platform has generated a library of over 100 proprietary, differentiated compounds which could have clinical benefit for diseases related to mitochondrial dysfunction and from which we plan to designate potential product candidates. We may also utilize certain of these compounds as part of our carrier platform, in which they could potentially serve as scaffolds to deliver other beneficial compounds to the mitochondria.
Since our inception in 2006, we have devoted substantially all of our resources to organizing and staffing our company, business planning, raising capital, acquiring and developing our proprietary technology, identifying potential product candidates and conducting preclinical and clinical studies of our product candidates. We have not generated any product revenue and have financed our operations primarily through the private placement of Series A convertible preferred shares and convertible notes and borrowings under a term loan. As of September 30, 2018, we have raised an aggregate of $362.6 million in gross proceeds from private placements of our securities and borrowings under the term loan. As of September 30, 2018, our principal source of liquidity was cash and cash equivalents, which totaled $4.1 million.
As of September 30, 2018, we had an accumulated deficit of $399.7 million. Our net loss was $61.0 million and $82.9 million for the years ended December 31, 2016 and 2017, respectively, and $70.1 million for the nine months ended September 30, 2018. We have incurred significant net operating losses in every year since our inception and expect to continue to incur increasing net operating losses and significant expenses for the foreseeable future. Our net losses may fluctuate significantly from quarter to quarter and year to year. We anticipate that our expenses will increase significantly as we:
| ∎ | continue to advance our clinical programs and initiate additional clinical programs; |
| ∎ | continue our current research programs and development activities; |
| ∎ | seek to identify additional research programs and additional product candidates; |
| ∎ | initiate preclinical testing and clinical trials for any product candidates we identify; |
| ∎ | develop, maintain, expand and protect our intellectual property portfolio; |
| ∎ | hire additional research, clinical and scientific personnel; and |
| ∎ | incur additional costs associated with operating as a public company, including expanding our operational, finance and management teams. |
We believe that our available funds subsequent to this offering will be sufficient to fund our operations for the next 12 months. We do not expect to generate revenues from product sales unless and until we successfully complete development and obtain regulatory approval for a product candidate, which is subject to significant uncertainty. We currently use contract research organizations, or CROs, and contract manufacturing organizations, or CMOs, to carry out our preclinical and clinical development activities, and we do not yet have a commercial organization. If we obtain regulatory approval for our product candidates, we expect to incur significant commercialization expenses related to product sales, marketing, manufacturing and distribution. Accordingly, we may seek to fund our operations through public or private equity or debt financings or other sources, including strategic collaborations. We may, however, be unable to raise additional funds or enter into such other arrangements when needed on favorable terms, if at all. Our failure to raise capital or enter into such other arrangements as and when needed would have a negative impact on our financial condition and our ability to develop our current product candidates, or any additional product candidates, if developed.
75
Table of Contents
Without giving effect to the anticipated net proceeds from this offering, we expect that our existing cash will be sufficient to fund our operating expenses and capital expenditure requirements into the first quarter of 2019. Beyond that point, we will need to raise additional capital to finance our operations, which cannot be assured. We have concluded that this circumstance raises substantial doubt about our ability to continue as a going concern within one year after the issuance date of our consolidated financial statements for the nine-months ended September 30, 2018. See Note 1 to our unaudited interim condensed consolidated financial statements appearing at the end of this prospectus for additional information on our assessment.
Similarly, in its report on our consolidated financial statements for the year ended December 31, 2017, our independent registered public accounting firm included an explanatory paragraph stating that our recurring losses from operations since inception and required additional funding to finance our operations raise substantial doubt about our ability to continue as a going concern.
Financial Overview
Revenue
We have not generated any revenue from product sales or otherwise and do not expect to do so in the near future. We expect that any revenue will be less than our expenses for the foreseeable future and that we will experience increasing losses as we continue our development of, and seek regulatory approvals for, our product candidates and begin to commercialize any approved products. Our ability to generate revenues for any product candidate for which we receive regulatory approval will depend on numerous factors, including competition, commercial manufacturing capability and market acceptance of our products.
Research and Development Expenses
Research and development expenses consist primarily of costs incurred for our research activities, including development of our preclinical and clinical product candidates, which include:
| ∎ | employee-related expenses, including salaries, benefits and share-based compensation expense; |
| ∎ | expenses incurred under agreements with CROs, CMOs and independent contractors that conduct research and development, preclinical and clinical activities on our behalf; |
| ∎ | costs of purchasing lab supplies andnon-capital equipment used in our preclinical activities and in manufacturing preclinical study and clinical trial materials; |
| ∎ | consulting, licensing and professional fees related to research and development activities; and |
| ∎ | facility costs, depreciation and other expenses, which include direct and allocated expenses for rent and maintenance of facilities, insurance and other supplies. |
We expense research and development costs as incurred. We recognize costs for certain development activities, such as preclinical studies and clinical trials, based on an evaluation of the progress to completion of specific tasks using information provided to us by our vendors such as patient enrollment or clinical site activations for services received and efforts expended.
Research and development activities are central to our business model. We expect research and development costs to increase significantly for the foreseeable future as our current development programs progress and new programs are added.
76
Table of Contents
We track certain external research and development expenses for our lead product candidates. We manage certain activities, such as contract research and manufacturing of our product candidates and our discovery programs, through our third-party vendors and have captured the costs of these activities on an individual product basis from our financial records. We use our employee, consultant and infrastructure resources across our development programs and do not track and do not allocate the cost of these activities on aprogram-by-program basis. The following summarizes our research and development expenses:
| YEAR ENDED DECEMBER 31, | NINE MONTHS ENDED SEPTEMBER 30, | |||||||||||||||
| 2016 | 2017 | 2017 | 2018 | |||||||||||||
(in thousands) | ||||||||||||||||
Product expenses: | ||||||||||||||||
Elamipretide | $ | 30,775 | $ | 40,530 | $ | 30,365 | $ | 26,115 | ||||||||
SBT-20 | 1,090 | 1,697 | 1,261 | 615 | ||||||||||||
SBT-272 | — | — | — | 332 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Total costs directly allocated to products | 31,865 | 42,227 | 31,626 | 27,062 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Expenses not directly allocated to products: | ||||||||||||||||
Research and development programs | 4,468 | 6,179 | 3,296 | 2,563 | ||||||||||||
Consultants and professional expenses | 3,921 | 4,457 | 3,706 | 4,094 | ||||||||||||
Employee expenses, including cash compensation, benefits and share-based compensation | 8,191 | 10,357 | 7,584 | 8,038 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Total expenses not directly allocated to products | 16,580 | 20,993 | 14,586 | 14,696 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Total research and development expenses | $ | 48,445 | $ | 63,220 | $ | 46,212 | $ | 41,758 | ||||||||
|
|
|
|
|
|
|
| |||||||||
Because of the numerous risks and uncertainties associated with product development, we cannot determine with certainty the duration and completion costs of the current or future preclinical studies and clinical trials or if, when, or to what extent we will generate revenues from the commercialization and sale of our product candidates. We may never succeed in achieving regulatory approval for any of our product candidates. The duration, costs and timing of preclinical studies and clinical trials and development of our product candidates will depend on a variety of factors, including:
| ∎ | successful completion of preclinical studies and investigational new drug-enabling studies; |
| ∎ | successful enrollment in and completion of clinical trials; |
| ∎ | receipt of marketing approvals from applicable regulatory authorities; |
| ∎ | establishing commercial manufacturing capabilities or making arrangements with third-party manufacturers; |
| ∎ | obtaining and maintaining patent and trade secret protection andnon-patent exclusivity; |
| ∎ | launching commercial sales of the product, if and when approved, whether alone or in collaboration with others; |
| ∎ | acceptance of the product, if and when approved, by patients, the medical community and third-party payors; |
| ∎ | effectively competing with other therapies and treatment options; |
| ∎ | continued acceptable safety profile following approval; |
| ∎ | enforcing and defending intellectual property and proprietary rights and claims; and |
| ∎ | achieving desirable therapeutic properties for the intended indications. |
A change in the outcome of any of these factors could mean a significant change in the costs and timing associated with the development of our current and future preclinical and clinical product candidates. For example, if the FDA or other regulatory authority were to require us to conduct clinical trials beyond those that we currently anticipate will be required for the completion of clinical development, or if we experience significant delays in execution of or
77
Table of Contents
enrollment in any of our preclinical studies or clinical trials, we could be required to expend significant additional financial resources and time on the completion of preclinical and clinical development. We expect our research and development expenses to increase for the foreseeable future as we continue the development of product candidates.
General and Administrative Expenses
General and administrative expenses consist primarily of employee-related expenses, including salaries, benefits and share-based compensation for personnel in executive, finance,pre-commercial, facility operations and administrative functions. Significant costs are incurred in ourpre-commercial activities including market research, public relations, patient advocacy, advisory boards and conferences and professional consulting. Other significant costs include facility costs not otherwise included in research and development expenses, legal fees relating to intellectual property and patent prosecution and maintenance, other legal fees and fees for accounting, tax and consulting services.
We anticipate that our general and administrative expenses will increase in the future to support continued research and development activities, potential commercialization of our product candidates and increased costs of operating as a public company. These increases will likely include costs related to the hiring of additional personnel and fees to outside consultants, attorneys and accountants, among other expenses. We expect the increased costs associated with being a public company to include expenses related to services associated with maintaining compliance with the requirements of Nasdaq and the SEC, director and officer insurance and investor and public relations costs.
Other Income (Expense), Net
Other income (expense), net, primarily consists of interest expense incurred on convertible notes payable and incurred on our term loan facility, interest income earned on a shareholder demand note receivable and on cash and cash equivalents and changes in the fair value of our warrant liability.
Results of Operations
Comparison of the Nine Months Ended September 30, 2017 and 2018
The following table summarizes our results of operations for the nine months ended September 30, 2017 and 2018, together with the dollar change in those items:
| NINE MONTHS ENDED SEPTEMBER 30, | DOLLAR CHANGE | |||||||||||
| 2017 | 2018 | |||||||||||
| (in thousands) | ||||||||||||
Operating expenses: | ||||||||||||
Research and development | $ | 46,212 | $ | 41,758 | $ | (4,454 | ) | |||||
General and administrative | 12,937 | 12,541 | (396 | ) | ||||||||
|
|
|
|
|
| |||||||
Total operating expenses | 59,149 | 54,299 | (4,850 | ) | ||||||||
Loss from operations | (59,149 | ) | (54,299 | ) | 4,850 | |||||||
Other income/(expense), net | (1,691 | ) | (15,824 | ) | (14,133 | ) | ||||||
|
|
|
|
|
| |||||||
Net loss | $ | (60,840 | ) | $ | (70,123 | ) | $ | (9,283 | ) | |||
|
|
|
|
|
| |||||||
Research and Development Expenses
Research and development expenses decreased by $4.4 million to $41.8 million for the nine months ended September 30, 2018 from $46.2 million for the nine months ended September 30, 2017. This decrease was primarily due to a $3.6 million net decrease in clinical trial related costs as several trials ended in 2018, offset by increased costs associated with our Phase 3 primary mitochondrial myopathy trial, which was active for only a small portion of the nine months ended September 30, 2017. Consulting and professional services increased by $1.0 million as we began integrated safety summary reporting and new drug application initiatives.
General and Administrative Expenses
General and administrative expenses decreased by $0.4 million to $12.5 million for the nine months ended September 30, 2018 from $12.9 million for the nine months ended September 30, 2017. The decrease in general and administrative expenses was primarily attributable to a $1.3 million reduction in legal and professional costs
78
Table of Contents
partially offset by an increase in intellectual property expenses of $0.6 million and an increase in pre-commercial activities of $0.3 million.
Other Income (Expense)
Other expense increased by $14.1 million to $15.8 million for the nine months ended September 30, 2018 from $1.7 million for the nine months ended September 30, 2017. This increase was driven by (i) interest expense recorded as a result of the debt discount on the convertible debt of $7.8 million, (ii) an increase in interest expense of $4.8 million due to the debt being for the full nine month period in 2018 and (iii) interest expense on additional convertible debt and an additional advance on our term loan facility. The change in valuation of our warrant liability was $1.7 million. This increase in other expense was partially offset by increased interest income of $0.1 million, as we had greater bank balances in 2018, and a $0.1 million gain on the change in the warrant liability valuation.
Comparison of the Years Ended December 31, 2016 and 2017
The following table summarizes our results of operations for the years ended December 31, 2016 and 2017, together with the dollar change in those items:
| YEAR ENDED DECEMBER 31, | DOLLAR CHANGE | |||||||||||
| 2016 | 2017 | |||||||||||
| (in thousands) | ||||||||||||
Operating expenses: | ||||||||||||
Research and development | $ | 48,445 | $ | 63,220 | $ | 14,775 | ||||||
General and administrative | 13,403 | 16,500 | 3,097 | |||||||||
|
|
|
|
|
| |||||||
Total operating expenses | 61,848 | 79,720 | 17,872 | |||||||||
|
|
|
|
|
| |||||||
Loss from operations | (61,848 | ) | (79,720 | ) | (17,872 | ) | ||||||
Other income (expense), net | 799 | (3,190 | ) | (3,989 | ) | |||||||
|
|
|
|
|
| |||||||
Net loss | $ | (61,049 | ) | $ | (82,910 | ) | $ | (21,861 | ) | |||
|
|
|
|
|
| |||||||
Research and Development Expenses
Research and development expenses increased by $14.8 million to $63.2 million for the year ended December 31, 2017 from $48.4 million for the year ended December 31, 2016. This increase was primarily due to a $10.2 million increase in clinical trial related costs, mainly relating to our primary mitochondrial myopathy program, which increased by $4.4 million due to initiation of ourpre-Phase 3 trial registry and Phase 3 clinical trial, a $2.9 million increase in manufacturing costs for elamipretide and a $1.6 million increase in employee-related costs as we expanded our team to support later stage clinical development.
General and Administrative Expenses
General and administrative expenses increased by $3.1 million to $16.5 million for the year ended December 31, 2017 from $13.4 million for the year ended December 31, 2016. The increase in administrative expenses was primarily attributable to an increase of $2.8 million in legal and professional costs related to a potential financing initiative that was deferred to 2018 due to market considerations, as well as an increase of approximately $0.3 million in market research activities.
Other Income (Expense)
Other income (expense) was $3.2 million of other expense for the year ended December 31, 2017, consisting primarily of interest expense in connection with convertible promissory notes issued in 2017 and interest expense related to our term loan facility, which we entered into in June 2017. Other income (expense) was $0.8 million in other income for the year ended December 31, 2016, consisting of interest received on a note receivable, which was repaid in full by the end of 2016.
79
Table of Contents
Liquidity and Capital Resources
Overview
We have funded our operations from inception through September 30, 2018 primarily through gross proceeds of $362.6 million from the sale of Series A convertible preferred shares, the issuance of convertible promissory notes, and a term loan. As of September 30, 2018, we had cash and cash equivalents of $4.1 million.
Indebtedness
Term Loan Facility
On June 30, 2017, we entered into a loan and security agreement providing for a $40.0 million term loan facility with Hercules Capital, Inc., or Hercules, which we refer to as the term loan facility. The loan and security agreement was amended in March 2018, July 2018 and October 2018.
Borrowings under the term loan facility bear interest at a floating per annum rate equal to the greater of (i) theWall Street Journal prime rate plus 5.50% or (ii) 9.50%. In an event of default, as defined in the loan and security agreement, the interest rate applicable to borrowings under such agreement will be increased by 4.0%. Interest payments are due monthly in arrears. Under the term loan facility, as amended, we make interest only payments through November 30, 2018, at which time payments are made in equal monthly installments of principal and interest, continuing through the scheduled maturity date of January 1, 2021.
We may voluntarily prepay all, but not less than all, of the outstanding principal at any time prior to the maturity date, subject to a prepayment fee, which ranges from 0.5% to 3.0% of the outstanding principal depending on when the prepayment is made. A final payment of $1.25 million is due upon the earlier to occur of the maturity of the loan, the acceleration or prepayment of all outstanding principal or the termination of the term loan facility.
Borrowings under the term loan facility are secured by a first priority lien on all of our assets, excluding our intellectual property. We have agreed to a negative pledge on our intellectual property. The term loan facility contains customary events of default and affirmative and negative covenants, including restrictions on our ability to pay dividends and incur additional debt, but does not contain any financial covenants. An event of default had not occurred as of September 30, 2018.
In connection with our entry into the term loan facility, we issued to Hercules a warrant to purchase our ordinary shares. See “Description of Share Capital and Articles of Association—Warrant” for a description of the warrant.
Convertible Notes
During 2017, pursuant to a note purchase agreement with Morningside Venture (I) Investments Limited, or MVIL, as the same was amended and restated, we issued convertible promissory notes to MVIL in an aggregate principal amount of $50.0 million, or the 2017 Shareholder Notes. In January 2018, we entered into a note exchange agreement with MVIL pursuant to which MVIL exchanged the 2017 Shareholder Notes for a new convertible note in the principal amount of $52.4 million, representing the aggregate principal amount of the 2017 Shareholder Notes plus accrued interest, or the January 2018 Shareholder Note. The exchange terminated the existing 2017 Shareholder Notes. The January 2018 Shareholder Note has substantially the same terms as the notes described in the following paragraph.
In January 2018, we entered into a note purchase agreement with new investors, or the 2018 Note Purchase Agreement. Under the 2018 Note Purchase Agreement, as subsequently amended, we issued convertible promissory notes in the aggregate principal amount of $50.0 million, or the 2018 New Investor Notes. The 2018 New Investor Notes accrue interest at 7% per annum, which compounds annually, and upon such compounding, is added to the outstanding principal amount. The 2018 New Investor Notes are convertible upon a qualified financing, which means (i) the closing of an initial public offering or (ii) a subsequent financing occurring after January 10, 2019. Effective upon the closing of a qualified financing, the outstanding principal and accrued interest plus a 25% premium, defined as the sum of principal plus interest multiplied by 25%, will automatically convert into shares of the same class and series of our shares issued to other investors in the qualified financing at the same price per share. Unless earlier repaid, retired, discharged, or automatically converted into our shares, all amounts outstanding become due and payable on the later of (i) January 10, 2020 and (ii) five business days after the date on which the term loan with Hercules is repaid, terminated and discharged in full.
80
Table of Contents
In October 2018, we entered into an additional note purchase agreement with MVIL, under which we have borrowed an aggregate principal amount of $30.0 million pursuant to notes issued in October 2018, December 2018 and January 2019. The notes issued under the October 2018 note purchase agreement are convertible upon a qualified initial public offering, or qualified IPO, in the United States at the qualified IPO price per share giving effect to any applicable ratio of ADS to ordinary shares. A qualified IPO is defined under these notes as firm commitment underwritten public offering of ordinary shares or ADSs in which aggregate gross proceeds equal or exceed $35 million pursuant to an effective registration statement under the Securities Act. Effective upon the closing of a qualified IPO, the outstanding principal and accrued interest plus a 25% premium of such principal and interest will automatically convert into shares of the same class and series of our shares issued to other investors in the qualified IPO. These notes accrue interest at 7% per annum and accrued interest compounds annually, and upon such compounding, is added to the outstanding principal amount. Unless earlier converted into shares, these notes become due and payable on the later of (i) October 3, 2020 and (ii) five business days after the date on which the term loan facility with Hercules is repaid, terminated and discharged in full.
We refer to the January 2018 Shareholder Note, the 2018 New Investor Notes, and the notes issued under the October 2018 note purchase agreement collectively as the 2018 Notes.
Cash Flows
The following table provides information regarding our cash flows for each of the periods presented:
| YEAR ENDED DECEMBER 31, | NINE MONTHS ENDED SEPTEMBER 30, | |||||||||||||||
| 2016 | 2017 | 2017 | 2018 | |||||||||||||
(in thousands) | ||||||||||||||||
Net cash (used in) provided by: | ||||||||||||||||
Operating activities | $ | (54,020 | ) | $ | (69,836 | ) | $ | (51,366 | ) | $ | (50,915 | ) | ||||
Investing activities | (183 | ) | (173 | ) | (140 | ) | (12 | ) | ||||||||
Financing activities | 50,292 | 64,418 | 64,418 | 50,886 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Net increase (decrease) in cash and cash equivalents | $ | (3,911 | ) | $ | (5,591 | ) | $ | 12,912 | $ | (41 | ) | |||||
|
|
|
|
|
|
|
| |||||||||
Net Cash Used in Operating Activities
The use of cash for operating activities in all periods resulted primarily from our net losses adjusted fornon-cash charges and changes in components of working capital.
Net cash used in operating activities decreased by $0.5 million to $50.9 million during the nine months ended September 30, 2018 from $51.4 million during the nine months ended September 30, 2017. Cash used in operating activities during the nine months ended September 30, 2018 consisted of our net loss of $70.1 million, partially offset by non-cash charges including $4.8 million in non-cash interest expense and $1.0 million in share-based compensation, and changes in operating assets and liabilities including $1.4 million in increases in accounts payable, accrued expenses and other current liabilities and a $0.9 million decrease in prepaid expenses and other current assets. Cash used in operating activities during the nine months ended September 30, 2017 consisted of our net loss of $60.8 million, partially offset by non-cash charges including $1.3 million in non-cash interest expense and $1.0 million in share-based compensation, as well as changes in operating assets and liabilities including $7.1 million in increases in accounts payable, accrued expenses and other current liabilities.
Net cash used in operating activities was $69.8 million during the year ended December 31, 2017, compared to $54.0 million during the year ended December 31, 2016. Cash used in operating activities during the year ended December 31, 2017 consisted of our net loss of $82.9 million, partially offset by non-cash charges including $2.5 million in non-cash interest expense and $1.3 million in share-based compensation, and changes in operating assets and liabilities including $8.2 million in increases in accounts payable, accrued expenses and other current liabilities. Cash used in operating activities during the year ended December 31, 2016 consisted of our net loss of $61.0 million, partially offset by non-cash charges of $1.8 million in share-based compensation and $0.3 million in depreciation and amortization, and changes in operating assets and liabilities including $3.3 million in increases in
81
Table of Contents
accounts payable, accrued expenses and other current liabilities and $1.5 million in decreases in prepaid expenses and other current assets.
Net Cash Used in Investing Activities
Net cash used in investing activities was $0.1 million during the nine months ended September 30, 2017. Net cash used in investing activities was $0.2 million during the years ended December 31, 2016 and 2017.
Net Cash Provided by Financing Activities
Net cash provided by financing activities was $64.4 million during the nine months ended September 30, 2017, compared to $50.9 million during the nine months ended September 30, 2018. Cash provided by financing activities in the nine months ended September 30, 2017 was attributable to net proceeds of $50.0 million in connection with the issuance of convertible promissory notes to a shareholder, as well as $14.4 million related to net proceeds from the term loan facility. Cash provided by financing activities in the nine months ended September 30, 2018 was attributable to net proceeds of $50.0 million in connection with the issuance of convertible promissory notes to new investors and $5.0 million in net proceeds from the term loan facility offset by deferred public offering costs of $4.1 million.
Net cash provided by financing activities was $64.4 million during the year ended December 31, 2017, compared to $50.3 million during the year ended December 31, 2016. Cash provided by financing activities in the year ended December 31, 2017 was attributable to net proceeds of $50.0 million in connection with the issuance of convertible promissory notes to a shareholder, as well as $14.4 million related to net proceeds from the term loan facility. Cash provided by financing activities in the year ended December 31, 2016 was attributable to net proceeds of $50.7 million related to a demand note receivable offset by deferred public offering costs of $0.4 million.
Funding Requirements
We expect our expenses to increase in connection with our ongoing clinical activities, particularly as we continue to develop and conduct clinical trials with respect to elamipretide and new compounds, including our ongoing and planned clinical trials; advance the development of pipeline programs; initiate new research and preclinical development efforts; and seek marketing approval for any product candidates that we successfully develop. In addition, if we obtain marketing approval for any of our product candidates, we expect to incur significant commercialization expenses related to establishing sales, marketing, distribution and other commercial infrastructure to commercialize such products. Furthermore, upon the closing of this offering, we expect to incur additional costs associated with operating as a public company. Accordingly, we will need to obtain substantial additional funding in connection with our continuing operations. If we are unable to raise capital when needed or on attractive terms, we would be forced to delay, reduce or eliminate our research and development programs or future commercialization efforts.
We believe that the net proceeds from this offering, together with our existing cash and cash equivalents, will enable us to fund our operating expenses and capital expenditure requirements for the next 12 months.
We have based our projections of operating capital requirements on assumptions that may prove to be incorrect, and we may use all of our available capital resources sooner than we expect. Because of the numerous risks and uncertainties associated with the research, development and commercialization of our product candidates, we are unable to estimate the exact amount of our operating capital requirements. Our future capital requirements will depend on many factors, including:
| ∎ | scope, progress, timing, costs and results of our current and future clinical trials; |
| ∎ | research and preclinical development efforts for any future product candidates that we may develop; |
| ∎ | our ability to enter into and the terms and timing of any collaborations, licensing agreements or other arrangements; |
| ∎ | number of future product candidates that we pursue and their development requirements; |
| ∎ | outcome, timing and costs of seeking regulatory approvals; |
| ∎ | costs of commercialization activities for any of our product candidates that receive marketing approval to the extent such costs are not the responsibility of any future collaborators, including the costs and timing of establishing product sales, marketing, distribution and manufacturing capabilities; |
82
Table of Contents
| ∎ | subject to receipt of marketing approval, revenue, if any, received from commercial sales of our current and future product candidates; |
| ∎ | our headcount growth and associated costs as we expand our research and development and establish a commercial infrastructure; |
| ∎ | costs of preparing, filing and prosecuting patent applications, maintaining and protecting our intellectual property rights and defending against intellectual property related claims; and |
| ∎ | costs of operating as a public company. |
Identifying potential product candidates and conducting preclinical studies and clinical trials is a time-consuming, expensive and uncertain process that takes many years to complete, and we may never generate the necessary data or results required to obtain marketing approval and achieve product sales. In addition, our product candidates, if approved, may not achieve commercial success. Accordingly, we will need to continue to rely on additional financing to achieve our business objectives. Adequate additional financing may not be available to us on acceptable terms, or at all.
Until such time, if ever, that we can generate substantial revenues, we expect to finance our cash needs through a combination of equity offerings, debt financings, collaborations, strategic alliances and licensing arrangements. To the extent that we raise additional capital through the sale of equity or convertible debt securities, your ownership interest will be diluted, and the terms of these securities may include liquidation or other preferences that adversely affect your rights as a holder of ADSs. Debt financing, if available, may involve agreements that include covenants limiting or restricting our ability to take specific actions, such as incurring additional debt, making capital expenditures or declaring dividends.
If we raise funds through future collaborations, strategic alliances or licensing arrangements with third parties, we may have to relinquish valuable rights to our technologies, future revenue streams, research programs or product candidates or to grant licenses on terms that may not be favorable to us. If we are unable to raise additional funds through equity or debt financings when needed, we may be required to delay, limit, reduce or terminate our product development or future commercialization efforts or grant rights to develop and market product candidates that we would otherwise prefer to develop and market ourselves.
Critical Accounting Policies and Significant Judgments and Estimates
Our management’s discussion and analysis of our financial condition and results of operations is based on our consolidated financial statements, which we have prepared in accordance with U.S. generally accepted accounting principles. We believe that several accounting policies are important to understanding our historical and future financial performance. We refer to these policies as critical because these specific areas generally require us to make judgments and estimates about matters that are uncertain at the time we make the estimate, and we could have used different estimates which also would have been reasonable. On an ongoing basis, we evaluate our estimates and judgments, including those described in greater detail below. We base our estimates on historical experience and other market-specific or other relevant assumptions that we believe to be reasonable under the circumstances, the results of which form the basis for making judgments about the carrying value of assets and liabilities that are not readily apparent from other sources. Actual results may differ from these estimates under different assumptions or conditions.
While our significant accounting policies are described in more detail in the notes to our consolidated financial statements appearing elsewhere in this prospectus, we believe the following accounting policies to be most critical to the judgments and estimates used in the preparation of our consolidated financial statements.
Accrued Research and Development Expenses
As part of the process of preparing our consolidated financial statements, we are required to estimate our accrued expenses. This process involves reviewing open contracts and purchase orders, communicating with our personnel to identify services that have been performed for us and estimating the level of service performed and the associated cost incurred for the service when we have not yet been invoiced or otherwise notified of the actual cost. The majority of our service providers invoice us monthly in arrears for services performed or when contractual milestones are met. We make estimates of our accrued expenses as of each balance sheet date in our consolidated financial statements based on facts and circumstances known to us at that time. We periodically confirm the accuracy of our
83
Table of Contents
estimates with the service providers and make adjustments, if necessary. Examples of estimated accrued research and development expenses include fees paid to:
| ∎ | CROs in connection with clinical trials; |
| ∎ | CMOs with respect to clinical materials, intermediates, drug substance and drug product; |
| ∎ | vendors in connection with research and preclinical development activities; and |
| ∎ | vendors related to manufacturing, development and distribution of clinical supplies. |
We base our expenses related to clinical trials on our estimates of the services received and efforts expended pursuant to contracts with CROs that conduct and manage clinical trials on our behalf. The financial terms of these agreements are subject to negotiation, vary from contract to contract and may result in uneven payment flows. There may be instances in which payments made to our vendors will exceed the level of services provided and result in a prepayment of the clinical expense. Payments under some of these contracts depend on factors such as the successful enrollment of subjects and the completion of clinical trial milestones. In accruing service fees, we estimate the time period over which services will be performed, enrollment of subjects and the level of effort to be expended in each period. If the actual timing of the performance of services or the level of effort varies from our estimate, we adjust the accrual or prepaid expense accordingly. To date, there have been no material differences from our estimates to the amounts actually incurred.
Share-based Compensation
We account for share-based compensation awards in the consolidated statements of operations based on their grant-date fair value. We recognize compensation costs related to employees based on the estimated fair value of the awards on the date of grant and over the associated service periods, using the straight-line method. The options vest in accordance with the terms of the applicable agreements and expire no later than ten years after the date of grant. Compensation expense is recognized for the fair value of the consideration received, or the equity instruments issued, whichever is more reliably measurable. We measure share-based awards granted tonon-employees based on the fair value of the award on the date on which the related service is complete. Compensation expense is recognized over the period during which services are rendered by suchnon-employees until completed. At the end of each financial reporting period prior to completion of the service, the fair value of these awards is remeasured using the then-current fair value of our ordinary shares and updated assumption inputs in the Black-Scholes option-pricing model, or Black-Scholes.
We estimate the fair value of our share-based awards to employees andnon-employees using Black-Scholes, which requires the input of assumptions, some of which are highly subjective, including:
| ∎ | expected volatility of our ordinary shares; |
| ∎ | expected term of the award; |
| ∎ | risk-free interest rate; |
| ∎ | expected dividends; and |
| ∎ | estimated fair value of our ordinary shares on the measurement date. |
Due to the lack of a public market for the trading of our ordinary shares and a lack of company-specific historical and implied volatility data, we have based our estimate of expected volatility on the historical volatility of a group of comparable companies that are publicly traded. For these analyses, we selected representative companies from the life sciences industry with characteristics similar to ours, including enterprise value, risk profiles, position within the industry and historical share price information, sufficient to meet the expected life of the share-based awards. We compute the historical volatility data using the daily closing prices for the selected companies’ shares during the equivalent period of the calculated expected term of our share-based awards. We will continue to apply this process until a sufficient amount of historical information regarding the volatility of our own share price becomes available. We use a dividend yield of 0% based on the fact that we have never declared cash dividends and have no current intention of paying cash dividends over the expected term of the option.
The expected term of options granted represents the weighted average of previously transacted awards plus the minimum and maximum expected life of the outstanding awards based on vest and expiry. Fornon-employee
84
Table of Contents
options, we have determined the expected life based on the respective contractual life. The risk-free interest rates for periods within the expected life of the option are based on the U.S. Treasury yield curve in effect during the period the options were granted and with maturity dates equivalent to the expected term of the options.
The fair value of each share option granted to employees and directors was estimated on the date of grant using Black-Scholes, with the following assumptions:
| ||||||||||||
| YEAR ENDED DECEMBER 31, | NINE MONTHS ENDED SEPTEMBER 30, 2017 | |||||||||||
| 2016 | 2017 | |||||||||||
Risk free interest rate | 1.23%-2.42 | % | 1.89%-2.83 | % | 2.65%-3.02 | % | ||||||
Expected dividend yield | — | — | — | |||||||||
Expected term (in years) | 6.4 | 6.0 | 6.1 | |||||||||
Expected volatility | 50 | % | 57 | % | 59 | % | ||||||
Underlying fair value of ordinary shares | $1.14 | $1.38 | 1.53 | |||||||||
| ||||||||||||
We are also required to estimate forfeitures at the time of grant and revise those estimates in subsequent periods if actual forfeitures differ from the estimates. The estimation of the number of awards that will ultimately vest requires judgment and, to the extent actual results or updated estimates differ from our current estimates, such amounts will be recorded as a cumulative adjustment in the period in which estimates are revised.
The following table presents information regarding share options granted from October 1, 2017 through the date of this prospectus, along with the corresponding exercise price for each option grant and our current estimate of the fair value per share of our ordinary shares on each grant date, which we utilized to calculate share-based compensation expense:
DATE OF GRANT | NUMBER OF SHARES UNDERLYING OPTIONS GRANTED | EXERCISE PRICE PER SHARE | FAIR VALUE OF ORDINARY SHARES ON GRANT DATE | PER SHARE ESTIMATED FAIR VALUE OF AWARD ON GRANT DATE (1) | ||||||||||||
October 22, 2017 | 255,000 | $ | 1.38 | $ | 1.38 | $ | 0.75 | |||||||||
February 28, 2018 | 1,138,750 | $ | 1.20 | $ | 1.20 | $ | 0.69 | |||||||||
June 10, 2018 | 210,833 | $ | 2.22 | (2) | $ | 2.22 | $ | 1.29 | (3) | |||||||
June 27, 2018 | 175,000 | $ | 2.22 | (2) | $ | 2.22 | $ | 1.29 | (3) | |||||||
October 19, 2018 | 251,667 | $ | 1.53 | $ | 1.53 | $ | 0.87 | |||||||||
December 13, 2018 | 83,333 | $ | 1.53 | $ | 1.53 | $ | 0.87 | |||||||||
| (1) | Reflects the fair value of options as estimated at the date of grant using Black-Scholes. |
| (2) | In October 2018, the exercise price per share of these options was reduced from $2.22 to $1.53 per share. |
| (3) | As a result of the repricing of these options in October 2018, the per share estimated fair value of these awards will be adjusted as of the date of the repricing using Black-Scholes. |
Share-based compensation totaled $1.8 million and $1.3 million for the years ended December 31, 2016 and 2017, respectively, and $1.0 million and $1.0 million for the nine months ended September 30, 2017 and 2018, respectively. As of December 31, 2017 and September 30, 2018, unrecognized compensation expense related tonon-vested options, net of related forfeiture estimates, was $1.8 million and $2.0 million, respectively. We expect to recognize our remaining share-based compensation expense as of December 31, 2017 over a weighted-average remaining vesting period of approximately 2.6 years. We expect our share-based compensation expense to increase in future periods due to the potential increase in the value of our ordinary shares and future option grants to new and current employees, directors and consultants.
85
Table of Contents
Determination of the Fair Value of Ordinary Shares on Grant Dates
Following the consummation of this offering, the fair value of our ordinary shares will be determined based on the quoted market price of our ADSs. We have historically granted share options at exercise prices not less than the fair value of our ordinary shares. Our board of directors has determined the fair value of our ordinary shares considering, in part, the work of an independent valuation specialist. Our board of directors determined the estimated per share fair value of our ordinary shares at various dates considering contemporaneous valuations performed in accordance with the guidance outlined in the American Institute of Certified Public Accountants Practice Aid,Valuation of Privately-held Company Equity Securities Issued as Compensation, or the Practice Aid.
Our ordinary share valuations were prepared using the Hybrid Method. The Hybrid Method is a hybrid between the Probability Weighted Expected Returns Method and the option-pricing method, or OPM. It is used to estimate the probability weighted value across multiple scenarios, but uses OPM to estimate the allocation of value within one or more of those scenarios. The market approach was selected to determine our enterprise value under various initial public offering, or IPO, and merger and acquisition, or M&A, scenarios, and OPM was utilized to allocate the value between the share classes under an M&A scenario, resulting in a value for the ordinary shares.
The ordinary share value is based on the probability-weighted present value of expected future investment returns considering each of the possible outcomes available, as well as the rights of each class of security. The estimated future value under each outcome is discounted back to the valuation date at an appropriate risk- adjusted discount rate and probability weighted to arrive at an indication of value for an ordinary share. OPM treats common and preferred shares as call options on the total equity value of a company, with exercise prices based on the value thresholds at which the allocation among the various holders of a company’s securities changes. Under this method, an ordinary share has value only if the funds available for distribution to equity holders exceeds the value of the preferred security liquidation preference at the time of the liquidity event, such as a strategic sale or a merger.
Each valuation of our ordinary shares depends upon judgments and estimates. The underlying ordinary share value could vary based on changes in these judgments and estimates. Accordingly, investors are cautioned not to place reliance on the foregoing valuation methodologies as an indicator of future share prices. We performed ordinary share valuation, with the assistance of an independent valuation specialist as of: December 15, 2016, resulting in a valuation of $1.38 per share; December 31, 2017, resulting in a valuation of $1.20 per share; May 31, 2018, resulting in a valuation of $2.22 per share; and September 30, 2018, resulting in a valuation of $1.53 per share. In conducting the valuations, the independent valuation specialist considered objective and subjective factors that it believed to be relevant for each valuation conducted in accordance with the Practice Aid, including our best estimate of our business condition, prospects and operating performance at each valuation date. Other significant factors included:
| ∎ | the prices of our convertible preferred shares sold to investors and the rights, preferences and privileges of our preferred shares, including the liquidation preferences of our convertible preferred shares, as compared to those of our ordinary shares; |
| ∎ | our stage of development and business strategy and the material risks related to our business and industry; |
| ∎ | valuations of publicly traded companies in the life sciences and biotechnology sectors, as well as recently completed M&A of guideline companies; |
| ∎ | our results of operations and financial position; |
| ∎ | the composition of and changes to our management team and board of directors; |
| ∎ | the lack of liquidity of our ordinary shares; |
| ∎ | any external market conditions affecting the life sciences and biotechnology industry sectors; |
| ∎ | the likelihood of achieving a liquidity event for the holders of our ordinary shares and share options, such as an IPO or M&A, given prevailing market conditions; and |
| ∎ | the state of the IPO market for similarly situated privately held life sciences companies. |
The dates of our contemporaneous valuations have not always coincided with the dates of our share option grants. In determining the exercise prices of the share options set forth in the table above, our board of directors considered, among other things, the most recent valuation of our ordinary shares and their assessment of additional objective and
86
Table of Contents
subjective factors that were relevant as of the grant dates. The estimates of fair value of our ordinary shares are highly complex and subjective. There are significant judgments and estimates inherent in the determination of the fair value of our ordinary shares. These judgments and estimates include assumptions regarding our future operating performance, the time to complete an IPO or other liquidity event, the related valuations associated with these events, and the determinations of the appropriate valuation methods at each valuation date. The assumptions underlying these valuations represent management’s best estimates, which involve inherent uncertainties and the application of management judgment. If we had made different assumptions, our share-based compensation expense, net loss and net loss per share applicable to holders of ordinary shares could have been materially different.
Contractual Obligations
The following table summarizes our outstanding contractual obligations as of payment due date by period at December 31, 2017:
| TOTAL | LESS THAN 1 YEAR | 1 TO 3 YEARS | 3 TO 5 YEARS | MORE THAN 5 YEARS | ||||||||||||||||
| (in thousands) | ||||||||||||||||||||
Convertible promissory notes(1) | $ | 50,000 | $ | — | $ | 50,000 | $ | — | $ | — | ||||||||||
Operating leases | 1,813 | 608 | 1,205 | — | — | |||||||||||||||
Term loan facility(2) | 15,000 | 2,242 | 12,160 | 598 | — | |||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Total | $ | 66,813 | $ | 2,850 | $ | 63,365 | $ | 598 | $ | — | ||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||
| (1) | Represents principal amount of convertible notes outstanding as of December 31, 2017. In January 2018, such notes were exchanged for a convertible promissory note in the aggregate amount of $52.4 million. Also in January 2018, we entered into a note purchase agreement pursuant to which we issued convertible promissory notes in an aggregate principal amount of $50.0 million, and in October 2018, we entered into a note purchase agreement pursuant to which we issued convertible promissory notes in an aggregate principal amount of $30.0 million. |
| (2) | In March 2018, we drew an additional $5.0 million under the term loan facility. |
We enter into contracts in the normal course of business with CROs and clinical sites for the conduct of clinical trials, professional consultants and other vendors for clinical supply, manufacturing or other services. These contracts are not included in the table above as they provide for termination on notice and, therefore, are cancelable contracts and do not include any minimum purchase commitments.
We have entered into several license agreements with Cornell and the IRCM, pursuant to which Cornell and IRCM granted us an exclusive, worldwide rights under patents related to elamipretide,SBT-20 and other technology. In connection with the licenses granted under the original Cornell agreement, we issued Cornell 666,667 ordinary shares. With respect to the other Cornell license agreements, we are obligated to pay Cornell upfront license fees of $55,000 and royalties on net sales, if any, by us and our sublicensees of any licensed product. Subject to specified reductions and royalty offsets, such royalties are calculated as a tiered,low-to-mid single digit percentage of net sales of licensed products under each of the Cornell license agreements, except that for licensed products under the original Cornell agreement, such royalties are calculated as a tiered, low single-digit tosub-teen double-digit percentage of net sales, depending on patent coverage, amount of net sales and type of licensed product. Our obligation to pay royalties as to any licensed product extends until the later of the expiration of thelast-to-expire valid claim of any licensed patent covering such licensed product or 15 years after the date of our first commercial sale of such licensed product. If a licensed product is covered by licenses granted under the original Cornell agreement and another Cornell license agreement, then, for each unit of product, royalties will only be due under the original Cornell agreement.
We are obligated to pay Cornell a low double-digit percentage of specified payments we receive in connection with granting a sublicense under the Cornell license agreements. We have also agreed to reimburse Cornell for itsout-of-pocket expenses incurred in preparing, filing, prosecuting and maintaining the licensed patents, except for any licensed patents as to which we elect to waive our licensed rights. We also have agreed to pay Cornell annual license maintenance fees in dollars in themid-five-digits for the original Cornell agreement, and mid-four-digits for each of the other Cornell license agreements starting on the date specified in each such agreement, in all cases until the first commercial sale of a specified type of licensed product under such agreement.
87
Table of Contents
Off-balance Sheet Arrangements
We did not have during the periods presented, and we do not currently have, anyoff-balance sheet arrangements, as defined under the applicable regulations of the SEC.
Recent Accounting Pronouncements
Note 2, “Summary of Significant Accounting Policies,” in the accompanying notes to the consolidated financial statements includes a discussion of recent accounting pronouncements. There were no new accounting pronouncements adopted during 2017 that had a material effect on our consolidated financial statements.
Emerging Growth Company Status
The Jumpstart Our Business Startups Act of 2012 permits an “emerging growth company” such as us to take advantage of an extended transition period to comply with new or revised accounting standards applicable to public companies until those standards would otherwise apply to private companies. We have elected to avail ourselves of this exemption from new or revised accounting standards and, therefore, we will not be subject to the same new or revised accounting standards as other public companies. As a result, our financial statements may not be comparable to the financial statements of reporting companies that are required to comply with the effective dates for new or revised accounting standards that are otherwise applicable to public companies.
Qualitative and Quantitative Disclosures about Market Risk
We are minimally exposed to market risk related to changes in interest rates. As of September 30, 2018, we had cash and cash equivalents of $4.1 million, consisting primarily of money market funds. Our primary exposure to market risk is interest rate sensitivity, which is affected by changes in the general level of U.S. interest rates, particularly because our cash equivalents are held in short-term money market funds. We do not believe we are materially at risk to sudden drops in interest rates based on the amounts subject to these potential changes.
88
Table of Contents
Overview
We are a clinical-stage biotechnology company focused on the discovery, development and commercialization of novel therapies for diseases involving mitochondrial dysfunction. Mitochondria, found in nearly every cell in the body, are the body’s main source of energy production and are critical for normal organ function. Dysfunctional mitochondria characterize a number of rare genetic diseases, collectively known as primary mitochondrial diseases, and are also involved in many commonage-related diseases. We believe our lead product candidate, elamipretide, has the potential to treat both rare genetic and commonage-related mitochondrial diseases. We are studying elamipretide in the following primary mitochondrial diseases: primary mitochondrial myopathy, Barth and LHON. We are also studying elamipretide in dry AMD. Our other pipeline candidates includeSBT-20, which we are evaluating for rare peripheral neuropathies, andSBT-272, which we are evaluating for rare neurodegenerative disease indications. We have optimized our discovery platform to identify novel mitochondrial targeted compounds, which may be nominated as therapeutic product candidates or utilized as scaffolds to deliver other compounds to mitochondria. Our mission is to be the leader in mitochondrial medicine, and we have assembled a highly experienced management team, board of directors and group of scientific advisors to help us achieve this mission.
Elamipretide is a small peptide that targets and binds reversibly to cardiolipin, an essential structural element of mitochondria, stabilizing it under conditions of oxidative stress. This novel mechanism of action has shown potential clinical benefit in both rare genetic and commonage-related mitochondrial diseases. We are studying elamipretide in the following indications:
| ∎ | primary mitochondrial myopathy, for which we are conducting a Phase 3 pivotal clinical trial in North America and in Europe; |
| ∎ | Barth, for which we have conducted a Phase 2/3 clinical trial in the United States; |
| ∎ | LHON, for which we have conducted a Phase 2 clinical trial in the United States and plan to apply for approval to open clinical sites in China in conjunction with a potential Phase 3 clinical trial; and |
| ∎ | dry AMD, for which we have conducted a Phase 1 clinical trial in the United States and plan to initiate a Phase 2b clinical trial in the United States for geographic atrophy, an advanced form of dry AMD, in the first quarter of 2019. |
Elamipretide has been generally well-tolerated in over 900 subjects exposed to it systemically and 53 subjects exposed to it topically as of December 31, 2018.
In addition to our clinical development programs for elamipretide, we plan to evaluateSBT-20, our second clinical-stage product candidate, for which we have completed two Phase 1 clinical safety trials in healthy volunteers, for rare peripheral neuropathies. We are developingSBT-272, a preclinical-stage product candidate, for rare neurodegenerative diseases. In addition, ourin-house discovery platform has generated a library of over 100 proprietary, differentiated compounds that could have clinical benefit for diseases related to mitochondrial dysfunction and from which we plan to designate potential product candidates. We may also utilize certain of these compounds as part of our carrier platform, in which they could potentially serve as scaffolds to deliver other beneficial compounds to the mitochondria.
As of December 31, 2018, we held exclusive world-wide rights or an option for exclusive world-wide rights under 374 issued patents and 298 patent applications to protect our platform and product candidates. Since licensing elamipretide andSBT-20, we and our collaborators have published approximately 100 peer-reviewed articles highlighting the activity of our compounds in several disease models, including heart failure, kidney disease, skeletal muscle weakness, diabetic retinopathy and neurodegenerative diseases. Our compounds have been evaluated inpre-clinical and clinical studies at academic and clinical institutions, including Charité Berlin, Children’s Hospital of Philadelphia, Columbia University, Cornell University, Duke University, Massachusetts General Hospital, Mayo Clinic, Stanford University, University of California Los Angeles, University of California San Diego and University of Washington.
89
Table of Contents
Our Pipeline
The following table summarizes our development pipeline, including preclinical studies and ongoing and planned clinical trials of our product candidates we have advanced, or expect to advance in the next year, to clinical development.
We previously completed a Phase 1/2 clinical trial for the evaluation of SBT-20 in subjects with early-stage Huntington’s disease and a Phase 1 healthy volunteer study. We are currently evaluating preclinical disease models for the selection of an indication ahead of planning for a Phase 2 clinical trial.
Our Strategy
We aim to continue the development of mitochondrial medicine to improve the lives of patients with unmet medical needs. There are no treatments approved by the FDA, the EMA or the NMPA for primary mitochondrial myopathy, Barth or dry AMD, and there are no FDA or the NMPA approved treatments for LHON. We are pioneering the development of treatments for these diseases with unmet medical needs and believe we are well-positioned to be among the first to address these largely untapped markets in the United States, Europe and China. Although our initial development focus is on rare primary mitochondrial diseases, we believe that over the longer term there could be significant opportunities with regard to commonage-related diseases, including dry AMD. Our strategies include:
Rapidly advance the clinical development of elamipretide in rare mitochondrial diseases
We are developing elamipretide for rare mitochondrial diseases, including primary mitochondrial myopathy, Barth and LHON. We have received Fast Track and Orphan Drug designations in the United States for each of these indications. We are enrolling subjects into our ongoing Phase 3 clinical trial for the treatment of primary mitochondrial myopathy, which we expect to have fully enrolled during the first half of 2019. We have completed the placebo-controlled portion of a Phase 2/3 clinical trial for the treatment of Barth, which did not meet its primary efficacy endpoints, and are continuing to evaluate efficacy endpoints during an open-label extension, in which all subjects are eligible to continue receiving elamipretide. Eight subjects are continuing in the open-label extension phase. We plan to meet with the FDA regarding this program during the first half of 2019 to discuss a potential NDA submission.We have completed the placebo-controlled portion of a Phase 2 clinical trial for the treatment of LHON, which did not meet its primary efficacy endpoints, and are continuing to evaluate efficacy endpoints during an open-label extension trial, in which all subjects are eligible to continue receiving the study drug. We plan to meet with the FDA for an end-of-Phase 2 meeting regarding this program during the first half of
90
Table of Contents
2019. Following that meeting, we plan to submit a clinical trial application to the NMPA for the inclusion of clinical sites in China in a potential Phase 3 clinical trial, which we believe may help expedite clinical trial enrollment. We will continue to evaluate development of elamipretide for additional rare disease indications.
Accelerate the clinical development of elamipretide for dry AMD
We are advancing development of elamipretide for dry AMD, anage-related disease, which is the leading cause of blindness in older adults. Dry AMD is estimated to impact approximately 10 million individuals in the United States and is the leading cause of blindness among older adults in the developed world. We received Fast Track designation in the United States for dry AMD with geographic atrophy in November 2018. Dry AMD would provide a significantly larger potential market size than our rare disease indications if we are able to successfully develop and commercialize elamipretide or one of our pipeline compounds for this indication. In our Phase 1 clinical trial of elamipretide, we observed evidence of clinical benefit for patients with dry AMD. We plan to initiate a Phase 2b placebo-controlled clinical trial for the treatment of patients with geographic atrophy, an advanced form of dry AMD, in the first quarter of 2019.
Expand clinical development efforts in China under new regulatory pathways
The prevalence of primary mitochondrial diseases, such as primary mitochondrial myopathy, Barth and LHON, is thought to be comparable in China to that in the United States because evidence suggests that prevalence does not vary by race or ethnicity for mitochondrial diseases. China has recently implemented policies to expedite regulatory pathways for rare diseases, including publication of a list of rare diseases that includes mitochondrial related diseases such as LHON. For primary mitochondrial myopathy, with respect to which we are currently conducting a pivotal trial in the United States and Europe, and Barth, we may apply to the NMPA for clinical trial waivers and expedited approval if and when we receive FDA approval for these indications. For LHON, we plan to submit a clinical trial application to the NMPA for the inclusion of Chinese clinical sites in our subsequent clinical trials, which may be used to support FDA approval. We believe that inclusion of Chinese sites may help expedite enrollment of clinical trials in rare diseases, as well as progress potential commercial collaboration opportunities for the China market for our product candidates, if approved.
Advance the development of pipeline mitochondrial medicines in rare diseases
We believe that our mitochondrial targeted product candidates may be beneficial in rare diseases involving mitochondrial dysfunction and hope to nominate compounds from our pipeline for select rare disease indications. We plan to evaluate our second clinical product candidate,SBT-20, for which we have completed two Phase 1 clinical safety trials in healthy volunteers, for rare peripheral neuropathies. We are evaluating our lead pipeline compound,SBT-272, for rare neurodegenerative diseases, such as amyotrophic lateral sclerosis, or ALS. We expect to initiate a Phase 1 clinical safety trial forSBT-272 by the end of 2019.
Advance the development of pipeline mitochondrial medicines in commonage-related diseases
We believe that mitochondrial medicine may be a promising approach for many commonage-related diseases beyond AMD, including neurodegenerative diseases. We believe that the United States, Europe and China are important markets for the clinical development ofage-related diseases, and we are evaluating further development of our product candidates and pipeline compounds forage-related indications in these markets.
Expand our carrier platform
We have extensive experience in optimizing delivery of our compounds to the mitochondria, which has been a challenge for other drug delivery technologies. We have demonstrated capability to deliver beneficial payloads to mitochondria by conjugating them with our proprietary compounds, which serve as vectors or carriers to the mitochondria, conferring organelle specificity to promising therapies. These payloads could include small molecules, proteins, oligonucleotides and complex formulations, such as DNA, siRNA and miRNA, nanoparticles and liposomes. This delivery platform, which we call our carrier platform, could enable delivery of missing proteins or even gene therapy to address inherited mitochondrial disorders.
Explore potential strategic partnerships and alliances to maximize the value of our development programs
We hold worldwide exclusive rights for our two clinical-stage assets, elamipretide andSBT-20, from the Cornell Research Foundation, Inc. and the Institut de recherches cliniques de Montréal. We have full ownership of our preclinical compound library, includingSBT-272. We may explore select strategic partnerships and alliances to support our drug development programs, while preserving significant development and commercialization rights, if
91
Table of Contents
we believe that such alliances may allow us to leverage the financial support and therapeutic area expertise and resources of a strategic partner to accelerate the development and commercialization of our drug candidates, particularly in common disease indications. We plan to retain rights to lead the development and commercialization of elamipretide for primary mitochondrial myopathy, Barth, LHON and dry AMD in the United States but will consider collaborating in Europe and China.
Expand our intellectual property portfolio in the field of mitochondrial medicine
We continue to invest in our mitochondrial medicine discovery platform to identify new approaches to improve absorption, distribution, metabolism and excretion of active mitochondrial compounds. We have an active discovery and development program focused on novel compounds targeting mitochondria. We believe the differentiated mitochondrial targeting characteristics of our compounds, our development of proprietary assays to screen new compounds for mitochondrial targeting and activity characteristics, and our experience working with various models of mitochondrial dysfunction position us to be a leader in next generation development of mitochondrial product candidates that are improved relative to elamipretide and SBT-20. We intend to use our insight into mitochondrial biology to continue developing additional intellectual property as we pursue additional novel therapeutic compounds that target mitochondrial disease. As of December 31, 2018, our intellectual property portfolio included 374 issued patents and 298 patent applications relating to mitochondrial medicine, either wholly-owned orin-licensed, in select commercially relevant jurisdictions, including the United States, key European countries, China, Japan and Canada.
Our Team
We have assembled a highly experienced leadership team with decades of experience leading drug discovery and development programs, including at GlaxoSmithKline, Novo Nordisk, Pfizer and Sanofi Genzyme. Our largest shareholder is a member of the Morningside group, a worldwide investment group.
Background
Mitochondria
Mitochondria, found in almost all human cells, are the “powerhouse of the cell.” Mitochondria produce 90% of our energy by converting food into adenosine triphosphate, or ATP, a molecule that carries energy within cells. Mitochondria produce approximately our body weight in ATP daily, providing the energy that allows cardiac muscles, for example, to beat an estimated 100,000 times every 24 hours, or 2.5 billion times by age 70, without stopping. Our skeletal muscle, heart, kidney, eyes and brains are among the highest producers and users of mitochondrial ATP in our bodies, as ATP is required for their critical functions such as the contraction of skeletal, cardiac, vasculature
92
Table of Contents
and lung muscle, maintenance of cell membrane potential, cellular transport and secretion of hormones and neurotransmitters. Normal mitochondrial function is essential for human life and for the proper functioning of many systems in our bodies, as illustrated below.
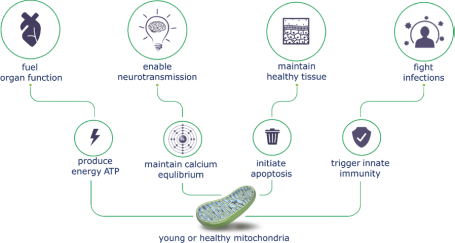
Mitochondria are highly specialized structures. They have their own DNA, called mitochondrial DNA, or mtDNA, which is inherited only from our mothers and is separate and distinct from nuclear DNA, or nDNA. Mitochondria are located within the cell, which is protected by the cell membrane, and they also have their own inner and outer membrane, which create further barriers to the effective delivery of therapeutics to these specialized organelles. In normal mitochondria, the inner mitochondrial membrane, or IMM, is highly folded, creating curves, called cristae. The cristae house the electron transport chain, or ETC, which is composed of five protein complexes responsible for mitochondrial ATP production through a process known as oxidative phosphorylation. The curved architecture of the cristae in the IMM is essential to keep the electron transport chain complexes in optimal close configuration for normal oxidative phosphorylation. Our product candidates target and bind to cardiolipin, an important structural component of the cristae and the IMM, stabilizing it from degradation due to dysfunction caused by inherited or acquired mutations in mtDNA or nDNA. An illustration of a healthy mitochondria and its curved cristae structure is shown below.
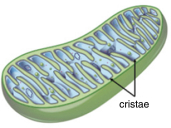
Mitochondrial Dysfunction, Aging and Human Disease
Mitochondrial dysfunction most often arises from mutations in mtDNA or nDNA, that can either be inherited or, in the case of mtDNA mutations, can occur as we age. Dysfunctional mitochondria not only produce less ATP, which impairs the normal functioning of our major organ systems, but they also generate unhealthy levels of reactive oxygen
93
Table of Contents
species, or ROS, which damages cardiolipin.ROS-mediated damage of cardiolipin can lead to pathological oxidative stress, causing the inflammation, fibrosis and cell death which are causal or contributory to the process of human aging, as illustrated below.
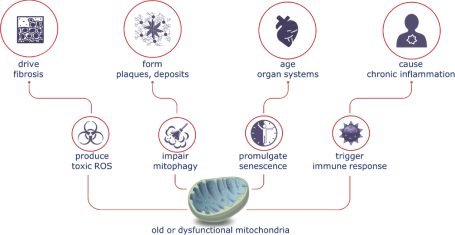
Mitochondrial diseases arising from inherited genetic defects, called primary mitochondrial diseases, are typically rare diseases which can impact multiple organ systems within the body and may lead to reduced lifespan. Symptoms of primary mitochondrial disease, including chronic pain, vision problems, cardiovascular problems and kidney problems, may be compared to “accelerated aging” as described by individuals with the disease and their caregivers.
Although mtDNA is originally inherited from our mothers, it is replicated within cells as mitochondria reproduce and is highly susceptible to mutation within specific cells and organ systems as we age. Mitochondrial diseases arising from these spontaneous mutations in our mtDNA, called secondary mitochondrial diseases, include senescence, neurodegenerative diseases (such as Alzheimer’s, Parkinson’s and amyotrophic lateral sclerosis), heart disease (such as heart failure and atherosclerosis), diabetes, ophthalmic conditions (such asage-related macular degeneration, glaucoma, diabetic retinopathy and diabetic macular edema), cancer, diabetes, skeletal muscle dysfunction (such as sarcopenia) and kidney diseases.
Mitochondrial dysfunction, whether inherited or acquired, often impacts high energy-demanding organs such as the skeletal muscle, cardiac, renal, visual, neurological, central nervous, circulatory or endocrine systems.
Targeting Mitochondrial Dysfunction: Role of Cardiolipin
Our product candidates target cardiolipin in the IMM, stabilizing it under conditions of oxidative stress.
Cardiolipin is a conically shaped phospholipid that plays an important role in establishing the cristae architecture within the IMM and optimizing the function of the ETC. Reduced and damaged cardiolipin content has been observed in many diseases, and a deficiency of normal cardiolipin is thought to be centrally involved in mitochondrial dysfunction.
Cardiolipin is essential for normal oxidative phosphorylation, the process by which ATP is made. Cardiolipin congregates in and around the cristae of the IMM. Cardiolipin’s conical shape is responsible for creating the curved architecture of the cristae. This curvature helps to keep the electron transport chain complexes in close association with one another, increasing the efficiency of ATP production and minimizing the electron leak that leads to oxidative stress, as illustrated below.
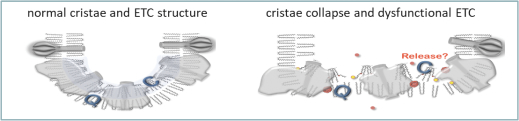
94
Table of Contents
Cardiolipin is embedded within the complexes of the ETC, as can be seen above, and its interaction with the ETC complexes facilitates super-complex association, a process by which electron transport chain complexes selectively associate with, or merge with, one another, to optimize the efficiency of the oxidative phosphorylation process.
Correct mitochondrial morphology is also essential for mitochondrial network connectivity and function. Mitochondrial networks exhibit coordination of inner mitochondrial membrane cristae at inter-mitochondrial junctions, as illustrated below.
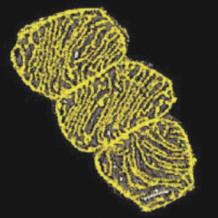
Mitochondrial network connectivity is associated with cellular signaling pathways, including:
| ∎ | fusion, in which mitochondria join to spread metabolites, enzymes, and mitochondrial gene products through the mitochondrial network, optimizing mitochondrial function and counteracting the accumulation of mitochondrial mutations during aging; |
| ∎ | fission, or the division of mitochondria, which plays an important role in the removal of damaged organelles; |
| ∎ | mitophagy, a mechanism to remove damaged mitochondria; |
| ∎ | ROS-mediated pathways, including the PI3K/Akt pathway, an intracellular signaling pathway important in regulating the cell cycle, and the tumor necrosis factor alpha (TNFa) signaling pathway, a proinflammatory pathway involved in various biological processes including regulation of cell proliferation, differentiation, apoptosis and immune response; |
| ∎ | calcium regulation, entailing the transfer of calcium from the endoplasmic reticulum to the mitochondrial to facilitate mitochondrial respiration; |
| ∎ | various transcription factors, which are proteins that control the rate of transcription of genetic information from DNA to messenger RNA; and |
| ∎ | certain protein kinase C (PKC) signaling pathways that can affect cardiomyocyte function and are involved in the induction of mitophagy. |
Cardiolipin is susceptible to peroxidation, or degradation, by oxidative stress produced by dysfunctional mitochondria. When cardiolipin is degraded, it can lose its conical shape, compromising the structural integrity of the IMM by leading to a relaxation of the cristae and a drifting apart of the electron transport chain complexes. Shuttling of electrons through the electron transport chain becomes less efficient with the complexes further apart from one another, resulting in lower ATP production and higher ROS generation. Disruption of mitochondrial morphology also impairs fission and fusion, impacting signaling pathways including mitophagy. This can trigger the
95
Table of Contents
cellular and extra- cellular cascades involving inflammation, fibrosis and cell death that underlie many diseases. The images below show healthy mitochondria, on the left, with normal cardiolipin content and cristae structure, and unhealthy mitochondria, on the right, with reduced cardiolipin content and collapsed cristae.
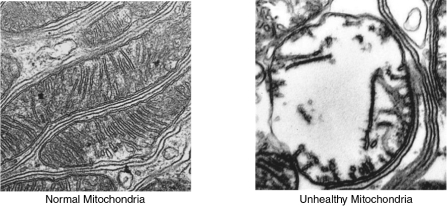
Various diseases alter cardiolipin composition and reduce cardiolipin content within the mitochondria. Biopsies from patients with primary mitochondrial disease arising from mitochondrial encephalitis, lactic acidosis and stroke-like episodes, or MELAS, and multiple mitochondrial DNA deletions were found to have approximately 15% less normal cardiolipin composition than normal. Experiments in Barth patient-derived lymphoblastoid cell lines showed 50%-60% less cardiolipin than control cell lines, and work done in Barth patient-derived cardiomyocytes showed up to 75% less cardiolipin than control cardiomyocytes. Aging has also been shown to decrease cardiolipin content in high energy-demanding organs, such as the heart, brain, liver and kidney, as well as the epidermis. Studies suggest that oxidative stress and peroxidation of cardiolipin may contribute to the overall loss of cardiolipin content in these diseases.
Our Approach to Mitochondrial Medicine
We have exclusive worldwide rights to elamipretide andSBT-20, both of which we licensed from Cornell and IRCM, in 2006. The unique mitochondrial activity of elamipretide was first published inThe Journal of Biological Chemistryin August 2004. Since licensing elamipretide andSBT-20, we and our collaborators have published approximately 100 peer-reviewed articles highlighting the activity of our compounds in several disease models, including heart failure, kidney disease, skeletal muscle weakness, diabetic retinopathy and neurodegenerative diseases. We have discovered and own over 100 compounds that also target the mitochondria and form the basis of our broad proprietary pipeline of mitochondrial targeted product candidates. We have focused our development efforts on diseases and conditions that affect the organs in the body that generate significant energy because of the high mitochondrial content found in the cells comprising these organs.
Our lead product candidate, elamipretide, along with several of our pipeline compounds, target and bind reversibly to cardiolipin, stabilizing it under conditions of oxidative stress, thereby preserving the curved architecture of the IMM, as illustrated below.
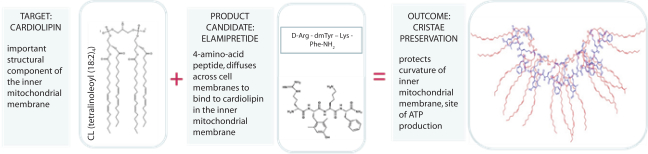
96
Table of Contents
In preclinical studies or clinical trials, we have observed that elamipretide normalized function in dysfunctional mitochondria, including as outlined in the table below. The below table referencesp-values, which is a conventional statistical method for measuring the statistical significance of clinical trial results. Ap-value of 0.05 or less represents statistical significance, meaning that there is a1-in-20 or less statistical probability that the observed results occurred by chance.
FUNCTIONAL FINDING | PRECLINICAL STUDY | |
| Reduced peroxidation of, or damage to, cardiolipin | In a study of dogs with induced heart failure published inCirculation: Heart Failure in February 2016, researchers at Henry Ford Health System observed that cardiolipin content was restored to near-normal levels in seven dogs treated with elamipretide versus seven dogs treated with placebo once daily subcutaneous injections for three months (p<0.05). | |
| Increased mitochondrial respiration, the process in which mitochondria produce energy | In a study of human heart tissue explanted from 21 heart transplant subjects with heart failure conducted by researchers at the University of Colorado and presented in 2017, researchers observed that elamipretide significantly improved mitochondrial respiration and increased it to levels comparable to those measured in healthy heart tissue levels, as compared to placebo (p<0.0005). | |
| Improved ATP levels | In a preclinical study at the University of Washington published inAging Cell in October 2013, two groups of between five and seven27-months old (equivalent to80-year-old human) and five-month old (equivalent to30-year-old human) mice were injected with a single dose of 3 mg/kg of elamipretide or placebo. In the older mice, researchers observed that a single dose of elamipretide significantly increased the maximum capacity of the mitochondria to produce ATP, called ATPmax, to near normal levels, as compared to placebo (p<0.01). | |
| Reduced formation of ROS, or oxidative stress | Researchers at the University of Florida conducted a study, published in theJournal of Applied Physiology in August 2011, of 72 mice, 24 of which received no treatment, 24 of which received placebo and hind limb immobilization to induce muscle atrophy (cast), and 24 of which received 1.5 mg/kg subcutaneous once daily elamipretide and hind limb immobilization (cast), in each case for 14 days. Researchers observed that elamipretide-treated immobilized mice had significantly lower levels of mitochondrial ROS production than the placebo-treated immobilized mice (p<0.05), as well as significantly reduced levels of H2O2, a precursor of ROS, in the soleus and plantaris calf muscles as compared to placebo (p<0.05). | |
| Reduced inflammation, fibrosis and cell death | In a preclinical study at the Mayo Clinic, published in theJournal of the American Heart Association in May 2016, two groups of seven pigs—each with unilateral renal artery stenosis—were injected with a 0.1 mg/kg dose of elamipretide for five consecutive days per week for four weeks or placebo, following percutaneous transluminal renal angioplasty, or PRTA. Four weeks later, researchers observed that elamipretide treated animals demonstrated significantly improved diastolic function, mitochondrial biogenesis improvement and oxidative stress and fibrosis reduction relative to placebo. In a separate preclinical study of pigs with unilateral renal artery stenosis published in theJournal of Hypertensionin January 2014, researchers at the Mayo Clinic observed improvements in cardiac function and oxygenation and reductions in apoptosis, oxidative stress, inflammation (p<0.05) and fibrosis (P<0.05), each as compared to placebo, four weeks following PTRA concurrent with a continuous 0.05 mg/kg intravenous infusion of elamipretide. | |
| No observed effect on normal mitochondria | An important safety aspect of elamipretide is that it has not had any observed effect on normal mitochondria. In the study of explanted human heart tissue | |
97
Table of Contents
FUNCTIONAL FINDING | PRECLINICAL STUDY | |
| described above, mitochondrial respiration in the normal donor heart tissue was unchanged following exposure to elamipretide. In the study of young and old mice described above, ATPmax levels in the young mice were unchanged following treatment with elamipretide. |
Following treatment with elamipretide andSBT-20, we observed normalization of mitochondrial morphology across various disease models, including models of diabetic retinopathy, as illustrated by the electron microscopic images below, and kidney reperfusion injury, each of which were published inClinical Pharmacology & Therapeutics in December 2014.
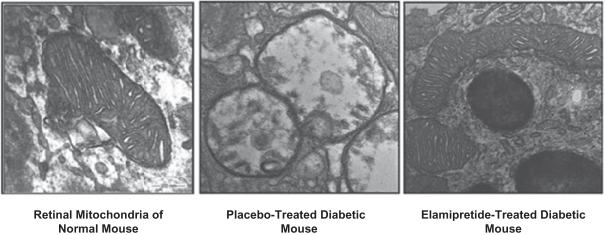
Our Product Candidates
We believe that our product candidates have significant potential to address the various diseases associated with mitochondrial dysfunction. In addition to our focus on rare diseases, including primary mitochondrial myopathy, Barth and LHON, we have conducted preclinical studies and Phase 1 clinical trials on common diseases and conditions that affect the organs in the body that have significant mitochondrial content to meet their high energy needs; these include the heart, the kidney, the brain (inclusive of the visual system), and active skeletal muscle. We believe that our product candidates may be most relevant for these organs, which are highly dependent on mitochondrial bioenergetics, and we expect these to be key focus areas with respect to some of our pipeline compounds.
We believe that there is significant potential for mitochondrial medicine beyond the indications we are currently studying, including with respect to common diseases associated with aging. In addition to our lead product candidate, we have a growing pipeline of over 100 compounds in preclinical testing that have been screened for mitochondrial activity, including in some cases preferential mitochondrial targeting characteristics and improved tissue distribution in targeted tissues, such as the heart and brain. Some of these compounds, includingSBT-272, may be suitable for oral formulations, and we believe they may be more appropriate for development for common diseases associated with aging. We have also designed proprietary compounds, which we refer to as carriers, that can potentially deliver beneficial payloads to mitochondria; for example, if genetic mutations impact the production of certain proteins necessary for proper mitochondrial function, this proprietary technology might help us deliver those missing proteins to mitochondria.
Elamipretide
Elamipretide is a small peptide that targets and binds reversibly to cardiolipin, stabilizing mitochondrial structure and function under conditions of oxidative stress. Elamipretide has been reported to be well-tolerated in over 900 people exposed to it systemically and 53 subjects exposed to it topically as of December 31, 2018. See “—Elamipretide Safety Data” below. We are evaluating elamipretide in primary mitochondrial diseases where there is a genetic basis for the underlying mitochondrial dysfunction and where we have the potential for expedited regulatory review, including primary mitochondrial myopathy, Barth and LHON, for which we have received Fast
98
Table of Contents
Track and Orphan Drug designations from the FDA. We also believe that elamipretide and our pipeline compounds may be able to address the significant unmet medical needs of larger populations affected by common diseases associated with aging. We are progressing our development of elamipretide for dry AMD with geographic atrophy, for which we have received Fast Track designation from the FDA, and we plan to evaluate clinical trials for other commonage-related disease indications in conjunction with our pipeline compounds.
Elamipretide Clinical Programs—Primary Mitochondrial Diseases
We are studying the effect of elamipretide in an ongoing Phase 3 pivotal trial for the treatment of primary mitochondrial myopathy. We plan to meet with the FDA to discuss the treatment of Barth, and to discuss data from our Phase 2 clinical trial for the treatment of LHON. Individuals with these primary mitochondrial diseases are born with a genetic mutation that causes mitochondrial dysfunction, leading to clinical signs and symptoms of disease. These diseases can result in reduced lifespan, as in Barth and, in some cases, mitochondrial myopathy, and can impair vital organ functions, such as vision, in the case of LHON, skeletal muscle function, in the case of primary mitochondrial myopathy and Barth, and cardiac function, in the case of Barth.
Primary mitochondrial myopathy (MMPOWER Trials)
We estimate that approximately 40,000 individuals in the United States have mitochondrial myopathy. There are no therapies approved by the FDA, EMA or NMPA for the treatment of primary mitochondrial myopathy. We have received Fast Track designation and Orphan Drug designation from the FDA for the development of elamipretide in this indication.
Primary mitochondrial myopathy is characterized by debilitating skeletal muscle weakness, exercise intolerance and fatigue accompanied by a confirmed molecular genetic diagnosis of primary mitochondrial disease. Individuals with this disease may experience muscle pain, muscle wasting, muscle cramps, rhabdomyolysis, or breakdown of muscle, progressive external ophthalmoplegia characterized by drooping of the eyelids, which often impairs vision, abnormal tilting of the head due to shortening of the neck muscles, difficulty swallowing, low muscle tone (also known as floppy infant syndrome), respiratory insufficiency and reduced deep tendon reflexes. These symptoms can result in significant deterioration of quality of life, such that routine activities of daily living (such as walking, climbing stairs, vacuuming, reaching, driving, reading or carrying out normal job functions) are limited by poor endurance and easy fatigue. Severely impacted individuals can lose their ability to walk entirely.
Morphology of mitochondria in individuals with primary mitochondrial myopathy is abnormal, and, unlike mitochondria in normal skeletal muscle cells, as shown below on the left, can be characterized by inclusion of abnormal rectangular-shaped, crystal-like structures, as shown below on the right.
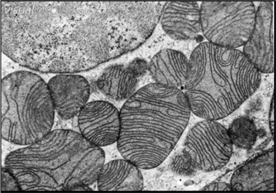 | 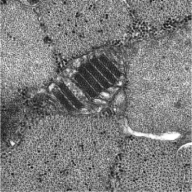 | |||
| Normal skeletal muscle mitochondria | Mitochondrial myopathy mitochondria |
We are assessing elamipretide in subjects with primary mitochondrial myopathy irrespective of their specific primary mitochondrial disease genotype. This strategy offers us the potential to treat all individuals with genetic mitochondrial disease who experience myopathic symptoms, estimated at greater than 90% of the primary mitochondrial disease population, which is a much larger target market than any specific genetic mutation or syndrome within it.
99
Table of Contents
We are currently enrolling subjects with primary mitochondrial myopathy inMMPOWER-3, a Phase 3 clinical trial, in which we have enrolled 86 out of a targeted 202 subjects in the United States, Canada and Europe as of September 30, 2018. We have established apre-trial registry forMMPOWER-3 at our Phase 3 sites, and have registered over 400 subjects who have beenpre-screened for eligibility forMMPOWER-3. We expect that this registry will expedite timely enrollment ofMMPOWER-3 since many eligible subjects are already identified.
We have completed two clinical trials in this indication, MMPOWER, completed in April 2016, andMMPOWER-2, completed in March 2017. In MMPOWER, we observed an improvement in the distance walked in six minutes (thesix-minute walk test, or 6MWT) in subjects treated with elamipretide—a primary efficacy endpoint of the study and a standard accepted test of functional exercise capacity. InMMPOWER-2, we observed an improvement in the 6MWT in subjects treated with elamipretide, a primary efficacy endpoint of the study, and in secondary efficacy endpoints, including several endpoints measuring fatigue, a hallmark symptom of primary mitochondrial myopathy. Twenty-four subjects remain enrolled in an ongoing open-label extension trial, in which they continue to receive once daily elamipretide and during which we continue to collect safety and select efficacy data, primarily to add to our safety database.
MMPOWER-3
MMPOWER-3 is a Phase 3, double-blind, placebo-controlled, parallel group trial enrolling an estimated 202 subjects ranging from 16 to 80 years old, with primary mitochondrial myopathy at up to 28 sites in North America and Europe, including the United States, Canada, Denmark, Hungary, Italy, Germany and the United Kingdom to evaluate the efficacy and safety of once daily subcutaneous injections of elamipretide. Subjects are randomized in aone-to-one ratio to either 40 mg once daily subcutaneous elamipretide or placebo injection for an initial treatment period of 24 weeks, following which subjects will be eligible to participate in an open-label extension trial.
The objectives of the trial are to evaluate the safety, tolerability and efficacy of once daily subcutaneous elamipretide injections in individuals with primary mitochondrial myopathy. Subjects will complete assessments including the 6MWT, at initial screening, at baseline (prior to receiving the first dose), at week four, at week 12 and at week 24, which is the end of treatment. In addition, the primary mitochondrial myopathy symptom assessment, or PMMSA, a patient reported outcome questionnaire developed based upon interviews of individuals with primary mitochondrial disease to measure the fatigue and muscle weakness that are hallmark symptoms of the disease, will be completed daily. Based on observations from ourMMPOWER-2 clinical trial andpost-hoc observations from our MMPOWER clinical trial, which suggest that subjects walking more than 100 meters (because lesser distances may be indicative ofco-morbidities in this population) and less than 450 meters (because an above 500 meter 6MWT distance is not indicative of impairment) at baseline on the 6MWT are more likely to improve in meters walked following elamipretide treatment, we have endeavored to enrich our Phase 3 population by excluding individuals who walk less than 100 meters or more than 450 meters at their screening or baseline visits.
The primary efficacy analysis will compare mean changes as between the elamipretide and placebo treatment groups in:
| (i) | distance walked on the 6MWT from baseline to the week 24 visit, and |
| (ii) | PMMSA Total Fatigue score, measuring tiredness at rest, tiredness during activities, muscle weakness at rest and muscle weakness during activities, from baseline to the week 24 visit. |
The 6MWT and PMMSA Total Fatigue score together comprise a family of primary endpoints. The trial design contemplates a statistical analysis under which we will meet our primary endpoint if both endpoints are met at the p<0.05 level of significance, or if one of the two is met at the p<0.025 level of significance. The PMMSA Total Fatigue score not only measures improvements in the fatigue and weakness, which are the hallmark clinical symptoms of the disease, but it was also highly sensitive to change (p=0.0006) in our prior 30-patient Phase 2 clinical trial,MMPOWER-2.
100
Table of Contents
Secondary endpoints include the following, listed in order of interest:
ASSESSMENT | DESCRIPTION | |
| Neuro-QoL Fatigue Short- Form(Neuro-QoL Fatigue) | A standard questionnaire developed by the National Institutes of Health to assess fatigue in neuromuscular indications, with respect to which a reduction in score indicates reduced fatigue. | |
| PMMSA Most Bothersome Symptom | The first-time subjects complete the PMMSA, they are asked to identify which of the 10 items on the questionnaire is the “most bothersome” symptom of their disease; this is then assessed at trial completion to ascertain any changes in this symptom of interest. A similar endpoint approach is endorsed in the FDA’sGuidance on Developing Drugs for Acute Treatment of Migraine (2014). By focusing on the most severe symptoms for each subject, there is inherent clinical relevance in the individualized symptom endpoint. | |
| Patient global impression scale of change | A single question allowing the patient to assess his or her general health. | |
| Clinical global impression scale of change | A single question allowing the physician or caregiver to assess the patient’s general health. | |
| PMMSA Total Fatigue During Activities | Comprised of two questions from the PMMSA, assessing tiredness during activities and muscle weakness during activities. | |
| Neuro-QoL Activities of Daily Living | Specific questions from theNeuro-QoL Fatigue long-form questionnaire, a19-question questionnaire developed by the National Institutes of Health, which assess the impact of fatigue on subjects’ activities of daily living. The FDA requested that we include activities of daily living questions inMMPOWER-3, and indicated that it would be appropriate for us to utilize the activities of daily living questions from theNeuro-QoL which were responsive to change inMMPOWER-2, including questions 4 (I was too tired to do my household chores), 6 (I was frustrated by being too tired to do the things I wanted to do), 8 (I had to limit my social activity because I was tired), 9 (I needed help doing my usual activities because of my fatigue), 12 (I had trouble finishing things because I was too tired), 13 (I was too tired to take a short walk), 18 (I had to limit my social activity because of weakness) and 19 (I had to force myself to get up and do things because I was physically too weak). | |
We have registered over 400 subjects with signs and symptoms of primary mitochondrial myopathy in a multi-nationalpre-trial registry, participation in which is a prerequisite to participation inMMPOWER-3. As of September 30, 2018, 86 subjects were enrolled inMMPOWER-3, and 11 sites in the United States, one site in Canada and two sites in Europe, out of an anticipated 28 sites, were initiated for enrollment. Our goal is to achieve full enrollment in the trial in early 2019.
MMPOWER-2
We initiatedMMPOWER-2, our second clinical trial for the treatment of individuals with primary mitochondrial myopathy, with the goals of understanding whether subjects with primary mitochondrial myopathy would tolerate once daily subcutaneous dosing of elamipretide, and exploring efficacy endpoints in addition to the 6MWT that we could use to assess potential benefit in our Phase 3 pivotal trial.
MMPOWER-2 was a Phase 2, double-blind, placebo-controlled crossover trial to evaluate the safety and efficacy of once daily subcutaneous administration of elamipretide in subjects previously enrolled in MMPOWER. The trial was conducted at Massachusetts General Hospital, University ofCalifornia-San Diego, University of Pittsburgh Medical Center and Akron Children’s Hospital. Thirty of the 36 MMPOWER subjects enrolled inMMPOWER-2, although one subject discontinued the trial in the second four-week treatment period due to injection site pain. Subjects were randomized in aone-to-one ratio to either 40 mg once daily subcutaneous elamipretide, which is slightly lower than the average dose exposure achieved in the high dose cohort in MMPOWER and equivalent to the dose we are testing
101
Table of Contents
inMMPOWER-3, or placebo injection for an initial treatment period of four weeks. After treatment period one, treatment was discontinued for a four-weekwash-out period. The subjects were then crossed over to the other treatment arm for a second four-week treatment period. After finishing both treatment periods, subjects were eligible to continue on elamipretide during an open-label extension trial, in which we continue to assess safety to support a potential regulatory submission and conduct limited efficacy assessments.
The objectives of the trial were to evaluate the safety, tolerability and efficacy of once daily subcutaneous elamipretide injections in individuals with primary mitochondrial myopathy. Subjects completed assessments, including the 6MWT, at initial screening, at baseline (prior to receiving the first dose) at week four, the last visit for the first treatment period at week eight, the beginning of the second treatment period at week 12, the end of the second treatment period and at week 14.
Efficacy endpoints were assessed by comparing values for subjects randomized to elamipretide at the end of each treatment period to values for subjects randomized to placebo at the end of each treatment period; exploratory biomarkers and activity counts were also evaluated. Although the primary efficacy endpoint was difference in the 6MWT from end of treatment on elamipretide to end of treatment on placebo, an important objective in conducting this trial was to identify other efficacy endpoints which might be sensitive to change, which we have now brought forward intoMMPOWER-3.
We observed statistically significant results for elamipretide across multiple endpoints, as shown in the table below.
MMPOWER-2 Summary of Data
ENDPOINT | LEAST SQUARED MEAN (CONFIDENCE INTERVAL) | P-VALUE | ||||||
6MWT (meter) | 19.8 (-2.8, 42.5) | 0.0833 | ||||||
6MWT Treatment Period 1 (meter)* | 45.3 (3.7, 85.9) | 0.0340 | ||||||
3TUG (seconds) | -0.2(-2.7, 2.2) | 0.8423 | ||||||
Neuro-QoL(T-score) | -4.0(-7.0,-1.0) | 0.0115 | ||||||
PMMSA Total Fatigue (mean score) | -1.7(-2.6,-0.8) | 0.0006 | ||||||
PMMSA Fatigue During Activity (mean score) | -0.8(-1.2,-0.3) | 0.0018 | ||||||
PMMSA Muscle Pain (mean score) | -0.4(-0.6,-0.1) | 0.0079 | ||||||
PMMSA Muscle Weakness During Activity (mean score) | -0.4(-0.7,-0.2) | 0.0019 | ||||||
PMMSA Subject Reported Most Bothersome Symptom | -0.3(-0.5,-0.1) | 0.0111 | ||||||
Patient Global Assessment (mean score) | -0.3(-0.6, 0.0) | 0.0421 | ||||||
Physician Global Assessment (mean score) | -0.3(-0.5, 0.0) | 0.0638 | ||||||
| * | Post-hoc sequence effect among subjects walking <450 meters at baseline (p=0.047 6MWT; p=0.0006 3TUG), triggeredpost-hoc Treatment Period 1 analysis. |
Regulatory agencies such as the FDA recommend that sponsors present data sets in forest plots, in which the treatment effect across various endpoints is rescaled to a common standard error unit of one and we utilized the forest plot construct in our FDA submissions. We believe this presentation to the FDA is useful to demonstrate whether there is alignment of benefit across endpoints, since concordance of benefit across multiple endpoints may provide more persuasive evidence of a treatment effect.
In the elamipretide-treated group, we observed a19.8-meter improvement on the distance walked on the 6MWT relative to the placebo-treated group, although this was not statistically significant (p=0.0833).
We observed that the subjects who were more impaired on the 6MWT at baseline, walking under 450 meters, may derive greater benefit from elamipretide treatment, as shown below. We incorporated this observation into ourMMPOWER-3 trial by excluding subjects who walk 450 meters or more on the 6MWT at screening or baseline, which we believe may enrichMMPOWER-3 trial for subjects more likely to respond on this endpoint.
102
Table of Contents
BASELINE WALK DISTANCE | CHANGE (LEAST-SQUARED-MEANS DIFFERENCE) ELAMIPRETIDE VS. PLACEBO | |
Low Walker (under 450m) (n=22) | 24.3 meters | |
High Walker (at/over 450m) (n=8) | 8.6 meters |
The PMMSA Total Fatigue score was designed to assess the fatigue and weakness that are the hallmark symptoms of primary mitochondrial myopathy. The worst (most fatigued) possible score was 16; the best (least fatigued) possible score was four. Subjects treated with elamipretide reported a clinically meaningful reduction in total fatigue from their baseline values (2.2 point, or 19%, reduction relative to baseline) and as compared to placebo (1.7 point reduction relative to placebo)(p=0.0006). Notably, subjects did not report meaningful changes in their fatigue while on placebo (0.1 points) and, for subjects on elamipretide, their fatigue levels increased toward baseline levels after withdrawal of elamipretide, as shown below.
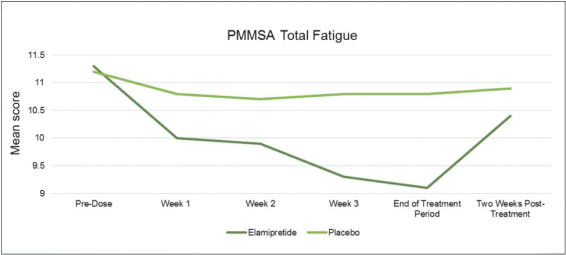
103
Table of Contents
Our interpretation of the other secondary endpoints is summarized below.
ENDPOINT | P-VALUE | INTERPRETATION | ||
Neuro-QoL Fatigue | 0.0115 | TheNeuro-QoL Fatigue Short-Form showed a reduction in fatigue in the elamipretide-treated population, with a least-squared-means differenceT-score, a converted standardized score, of(-4) (p=0.0115) relative to placebo. | ||
PMMSA Fatigue During Activities | 0.0018 | The worst (most fatigued) possible score was an 8; the best (least fatigued) possible score was a 2. Comparing the values from the final week of treatment period 1 and the final week of treatment period 2, elamipretide-treated subjects reported lower Total Fatigue During Activities relative to placebo- treated subjects, scoring a least-squared-means difference of(-0.8). | ||
| PMMSA Most Bothersome Symptom | 0.0111 | We observed an improvement in the subjects’ “most bothersome” symptom of their disease. | ||
| Triple Time Up and Go Test (TUG) | 0.8423 | The TUG showed no difference between those treated with elamipretide and those receiving placebo; however, subjects were not found to be significantly impaired on this assessment at baseline relative to healthy historic controls. This assessment was also completed in less thanone-minute, which may besub-optimal for measuring endurance-related skeletal muscle weakness and fatigue. | ||
| Patient global impression scale | 0.0421 | Elamipretide-treated subjects reported a least-squared-means(-0.28) improvement in their general health relative to placebo. | ||
| Physician global impression scale | 0.0636 | Physicians reported a least-squared means(-0.26) improvement in subject’s general health, however this was not statistically significant. | ||
Based on FDA feedback, we developed our Phase 3 secondary endpoint, theNeuro-QoL Activities of Daily Living, consisting of the following activities of daily living questions from theNeuro-QoL questionnaire developed by the National Institutes of Health which were responsive to change inMMPOWER-2, as shown below.
QUESTION | ELAMIPRETIDE (N =30) | PLACEBO (N = 30) | P-VALUE | |||||||||
I was too tired to do my household chores | 2.6 | 3.2 | 0.0025 | |||||||||
I was frustrated by being too tired to do the things I wanted to do | 2.8 | 3.3 | 0.0296 | |||||||||
I had to limit my social activity because I was tired | 2.6 | 2.9 | 0.1652 | |||||||||
I needed help doing my usual activities because of my fatigue | 2.3 | 2.7 | 0.0520 | |||||||||
I had trouble finishing things because I was too tired | 2.5 | 3.0 | 0.0189 | |||||||||
I was too tired to take a short walk | 2.4 | 3.0 | 0.0025 | |||||||||
I had to limit my social activity because of weakness | 2.2 | 2.7 | 0.0145 | |||||||||
I had to force myself to get up and do things because I was physically too weak | 2.2 | 2.8 | 0.0260 | |||||||||
Twenty-seven of the 29 subjects who completed MMPOWER and/orMMPOWER-2 enrolled inMMPOWER-OLE, an open-label extension trial we are conducting which will contribute to our safety database in this population and includes periodic efficacy assessments to support the durability of any effects observed in the controlled phase of the trial. In addition, one of the subjects from MMPOWER who did not participate inMMPOWER-2 has subsequently enrolled inMMPOWER-OLE. While we have not observed meaningful changes in 6MWT during ongoing assessments, we have observed maintenance of the reduced PMMSA Total Fatigue through 12-months of therapy (which 24 subjects have now completed) during this open-label extension trial.
MMPOWER
MMPOWER was a Phase 1/2, multiple ascending dose, double-blind, placebo-controlled trial with 36 subjects between the ages of 16 and 65 with genetic confirmation of mitochondrial disease and a clinical diagnosis of primary mitochondrial myopathy. The trial was conducted at Massachusetts General Hospital, University of
104
Table of Contents
California-San Diego, University of Pittsburgh Medical Center and Akron Children’s Hospital. Nine subjects received a low dose of elamipretide (0.01 mg/kg hour, for an average actual drug exposure of 1.4 mg), nine subjects received amid-dose of elamipretide (0.10 mg/kg hour, for an average actual drug exposure of 12.7 mg), nine subjects received a high dose of elamipretide (0.25 mg/kg hour, for an average actual drug exposure of 29.6 mg) and nine subjects received a placebo dose once daily bytwo-hour IV infusion over a treatment period of five days. The high dose of elamipretide tested in MMPOWER is slightly lower than the 40mg subcutaneous dose we tested inMMPOWER-2 and are testing inMMPOWER-3.
The objectives of the trial were to evaluate the safety, tolerability and efficacy of elamipretide in individuals with primary mitochondrial myopathy. Subjects completed efficacy assessments, including the 6MWT (the primary efficacy endpoint) at initial screening, at baseline (prior to receiving the first dose), on the fifth day (after the last dose), and on the seventh day (two days after the last dose).
We observed a dose-dependent increase insix-minute walk distance (p=0.0142 by linear trend test) after five days of treatment. The data showed that subjects who received the high dose of elamipretide, which was the primary dose of interest, walked an average of 64.5 meters further after five days of treatment with elamipretide than they walked before receiving elamipretide. As adjusted for the 20.4 meter improvement observed in the placebo-treated group, this represents a44.1-meter least-squares mean improvement relative to placebo (p=0.053). Apost-hoc adjustment for gender and baseline distance walked, the factors most responsible for variability within the data, as published inNeurologyinMarch 2018 by our principal investigators, demonstrated a51.2-meter least-squares mean improvement relative to placebo (p=0.03), as depicted below.
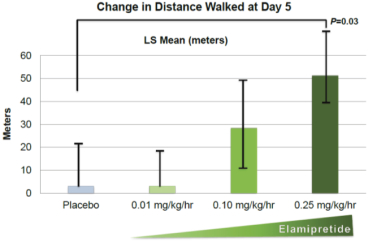
As noted above, apost-hoc analysis of the data revealed that subjects’ performance on the 6MWT at baseline was predictive of how much they may improve after elamipretide treatment (a treatment by baseline interaction, with anR-squared value of 0.42, meaning approximately 42% of the variability in the data as a whole is explained by the model). This analysis demonstrated that the more impaired subjects, walking less than 450 meters at baseline, were more likely to improve with elamipretide, whereas less impaired subjects, walking more than 450 meters at baseline, had less potential for improvement. A healthy individual can typically walk between 500 and 600 meters on the 6MWT, which may suggest that those walking over 450 meters at baseline are not substantially impaired in their ability to perform this assessment. As discussed above, we observed similar preferential benefit for more impaired subjects inMMPOWER-2 and have accordingly enriched ourMMPOWER-3 trial population by excluding subjects who walk more than 450 meters on the 6MWT at screening or baseline.
We explored other secondary and exploratory efficacy endpoints in MMPOWER, including questionnaires and biomarkers, but we did not observe meaningful findings in these other endpoints.
Elamipretide Clinical Programs—Barth Syndrome
Barth is estimated to affect between one in 300,000 to one in 400,000 births in the United States and there are estimated to be less than 200 known living patients worldwide with Barth. There are no therapies approved by the FDA, EMA or NMPA for the treatment of Barth. We have received Fast Track designation and Orphan Drug designation from the FDA for the development of elamipretide in Barth.
105
Table of Contents
Barth typically presents in infancy or early childhood. The disease is characterized by reduced muscle tone, muscle weakness, undeveloped skeletal muscles, delayed growth, fatigue, varying degrees of physical disability, heart muscle weakness, or cardiomyopathy, which makes it harder for the heart to pump blood to the rest of the body, and low white blood cell count, or neutropenia, which can compromise the body’s ability to fight off infections. Some individuals with Barth require one or more heart transplants, including during infancy. Implantable cardioverter defibrillators may be used to prevent sudden death due to life-threatening ventricular arrhythmias, and other heart failure medications includingACE-inhibitors and beta blockers may also be used to help manage cardiac symptoms. In addition to medical and surgical intervention, individuals with Barth may require physiotherapists and occupational therapists, speech and language therapists, psychologists and educational support workers. Barth can be a lethal infantile and early childhood disease, and mortality is highest in the first four years of life. Although improvements in the management of the disease have increased survival for some patients, with reports of individuals with Barth living into their late 40s and a single individual with Barth reported as surviving to age 51, the disease nevertheless is associated with premature death.
Barth is caused by a genetic mutation in the TAZ gene that leads to decreased production of tafazzin, an enzyme required to assemble cardiolipin; as a result there is an abnormal composition of cardiolipin, particularly in the heart and skeletal muscle mitochondria in individuals with Barth. Barth patients have less tetralinoleylcardiolipin, orL4-CL, and increased amounts of monolysocardiolipin, or MLCL, than healthy subjects, and the disease can be diagnosed by the ratio of MLCL to L4-CL, called the MLCL:CL ratio or genetic testing. MLCL, a phospholipid found in the inner mitochondrial membrane, is considered to be an immature form of cardiolipin. As illustrated below, MLCL is structurally differentiated from L4-CL due to its lack of a fourth acyl chain, which alters the typical conical structure of the lipid causing alterations to mitochondrial morphology. These morphological alterations result in destabilization of respiratory chain supercomplexes and increased oxidative stress. Studies have shown increased susceptibility of cardiolipin to peroxidation in Barth patient derived pluripotent stem cells, leading to increased accumulation of MLCL.
106
Table of Contents
The images of lymphoblast mitochondria below indicate that, compared to normal mitochondria, the mitochondria of individuals with Barth have unhealthy morphology, including a lack of inner membranes, a poor alignment of cristae, which are the curves of the IMM, and swollen or collapsed segments of cristae.
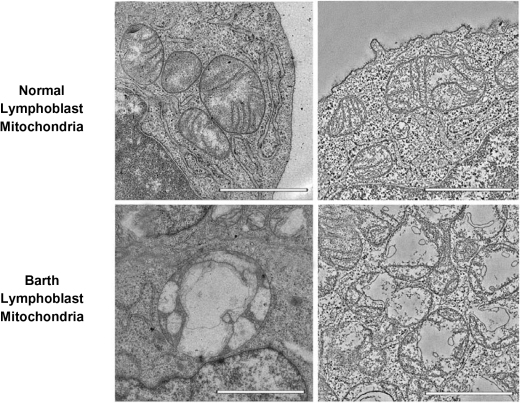
The Barth Syndrome Foundation, an advocacy group for Barth awareness and research, asked us to conduct a clinical trial of elamipretide for Barth. As the mechanism of elamipretide is to bind reversibly to cardiolipin, which is deficient in individuals with Barth, we undertook preclinical work to better characterize the safety profile of elamipretide for Barth as well as to gain insight into whether there would be adequate target engagement for elamipretide given the severe depletion of cardiolipin that characterizes this disease. Analyses of cardiolipin levels in Barth patient-derived lymphoblasts have shown up to 60% lower levels of cardiolipin than in healthy control cells, as shown below; this cardiolipin deficit has been found to range to up to 95% in other Barth cell lines or animal models.

107
Table of Contents
Preliminary preclinical results from a study in mice in which the TAZ gene was “knocked down” did not indicate any safety concerns.
Additionally, as shown below,ex vivo studies of elamipretide in cardiomyocytes, or heart cells, derived from individuals with Barth demonstrated elamipretide’s potential to improve Barth oxygen consumption rate, or OCR, an indicator of mitochondrial respiration, despite an approximate 80% reduction in cardiolipin levels. In this study, the ‘resting’ period, which represents a ‘basal’ state, is when substrates required for ATP production are present and respiration and ATP production is occurring. Then, oligomycin, an ATP synthase inhibitor, is added to block ATP production. At this stage, respiration represents requirements to keep the mitochondrial membrane potential in place without energy required to synthesize ATP. Next, inhibitors (Antimycin and Rotenone) are added to block respiration completely. Maximal respiration was achieved by the addition of carbonilcyanide p-triflouromethoxyphenylhydrazone, or FCCP, an uncoupler of mitochondrial oxidative phosphorylation which stimulates increased respiration.
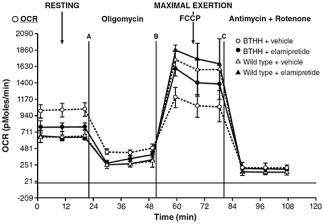
In laboratory experiments, elamipretide interacted with the abnormal MLCL found in Barth cardiac and skeletal muscle tissue in a similar ratio as it interacted with normal cardiolipin, which is believed to be a two cardiolipin to one elamipretide molar ratio. In another experiment, lipid vesicles that model the IMM were synthesized, and the effect of membrane lipid composition on membrane structure (area) was determined. Cardiolipin comprises approximately 20% of inner membrane lipids, and the addition of cardiolipin was observed to increase membrane area, consistent with the cone-shaped structure of cardiolipin. Losses of cardiolipin were modeled based on changes typically seen in diseases including heart failure and renal disease and the loss of cardiolipin was associated with decreased membrane area. We observed that elamipretide-mediated aggregation of cardiolipin ameliorated the loss by acutely restoring the membrane area, as shown below. In diseases characterized by pronounced loss of cardiolipin such as Barth, there is a profound decrease in membrane structure that was attenuated with elamipretide. These observations suggest that elamipretide’s therapeutic benefit may be more pronounced or more rapidly observed in subjects with more moderate cardiolipin loss.
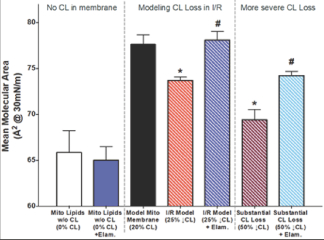
108
Table of Contents
While Barth patients have some normal cardiolipin, the ratio of abnormal MLCL to normal cardiolipin (the MLCL:CL ratio) may vary from patient to patient. For example, in the study we conducted with Barth patient-derived cardiomyocytes, described above, we observed an approximate 80% reduction in normal cardiolipin, whereas other studies of patient-derived lymphoblasts have shown an approximate 60% reduction in normal cardiolipin, as discussed above. Up to 95% reduction has, at times, been reported in the literature.
The MLCL:CL ratio has been observed to correlate with functional impairment; patients with a lower MLCL:CL ratio are typically less impaired than those with a higher MLCL:CL ratio. For example, a prior observational study of 34 Barth patients suggests that the MLCL:CL ratio is inversely correlated with performance on the 6MWT (p=0.00014). Accordingly, if elamipretide’s reaction to normal cardiolipin is critical to therapeutic effect, such therapeutic effect may also vary among patients, and as a result may only benefit a subset of such patients.
We initiated TAZPOWER, a clinical trial of elamipretide for individuals diagnosed with Barth, in the third quarter of 2017 at Johns Hopkins. TAZPOWER is a double-blind, placebo-controlled cross-over trial to evaluate the efficacy of once daily subcutaneous administration of elamipretide in 12 individuals who are 12 years of age or older and have been diagnosed with Barth. Subjects were randomized in aone-to-one ratio to either 40 mg elamipretide administered daily by subcutaneous injection or placebo for an initial12-week treatment period. After this initial treatment period, treatment is discontinued for a four-weekwash-out period, following which the subjects cross over to the other treatment arm for a second12-week treatment period.
Subjects enrolled in TAZPOWER are eligible for participation in an optional open-label extension trial that will contribute to our safety database and may include periodic efficacy assessments to support the durability of any effects observed in the controlled phase of the trial. We have completed the placebo-controlled portion of TAZPOWER, and are continuing to assess efficacy endpoints during the open-label extension phase, in which eight subjects are currently enrolled.
The objectives of the trial were to evaluate the safety, tolerability and efficacy of once daily subcutaneous elamipretide injections in individuals with Barth. During each of treatment periods one and two, subjects completed assessments including the 6MWT at the beginning of each treatment period, four weeks into each treatment period, and at the end of each treatment period; certain assessments were also conducted at initial screening, and at afollow-up visit, four weeks following the end of the second treatment period. In addition, the Barth Syndrome Symptom Assessment, or BTHSA, a patient reported outcome questionnaire developed based upon interviews of individuals with Barth to measure the fatigue and muscle weakness associated with the disease, was completed by subjects daily, and assessed based on the average of seven days of daily values preceding the assessment date.
Elamipretide was reported to be well-tolerated by patients with Barth. Other than injection site reactions, which were experienced in both groups but with higher frequency in the elamipretide treatment group, there were overall less events reported during the elamipretide treatment periods of the trial, as compared to the placebo treatment periods.
TAZPOWER did not meet its primary efficacy endpoints of (i) change in the 6MWT between end of treatment on elamipretide and end of treatment on placebo or (ii) change in Total Fatigue on the BTHSA, which is composed of three questions from the BTHSA, assessing tiredness at rest and during activities and muscle weakness during activities, between end of treatment on elamipretide and end of treatment on placebo. With respect to the Clinical Global Impression of Change, a secondary endpoint involving an overall assessment by the investigator of each subject’s Barth symptoms, we observed an improvement between end of treatment on elamipretide and end of treatment on placebo, with the investigator reporting positive change for nine out of the 12 patients over the elamipretide treatment period. Additionally, eight of 11 caregivers completing the Caregiver’s Global Impression of Change also reported positive changes in Barth symptoms during the elamipretide treatment period.
109
Table of Contents
We conducted a prespecified subgroup analysis intended to assess whether elamipretide’s association with normal cardiolipin is related to therapeutic effect, that is, whether elamipretide may provide greater benefit to a subset of Barth patients who have lower MLCL:CL ratios. This entailed an assessment of the six patients above (“high ratio subjects”) and six patients below (“low ratio subjects”) the median MLCL:CL ratio of the subjects enrolled in TAZPOWER, which was 17.3. In this subgroup analysis, we observed a correlation between improvements in 6MWT and baseline ratios, as shown below. We believe this suggests that elamipretide therapy may preferentially affect low ratio subjects.
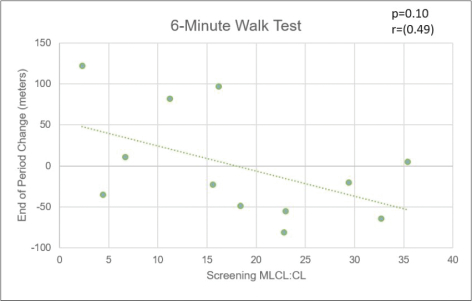
We assessed performance between high ratio and low ratio subjects on other key efficacy endpoints. From this analysis, we observed that low ratio subjects showed overall greater improvement on elamipretide therapy than on placebo, particularly as compared to high ratio subjects, as reflected below. We believe these signals, coupled with data from the ongoing open-label extension portion of the trial, may support submission of an NDA for this indication. We plan to discuss a potential NDA submission with the FDA during the first half of 2019.
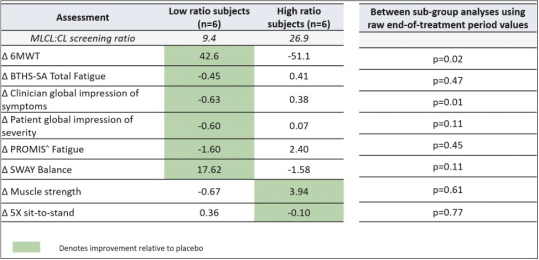
The 21st Century Cures Act, or the Cures Act, elevates the role of the patient in the development of drugs, giving patients a greater voice when developing treatments for their diseases. Under this Act, sponsors are encouraged to incorporate the patient experience in their regulatory submissions. Accordingly, all subjects participating in the TAZPOWER trial were eligible to participate in a qualitative study in which we conducted videotaped interviews with trial participants through a smartphone application to explore their experiences during and after the trial and to
110
Table of Contents
better understand the treatment outcomes that are meaningful to them. For subjects participating in open-label extension, interviews were conducted after three-months of open-label extension therapy, unless sooner terminated. As of November 30, 2018, nine of the 12 TAZPOWER subjects and/or their caregivers have participated in this study. Interview questions addressed life before elamipretide injections (shots), daily life today (i.e., as of the date of each participant’s interview), fatigue and weakness today, other aspects of Barth today, shots: round 1, stopping the shots, and shots: round 2. Eight of the nine participating subjects reported improvement while on elamipretide therapy during open-label extension, and six of those eight subjects correctly identified during which of the two double-blind treatment periods they were receiving elamipretide.
Subjects characterized the improvement in fatigue in relation to their activities of daily living and quality of life. For example, one subject was able to go swimming and hiking with his friends at Boy Scout camp, which he had not previously been able to do. Another subject was able to walk his dog without stopping to rest and required less recovery time from that exertion. Two subjects reported being able to participate in physical education class at school instead of having to sit out. Several subjects reported increased appetite.
Two of the four study participants randomized to elamipretide in the placebo-controlled portion of the TAZPOWER trial reported reversion to their baseline symptoms quickly after withdrawal of therapy during the washout period. One reported a perceived decline in quality of life less than 48 hours from stopping therapy, which he characterized as depressing. Another reported that his grades declined because he found it harder to focus and was falling asleep at school again.
We are observing continued improvement in distance walked on the 6MWT during the open-label extension portion of the TAZPOWER trial, in which 10 subjects enrolled and two subjects have completed 36 weeks of treatment, an additional five subjects have completed 24 weeks of treatment, and an additional two subjects have completed 12 weeks of treatment, as shown below. We are conducting a review of the natural history of Barth to evaluate this and any other longitudinal trends we may observe during open-label treatment.
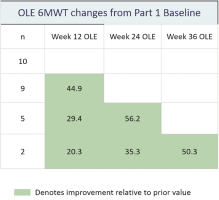
We plan to request a meeting with the FDA, which we expect to have during the first half of 2019. The objective of the meeting will be to discuss our plan to submit an NDA for elamipretide for the treatment of Barth and to seek alignment regarding our regulatory path forward. We believe the data from our MMPOWER program may be supportive of our Barth development efforts. We also believe our development efforts in Barth may support the development of elamipretide in primary mitochondrial myopathy, given that patients with Barth have even lower levels of cardiolipin and we have still seen evidence of target engagement. We also believe that our experience from a compassionate use protocol for an infant with Sengers syndrome may provide further support.
Elamipretide Compassionate Use—Sengers syndrome
Sengers syndrome (Sengers) is an autosomal recessive mitochondrial disorder characterized by early onset hypertrophic cardiomyopathy, congenital cataracts and hypotonia. The prevalence of Sengers is unknown, however, according to Orphanet, a European reference portal for information on rare diseases, approximately 40 cases had been reported worldwide as of June 2014. Approximately half of the patients diagnosed with Sengers die within the first year of life due to cardiac failure associated with a fatal neonatal form of the disease. Sengers and Barth are thought to have overlapping phenotypes since both lead to depletion of mitochondrial cardiolipin and both are known to cause severe hypertrophic cardiomyopathy.
111
Table of Contents
In June 2018, we collaborated with doctors at the Department of Pediatrics, Barnaspitali Hringsins and the Department of Genetics and Molecular Medicine, Landspitali University Hospital, both in Reykjavik, Iceland, and the McKusick-Nathans Institute of Genetics Medicine at Johns Hopkins University to implement an elamipretide compassionate care protocol for a 3-month old infant diagnosed with the neonatal form of Sengers being treated at the neonatal intensive care unit at Landspitali University Hospital. In the first few months of life, the child was noted to have severe hypertrophic cardiomyopathy, bilateral cataracts and significant hypotonia. Average published survival of children presenting at this age is approximately 4.2 months.
The child received 0.25 mg/kg/day of elamipretide intravenously for the first six weeks, and thereafter received 0.5 mg/kg/day elamipretide therapy once daily. The patient’s cardiac function improved in the first few weeks of treatment and remained stable through November 30, 2018, with a 53% increase in left ventricular internal dimension in end-diastole and stabilization of left ventricle septal and posterior wall thickness despite a 40% weight gain due to normal growth. After approximately six months of elamipretide therapy, the patient improved from markedly ill to borderline ill as reported by a clinical global impression of severity of illness assessment, as shown below. This assessment, which is based on weekly evaluations, suggests that the patient improved at over 60% of the evaluations conducted since starting elamipretide therapy and was only thought to worsen on one occasion. The patient was subsequently discharged to home. Elamipretide appeared to be well-tolerated by this patient with no obvious associated side effects. The treating physician expressed a belief that elamipretide contributed to the patient’s disease stabilization.
After a surgical procedure in December 2018, prior to which the patient had been stable, the patient experienced severe cardiac decompensation and multi-organ failure and succumbed to his disease at approximately nine months of age.
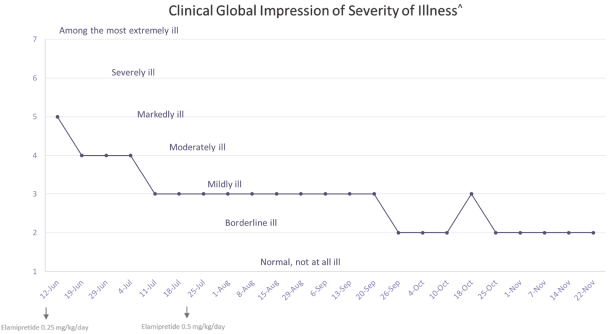
Elamipretide Clinical Programs—LHON
We estimate that approximately 10,000 individuals in the United States have LHON. Currently, there are no treatments approved by the FDA or the NMPA for the treatment of LHON. Raxone (idebenone), a synthetic form of Coenzyme Q10, has been approved by the EMA for the treatment of LHON, although actual availability varies by country. Raxone has orphan designation, and its marketing authorization was granted by the EMA under its authority to grant marketing authorization under “exceptional circumstances” due to the lack of comprehensive data on efficacy and safety.
112
Table of Contents
We have received Fast Track status and Orphan Drug designation from the FDA for the development of elamipretide for this indication. China has recently included LHON as an orphan disease on its published list of orphan diseases.
We have conducted a Phase 1 clinical trial of elamipretide topical ophthalmic drops for this indication, in which we observed some trends in response rates suggestive of therapeutic effect, for which we are continuing to assess efficacy data in an ongoing open-label extension trial. We plan to expand the open-label portion of this trial to include additional patients in the United States and China. We have engaged regulatory advisors in China to begin preparation for this expansion and expect to file our pre-clinical trial application to the NMPA by the end of 2018.
LHON is a mitochondrially inherited genetic disorder passed from a mother carrying the mutation to her children. LHON causes degeneration of the optic nerve in the back of the eye and leads to bilateral blindness, and primarily affects young men between the ages of 18 and 30, although it can affect women as well as younger children. The initial clinical expression of LHON is often a sudden, painless, acute orsub-acute central vision loss, often accompanied by loss of color vision and reduced visual acuity. A typical presentation involves a young man experiencing increased oxidative stress, sometimes from increased alcohol and/or tobacco consumption, leading to sudden vision loss in one eye that typically progresses within six months of onset to bilateral blindness. The disease has a substantial impact onday-to-day functioning, making it difficult to read and perform everyday activities, including employment-related activities and driving. The disease has a severe negative impact on quality of life and LHON individuals may require social services, occupational rehabilitation and visual aids.
A subclass of LHON patients also present symptoms, including muscle weakness, poor coordination, and numbness, tremors and abnormalities of the electrical signals that control the heartbeat (cardiac conduction defects). Some families have particularly severe manifestations, including ataxia, juvenile onset encephalopathy, spastic dystonia and psychiatric disturbances. These phenotypes have been called “LHON plus syndromes.”
Mitochondria are central to retinal cell function and survival and dysfunctional mitochondria may lead to death of retinal ganglion cells, which are neurons located near the inner surface of the retina. Mitochondrial dysfunction is a key factor in LHON and other genetic optic neuropathies characterized by loss of visual function resulting from impaired cellular energetics within retinal ganglion cells and the optic nerve.
Electron microscopy imaging of mitochondria from LHON subjects shows abnormal morphology suggestive of dysfunctional mitochondria. This abnormal mitochondrial morphology has also been observed in the retinal ganglion cells in a mouse model of LHON. The images below show retinal ganglion cells from a wild-type mouse, left, and an LHON mutant mouse model, middle. The image on the right shows an enlarged image of the mitochondria in the retinal ganglion cells of the mutant mouse.
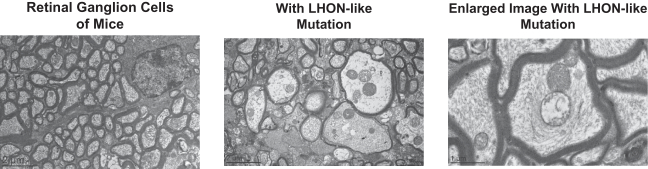
We believe based onpre-clinical and early clinical findings that systemic elamipretide may be beneficial for subjects with LHON and LHON plus, in which the mitochondrial dysfunction is the result of a mutation in a subunit of Complex I of the electron transport chain which impacts the retinal ganglion cells and the optic nerve. Preclinically, elamipretide has been observed to improve mitochondrial function under oxidative stress conditions in mouse-derived retinal ganglion cells, the type of cells most affected by LHON, by dose-dependently reducing ROS production, mitochondrial depolarization, cytochrome c release, morphological change, apoptosis and cell death. Ongoing experiments in a mouse model of acute traumatic optic neuropathy also suggest that systemic administration of
113
Table of Contents
elamipretide post-trauma may improve retinal ganglion cell survival and visual function, supporting the plausibility of therapeutic benefit in the presence of LHON associated, oxidative-stress mediated damage of the optic nerve.
In our MMPOWER andMMPOWER-2 clinical trials, in which most subjects are believed to have had some degree of Complex I dysfunction, we observed clinical benefit following systemic elamipretide administration. One LHON plus subject who enrolled in both studies and continues to receive elamipretide during the open-label extension trial experienced improvement in various disease symptoms, including improvement in vision such that the subject received medical clearance to drive for the first time in seven years. In addition, we believe we are observing trends suggestive of potential clinical benefit in our ReSIGHT Phase 2 clinical trial of topical ophthalmic drops for patients with the G11778A mutation of LHON, in which subjects are continuing treatment with elamipretide during an open-label extension trial.
ReSIGHT, our first clinical trial of elamipretide for the treatment of LHON, was a52-week, randomized, double-masked, vehicle-controlled clinical trial of elamipretide topical ophthalmic drops in 12 subjects with LHON. Subjects were randomized to a single drop of elamipretide 1.0% ophthalmic solution or placebo, twice daily, with four subjects receiving elamipretide dosed in both eyes and eight subjects receiving elamipretide in one eye and placebo in the other eye. The endpoints were safety, tolerability and efficacy. The primary efficacy endpoint was change in best corrected visual acuity, or BCVA, during the period from week 20 through the end of treatment at week 52; secondary endpoints included changes in color vision, changes in photopic negative response electroretinography, a biomarker measuring the response of the retinal ganglion cells to light, changes in the retinal nerve fiber layer and retinal ganglion layer thickness, and changes in visual field, or field of vision, as measured by the Humphrey visual field score, which is the expanse of space visible at a given instant without moving the eyes. Subjects enrolled in ReSIGHT were eligible for participation in an optional open-label extension trial that will both contribute to our safety database and include periodic efficacy assessments to support the durability of any effects observed in the controlled phase of the trial. Eleven of the 12 subjects are currently participating in the open-label extension trial.
ReSIGHT enrolled individuals with the G11778A LHON genetic mutation who experienced loss of vision in both eyes of greater than one year and less than ten years, because the degree of visual impairment in these patients was expected to remain stable absent therapeutic intervention. It is considered unlikely that individuals with the G11778A genetic mutation will experience visual recovery spontaneously, meaning without any therapeutic intervention; the partial recovery rate, most commonly occurring within the first year following vision loss, has been reported to be between 4% and 33% for these individuals.
114
Table of Contents
We observed trends suggestive of therapeutic effect in ReSIGHT, but the trial did not meet its primary endpoint of change in BCVA as the average change over week 20 to 52 from baseline. We believe this was largely due to unexpected variability in the placebo group, in which two subjects experienced gains in BCVA of more than 20 letters on a standard eye chart and one subject experienced a loss of more than 20 letters, resulting in no change overall between elamipretide and placebo treated groups. However, improvement in elamipretide-treated eyes was observed across a number of other endpoints over the treatment period, as shown below.
The following table sets out certain data with respect to the ReSIGHT clinical trial measuring the endpoints from baseline to week 52 (averaged, in the case of BCVA, Humphrey Visual Field and Color Discrimination, over the entire treatment period). We plan to utilize a forest plot construct in our submission of the ReSIGHT data to the FDA.
ReSIGHT Summary of Data
ENDPOINT | LEAST SQUARED MEAN (CONFIDENCE INTERVAL) | P-VALUE | ||||||
BCVA (letters) | 0.6 (-0.9, 2.1) | 0.4370 | ||||||
Humphrey Visual Field (mean deviation) | 0.8 (0.1, 1.4) | 0.0173 | ||||||
Color Discrimination | 0.2 (0.0, 0.4) | 0.0826 | ||||||
Retinal Nerve Fiber Layer Thickness | 1.9 (-3.3, 7.0) | 0.4390 | ||||||
Retinal Ganglion Cell Layer Thickness | 1.6 (-0.5, 3.7) | 0.1274 | ||||||
Visual Function Questionnaire Composite* | 6.0 (2.1, 9.9) | 0.0063 | ||||||
| * | Post-hoc analysis of change from baseline (all subjects). |
The below further summarizes certain post hoc analysis of the data from ReSIGHT, which was conducted with a central field analysis.
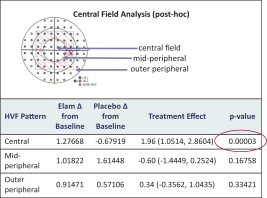
All subjects participating for at least three months in the open-label extension part of the ReSIGHT trial were eligible to participate in a qualitative study in which we conducted videotaped interviews with trial participants through a smartphone application to explore their vision experiences during and after the trial and to better understand the treatment outcomes that are meaningful to them. Nine of the 12 ReSIGHT subjects participated in this study. Interviews addressed aspects of changes in vision with respect to general vision, testing their eyes, screens and magnification, daily living, color and light and summary. A number of subjects reported improvements in visual function as well as quality of life, as summarized in the charts below, which were prepared by external evaluators who analyzed written transcripts of the interviews pursuant to pre-identified conceptual frameworks. With respect to improvements in activities of daily living, one subject reported being able to see the denomination of money better, another remarked that he can see faces better and now has the vision he needs to get to his classes independently, another remarked that he does not rely upon accessibility devices such as CCTV as much as he used to, and is able to see street crossing signs now. Another advised that he can now see when to cross the street from the distance of across the street, another reported he does not rely upon friends for help cooking or doing laundry as much as he
115
Table of Contents
used to, and another mentioned he can now ride his bike again and has experienced improvement in his activities of daily living. We believe these interviews help qualify the clinical relevance and meaningfulness of changes in endpoints observed during the ReSIGHT trial.
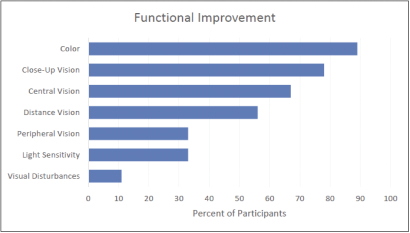
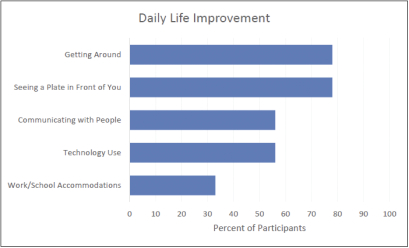
We also observed continued improvement in parameters of visual function, including BCVA, color sensitivity, contrast sensitivity and visual field, particularly central visual field, as illustrated below.
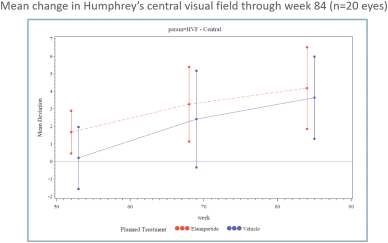
116
Table of Contents
Our original discussions with the FDA presumed we would conduct a pivotal Phase 3 trial following ReSIGHT. We plan to discuss the results of the ReSIGHT trial with the FDA to inform next steps with respect to the regulatory path forward in the United States, including whether a second trial will be required to support approval and the design of any such trial. We have identified sites in China willing to participate in a subsequent trial, and are preparing our NMPA clinical trial application to submit following our end-of-Phase 2 meeting with the FDA. We may consider increasing the dose or frequency of administration of topical ophthalmic drops or administering elamipretide subcutaneously based upon the results of our discussions with the FDA and NMPA. If we decide to conduct a Phase 3 clinical trial, we expect it would include sites in the United States and China. We believe the inclusion of sites in China may help expedite enrollment.
Patient-focused Drug Development and 21st Century Cures Act in the Context of Primary Mitochondrial Myopathy, Barth and LHON
The FDA’s Patient-Focused Drug Development initiative is an FDA commitment under the fifth authorization of the Prescription Drug User Fee Act to more systematically gather patients’ perspectives on their condition and available therapies to treat their condition. As part of this commitment, the FDA is holding a series of public meetings, each focused on a specific disease area. Pursuant to this initiative, the FDA met with Barth patients and advocates in July 2018, and has agreed to meet with primary mitochondrial myopathy patients and advocates in March 2019, in each case to hear directly from patients, patient caretakers and other patient representatives about their experiences with their debilitating conditions, including the disease symptoms and daily impacts that matter most to patients. At the Barth meeting, for example, patients and their caretakers spoke about the severe impact that fatigue has upon the quality of life for Barth patients. There was also a discussion of treatment options for Barth, during which a father of twin sons enrolled in our TAZPOWER trial remarked that he believed one of his sons was on elamipretide in treatment period one, and the other in treatment period two, before both went into open-label extension. He commented on his perceived positive impact of the study on his sons, including better appetites, improved energy levels and increased physical activity. We believe these meetings are important to educate the FDA about the significant clinical burden of these diseases and their devastating impact on patient’s activities of daily living, and we have supported advocacy groups’ efforts to prepare for these meetings. Other than educating regulators about the burden of these diseases in which we are studying elamipretide as a potential therapy, these meetings have no direct impact on our clinical development efforts.
The video protocols we conducted or are conducting as part of our MMPOWER-3, TAZPOWER and ReSIGHT programs will enable us to incorporate the patient experience in our regulatory submissions as encouraged by the Cures Act. The video protocol will be open during the open-label extension for subjects that participated in MMPOWER-3 at U.S. sites. Our approach to incorporate the patient voice under the Cures Act in this manner was informed by prior experience in our MMPOWER andMMPOWER-2 programs. In MMPOWER, certain of our clinical trial sites collected videotaped interviews of consenting subjects at baseline, before treatment commenced, at day five, which was the end of treatment, and at day seven, which was two days after treatment stopped. Our review of those interviews revealed important anecdotal learnings about certain subjects’ perceptions of changes in their symptoms over the course of the trial, as described in several examples below:
| ∎ | one subject reported that following five days of high dose elamipretide, he no longer needed to use his walker for support while ambulating and he was able to complete more daily activities, such as shaving, due to his increased strength; his clinician observed increases in his muscle tone; |
| ∎ | one subject reported that following five days ofmid-dose elamipretide, she experienced more energy and felt more sensations, such as being able to feel the air she inhaled when taking a deep breath, which she had not realized she was unable to feel before she received elamipretide treatment; |
| ∎ | one subject reported improved ability to walk, including being able to go up hills without her legs burning and her heart racing, and to see, including improvements in her double vision and ability to read; and |
| ∎ | one subject sent us videos chronicling her disease manifestation, diagnostic journey and perceived improvement during (i) MMPOWER, in which she progressed from needing a wheelchair or scooter to walk, at the beginning of the trial, to being able to walk without assistance, after five days ofmid-dose elamipretide,(ii) MMPOWER-2, after which she was able to dance, was cleared to drive for the first time in seven years due to visual improvement and was able to reduce her pain medications, and (iii) the open-label extension trial, during which she reported continued improvement. |
117
Table of Contents
Although reports of this nature are anecdotal in nature and not all subjects report improvements following treatment with elamipretide, we do think accounts of this nature will help encapsulate the patients’ perspective on any benefits they experience in ourMMPOWER-3, TAZPOWER and ReSIGHT programs consistent with the Cures Act.
Elamipretide Clinical Programs—Diseases Associated with Aging
We believe that there is significant potential for mitochondrial medicine in diseases related to aging. We are evaluating the potential clinical utility of elamipretide in dry AMD, a disease associated with aging. We have also evaluated the potential clinical utility of elamipretide in proof-of-concept clinical trials in aging skeletal muscle weakness, acute kidney injury and heart failure, which are also associated with aging. Although we saw signs of clinical benefit in some of these studies, we do not plan to progress development of elamipretide for indications other than dry AMD in the United States. We may consider development of certain of these indications for other territories, including China, and we also believe that certain of these indications may be suitable for new pipeline compounds.
Ophthalmic Diseases
Normal mitochondria play a critical role for ocular function, and dysfunctional mitochondria are implicated in several common diseases of the eye, many of which are associated with aging. Ophthalmologic diseases that have not traditionally been considered to have obvious mitochondrial origins are increasingly recognized to result in part from impaired mitochondrial function, increased oxidative stress and increased apoptosis. As a high energy-demand organ, the eye is particularly susceptible to the consequences of mitochondrial damage. Oxidative damage that results over time from mtDNA instability leads to cumulative mitochondrial damage, which is recognized to be an important pathogenic factor inage-related ophthalmologic disorders such as diabetic retinopathy, glaucoma and dry AMD.
Delivery of therapeutic compounds to various sections of the human eye can be challenging. The eye has evolved to protect itself by washing foreign substances such as eye drops from the surface, with tears capable of removing as much as 95% of an eye drop. The vitreous in the interior of the eye also poses a barrier to delivery of therapies from the front of the eye to the retina. For systemic delivery, the blood—retinal barrier can prevent substances, particularly large molecules, from entering the tissue of the retina. We have evaluated both systemic and topical delivery of elamipretide in both preclinical studies and clinical trials.
Dry AMD
We are advancing development of elamipretide for dry AMD, an ophthalmic disease associated with aging and the leading cause of blindness among older adults. Dry AMD is estimated to impact approximately 10 million individuals in the United States and is the leading cause of blindness among older adults in the developed world. There are no treatments approved by the FDA, the EMA or the NMPA for the disease.
The earliest clinical manifestation of dry AMD is often a reduction in low luminance, or low light, visual acuity, which can make it challenging to conduct normal daily activities such as reading in artificial light, driving at dusk or at night and navigating indoors in low light. The disease may progress to entail blurred vision and loss of central vision, which can impair facial recognition, mobility, watching television and computer use, and can eventually lead to blindness. These limitations may impair the independence of older adults and have been associated with increased depression.
The pathophysiology of dry AMD includes the formation of cellular debris, called drusen, which disrupt the retinal pigment epithelium, a layer of cells between the retina, which collects light and converts it into neural signals to transmit to the brain, and the choroid, or vascular membrane, at the back of the eye. The disease may also involve the gradual deterioration, or geographic atrophy, of the central part of retina, known as the macula. The retinal pigment epithelium provides nutrition to the retina, which has a very active metabolism. The eye is the highest consumer of mitochondrial ATP in the central nervous system, due to the intensive bioenergetics required to support visual function. Preclinical studies suggest that diseases of the retinal pigment epithelium, such as dry AMD, may be exacerbated by light- induced mitochondrial dysfunction, and that mitochondrial DNA mutations appear to accumulate over time in diseased retinal pigment epithelium as a consequence of chronic and ongoing oxidative stress. Cigarette smoking and high fat diets, both of which contribute to mitochondrially deleterious oxidative stress, are known to be environmental risk factors for dry AMD onset and progression. These findings suggest a key role for mitochondrial dysfunction in the pathology of the disease.
118
Table of Contents
The table below provides a summary of our completed and planned trials for dry AMD.
TRIAL | INDICATION | STAGE; | TRIAL DESIGN | |||
| ReCLAIM | dry AMD | Phase 1; completed in March 2018 | Open label, single-center clinical trial involving 19 subjects withnon-central geographic atrophy, which occurs when the photoreceptors no longer work and the patients develop a blind spot or spot of poor vision in the macula, and 21 subjects with high risk drusen, which are large deposits of debris located between the retina and the Bruch’s membrane, that can interfere with waste products getting removed from the macula. Subjects received once daily subcutaneous injections of elamipretide for 24 weeks. | |||
| ReCLAIM-2 | dry AMD | Phase 2b; planning for start in the first quarter of 2019 | Double-blind, placebo controlled, multi-center clinical trial involving approximately 180 subjects withnon-central geographic atrophy, receiving once daily subcutaneous injections of either elamipretide or placebo for ~48 weeks. | |||
In preclinical models of dry AMD, published inRetina Todayin May/June 2015, researchers at Duke Eye Center observed that elamipretide prevented disease progression and reversed symptoms of disease. This study utilized hydroquinone, a toxic chemical in tobacco tar, to induce dryAMD-like symptoms in mice over atwo-week course of exposure. Concurrent treatment with 3 mg/kg subcutaneous elamipretide during hydroquinone exposure protected against these symptoms, as evidenced by a reduction of the drusen-like deposit formation and maintenance of normal membrane thickness, mitochondrial morphology and ultrastructure of the retinal pigment endothelium cells in treated mice.
In another preclinical model of a24-month old Alzheimer’s disease mouse (roughly equivalent to a human octogenarian) which, when fed a high fat diet, accumulated drusen-like deposits, one month of subcutaneous administration of elamipretide eliminated the drusen-like deposits and restored normal mitochondrial morphology and the ultrastructure of the retinal pigment endothelium cells. In addition, the animals treated with elamipretide were observed to have normalization ofb-wave amplitudes on electroretinograms, which suggests an improvement in photoreceptor function reflecting improved visual acuity.
We conducted our ReCLAIM Phase 1 open-label clinical trial at Duke Eye Center to evaluate the safety, tolerability and efficacy of daily subcutaneous injections of 40 mg elamipretide given over 24 weeks to 40 individuals with intermediate characteristics of dry AMD. We enrolled 21 subjects who have high-risk drusen, the most common early signs of dry AMD, and 19 subjects who havenon-central geographic atrophy, or areas of dysfunctional macula. Individuals with high-risk drusen typically have difficulty seeing in low light conditions and mild to moderate deficits in visual acuity under normal light condition, while those withnon-central geographic atrophy have more advanced symptoms but are not yet blind. The primary endpoint was safety and tolerability, evaluated based on review of adverse events, or AEs, and compliance of self-administration of subcutaneous elamipretide, measured at 24 weeks compared to baseline. Secondary endpoints for both high-risk drusen subjects and subjects withnon-central geographic atrophy included change from baseline in visual acuity in low light conditions, or low luminance visual acuity, or LLVA, a five-letter deficit in which was required for inclusion in the trial, visual acuity in standard light conditions, BCVA, reading speed and acuity in low light conditions and standard light conditions, drusen volume and patient reported outcome assessments. Assessments for most secondary endpoints occurred at baseline, week four, week eight, week 12 and week 16.
We analyzed the data for subjects in each cohort who completed 24 weeks of therapy, which included 19 subjects with high-risk drusen and 15 subjects withnon-central geographic atrophy. We observed improvements in functional assessments across both cohorts, as summarized below. As noted above, a five-letter deficit in LLVA, which is among the first clinical symptoms of the disease, was a required inclusion criterion for the trial, and improvements in this
119
Table of Contents
endpoint were statistically significant across both the drusen (p=0.0055) and geographic atrophy (p=0.0186) cohorts.
ENDPOINT | DRUSEN COHORT (N=19) | GEOGRAPHIC ATROPHY COHORT (N=15) | ||
Best corrected visual acuity (regular light) mean letters gained/p value | 3.58 | 4.60 | ||
| (p=0.0253) | (p=0.0034) | |||
Low luminance visual acuity mean letters gained/p value | 5.63 | 5.40 | ||
| (p=0.0055) | (p=0.0186) | |||
Reading speed (regular light) mean reduction in time/p value | -0.11 | -0.02 | ||
| (p=0.0054) | (p=0.5501) | |||
Low luminance reading speed mean reduction in time/p value | -0.28 | -0.52 | ||
| (p<0.0001) | p=0.0172 | |||
Visual function questionnaire composite score | 9.25 | 6.59 | ||
| (p=0.0004) | (p=0.0125) | |||
Low luminance questionnaire general dim light vision score | 20.75 | 10.32 | ||
| (p=0.0003) | (p=0.027) |
Since we did not have a placebo, or control group, in this study, we evaluated natural history data and prior placebo-controlled trials of subjects with similar disease burden to understand the likelihood that we would observe a learning or placebo effect in this study. In a number of other reported interventional studies conducted by others, including Chroma, Spectri and Filly (combined n>700), as well as in several natural history studies conducted by others, including Proxima, Holz and Ladd (combined n>250), BCVA was observed to decline in similar patient groups by four to six letters over an up toone-year period, and LLVA was observed to decline in similar patient groups by approximately two letters over asix-month toone-year period. This supports our belief that the improvements observed in the ReCLAIM trial are unlikely to be due to the natural variability of the disease.
While each subject in ReCLAIM had one eye designated as a study eye, which met the inclusion criteria for the trial, the other eye was not required to meet inclusion criteria. Fourteen subjects in the trial had neovascularage-related macular degeneration, or wet AMD, that was at the quiescent stage, meaning that it was stable onstandard-of-care anti-vascular endothelial growth factor, or anti-vegF, therapy. While there is an improvement in visual acuity when some subjects are first dosed with anti-vegF therapy, improvement typically plateaus and even declines slightly when the disease reaches the quiescent state. We observed that subjects with wet AMD experienced similar improvements in vision as was observed in the study eyes, with a 5.6 letter mean gain from baseline in BCVA, which was statistically significant at p=0.0027, and a 6.1 letter mean gain from baseline in LLVA, which was statistically significant at p=0.0012.
We also assessed the rate of progression of geographic atrophy in thenon-central geographic atrophy cohort relative to what has been observed in other studies. The typical rate of geographic atrophy progression in dry AMD iswell-understood from prior studies and the natural history, and we believe slowing of geographic atrophy progression could be a meaningful endpoint as we pursue approval by the FDA. This analysis was conducted using several types of imaging technologies including fundus auto- fluorescence, or FAF, an advanced imaging technique for observing the fundus, which is the interior surface of the eye opposite the lens including the retina, optic disk, macula, fovea and posterior pole, FAF squared, or FAF SQRT, a calculation performed to eliminate dependence of growth rates on lesion measurements, and optical coherence tomography, or OCT, anon-invasive imaging test which uses light waves to take cross-sectional pictures of the retina, also squared, or OCT SQRT, to eliminate dependence of growth rates on lesion measurements. Each of these imaging technologies showed that six months’ treatment with elamipretide was associated with slower progression of geographic atrophy than was observed in prior published studies conducted by others (assuming, for prior studies which were completed over a longer time period, a linear progression of geographic atrophy enabling calculation at the6-month time point). FAF demonstrated mean growth of 0.50 mm2, versus 0.91 mm2 mean observation from ten prior studies over a similar time period (assuming linear progression), FAF SQRT demonstrated mean growth of 0.14 mm, versus 0.19 mm mean observation from five prior studies over a
120
Table of Contents
similar time period (assuming linear progression), and OCT SQRT demonstrated mean growth of 0.11 mm, versus 0.18 mm mean observation from five prior published studies over a similar time period (assuming linear progression).
We plan to initiate ReCLAIM 2, a Phase 2b placebo-controlled clinical trial with once daily subcutaneous dosing in subjects withnon-central geographic atrophy during the first quarter of 2019. ReCLAIM 2 is designed to enroll up to 180 subjects, of whom 120 will be treated with an elamipretide 40 mg once daily subcutaneous injection, and the remainder will receive placebo for a 48-week period. Eligible subjects are required to have a geographic atrophy area greater than or equal to 0.05mm2 and less than 10.16 mm2, BCVA greater than or equal to 55 letters and greater than 5 letters low luminance deficit. Efficacy endpoints in ReCLAIM 2 include BCVA, FAF, OCT, low-luminance best-corrected visual acuity, low-luminance reading acuity, National Eye Institute Visual Function Questionnaire-39 score, visual function by the Low-luminance Questionnaire and conversion to choroidal neovascularization.
Although we believe that individuals experiencing a progressive decline in visual activity will be compliant with daily subcutaneous injections, we may consider a second Phase 2b placebo-controlled clinical trial using the drop formulation because it may be commercially advantageous to utilize a topical drop formulation. We observed signs of clinical benefit with elamipretide topical ophthalmic drops in our ReVEAL Phase 1/2 clinical trial enrolling subjects with Fuchs’ corneal endothelial dystrophy, or Fuchs, as well as in our ReSIGHT trial, and we are continuing to assess open-label efficacy data from our ReSIGHT study to inform the decision whether to pursue further development of the drop formulation.
Fuchs’ corneal endothelial dystrophy
Fuchs’ affects the endothelium, the thin layer of cells that line the back part of the cornea in the front of the eye. Endothelial cells are key to pumping excess water from the cornea, where it otherwise accumulates and results in corneal damage and cell death. When endothelial cells die, they cannot be regenerated. As more cells are lost, fluid builds up in the cornea and the tissue gradually thickens, resulting in a swollen and cloudy cornea. Fuchs’ is thought to be caused by oxidative stress in the endothelial cells, which in turn causes mtDNA damage and leads to morphological changes in the cells of the corneal epithelium. There are nonon-surgical therapies approved for Fuchs’. In 2016, there were an estimated 28,000 corneal transplants in the United States for treatment of Fuchs’.
Our ReVEAL Phase 1/2 clinical trial was a randomized, double-masked, vehicle-controlled,two-part trial, with two separate12-week treatment periods measuring two doses of elamipretide, intended to enroll 27 subjects at two sites in the United States. We completed the first part of ReVEAL, in which 16 individuals diagnosed with Fuchs’ and experiencing mild to moderate corneal edema received elamipretide 1.0% ophthalmic solution twice daily for up to 12 weeks in a randomly selected eye and a single drop of placebo twice daily to the control eye. We were unable to identify sufficient subjects to meet the enrollment criteria for the second part, in which an intended eight subjects were to receive elamipretide 3.0% ophthalmic solution twice daily in both eyes for up to 12 weeks, and three patients were to receive a single drop of placebo twice daily to each eye. We terminated the study early due to these enrollment challenges, enrolling only four of the intended 11 subjects in the second part.
In the fully enrolled, completed first part of the ReVEAL study, we observed significant differences in the primary efficacy endpoint of interest, which was central corneal thickness, in elamipretide-treated subjects relative to placebo-treated subjects (p=0.0293). This suggests that elamipretide may have reduced the degree of edema, or swelling, which contributes to corneal damage and endothelial cell death in this disease. We will evaluate this data in the context of our ongoing development of elamipretide forage-related diseases, but we do not currently plan to continue development of elamipretide for Fuchs based on our evaluation of the market potential in this indication.
Elamipretide Safety Data
We have a significant amount of clinical trial data indicating that elamipretide is generally well tolerated. As of September 30, 2018, 22 clinical trials had been completed with single and multiple intravenous and subcutaneous administrations of elamipretide at dose levels ranging from approximately 0.7 mg/day to 300 mg/day. These included 14 clinical pharmacology studies enrolling approximately 276 healthy subjects in which the primary objective was to assess safety rather than to treat a disease state, and 10 clinical trials enrolling approximately 498 subjects across multiple patient populations, including subjects with primary mitochondrial myopathy, skeletal muscle mitochondrial dysfunction, stable chronic heart failure, acute coronary syndrome and acute kidney injury. Additionally, data from two open-label clinical trials with the subcutaneous formulation in 49 subjects with primary mitochondrial myopathy and 40 subjects with dry AMD are available.
121
Table of Contents
The following table summarizes, by dosing duration, the meaningful differences in systemic treatment-emergent adverse events reported in elamipretide-treated subjects versus placebo-treated subjects. For this purpose, we considered a difference of at least 2% to be meaningful. In addition, injection site reactions were reported in the majority of subjects receiving elamipretide by subcutaneous injection; most commonly these entailed mild redness, swelling and itchiness which usually resolved within four hours of dosing.
SUMMARY OF SYSTEMIC TREATMENT EMERGENT ADVERSE EVENTS (TEAEs) REPORTED IN GREATER FREQUENCY (³ 2% DIFFERENCE) IN ELAMIPRETIDE-TREATED SUBJECTS COMPARED TO PLACEBO-TREATED SUBJECTS | ||||||||||
| ELAMIPRETIDE | PLACEBO | DISCUSSION | ||||||||
Single Dose | n=356 | n=220 | ||||||||
Headache | 4.5 | % | 2.3 | % | ||||||
Repeat dose£8 days | n=186 | n=46 | ||||||||
Dizziness | 2.2 | % | 0.0 | % | ||||||
Repeat dose > 8 days (TEAEs³ 5%) | n=70 | n=30 | ||||||||
Increased eosinophils/eosinophilia | 48.6 | % | 0.0 | % | Mild to moderate increase in eosinophils, a variety of white blood cells that combat parasites and infections and control mechanisms associated with allergy and asthma, were observed in longer-term dosing regimens, with no associated clinical signs and symptoms. These appear to decrease to within normal limits with longer duration of elamipretide administration and return topre-treatment levels after the end of elamipretide treatment. | |||||
Upper respiratory tract infection | 15.7 | % | — | All 10 events of upper respiratory tract infection occurred in one open-label trial in an elderly population where there was no placebo-control group. | ||||||
Increased blood immunoglobulin E | 10.0 | % | 0.0 | % | No associated clinical signs and symptoms. | |||||
Dizziness | 8.6 | % | 1.4 | % | ||||||
Headache | 8.6 | % | 2.9 | % | ||||||
Urinary tract infection | 7.1 | % | 0.0 | % | ||||||
Viral gastroenteritis | 5.7 | % | 0.0 | % | ||||||
We have completed three clinical trials with topical ophthalmic elamipretide: ReSIGHT for the treatment of LHON, ReVEAL for the treatment of Fuchs’, and ReVIEW for the treatment of either diabetic macular edema, or DME, or dry AMD. In the ReSIGHT clinical trial, 12 subjects were treated with 1.0% ophthalmic solution twice daily for 52 weeks. There were no discontinuations in the ReSIGHT clinical trial. Ocular related TEAEs were reported in 56.3% of the elamipretide-treated and half of the placebo-treated eyes. In our ReVEAL clinical trial, 22 subjects were enrolled in one of two dosing cohorts, 1.0% ophthalmic solution or 3.0% ophthalmic solution, administered in the eye twice daily for 12 weeks. In this trial, there were two discontinuations, one of which was due to failure to meet inclusion criteria and one of which was due to a reported allergic reaction. Two unrelated systemic TEAEs were reported. In the 3.0% dose arm, two subjects reported ocular TEAEs of itching, foggy vision, redness and/or allergic conjunctivitis that led to discontinuation, each of which was deemed likely related to study drug. In the REVIEW clinical trial, 20 subjects were enrolled in one of two dosing cohorts, 0.3% ophthalmic solution or 1.0% ophthalmic solution, administered to one eye twice daily for 28 days. A total of four TEAEs were reported in the ReVIEW clinical trial and none were considered related to elamipretide by the investigator. There were no local tolerability issues reported, and there were no significant findings on physical examinations, ophthalmic examinations, vital signs or laboratory measurements.
122
Table of Contents
Earlier Clinical Trials of Elamipretide
We have studied elamipretide in clinical trials in several diseases associated with aging, including studies enrolling subjects with reduced skeletal muscle mitochondrial function, subjects with heart failure with reduced ejection fraction, or HFrEF, subjects with heart failure with preserved ejection fraction, or HFpEF, subjects undergoing percutaneous transluminal renal angioplasty and subjects with acute coronary syndrome. These trials were designed as smallproof-of-concept studies to inform our decision whether to progress later stage development in these indications, and as such were generally not well-powered to achieve statistical significance. Although we have decided not to independently progress development of elamipretide for these common disease indications, we saw signs of clinical benefit from treatment with elamipretide in several of these indications, which may help inform our future development of pipeline compounds forage-related diseases.
In April 2010, we submitted an investigational new drug application, or IND, to the FDA for purposes of conducting clinical trials of elamipretide for the prevention and treatment of ischemia reperfusion injury. In October 2014, we submitted an IND to the FDA for the purpose of conducting clinical trials of elamipretide for the treatment of primary mitochondrial myopathy. Although this IND was also intended to cover our Barth clinical trial, when the FDA granted Fast-Track Status to this program they recommended we file a new IND covering Barth, which we have done. Additionally, in October 2014, we submitted an IND for purposes of conducting clinical trials of elamipretide for the treatment of diabetic macular edema and dry AMD; this IND also covers our clinical trials of Fuchs’ and LHON. The initial study under this IND was a Phase 1/2 safety study in 15 patients with diabetic macular edema and 5 patients with dry AMD, in which elamipretide topical ophthalmic drops at concentrations of 0.3% and 1% were well-tolerated over four weeks of dosing. We were the sponsor for each of those INDs.
MOTION—reduced skeletal muscle mitochondrial function.Our Phase 2 MOTION clinical trial was a double-blind, placebo-controlled trial involving 38 elderly subjects with reduced mitochondrial function in the thenar muscle group, between the thumb and pointer finger, as measured by nuclear magnetic resonance technology, or P31 NMR, a magnet that can measure phosphorous peaks as it associates andde-associates with adenosine, a purine nucleoside found in every human cell, during the oxidative phosphorylation process. Subjects were randomizedone-to-one to a singletwo-hour IV of 0.25 mg/kg elamipretide or placebo. We measured the maximum capacity of the mitochondria to produce ATPin vivo using P31 NMR on the infusion day and seven days post- infusion. A sustained hand fatigue test determined the effect of increasing ATPmax on exercise tolerance.
Although ourpre-specified analysis did not show a statistically significant benefit in this population, our investigator conducted apost-hoc sensitivity analysis excluding one subject in the placebo group whose ATPmax value was believe to be an erroneous measurement that did not meet the quality control criteria. Thepost-hoc analysis excluding this subject showed that two hours after the start of a single IV, elamipretide-treated subjects experienced a 30% improvement in ATPmax compared to a 12.5% improvement in the placebo-treated subjects (p=0.0555). This improvement was reduced to near baseline levels seven days following treatment. The increase in ATPmax was statistically significantly correlated with functional improvement measured by force time integral (p=0.0041), a test of muscle endurance, two hours after the start of the infusion, with mean increases approximately two to four times greater in subjects treated with elamipretide compared to placebo. This post hoc finding suggests that increasing skeletal muscle mitochondrial capacity may increase skeletal muscle function.
PREVIEW-HF—heart failure.PREVIEW-HF was a Phase 1/2 randomized, double-blind, placebo-controlled, single ascending dose trial of elamipretide in 36 subjects aged 45 to 80 years with stable Class 2/3 chronic heart failure, or mild to moderate symptoms of heart failure, who were receiving concomitant standard of care pharmacologic therapy. The trial evaluated the safety, tolerability, pharmacokinetics, pharmacodynamics and the effect on heart function assessed by serial two dimensional echocardiograms of a single four-hour IV of elamipretide (0.005 mg/kg/hour, or low dose (n=8), 0.05 mg/kg/hr, ormid-dose (n=8), 0.25 mg/kg/hour, or high-dose (n=8)) or placebo (n=12). We observed that the highest dose of elamipretide significantly reduced mean left ventricularend-systolic volume (absolute change from baseline-11 mL versus 2.8 mL for placebo; mean difference =-13.7 mL; p=0.005) and mean left ventricularend-diastolic volume (absolute change from baseline-15 mL versus 2.9 mL for placebo; mean difference =-17.9 mL; p=0.009) at the end of a four- hour infusion. Volume measurements such asend-systolic volume andend-diastolic volume are viewed as the best predictor of an improvement in morbidity and mortality in heart failure subjects.
123
Table of Contents
We also observed that, as compared to subjects in the placebo cohort, subjects in the high-dose arm had reduced left atrial volume at all time points, as well as an increase in right ventricular fractional area change at all time points. Finally, right-ventricular systolic pressure appeared to be reduced at most time points in both the medium and high-dose elamipretide-treated subjects, as compared to placebo. We also observed reductions in urinary8-OH-2-deoxyguanosine and urinary8-isoprostane, production of both of which is well-documented to increase in direct proportion to oxidative stress, six hours after the start of a four-hour infusion of elamipretide.
PROGRESS-HF—heart failure with reduced ejection fraction.PROGRESS-HF was a Phase 2 randomized, double-blind, placebo-controlled trial, involving 71 subjects with Stage C heart failure with reduced ejection fraction, or HFrEF, randomized to receive28-days of once daily subcutaneous injections of 4mg elamipretide (low dose) (n=23) or 40mg elamipretide (high dose) (n=24) or placebo (n=24) injections. The trial evaluated the safety, tolerability, pharmacokinetics, pharmacodynamics and the effect on heart function of elamipretide assessed by cardiac magnetic resonance imaging, or MRI. The trial did not meet its primary efficacy endpoints of change from baseline in left ventricular ejection fraction and change from baseline in left ventricular end systolic volume, both assessed by cardiac MRI.NT-proBNP levels appeared to be consistently reduced in the elamipretide-treated subjects that received 40mg versus the placebo-treated group, an effect that appeared to be more pronounced in the subgroup where theNT-proBNP levels were highest at baseline. Although these values did not reach statistical significance, it may be suggestive of preferential benefit for more impaired subjects.
IDDEA-HF—acute heart failure with reduced ejection fraction.IDDEA-HF was a Phase 2 randomized, double-blind, placebo-controlled trial, involving 308 subjects with acute decompensated heart failure, which affects patients with advanced heart failure with HFrEF and is associated with severe congestion of multiple organs by fluid that is inadequately circulated by the failing heart. Subjects were randomized to receive 20 mg elamipretide in normal saline or placebo, dosed once daily over seven days by intravenous administration.
The trial evaluated the safety, tolerability, pharmacokinetics, pharmacodynamics and the effect on heart function of elamipretide assessed byNT-pro-BNP, a marker in the blood for brain natriuretic peptide, or BNP, which is a biomarker of cardiac function. AlthoughNT-pro-BNP levels were significantly reduced from baseline in the elamipretide treated group (p<0.0001), when adjusted for reductions from baseline in the placebo treated group the change was not significant and so the trial did not meet its primary efficacy endpoint. We observed trends toward improvement in biomarkers of kidney function in patients who received elamipretide relative to placebo, and we also observed that fewer patients who received elamipretide relative to placebo died or were readmitted to the hospital during the 40-day follow-up period.
ReSTORE-HF—heart failure with preserved ejection fraction.ReSTORE-HF was a Phase 2 randomized, double-blind, placebo-controlled trial, involving 47 subjects ranging between 45 and 80 years of age presenting with symptomatic heart failure with preserved ejection fraction, or HFpEF, randomized to receive 28 days of once daily subcutaneous injections of 40 mg elamipretide or placebo.
The trial evaluated the safety, tolerability, pharmacokinetics, pharmacodynamics and the effect on heart function of elamipretide assessed by echocardiogram. AlthoughReSTORE-HF failed to meet its primary efficacy endpoint of change in left ventricular filling pressures at rest (placebo adjusted change of(-1.13) favored elamipretide, but failed to meet statistical significance (p=0.31)), trends favoring elamipretide were observed across various endpoints, particularly on assessments conducted during sub maximal exercise when clinical symptoms most commonly present in this patient population. A key secondary endpoint of change in left ventricular filling pressures during submaximal exercise improved(-2.44; p=0.09) ), as did the change during submaximal stress in left ventricular systolic global longitudinal strain(-3.63; p=0.09). Notably, left ventricular end systolic volume, an important functional parameter in this disease in which the heart is not filling to its full potential, also improved (p=0.06).
EVOLVE—percutaneous transluminal renal angioplasty.EVOLVE was a Phase 2a randomized, double-blind, placebo-controlled trial, involving 14 subjectspre-treated with elamipretide or placebo prior to undergoing percutaneous transluminal renal angioplasty. We initiated EVOLVE in January 2013. In January 2014, the CORAL trial, a947-subject clinical trial sponsored by the Baim Institute for Clinical Research, concluded that renal-artery stenting did not confer a significant benefit with respect to the prevention of clinical events when added to comprehensive,
124
Table of Contents
multifactorial medical therapy in people with atherosclerotic renal-artery stenosis and hypertension or chronic kidney disease. This made recruitment in our EVOLVE trial challenging, and we terminated the trial in 2016 after enrolling only 14 of the anticipated 28 subjects. Although the primary endpoint of improvement in glomerular filtration rate assessed by iothalamate clearance did not show statistical significance when comparing elamipretide- and placebo-treated subjects, possibly because the trial was underpowered due to early termination, treatment with elamipretide was suggestive of other beneficial effects.
Subjects who received elamipretide were protected from a temporary lack of oxygen to kidney tissue, known as transient hypoxia. In contrast, subjects in the placebo group developed hypoxia 24 hours after the procedure (p<0.05). We observed a statistically significant improvement in kidney blood flow at three-months post procedure (261 mL/min ± 115.0 as compared to baseline 202 mL/min ± 129.0; p<0.05), and a statistically significant improvement in cortical perfusion at three-months post procedure (2.9 mL/ min/tissue ± 1.04 at three months as compared to 1.99 mL/min/tissue ± 0.8 at baseline; p<0.05) in the elamipretide-treated group, as opposed to the placebo-controlled group where differences from baseline were not statistically significant for kidney blood flow at three months post procedure (234 mL/min ± 133.0 as compared to baseline 234 mL/min ± 99.0; p<0.05) or for cortical perfusion at three- months post procedure (2.66 mL/min/tissue ± 0.9 at three months as compared to 2.4 mL/min/tissue ± 0.4 at baseline; p<0.05). These results suggest a potential renal protective effect of elamipretide.
EMBRACE—acute coronary syndrome.EMBRACE was a Phase 2 double-blind placebo- controlled trial evaluating elamipretide in subjects with acute coronary syndrome. EMBRACE failed to meet its primary efficacy endpoint, intended to determine whether elamipretide could protect the heart from muscle damage that can occur when a previously blocked vessel is opened abruptly, as determined by measuringcreatine-kinase-MB, orCK-MB, area under the curve, AUC, a cardiac marker of variants of the enzyme phosphocreatine kinase which is used to assist diagnoses of an acute myocardial infarction. AlthoughCK-MB AUC in elamipretide-treated subjects was lower than placebo (6582 ng.h/mL versus 6738 ng.h/mL for placebo), this difference did not achieve statistical significance in thepre-specified primary analysis population of 118 subjects. We believe that, due to a higher than anticipated exclusion rate in our primary analysis population attributable to absence of complete arterial blockage in 179 of the 297 subjects enrolled, EMBRACE was not properly powered to achieve statistical significance on the primary endpoint in the treatment population. It is also possible that, given the exigency of interventional treatment in this patient population, around which there is ongoing debate regarding clinically appropriate speed of intervention relative to pretreatment modalities, it was challenging to implement theper-protocol timelines between dosing with elamipretide and intervention in a clinical setting.
SBT-20
Our second product candidate,SBT-20, is a small peptide that also targets and binds reversibly to cardiolipin, stabilizing mitochondrial structure and function under conditions of oxidative stress.SBT-20 has been generally well-tolerated in 75 people exposed to it systemically as of December 31, 2018. We plan to evaluateSBT-20 for rare peripheral neuropathies.
Based on preclinical studies, we believe thatSBT-20 readily penetrates cell membranes and targets and binds reversibly to the inner membrane of mitochondria.
125
Table of Contents
SBT-20 has been observed to protect the normal morphology of the mitochondria from injury in a preclinical ischemic reperfusion model. In a preclinical study of rats treated withSBT-20 or placebo prior to occlusion and reperfusion of renal blood flow, published in theAmerican Journal of Physiology—Renal Physiologyin October 2014, researchers at Weill Cornell Medical College observed thatSBT-20 preserved normal mitochondrial structure and function, including mitochondrial density, mitochondrial matrix density, mitochondrial respiration and ATP levels. In the images below, the left shows kidney mitochondria prior to the insult, the center shows kidney mitochondria of the placebo-treated animals post-insult and the right shows kidney mitochondria of theSBT-20-treated animals post-insult.
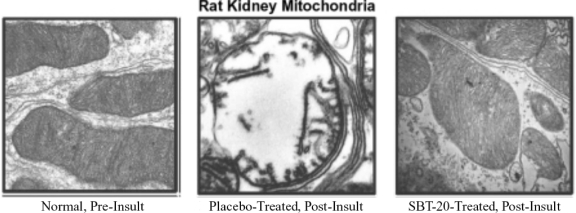
We plan to evaluateSBT-20 for rare diseases entailing mitochondrial dysfunction, including rare peripheral neuropathies associated with mitochondrial dysfunction. Mitochondrial dysfunction is thought to be involved in peripheral neuropathies including chemotherapy-induced peripheral neuropathy, neuropathies associated with mitochondrial myopathy, neuropathy, and gastrointestinal encephalopathy, or MNGIE, and both the axonal and demyelinating forms of Charcot-Marie-Tooth disease, or CMT, the most common inherited neuromuscular disorder.
SBT-20 was observed to have a protective effect against the development of chemotherapy-induced peripheral neuropathy in a mouse model, in which the mitotoxic effects of cancer chemotherapeutic agents are believed to contribute to dysregulation of primary afferent sensory neurons resulting in pain. In an experiment in which nine mice were treated withSBT-20 5 mg/kg/day, 10 mice were treated withSBT-20 10 mg/kg/day (the high dose cohort) and six mice were treated with vehicle, or normal saline, for two days prior to and for a three-week period during which oxaliplatin, a mitotoxic chemotherapy agent, was administered once-weekly,SBT-20 treated mice in the high dose cohort exhibited significantly decreased neuropathic pain measured by paw sensitivity to mechanical stimuli (p=0.009 relative to vehicle) and cold stimuli (p<0.001 relative to vehicle). Additionally, the loss of intraepidermal nerve fibers in the hind paw was observed to be significantly reduced inSBT-20 treated mice in the high dose cohort (p=0.006 relative to vehicle).
We expect to initiate preclinical studies in animal models of CMT during the first half of 2019, with data expected byyear-end, which will inform our further development plans for this indication.
SBT-20 Clinical Data
We have conducted two clinical safety studies ofSBT-20, one of which, ourCHALLENGE-HD trial, was a Phase 1/2 clinical trial for the treatment of subjects with early stage Huntington’s, and the other of which was a Phase 1 clinical trial involving healthy volunteers.
CHALLENGE-HD was a Phase 1/2 double-blind, placebo-controlled, multiple ascending dose trial evaluating the safety, tolerability and efficacy of daily subcutaneous injections ofSBT-20 compared to placebo in 24 subjects with early stage Huntington’s. Subjects were randomized six toSBT-20 compared to two to placebo in three dose cohorts of 5mg, 15mg and 25mgSBT-20 for an initial seven days during part one of the study. Subjects were subsequently randomized on a double-blindone-to-one basis to 25mgSBT-20 or placebo administered by subcutaneous injection once daily over afollow-on four-week course of treatment, or part two of the study. One subject who received placebo in part one of the study was randomized to receive SBT-20 in part two of the study. The primary endpoints of the
126
Table of Contents
trial was safety and tolerability; the secondary objectives included efficacy assessments including improvements in mitochondrial membrane potential, a standard battery of neurological assessments and assessment of function of brain mitochondria by magnetic resonance spectroscopy. In part one of the study, we observed an improvement in mitochondrial membrane potential in the 25mg, or high dose, cohort relative to placebo (p=0.0356). An improvement in mitochondrial membrane potential was also observed in part two of the study. However, this did not reach statistical significance relative to placebo (p=0.1693).
In addition to ourCHALLENGE-HD trial, we completed a Phase 1 clinical trial ofSBT-20 in healthy volunteers. In this trial, 24 healthy adults were exposed to single subcutaneous doses ofSBT-20 and 32 healthy adults were exposed to multiple subcutaneous doses ofSBT-20, ranging from 5 mg to 30 mg. In the single ascending dose portion of the trial, the incidence of AEs increased slightly with dose; however, there was no apparent dose-related trend in the multiple ascending dose portion of the trial. Injection site reactions, such as erythema, swelling, itching, or pain, were the most frequently reported AEs. No subject experienced injection site reactions that were assessed as severe with one exception, which was also reported as clinically significant, although there were eight clinically significant injection site reactions reported as moderate experienced in six subjects.
We did not observe any clinically significant findings in any laboratory assessments, vital signs or ECGs. Although not clinically significant, we did observe a mean increase in liver enzymes alanine aminotranferease, or ALT, in five of eight subjects, and/or aspartate aminotransferase, or AST, in three of eight subjects, in each case from baseline to day eight (after seven days of dosing) in subjects administeredSBT-20 at the highest dose of 30 mg per day. Three of the subjects with elevated ALT had greater than two times baseline at day eight, and two had 1.5 times baseline at day eight. Although two of eight subjects still had ALT levels above the reference range at thefollow-up visits, these values were trending toward baseline levels. Two of the subjects with elevated AST had greater than two times baseline at day eight and one had approximately 1.5 times baseline at day eight. Three of five subjects with increased AST levels on day eight demonstrated a return towards baseline at thefollow-up assessment. We did not observe increased ALT or AST levels in the 5, 10 or 20 mg/day dose cohorts in this study. We did not observe increased ALT levels in nonclinical toxicology studies.
Discovery Compounds
We have an active discovery and development program focused on novel compounds targeting mitochondria. Mitochondria have been an extremely challenging therapeutic target, due in part to difficulty in targeting delivery of drugs to mitochondria. Successful delivery requires traversing not only the cell membrane, which may have reduced membrane potential in disease states, but also achieving intracellular diffusion/transport to mitochondria and subsequent electrical potential across outer and IMM. We believe the differentiated mitochondrial targeting characteristics of our compounds, our development of proprietary assays to screen new compounds for mitochondrial targeting and activity characteristics, and our experience working with various models of mitochondrial dysfunction position us to lead next generation development of mitochondrial product candidates that are improved relative to elamipretide andSBT-20.
We have developed multiple series of novel compounds with improved pharmacokinetic properties. These include over 100 different compounds, including peptidomimetics, small molecules and novel peptides, that we are actively screening to broaden our existing mitochondrial product candidate portfolio. We are focused on producing agents with mitochondrial therapeutic potential with improved properties over our first-generation compounds, by altering the rate and extent of absorption, thebio-distribution and the routes of metabolism and excretion.
SBT-272
SBT-272, our lead pipeline compound, is among our novel peptides and peptidomimetics, which target the mitochondria and potentially improve mitochondrial function relative to our current product candidates as observed in early experiments. For example,SBT-272 and an analog have shown signs of biological activity in a rat model of kidney reperfusion injury, in which elamipretide, SBT-272, an analog of SBT-272 or vehicle is administered to a rat, the renal artery is clamped, restricting blood flow, and then released, permitting blood to flow back into the kidney. As illustrated below, treatment with SB-272 or its analog compounds resulted in greater reduction in plasma creatinine and blood urea nitrogen, biomarkers of kidney dysfunction, than treatment with vehicle or treatment with
127
Table of Contents
elamipretide. In the graph below, the sham columns represent rats that were not subjected to kidney reperfusion injury and not treated with any of the four alternatives.
Protection from acute ischemia reperfusion kidney injury in rats
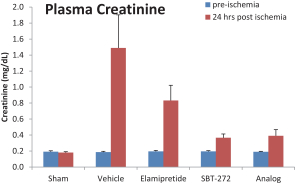 | 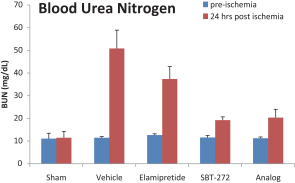 |
SBT-272 has shown greater than six times higher mitochondrial uptake relative to elamipretide in cell-based assays of isolated mitochondria, and has also demonstrated improved oral bioavailability in early animal studies, suggesting it may be a promising candidate for oral dosing.SBT-272 has demonstrated approximately three times greater maximum concentration, or Cmax, in the brain of rats relative to elamipretide, in each case dosed 10 mg/kg subcutaneously.SBT-272 has demonstrated more than 25 times greater area under the drug concentration-time curve in the brain of rats relative to elamipretide, in each case dosed 10 mg/kg subcutaneously, suggesting significantly higher brain exposure and residence time.
We have commenced preclinical toxicology studies, orIND-enabling studies, withSBT-272 in preparation for filing an IND application in 2019. Subject to FDA review, this would enable us to commence Phase 1 clinical trials in healthy volunteers by the end of 2019.
SBT-20 has shown signs of benefit in a mouse model of Parkinson’s disease. Based onSBT-272’s preferential concentration and residence time in the cerebrospinal fluid we are evaluatingSBT-272 for neurodegenerative indications characterized by mitochondrial dysfunction. Increasing evidence suggests that mitochondria are involved inage-related neurodegenerative diseases, including Alzheimer’s disease and Parkinson’s disease, as well as ALS.Age-related, mitochondrial-generated ROS is postulated to be one factor in the development and progression oflate-onset neurodegenerative diseases. Moreover, mitochondrial dysfunction is a common cellular change observed during the disease process in inherited neurodegenerative diseases, including Parkinson’s, in which mtDNA mutations are implicated as a factor, and Huntington’s. We have initiated preclinical studies in an ALS animal model and expect to receive data in the first half of 2019 to inform our further development plans for this indication.
Carrier program
We have also conducted experiments in our carrier program in which we observed that we can use our proprietary compounds as vectors or carriers to selectively deliver various therapeutic payloads to the mitochondria, conferring organelle specificity to promising therapies. Many individuals diagnosed with primary mitochondrial disease, for which there are no therapies approved by the FDA, take aso-called “mito cocktail” of vitamins and supplements, usually in high doses and comprising up to 50 pills per day if not compounded. These may typically includeco-enzymeQ-10, or CoQ-10, or its analogs,L-carnitine, B vitamins and antioxidants. The reason these are taken in such high doses is because delivery to the mitochondria is likely confounded by permeability challenges traversing the cell and outer mitochondrial membranes. By contrast, we have observed mitochondrial targeting capabilities of our proprietary compounds, and have also observed that we can conjugate payloads to our compounds and direct the conjoined carrier/payload to the mitochondria.
For example, idebenone is a CoQ-10 analog that introduces electrons into the electron transport chain downstream of complexes I and II, a promising mechanism for bypassing defective complexes in genetic diseases. Because idebenone is poorly absorbed and does not specifically target mitochondria, it has demonstrated limited pharmacologic activity even at high doses. Preliminary preclinicaldata shows that our idebenone-conjugated peptide
128
Table of Contents
was effective at stimulating complex III enzyme activity at a concentration of approximately 100 times lower than standard idebenone. We believe this is promising data supporting the potential of our carrier program, and we are actively evaluating other mitochondrial beneficial payloads for evaluation in this program.
Manufacturing
We do not have any manufacturing facilities. We currently rely, and expect to continue to rely, on third parties for the manufacture of our product candidates for preclinical studies and clinical trials, as well as for commercial manufacture if our product candidates receive marketing approval. We have also obtained key raw materials for elamipretide andSBT-20 from third-party manufacturers. For both elamipretide andSBT-20, we intend to identify and qualify a single manufacturer to provide the active pharmaceutical ingredient andfill-and-finish services prior to submission of an NDA to the FDA. This allows us to reduce the risk to NDA approval by preparing only one manufacturing site for active pharmaceutical ingredient and one for drug product forpre-approval inspections. We can sufficiently reduce the supply risk usually associated with a single source of product based on our capability to buildpre-launch inventory and the relatively small demand for material projected for our rare disease indications.
All of our product candidates are small molecules and are manufactured in reliable and reproducible synthetic processes from readily available starting materials. The chemistry is amenable to scale up and does not require unusual equipment in the manufacturing process. Elamipretide has been produced historically by a solid-phase manufacturing process that has been commonly used to produce commercial peptides. Due to a lack of scalability, we deemed this process undesirable for production of commercial quantities of elamipretide. A new solution-phase process for producing elamipretide as a hydrochloride, or HCI, salt has been developed and implemented at a contract manufacturing site at a scale sufficient for supply of near-term clinical trials. The new process for manufacturing is proprietary to us, and the equipment and the unit operations used in the process are not unique to any particular contract manufacturer. We have transferred this process to contract manufacturing sites capable of using such processes to manufacture large quantities of similar drug substances, and we are now producing drug supply for pivotal clinical trials and progressing toward commercial production. Manufacturing at a higher production scale has led to a significant reduction in ourcost-of-goods and provided us with the ability to respond to any need to supply large clinical trials or unanticipated commercial demand in the future. Following FDA review of test results demonstrating the same/similar identity, quality, purity and strength of product from the two processes, the FDA has stated that non-clinical and clinical trials with drug substance from the former process can be used to support further development and registration of elamipretide. As a result, we have filed the newly developed process with regulatory authorities and introduced drug substance batches from that process into our clinical trials.
We have active clinical programs for which our CMOs are routinely manufacturing a sterile solution product for subcutaneous injection or intravenous infusion and a solution product for topical administration to the eye. Our CMOs have successfully produced these products on a scale of tens of thousands of units and shown, using validated stability-indicating methods, that these products would meet specifications over a shelf-life typical of commercial products. We believe we are well-positioned to validate our manufacturing processes at one or more CMOs and support a commercial launch of these products. We have successfully filed regulatory applications to supplymulti-use cartridges and pens for subcutaneous self-administration in our Phase 3 clinical trial for primary mitochondrial myopathy. We believe, based on these clinical cartridge and pen injector designs, that we can commercialize similar products successfully.
Intellectual Property
We strive to protect the proprietary technologies that we believe are important to our business, including seeking and maintaining patent protection intended to cover our lead product candidates, elamipretide andSBT-20, and related compositions, our core clinical applications and otherknow-how, to operate without infringing on the proprietary rights of others and to prevent others from infringing our proprietary or intellectual property rights worldwide. Our patent portfolio, which includes patents and patent applications that we own, as well as those that we have exclusivelyin-licensed, is structured to provide layers of protection for the proprietary technologies central to our business. Our portfolio includes claims to the elamipretide andSBT-20 peptides, compositions comprising the same, and use of the peptides for our core clinical applications. As of December 31, 2018, the patent portfolio included 374 granted patents (38 U.S., 336 foreign, which include individual national patents based on granted
129
Table of Contents
European patents) and 298 pending applications, including provisional applications (79 U.S., 214 foreign, five Patent Cooperation Treaty).
We also rely on trade secret protection, technical knowledge, and continuing technological innovation to develop and maintain our proprietary and intellectual property position. We seek to protect our proprietary information, in part, using confidentiality agreements with our collaborators, scientific advisors, employees and consultants, and invention assignment agreements with our employees.
We also have agreements with selected consultants, scientific advisors and collaborators requiring assignment of inventions or, in limited cases, the grant of an exclusive, worldwide license or option to license intellectual property rights developed in the course of their work with or for us. As with other biotechnology and pharmaceutical companies, our capacity to obtain, maintain and protect our proprietary and intellectual property positions for our products and technologies depends on our continued ability to obtain relevant patent rights and to enforce those patent rights, if necessary. However, patent applications that we may file or license from third parties may not necessarily result in the grant of rights. We also cannot predict the scope of rights that may be granted to us in the future, our desire or ability to seek enforcement of any granted rights, or the willingness of courts or other administrative bodies to uphold or enforce our rights.
In addition, any currently issued patents or any future patents, should they issue, may be challenged, invalidated, or circumvented, such as through district court proceedings or inter partes review. For example, we cannot be certain of the priority of inventions covered by pending third-party patent applications, and proceedings to establish our rights could result in substantial costs, even if the eventual outcome is favorable. Due to the extensive time required for clinical development and regulatory review, it is possible that, before any of our product candidates can be commercialized, any related patent may expire or its term may have substantially run, leaving its remaining term in force for only a short period following commercialization. To the extent that occurs, the possible commercial advantage conferred by such patents would be reduced. Accordingly, we have attempted to design a patent portfolio with both breadth and depth of potential protection, with the goal of maximizing coverage for elamipretide and related peptides and their uses in commercially relevant countries.
Elamipretide
Patent rights relating to elamipretide peptide and compositions comprising elamipretide have been granted in Australia, Canada, China, Europe, Hong Kong, Japan and the United States. The U.S. patent has an adjusted statutory expiration date in 2026, which includes 717 days of patent term adjustment, or PTA, granted by the USPTO upon issue of the patent. The foreign patents have a statutory expiration date in 2024. We hold an exclusive license to these rights from Cornell and the IRCM.
Patent rights to the use of elamipretide as a carrier for the transport of therapeutic molecules into a cell as well as related compositions have been granted or allowed in Australia, Canada, China, Europe, Hong Kong, Japan, the United States and six other countries. The U.S. patent has an adjusted statutory expiration date in 2027, which includes 1,215 days of PTA granted by the USPTO upon issue of the patent. The foreign patents have a statutory expiration date in 2024. We hold an exclusive license to these patent rights from Cornell.
Patent rights related to compositions including elamipretide and a second therapeutic compound have also been granted. For example, claims directed to elamipretide-cyclosporine conjugates have been granted in the United States and are pending in Europe. The U.S. patent has a statutory expiration date in 2031, and any patent that may issue from the pending European application will similarly have a statutory expiration date in 2031. Each of these patent rights are owned exclusively by us. Additional patent rights related to compositions including elamipretide and glucagon-likepeptide-1 are pending in applications filed in Canada, China, Europe, Japan and the United States and, if granted, these will have statutory expiration dates in 2033.
Patents directed to methods of treating or preventing various diseases and medical conditions by administering elamipretide have been granted to us, or have beenin-licensed by us, in a number of countries. Where possible, the scope of granted claims has been tailored to provide broad generic support encompassing a wide range of conditions as well as specific disease states. By way of example, there are granted patents related to the use of elamipretide to treat basic, adverse cellular events that contribute to disease, such as mitochondrial permeability transition (MPT), and oxidative damage associated with a neurodegenerative disease.
130
Table of Contents
Patents related to MPT have been granted in Australia, Canada, China, Europe, Hong Kong, Japan and the United States. The U.S. patent has an adjusted statutory expiration date in 2026, and is the same patent referred to above as covering the composition of elamipretide. The foreign patents have statutory expiration dates in 2024. We hold exclusive rights to these patents by way of a license agreement with Cornell and the IRCM.
Our patent portfolio also protects or aims to protect the use of elamipretide to treat or prevent specific clinical indications. By way of example, our portfolio includes granted claims drawn to the use of elamipretide to treat diabetes, metabolic syndrome, renal diseases, certain cardiovascular diseases, ocular diseases, and neurodegenerative diseases (including Alzheimer’s disease, Huntington’s disease and ALS) that are in patents owned by us orin-licensed to us. Claims relating to the use of elamipretide to treat Barth, LHON, primary mitochondrial myopathy and mitochondrial diseases associated with certain gene mutations are pending in applications owned by us.
SBT-20
Claims drawn to theSBT-20 peptide and compositions comprising theSBT-20 peptide have been granted in Australia, Canada, Japan and the United States, and are pending in Europe. Claims drawn to a composition comprisingSBT-20 together with a cargo molecule are granted in China. The U.S. patent has an adjusted statutory expiration date in 2026, which includes 717 days of PTA granted by the USPTO upon issue of the patent, and is the same patent described above as related to elamipretide peptide. The foreign patents have statutory expiration dates in 2024. We hold exclusive rights to the patents and applications by way of an exclusive agreement with either Cornell alone or Cornell in conjunction with the IRCM.
Patent rights directed to the use of theSBT-20 peptide as a carrier for the transport of therapeutic molecules into cells, as well as related compositions, have been granted or allowed in Australia, Canada, China, Europe, Hong Kong, Japan, the United States and six other countries. The U.S. patent has an adjusted statutory expiration date in 2027, which includes 1,215 days of PTA granted by the USPTO upon issue of the patent, and is the same patent described above as related to the use of elamipretide as a carrier. The foreign patents have a statutory expiration date in 2024. We hold exclusive rights to these patents by way of our license agreements with Cornell and the IRCM.
Patent rights related to compositions comprisingSBT-20-cyclosporine conjugates have been granted in the United States and are pending in Europe. The U.S. patent has a statutory expiration date in 2031, and any patent that may issue from the pending European application will similarly have a statutory expiration date in 2031. Each of these patent rights are owned exclusively by us.
Our patent portfolio also protects or aims to protect the use ofSBT-20 to treat or prevent specific clinical indications. By way of example, our portfolio includes granted claims drawn to the use ofSBT-20 to treat complications of diabetes, renal diseases, ocular diseases, and neurodegenerative diseases that are owned by us orin-licensed. Claims relating to the use ofSBT-20 to treat Parkinson’s disease, Alzheimer’s disease, Huntington’s, and ALS are granted in Australia, in a patentin-licensed to us with a statutory expiration date in 2024.
We hold patent rights to additional pipeline compounds in the portfolio, and are continuing to expand coverage in the United States and commercially relevant foreign jurisdictions. Subject matter for new filings is expected to include, but will not necessarily be limited to, the use of peptides to treat additional disease indications, new combination therapies, new peptide formulations, new compositions and uses of the same.
The term of a patent depends upon the legal length of the term of patents in the jurisdiction in which it is issued. In most countries in which we file, the patent term is 20 years from the earliest date of filing of anon-provisional patent application. Patent term adjustment is a process of extending the term of a United States patent beyond the 20 year statutory patent term to accommodate for delays caused by the USPTO during prosecution. By contrast, a patentee or applicant may file a terminal disclaimer which disclaims or dedicates to the public the entire term or any terminal part of the term of a patent or patent to be granted.
In the United States, the term of a patent that covers anFDA-approved drug may also be eligible for patent term extension, which permits patent term restoration as compensation for the patent term lost during the FDA regulatory review process. The Hatch-Waxman Act permits a patent term extension of up to five years beyond the regularly scheduled expiration of a patent. The length of the patent term extension is related to the length of time the drug is
131
Table of Contents
under regulatory review. Patent extension cannot extend the remaining term of a patent beyond a total of 14 years from the date of product approval by the FDA, only one patent applicable to an approved drug may be extended, and a given patent can only be extended based on one approved drug. Similar provisions are available in Europe and certain other jurisdictions to extend the term of a patent that covers an approved drug. We anticipate that we will apply for patent term extensions for relevant U.S. patents, if and when our pharmaceutical products receive FDA approval. We also anticipate seeking patent term extensions for issued patents in any jurisdiction where patent term extension is available, however, there is no guarantee that the applicable authorities, including the FDA in the United States, will agree with our assessment of whether such extensions should be granted, and if granted, the length of such extensions. Unless specifically indicated, the above statutory patent terms refer to the20-year base statutory term and do not include any patent term adjustment or extension that may be available in any jurisdiction.
Cornell License Agreements
We have entered into several license agreements with Cornell and the IRCM, pursuant to which Cornell granted us specified exclusive, worldwiderights under patents related to elamipretide,SBT-20, and other technology described below, which we refer to collectively as the licensed patents. The original Cornell agreement was entered into in with Cornell and the IRCM in April 2006, and subsequently amended in October 2010. Concurrent with our execution of the original Cornell agreement, we entered into a sponsored research agreement with Cornell in which we agreed to fund specified research at Cornell for three years. We retained the right to license inventions arising under such sponsored research agreement, as well as certain material transfer agreement entered into between us and Cornell, through entry into license agreements on substantially the same terms as the original Cornell agreement. Such subsequent agreements under which we obtained rights under additional patent families, which we refer to as other Cornell license agreements, and collectively with the original Cornell agreement as the Cornell license agreements, were entered into in November 2010, November 2011, December 2012 and August 2013. In each of the Cornell license agreements, Cornell granted us an exclusive, worldwide license under specified patents and patent application families claiming certain inventions, including inventions related to elamipretide,SBT-20, certain other peptides and/or specified uses of the foregoing, which we refer to collectively as the licensed patents, to make, use, sell, lease, import, export or otherwise dispose of products or services that incorporate, utilize or are otherwise described and claimedin the licensed patents, which we refer to as the licensed products, in any and all fields. Our rights under the Cornell license agreements are subject to the rights of the United States government and other applicable restrictions imposed by the Bayh-Dole Act and its implementing regulations, and the rights of Cornell, and in some cases certain other specified institutions, to practice the inventions claimed in the licensed patents for educational and research purposes.
We have agreed to use best efforts (as defined in each of the Cornell license agreements) to commercialize licensed products, and to achieve specified diligence milestones by specified target dates. We are also required to periodically set forth additional milestones until first commercial sale of a specified licensed product. We believe that to date we have met each diligence milestone with respect to our licensed products and the specific licensed indications and/or formulations which we are developing. If however we fail in the future to meet any diligence milestone within a specified period after the corresponding target date, our exclusive license under the applicable Cornell license agreement will convert to anon-exclusive license and, in the case of the original Cornell agreement, such conversion will occur only with respect to the peptide, indication and/or formulation that is subject of the unachieved milestone.
In connection with the licenses granted under the original Cornell agreement, we issued Cornell 666,667 ordinary shares and Cornell agreed to provide us with a right of first refusal in the event Cornell sought to sell its equity position at any time prior to an initial public offering. With respect to the other Cornell license agreements, we paid Cornell upfront license fees of $55,000 and royalties on net sales, if any, by us and our sublicensees of any licensed product, on aproduct-by-product andcountry-by-country basis. Subject to specified reductions and royalty offsets, such royalties are calculated as a tiered,low-to-mid single digit percentage of net sales of licensed products under each of the Cornell license agreements, except that for licensed products under the original Cornell agreement, such royalties are calculated as a tiered, low single-digit tosub-teen percentage of net sales, depending on patent coverage, amount of net sales and type of licensed product. Our obligation to pay royalties as to any licensed product extends until the later of the expiration of thelast-to-expire valid claim of any licensed patent covering such licensed product or 15 years after the date of our first commercial sale of such licensed product. If a licensed product is covered by licenses granted under the original Cornell agreement and another Cornell license agreement, then, for each unit of product, royalties will only be due under the original Cornell agreement.
132
Table of Contents
We are obligated to pay Cornell a low double-digit percentage of specified payments we receive in connection with granting a sublicense under the Cornell license agreements. We have also agreed to reimburse Cornell for itsout-of-pocket expenses incurred in preparing, filing, prosecuting and maintaining the licensed patents, except for any licensed patents as to which we elect to waive our licensed rights. We also have agreed to pay Cornell annual license maintenance fees in themid-five-digits for the original Cornell agreement, and mid four-digits for each of the other Cornell license agreements starting on a date specified in each such agreement, in all cases until the first commercial sale of a specified type of licensed product under such agreement.
If Cornell identifies any licensed product that we are not actively developing or commercializing and we do not elect within a specified period to develop or commercialize such licensed product ourselves or through a sublicensee, or, if we do so elect, we do not then agree on reasonable diligence goals with Cornell or enter into an agreement with such a sublicensee within specified periods as to such licensed product, then Cornell may terminate our rights under the applicable Cornell license agreement for such licensed product.
Unless earlier terminated, each of the Cornell license agreements will remain in effect until the expiration or invalidation of the last of all licensed patents and as long as no licensed patent applications remain pending. Cornell (together with the IRCM in the case of the original Cornell agreement) can terminate a Cornell license agreement if we are in material breach of such license agreement or if we intentionally provide false reports, or if we are in default in our payment obligations, and fail to cure such breach, false report or default within a specified period. In addition, Cornell can terminate the original Cornell agreement and certain of the other Cornell license agreements if we fail to achieve first commercial sale of a therapeutic licensed product by the date specified in the respective agreement (which, with respect to the original Cornell agreement, is December 31, 2020); however, there are a number of exceptions to Cornell’s termination right, including:
| ∎ | delays due to clinical development, including clinical trial enrollment challenges or data read outs; |
| ∎ | delays due to regulatory matters; or |
| ∎ | delays due to other events over which we cannot exert direct control. |
We can terminate any of the Cornell license agreements in its entirety or on apatent-by-patent, licensedproduct-by-licensed product orcountry-by-country basis if we have a reasonable basis for doing so by giving Cornell a specified number of days’ prior notice. We can transfer each of the Cornell license agreements with Cornell’s prior written approval (not to be unreasonably withheld) in the event of a sale of the Company, sale of assets or sale of shares, provided that such sale is not primarily for the benefit of creditors. If we fail to obtain Cornell’s prior written approval for such transfer, Cornell can terminate the respective agreement and require that the transfer of such agreement be voided. We cannot assign the Cornell license agreements without Cornell’s (and in the case of the original Cornell agreement, IRCM’s) written consent.
Competition
The biotechnology and pharmaceutical industries are characterized by rapidly advancing technologies, intense competition and a strong emphasis on proprietary products. While we believe that our technology, knowledge, experience and scientific resources provide us with competitive advantages, we face potential competition from many different sources, including major pharmaceutical, specialty pharmaceutical and biotechnology companies, academic institutions and governmental agencies and public and private research institutions. Any product candidates that we successfully develop and commercialize will compete with existing therapies and new therapies that may become available in the future.
We are initially developing elamipretide for the treatment of rare primary mitochondrial diseases and common diseases of aging in which mitochondrial function is impaired. There are several companies developing treatments that target mitochondria or mitochondria-associated diseases. The majority of these efforts are in preclinical development, are focused on gene therapy or are proposing the use of generic compounds. To our knowledge, none of these are focused on cardiolipin remodeling. Our competitors include NeuroVive Pharmaceutical AB, Reata Pharmaceuticals, Inc., BioElectron Technology Corporation (formerly Edison Pharmaceuticals Inc.), LumiThera, Inc. and Santhera Pharmaceuticals Holding. In addition to competition from competitors who are developing treatments that seek to improve mitochondrial function or otherwise target the mitochondria, we also face competition from
133
Table of Contents
therapies that target the indications we are studying, particularly for diseases of aging such as dry AMD. Such competitors who are developing or who have developed competing therapies include Allegro Ophthalmics, LLC, Apellis Pharmaceuticals, Astellas Pharma Inc., Hemera Biosciences Inc., Ionis Pharmaceuticals, Inc. and Ophthotech Corporation.
Many of the companies against which we are competing or against which we may compete in the future may have significantly greater financial resources and expertise in research and development, manufacturing, preclinical testing, conducting clinical trials, obtaining regulatory approvals and marketing approved products than we do. Mergers and acquisitions in the pharmaceutical, biotechnology and diagnostic industries may result in even more resources being concentrated among a smaller number of our competitors. Smaller or early stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies. These competitors also compete with us in recruiting and retaining qualified scientific and management personnel and establishing clinical trial sites and patient registration for clinical trials, as well as in acquiring technologies complementary to, or necessary for, our programs.
The key competitive factors affecting the success of all of our therapeutic product candidates, if approved, are likely to be their efficacy, safety, tolerability, convenience and price and the availability of reimbursement from government and other third-party payors.
Our commercial opportunity could be reduced or eliminated if our competitors develop and commercialize products that are safer, more effective, have fewer or less severe side effects, are more convenient or are less expensive than any products that we may develop. Our competitors also may obtain FDA or other regulatory approval for their products more rapidly than we may obtain approval for ours, which could result in our competitors establishing a strong market position before we are able to enter the market.
Government Regulation and Product Approvals
Government authorities in the United States, at the federal, state and local level, and in other countries and jurisdictions, including the European Union, extensively regulate, among other things, the research, development, testing, manufacture, pricing, quality control, approval, packaging, storage, recordkeeping, labeling, advertising, promotion, distribution, marketing, post-approval monitoring and reporting, and import and export of biopharmaceutical products. The processes for obtaining marketing approvals in the United States and in foreign countries and jurisdictions, along with compliance with applicable statutes and regulations and other regulatory authorities, require the expenditure of substantial time and financial resources.
In the United States, the FDA regulates drugs under the Federal Food, Drug, and Cosmetic Act, or FDCA, and associated implementing regulations. The failure to comply with the FDCA and other applicable U.S. requirements at any time during the product development process, approval process or after approval may subject an applicant and/or sponsor to a variety of administrative or judicial sanctions, including refusal by the FDA to approve pending applications, withdrawal of an approval, imposition of a clinical hold, issuance of warning letters and other types of letters, product recalls, product seizures, total or partial suspension of production or distribution, injunctions, fines, refusals of government contracts, restitution, disgorgement of profits, or civil or criminal investigations and penalties brought by the FDA and the Department of Justice, or DOJ, or other governmental entities.
An applicant seeking approval to market and distribute a new drug product in the United States must typically undertake the following:
| ∎ | completion of preclinical laboratory tests, animal studies and formulation studies in compliance with the FDA’s good laboratory practice, or GLP, regulations; |
| ∎ | submission to the FDA of an IND, which must take effect before human clinical trials may begin in the United States; |
| ∎ | approval by an independent institutional review board, or IRB, representing each clinical site before each clinical trial may be initiated; |
| ∎ | performance of adequate and well-controlled human clinical trials in accordance with good clinical practices, or GCP, to establish the safety and efficacy of the proposed drug product for each indication; |
134
Table of Contents
| ∎ | preparation and submission to the FDA of an NDA; |
| ∎ | review of the product candidate by an FDA advisory committee, where appropriate or if applicable; |
| ∎ | satisfactory completion of one or more FDA inspections of the manufacturing facility or facilities at which the product, or components thereof, are produced to assess compliance with current Good Manufacturing Practices, or cGMP, requirements and to assure that the facilities, methods and controls are adequate to preserve the product’s identity, strength, quality and purity; |
| ∎ | satisfactory completion of FDA audits of clinical trial sites to assure compliance with GCPs and the integrity of the clinical data; |
| ∎ | payment of user fees and securing FDA approval of the NDA; and |
| ∎ | compliance with any post-approval requirements, including Risk Evaluation and Mitigation Strategies, or REMS, where applicable, and post-approval studies required by the FDA. |
Preclinical Studies
Preclinical studies include laboratory evaluation of the purity and stability of the manufactured drug substance or active pharmaceutical ingredient and the formulated drug or drug product, as well as in vitro and animal studies to assess the safety and activity of the drug for initial testing in humans and to establish a rationale for therapeutic use. The conduct of preclinical studies is subject to federal regulations and requirements, including GLP regulations. The results of the preclinical tests, together with manufacturing information, analytical data, any available clinical data or literature and plans for clinical trials, among other things, are submitted to the FDA as part of an IND. Additional preclinical testing, such as animal tests of reproductive adverse events and carcinogenicity, may continue after the IND is submitted.
Human Clinical Trials in Support of an NDA
Clinical trials involve the administration of the investigational product to human subjects under the supervision of qualified investigators in accordance with GCP requirements, which include, among other things, the requirement that all research subjects provide their informed consent in writing before their participation in any clinical trial. Clinical trials are conducted under written study protocols detailing, among other things, the objectives of the trial, inclusion and exclusion criteria, the parameters to be used in monitoring safety and the effectiveness criteria to be evaluated. A protocol for each clinical trial and any subsequent protocol amendments must be submitted to the FDA as part of the IND. An IND automatically becomes effective 30 days after receipt by the FDA, unless before that time the FDA raises concerns or questions related to a proposed clinical trial and places the trial on clinical hold. In such a case, the IND sponsor and the FDA must resolve any outstanding concerns before the clinical trial can begin.
In addition to the foregoing IND requirements, an IRB representing each institution participating in the clinical trial must review and approve the plan for any clinical trial before it commences at that institution, and the IRB must conduct continuing review and reapprove the study at least annually. The IRB must review and approve, among other things, the study protocol and informed consent information to be provided to study subjects. An IRB must operate in compliance with FDA regulations. Information about certain clinical trials must be submitted within specific timeframes to the National Institutes of Health for public dissemination on their ClinicalTrials.gov website.
Human clinical trials are typically conducted in three sequential phases, which may overlap or be combined:
| ∎ | Phase 1: The drug is initially introduced into healthy human subjects or patients with the target disease (e.g., cancer) or condition and tested for safety, dosage tolerance, absorption, metabolism, distribution, excretion and, if possible, to gain an early indication of its effectiveness and to determine optimal dosage. |
| ∎ | Phase 2: The drug is administered to a limited patient population to identify possible adverse effects and safety risks, to preliminarily evaluate the efficacy of the product for specific targeted diseases and to determine dosage tolerance and optimal dosage. |
| ∎ | Phase 3: The drug is administered to an expanded patient population, generally at geographically dispersed clinical trial sites, in well-controlled clinical trials to generate enough data to statistically evaluate the efficacy and safety of the product for approval, to establish the overall risk-benefit profile of the product, and to provide adequate information for the labeling of the product. |
| ∎ | Phase 4. Post-approval studies may be conducted after initial marketing approval. These studies are used to gain additional experience from the treatment of patients in the intended therapeutic indication. |
135
Table of Contents
Progress reports detailing the results of the clinical trials must be submitted at least annually to the FDA and more frequently if serious adverse events occur. In addition, IND safety reports must be submitted to the FDA for any of the following: serious and unexpected suspected adverse reactions; findings from other studies or animal or in vitro testing that suggest a significant risk in humans exposed to the drug; and any clinically important increase in the case of a serious suspected adverse reaction over that listed in the protocol or investigator brochure. Phase 1, Phase 2 and Phase 3 clinical trials may not be completed successfully within any specified period, or at all. Furthermore, the FDA or the sponsor or the data monitoring committee may suspend or terminate a clinical trial at any time on various grounds, including a finding that the research subjects are being exposed to an unacceptable health risk. Similarly, an IRB can suspend or terminate approval of a clinical trial at its institution, or an institution it represents, if the clinical trial is not being conducted in accordance with the IRB’s requirements or if the drug has been associated with unexpected serious harm to patients. The FDA will typically inspect one or more clinical sites to assure compliance with GCP and the integrity of the clinical data submitted.
In general, the FDA accepts foreign safety and efficacy studies that were not conducted under an IND provided that they are well designed, well conducted, performed by qualified investigators, and conducted in accordance with ethical principles acceptable to the world community. The conduct of these studies must meet at least minimum standards for assuring human subject protection. Therefore, for studies submitted in support of an NDA that were conducted outside the United States and not under an IND, the agency requires demonstration that such studies were conducted in accordance with GCP.
Submission of an NDA to the FDA
Assuming successful completion of required clinical testing and other requirements, the results of the preclinical studies and clinical trials, together with detailed information relating to the product’s chemistry, manufacture, controls and proposed labeling, among other things, are submitted to the FDA as part of an NDA requesting approval to market the drug product for one or more indications. Under federal law, the submission of most NDAs is additionally subject to an application user fee and the sponsor of an approved NDA is also subject to annual program user fees. Certain exceptions and waivers are available for some of these fees, such as an exception from the application fee for drugs with orphan designation.
The FDA conducts a preliminary review of an NDA within 60 calendar days of its receipt and strives to inform the sponsor by the 74th day after the FDA’s receipt of the submission to determine whether the application is sufficiently complete to permit substantive review. The FDA may request additional information rather than accepting an NDA for filing. In this event, the application must be resubmitted with the additional information. The resubmitted application is also subject to review before the FDA accepts it for filing. Once the submission is accepted for filing, the FDA begins anin-depth substantive review.
The FDA has agreed to specified performance goals in the review process of NDAs. Under that agreement, 90% of applications seeking approval of New Molecular Entities, or NMEs, are meant to be reviewed within ten months from the date on which FDA accepts the NDA for filing, and 90% of applications for NMEs that have been designated for “priority review” are meant to be reviewed within six months of the filing date. For applications seeking approval of drugs that are not NMEs, theten-month andsix-month review periods run from the date that FDA receives the application. The review process may be extended by the FDA for three additional months to consider new information or clarification provided by the applicant to address an outstanding deficiency identified by the FDA following the original submission.
Before approving an NDA, the FDA typically will inspect the facility or facilities where the product is or will be manufactured. Thesepre-approval inspections cover all facilities associated with an NDA submission, including drug component manufacturing (such as active pharmaceutical ingredients), finished drug product manufacturing and control testing laboratories. The FDA will not approve an application unless it determines that the manufacturing processes and facilities are in compliance with cGMP requirements and adequate to assure consistent production of the product within required specifications. Additionally, before approving an NDA, the FDA will typically inspect one or more clinical sites to assure compliance with GCP.
In addition, as a condition of approval, the FDA may require an applicant to develop a REMS. REMS use risk minimization strategies beyond the professional labeling to ensure that the benefits of the product outweigh the
136
Table of Contents
potential risks. To determine whether a REMS is needed, the FDA will consider the size of the population likely to use the product, seriousness of the disease, expected benefit of the product, expected duration of treatment, seriousness of known or potential adverse events and whether the product is a new molecular entity. REMS can include medication guides, physician communication plans for healthcare professionals and elements to assure safe use, or ETASU. ETASU may include, but are not limited to, special training or certification for prescribing or dispensing, dispensing only under certain circumstances, special monitoring and the use of patient registries. The FDA may require a REMS before approval or post-approval if it becomes aware of a serious risk associated with use of the product. The requirement for a REMS can materially affect the potential market and profitability of a product.
The FDA is required to refer an application for a novel drug to an advisory committee or explain why such referral was not made. Typically, an advisory committee is a panel of independent experts, including clinicians and other scientific experts, that reviews, evaluates and provides a recommendation as to whether the application should be approved and under what conditions. The FDA is not bound by the recommendations of an advisory committee, but it considers such recommendations carefully when making decisions.
Fast Track, Breakthrough Therapy, Priority Review and Regenerative Advanced Therapy Designations
The FDA is authorized to designate certain products for expedited review if they are intended to address an unmet medical need in the treatment of a serious or life-threatening disease or condition. These programs are Fast Track designation, breakthrough therapy designation, priority review designation and regenerative advanced therapy designation.
Specifically, the FDA may designate a product for Fast Track review if it is intended, whether alone or in combination with one or more other drugs, for the treatment of a serious or life-threatening disease or condition, and it demonstrates the potential to address unmet medical needs for such a disease or condition. For Fast Track products, sponsors may have greater interactions with the FDA and the FDA may initiate review of sections of a Fast Track product’s NDA before the application is complete. This rolling review may be available if the FDA determines, after preliminary evaluation of clinical data submitted by the sponsor, that a Fast Track product may be effective. The sponsor must also provide, and the FDA must approve, a schedule for the submission of the remaining information and the sponsor must pay applicable user fees. However, the FDA’s time period goal for reviewing a Fast Track application does not begin until the last section of the NDA is submitted. In addition, the Fast Track designation may be withdrawn by the FDA if the FDA believes that the designation is no longer supported by data emerging in the clinical trial process.
Second, in 2012, Congress enacted the Food and Drug Administration Safety and Innovation Act, or FDASIA. This law established a new regulatory scheme allowing for expedited review of products designated as “breakthrough therapies.” A product may be designated as a breakthrough therapy if it is intended, either alone or in combination with one or more other drugs, to treat a serious or life-threatening disease or condition and preliminary clinical evidence indicates that the product may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints, such as substantial treatment effects observed early in clinical development. The FDA may take certain actions with respect to breakthrough therapies, including holding meetings with the sponsor throughout the development process; providing timely advice to the product sponsor regarding development and approval; involving more senior staff in the review process; assigning a cross-disciplinary project lead for the review team; and taking other steps to design the clinical trials in an efficient manner.
Third, the FDA may designate a product for priority review if it is a drug that treats a serious condition and, if approved, would provide a significant improvement in safety or effectiveness. The FDA determines, on acase-by-case basis, whether the proposed drug represents a significant improvement when compared with other available therapies. Significant improvement may be illustrated by evidence of increased effectiveness in the treatment of a condition, elimination or substantial reduction of a treatment-limiting drug reaction, documented enhancement of patient compliance that may lead to improvement in serious outcomes and evidence of safety and effectiveness in a new subpopulation. A priority designation is intended to direct overall attention and resources to the evaluation of such applications, and to shorten the FDA’s goal for taking action on a marketing application from ten months to six months.
Finally, with passage of the Cures Act in December 2016, Congress authorized the FDA to accelerate review and approval of products designated as regenerative advanced therapies. A product is eligible for this designation if it is
137
Table of Contents
a regenerative medicine therapy that is intended to treat, modify, reverse or cure a serious or life-threatening disease or condition and preliminary clinical evidence indicates that the drug has the potential to address unmet medical needs for such disease or condition. The benefits of a regenerative advanced therapy designation include early interactions with FDA to expedite development and review, benefits available to breakthrough therapies, potential eligibility for priority review and accelerated approval based on surrogate or intermediate endpoints.
Accelerated Approval Pathway
The FDA may grant accelerated approval to a drug for a serious or life-threatening condition that provides meaningful therapeutic advantage to patients over existing treatments based upon a determination that the drug has an effect on a surrogate endpoint that is reasonably likely to predict clinical benefit. The FDA may also grant accelerated approval for such a condition when the product has an effect on an intermediate clinical endpoint that can be measured earlier than an effect on irreversible morbidity or mortality and that is reasonably likely to predict an effect on irreversible morbidity or mortality or other clinical benefit, taking into account the severity, rarity or prevalence of the condition and the availability or lack of alternative treatments. Drugs granted accelerated approval must meet the same statutory standards for safety and effectiveness as those granted traditional approval.
For the purposes of accelerated approval, a surrogate endpoint is a marker, such as a laboratory measurement, radiographic image, physical sign, or other measure that is thought to predict clinical benefit, but is not itself a measure of clinical benefit. Surrogate endpoints can often be measured more easily or more rapidly than clinical endpoints. An intermediate clinical endpoint is a measurement of a therapeutic effect that is considered reasonably likely to predict the clinical benefit of a drug, such as an effect on irreversible morbidity or mortality. The FDA has limited experience with accelerated approvals based on intermediate clinical endpoints, but has indicated that such endpoints generally may support accelerated approval where the therapeutic effect measured by the endpoint is not itself a clinical benefit and basis for traditional approval, if there is a basis for concluding that the therapeutic effect is reasonably likely to predict the ultimate clinical benefit of a drug.
The accelerated approval pathway is most often used in settings in which the course of a disease is long and an extended period of time is required to measure the intended clinical benefit of a drug, even if the effect on the surrogate or intermediate clinical endpoint occurs rapidly. Thus, accelerated approval has been used extensively in the development and approval of drugs for treatment of a variety of cancers in which the goal of therapy is generally to improve survival or decrease morbidity and the duration of the typical disease course requires lengthy and sometimes large trials to demonstrate a clinical or survival benefit.
The accelerated approval pathway is usually contingent on a sponsor’s agreement to conduct, in a diligent manner, additional post-approval confirmatory studies to verify and describe the drug’s clinical benefit. As a result, a drug candidate approved on this basis is subject to rigorous post-marketing compliance requirements, including the completion of Phase 4 or post-approval clinical trials to confirm the effect on the clinical endpoint. Failure to conduct required post-approval studies, or confirm a clinical benefit during post-marketing studies, would allow the FDA to withdraw the drug from the market on an expedited basis. All promotional materials for drug candidates approved under accelerated regulations are subject to prior review by the FDA.
The FDA’s Decision on an NDA
On the basis of the FDA’s evaluation of the NDA and accompanying information, including the results of the inspection of the manufacturing facilities, the FDA may issue an approval letter or a complete response letter. An approval letter authorizes commercial marketing of the product with specific prescribing information for specific indications. A complete response letter generally outlines the deficiencies in the submission and may require substantial additional testing or information in order for the FDA to reconsider the application. If and when those deficiencies have been addressed to the FDA’s satisfaction in a resubmission of the NDA, the FDA will issue an approval letter. The FDA has committed to reviewing such resubmissions in two or six months depending on the type of information included. Even with submission of this additional information, the FDA ultimately may decide that the application does not satisfy the regulatory criteria for approval.
If the FDA approves a product, it may limit the approved indications for use for the product, require that contraindications, warnings or precautions be included in the product labeling, require that post-approval studies, including Phase 4 clinical trials, be conducted to further assess the drug’s safety after approval, require testing and
138
Table of Contents
surveillance programs to monitor the product after commercialization, or impose other conditions, including distribution restrictions or other risk management mechanisms, including REMS, which can materially affect the potential market and profitability of the product. The FDA may prevent or limit further marketing of a product based on the results of post-market studies or surveillance programs. After approval, many types of changes to the approved product, such as adding new indications, manufacturing changes and additional labeling claims, are subject to further testing requirements and FDA review and approval.
Post-Approval Requirements
Drugs manufactured or distributed pursuant to FDA approvals are subject to pervasive and continuing regulation by the FDA, including, among other things, requirements relating to recordkeeping, periodic reporting, product sampling and distribution, advertising and promotion and reporting of adverse experiences with the product. After approval, most changes to the approved product, such as adding new indications or other labeling claims, are subject to prior FDA review and approval. There also are continuing, annual user fee requirements for any marketed products and the establishments at which such products are manufactured, as well as new application fees for supplemental applications with clinical data.
In addition, drug manufacturers and other entities involved in the manufacture and distribution of approved drugs are required to register their establishments with the FDA and state agencies, and are subject to periodic unannounced inspections by the FDA and these state agencies for compliance with cGMP requirements. Changes to the manufacturing process are strictly regulated and often require prior FDA approval before being implemented. FDA regulations also require investigation and correction of any deviations from cGMP and impose reporting and documentation requirements upon the sponsor and any third-party manufacturers that the sponsor may decide to use. Accordingly, manufacturers must continue to expend time, money and effort in the area of production and quality control to maintain cGMP compliance.
Once an approval is granted, the FDA may withdraw the approval if compliance with regulatory requirements and standards is not maintained or if problems occur after the product reaches the market. Later discovery of previously unknown problems with a product, including adverse events of unanticipated severity or frequency, or with manufacturing processes, or failure to comply with regulatory requirements, may result in revisions to the approved labeling to add new safety information; imposition of post-market studies or clinical trials to assess new safety risks; or imposition of distribution or other restrictions under a REMS program. Other potential consequences include, among other things:
| ∎ | restrictions on the marketing or manufacturing of the product, suspension of the approval, complete withdrawal of the product from the market or product recalls; |
| ∎ | fines, warning letters or holds on post-approval clinical trials; |
| ∎ | refusal of the FDA to approve pending NDAs or supplements to approved NDAs, or suspension or revocation of product license approvals; |
| ∎ | product seizure or detention, or refusal to permit the import or export of products; or |
| ∎ | injunctions or the imposition of civil or criminal penalties. |
The FDA strictly regulates marketing, labeling, advertising and promotion of products that are placed on the market. Drugs may be promoted only for the approved indications and in accordance with the provisions of the approved label. The FDA and other agencies actively enforce the laws and regulations prohibiting the promotion ofoff-label uses, and a company that is found to have improperly promotedoff-label uses may be subject to significant liability.
In addition, the distribution of prescription pharmaceutical products is subject to the Prescription Drug Marketing Act, or PDMA, as well as the Drug Supply Chain Security Act, or DSCA, which regulate the distribution and tracing of prescription drugs and prescription drug samples at the federal level, and set minimum standards for the registration and regulation of drug distributors by the states. Both the PDMA and state laws limit the distribution of prescription pharmaceutical product samples and impose requirements to ensure accountability in distribution. The DSCA imposes requirements to ensure accountability in distribution and to identify and remove counterfeit and other illegitimate products from the market.
139
Table of Contents
Abbreviated New Drug Applications for Generic Drugs
In 1984, with passage of the Hatch-Waxman Amendments to the FDCA, Congress authorized the FDA to approve generic drugs that are the same as drugs previously approved by the FDA under the NDA provisions of the statute. To obtain approval of a generic drug, an applicant must submit an abbreviated new drug application, or ANDA, to the agency. In support of such applications, a generic manufacturer may rely on the preclinical and clinical testing previously conducted for a drug product previously approved under an NDA, known as the reference listed drug, or RLD.
Specifically, in order for an ANDA to be approved, the FDA must find that the generic version is identical to the RLD with respect to the active ingredients, the route of administration, the dosage form and the strength of the drug. At the same time, the FDA must also determine that the generic drug is “bioequivalent” to the innovator drug. Under the statute, a generic drug is bioequivalent to a RLD if “the rate and extent of absorption of the drug do not show a significant difference from the rate and extent of absorption of the listed drug.”
Upon approval of an ANDA, the FDA indicates whether the generic product is “therapeutically equivalent” to the RLD in its publication “Approved Drug Products with Therapeutic Equivalence Evaluations,” also referred to as the “Orange Book.” Physicians and pharmacists consider a therapeutic equivalent generic drug to be fully substitutable for the RLD. In addition, by operation of certain state laws and numerous health insurance programs, the FDA’s designation of therapeutic equivalence often results in substitution of the generic drug without the knowledge or consent of either the prescribing physician or patient.
Under the Hatch-Waxman Amendments, the FDA may not approve an ANDA until any applicable period ofnon-patent exclusivity for the RLD has expired. The FDCA provides a period of five years ofnon-patent data exclusivity for a new drug containing a new chemical entity or NCE. An NCE is a drug that contains no active moiety that has previously been approved by the FDA in any other NDA. An active moiety is the molecule or ion responsible for the physiological or pharmacological action of the drug substance. In cases where such exclusivity has been granted, an ANDA may not be filed with the FDA until the expiration of five years unless the submission is accompanied by a Paragraph IV certification, in which case the applicant may submit its application four years following the original product approval. The FDCA also provides for a period of three years of exclusivity if the NDA includes reports of one or more new clinical investigations, other than bioavailability or bioequivalence studies, that were conducted by or for the applicant and are essential to the approval of the application. This three-year exclusivity period often protects changes to a previously approved drug product, such as a new dosage form, route of administration, combination or indication.
Hatch-Waxman Patent Certification and the30-Month Stay
Upon approval of an NDA or a supplement thereto, NDA sponsors are required to list with the FDA each patent with claims that cover the applicant’s product or an approved method of using the product. Each of the patents listed by the NDA sponsor is published in the Orange Book. When an ANDA or 505(b)(2) applicant files its application with the FDA, the applicant is required to certify to the FDA concerning any patents listed for the reference product in the Orange Book, except for patents covering methods of use for which the ANDA applicant is not seeking approval.
Specifically, the ANDA or 505(b)(2) applicant must certify with respect to each patent whether:
| ∎ | the required patent information has not been filed; |
| ∎ | the listed patent has expired; |
| ∎ | the listed patent has not expired, but will expire on a particular date and approval is sought after patent expiration; or |
| ∎ | the listed patent is invalid, unenforceable or will not be infringed by the new product. |
A certification that the new product will not infringe the already approved product’s listed patents or that such patents are invalid or unenforceable is called a Paragraph IV certification. If the applicant does not challenge the listed patents or indicates that it is not seeking approval of a patented method of use, the application will not be approved until all the listed patents claiming the referenced product have expired (other than method of use patents involving indications for which the ANDA applicant is not seeking approval).
140
Table of Contents
If the ANDA or 505(b)(2) applicant has provided a Paragraph IV certification to the FDA, the applicant must also send notice of the Paragraph IV certification to the NDA and patent holders once the ANDA or 505(b)(2) application has been accepted for filing by the FDA. The NDA and patent holders may then initiate a patent infringement lawsuit in response to the notice of the Paragraph IV certification. The filing of a patent infringement lawsuit within 45 days after the receipt of a Paragraph IV certification automatically prevents the FDA from approving the ANDA or 505(b)(2) application until the earlier of 30 months after the receipt of the Paragraph IV notice, expiration of the patent, or a decision in the infringement case that is favorable to the ANDA applicant.
Pediatric Studies and Exclusivity
Under the Pediatric Research Equity Act of 2003, an NDA or supplement thereto must contain data that are adequate to assess the safety and effectiveness of the drug product for the claimed indications in all relevant pediatric subpopulations, and to support dosing and administration for each pediatric subpopulation for which the product is safe and effective. With enactment of the FDASIA in 2012, sponsors must also submit pediatric study plans prior to the assessment data. Those plans must contain an outline of the proposed pediatric study or studies the applicant plans to conduct, including study objectives and design, any deferral or waiver requests, and other information required by regulation. The applicant, the FDA and the FDA’s internal review committee must then review the information submitted, consult with each other, and agree upon a final plan. The FDA or the applicant may request an amendment to the plan at any time.
The FDA may, on its own initiative or at the request of the applicant, grant deferrals for submission of some or all pediatric data until after approval of the product for use in adults, or full or partial waivers from the pediatric data requirements. Additional requirements and procedures relating to deferral requests and requests for extension of deferrals are contained in the FDASIA. Unless otherwise required by regulation, the pediatric data requirements do not apply to products with orphan designation.
Pediatric exclusivity is another type ofnon-patent marketing exclusivity in the United States and, if granted, provides for the attachment of an additional six months of marketing protection to the term of any existing regulatory exclusivity, including thenon-patent and orphan exclusivity. Thissix-month exclusivity may be granted if an NDA sponsor submits pediatric data that fairly respond to a written request from the FDA for such data. The data do not need to show the product to be effective in the pediatric population studied; rather, if the clinical trial is deemed to fairly respond to the FDA’s request, the additional protection is granted. If reports of requested pediatric studies are submitted to and accepted by the FDA within the statutory time limits, whatever statutory or regulatory periods of exclusivity or patent protection cover the product are extended by six months. This is not a patent term extension, but it effectively extends the regulatory period during which the FDA cannot approve another application.
Orphan Drug Designation and Exclusivity
Under the Orphan Drug Act, the FDA may designate a drug product as an “orphan drug” if it is intended to treat a rare disease or condition (generally meaning that it affects fewer than 200,000 individuals in the United States, or more in cases in which there is no reasonable expectation that the cost of developing and making a drug product available in the United States for treatment of the disease or condition will be recovered from sales of the product). A company must request orphan product designation before submitting an NDA. If the request is granted, the FDA will disclose the identity of the therapeutic agent and its potential use. Orphan product designation does not convey any advantage in or shorten the duration of the regulatory review and approval process.
If a product with orphan status receives the first FDA approval for the disease or condition for which it has such designation or for a select indication or use within the rare disease or condition for which it was designated, the product generally will receive orphan product exclusivity. Orphan product exclusivity means that the FDA may not approve any other applications for the same product for the same indication for seven years, except in certain limited circumstances. Competitors may receive approval of different products for the indication for which the orphan product has exclusivity and may obtain approval for the same product but for a different indication. If a drug or drug product designated as an orphan product ultimately receives marketing approval for an indication broader than what was designated in its orphan product application, it may not be entitled to exclusivity.
Patent Term Restoration and Extension
A patent claiming a new drug product may be eligible for a limited patent term extension under the Hatch-Waxman Amendments, which permit a patent restoration of up to five years for patent term lost during product development
141
Table of Contents
and the FDA regulatory review. The restoration period granted is typicallyone-half the time between the effective date of an IND and the submission date of an NDA, plus the time between the submission date of an NDA and the ultimate approval date. Patent term restoration cannot be used to extend the remaining term of a patent past a total of 14 years from the product’s approval date. Only one patent applicable to an approved drug product is eligible for the extension, and the application for the extension must be submitted prior to the expiration of the patent in question. A patent that covers multiple drugs for which approval is sought can only be extended in connection with one of the approvals. The U.S. Patent and Trademark Office reviews and approves the application for any patent term extension or restoration in consultation with the FDA.
Review and Approval of Drug Products in the European Union
In order to market any product outside of the United States, a company must also comply with numerous and varying regulatory requirements of other countries and jurisdictions regarding quality, safety and efficacy and governing, among other things, clinical trials, marketing authorization, commercial sales and distribution of drug products. Whether or not we obtain FDA approval for a product, we would need to obtain the necessary approvals from the comparable foreign regulatory authorities before we can commence clinical trials or marketing of any products in those countries or jurisdictions. The approval process ultimately varies between countries and jurisdictions and can involve additional product testing and additional administrative review periods. The time required to obtain approval in other countries and jurisdictions might differ from and be longer than that required to obtain FDA approval. Regulatory approval in one country or jurisdiction does not ensure regulatory approval in another, but a failure or delay in obtaining regulatory approval in one country or jurisdiction may negatively impact the regulatory process in others.
Clinical Trial Approval in the European Union
Requirements for the conduct of clinical trials in the European Union including Good Clinical Practice, or GCP, are set forth in the Clinical Trials Directive 2001/20/EC and the GCP Directive 2005/28/EC. Pursuant to Directive 2001/20/EC and Directive 2005/28/EC, as amended, a system for the approval of clinical trials in the European Union has been implemented through national legislation of the European Union member states. Under this system, approval must be obtained from the competent national authority of each European Union member state in which a study is planned to be conducted. To this end, a CTA is submitted, which must be supported by an investigational medicinal product dossier, or IMPD, and further supporting information prescribed by Directive 2001/20/EC and Directive 2005/28/EC and other applicable guidance documents. Furthermore, a clinical trial may only be started after a competent ethics committee has issued a favorable opinion on the clinical trial application in that country.
In April 2014, the European Union passed the new Clinical Trials Regulation, (EU) No 536/2014, which will replace the current Clinical Trials Directive 2001/20/EC. To ensure that the rules for clinical trials are identical throughout the European Union, the new European Union clinical trials legislation was passed as a regulation that is directly applicable in all European Union member states. All clinical trials performed in the European Union are required to be conducted in accordance with the Clinical Trials Directive 2001/20/EC until the new Clinical Trials Regulation (EU) No 536/2014 becomes applicable. According to the current plans of EMA, the new Clinical Trials Regulation will become applicable in October 2018. The Clinical Trials Directive 2001/20/EC will, however, still apply three years from the date of entry into application of the Clinical Trials Regulation to (i) clinical trials applications submitted before the entry into application and (ii) clinical trials applications submitted within one year after the entry into application if the sponsor opts for old system.
The new Clinical Trials Regulation aims to simplify and streamline the approval of clinical trial in the European Union. The main characteristics of the regulation include: a streamlined application procedure via a single entry point, the European Union portal; a single set of documents to be prepared and submitted for the application as well as simplified reporting procedures that will spare sponsors from submitting broadly identical information separately to various bodies and different member states; a harmonized procedure for the assessment of applications for clinical trials, which is divided in two parts. Part I is assessed jointly by all member states concerned. Part II is assessed separately by each member state concerned; strictly defined deadlines for the assessment of clinical trial applications; and the involvement of the ethics committees in the assessment procedure in accordance with the national law of the member state concerned but within the overall timelines defined by the Clinical Trials Regulation.
142
Table of Contents
Marketing Authorization in the European Union
To obtain marketing approval of a drug under European Union regulatory systems, an applicant must submit a marketing authorization application, or MAA, either under a centralized or decentralized procedure. The centralized procedure provides for the grant of a single marketing authorization by the European Commission that is valid for all European Union member states. The centralized procedure is compulsory for specific products, including for medicines produced by certain biotechnological processes, products designated as orphan medicinal products, advanced therapy products and products with a new active substance indicated for the treatment of certain diseases. For products with a new active substance indicated for the treatment of other diseases and products that are highly innovative or for which a centralized process is in the interest of patients, the centralized procedure may be optional.
Under the centralized procedure, the Committee for Medicinal Products for Human Use, or the CHMP, established at the EMA, is responsible for conducting the initial assessment of a drug. The CHMP is also responsible for several post-authorization and maintenance activities, such as the assessment of modifications or extensions to an existing marketing authorization. Under the centralized procedure in the European Union, the maximum timeframe for the evaluation of an MAA is 210 days, excluding clock stops, when additional information or written or oral explanation is to be provided by the applicant in response to questions of the CHMP. Accelerated evaluation might be granted by the CHMP in exceptional cases, when a medicinal product is of major interest from the point of view of public health and in particular from the viewpoint of therapeutic innovation. In this circumstance, the EMA ensures that the opinion of the CHMP is given within 150 days.
The decentralized procedure is available to applicants who wish to market a product in various European Union member states where such product has not received marketing approval in any European Union member states before. The decentralized procedure provides for approval by one or more other, or concerned, member states of an assessment of an application performed by one member state designated by the applicant, known as the reference member state. Under this procedure, an applicant submits an application based on identical dossiers and related materials, including a draft summary of product characteristics, and draft labeling and package leaflet, to the reference member state and concerned member states. The reference member state prepares a draft assessment report and drafts of the related materials within 210 days after receipt of a valid application. Within 90 days of receiving the reference member state’s assessment report and related materials, each concerned member state must decide whether to approve the assessment report and related materials.
If a member state cannot approve the assessment report and related materials on the grounds of potential serious risk to public health, the disputed points are subject to a dispute resolution mechanism and may eventually be referred to the European Commission, whose decision is binding on all member states.
Data and Market Exclusivity
In the European Union, NCEs qualify for eight years of data exclusivity upon marketing authorization and an additional two years of market exclusivity. This data exclusivity, if granted, prevents regulatory authorities in the European Union from assessing a generic (abbreviated) application for eight years, after which generic marketing authorization can be submitted but not approved for two years. The overallten-year period will be extended to a maximum of eleven years if, during the first eight years of those ten years, the marketing authorization holder obtains an authorization for one or more new therapeutic indications which, during the scientific evaluation prior to their authorization, are held to bring a significant clinical benefit in comparison with existing therapies. Even if a compound is considered to be an NCE and the sponsor is able to gain the prescribed period of data exclusivity, another company nevertheless could also market another version of the drug if such company can complete a full MAA with a complete human clinical trial database and obtain marketing approval of its product.
Orphan Drug Designation and Exclusivity
Regulation 141/2000 provides that a drug shall be designated as an orphan drug if its sponsor can establish: that the product is intended for the diagnosis, prevention or treatment of a life-threatening or chronically debilitating condition affecting not more than five in ten thousand persons in the European Community when the application is made, or that the product is intended for the diagnosis, prevention or treatment of a life-threatening, seriously debilitating or serious and chronic condition in the European Community and that without incentives it is unlikely that the marketing of the drug in the European Community would generate sufficient return to justify the necessary investment. For either of these conditions, the applicant must demonstrate that there exists no satisfactory method
143
Table of Contents
of diagnosis, prevention or treatment of the condition in question that has been authorized in the European Community or, if such method exists, the drug will be of significant benefit to those affected by that condition.
Regulation 847/2000 sets out criteria and procedures governing designation of orphan drugs in the European Union. Specifically, an application for designation as an orphan product can be made any time prior to the filing of an application for approval to market the product. Marketing authorization for an orphan drug leads to aten-year period of market exclusivity. This period may, however, be reduced to six years if, at the end of the fifth year, it is established that the product no longer meets the criteria for orphan drug designation, for example because the product is sufficiently profitable not to justify market exclusivity. Market exclusivity can be revoked only in very selected cases, such as consent from the marketing authorization holder, inability to supply sufficient quantities of the product, demonstration of “clinically relevant superiority” by a similar medicinal product, or, after a review by the Committee for Orphan Medicinal Products, requested by a member state in the fifth year of the marketing exclusivity period (if the designation criteria are believed to no longer apply). Medicinal products designated as orphan drugs pursuant to Regulation 141/2000 shall be eligible for incentives made available by the European Community and by the member states to support research into, and the development and availability of, orphan drugs.
Brexit and the Regulatory Framework in the United Kingdom
On June 23, 2016, the electorate in the United Kingdom voted in favor of leaving the European Union, commonly referred to as Brexit. On March 29, 2017, the country formally notified the European Union of its intention to withdraw pursuant to Article 50 of the Lisbon Treaty. Since the regulatory framework for pharmaceutical products in the United Kingdom covering quality, safety and efficacy of pharmaceutical products, clinical trials, marketing authorization, commercial sales and distribution of pharmaceutical products is derived from European Union directives and regulations, Brexit could materially impact the future regulatory regime which applies to products and the approval of product candidates in the United Kingdom. It remains to be seen how, if at all, Brexit will impact regulatory requirements for product candidates and products in the United Kingdom.
Pharmaceutical Coverage, Pricing and Reimbursement
Significant uncertainty exists as to the coverage and reimbursement status of products approved by the FDA and other government authorities. Sales of any approved products will depend, in part, on the extent to which the costs of the products will be covered by third-party payors, including government health programs in the United States such as Medicare and Medicaid, commercial health insurers and managed care organizations. The process for determining whether a payor will provide coverage for a product may be separate from the process for setting the price or reimbursement rate that the payor will pay for the product once coverage is approved. Third-party payors are increasingly challenging the prices charged, examining the medical necessity and reviewing the cost-effectiveness of medical products and services and imposing controls to manage costs. Third-party payors may also limit coverage to specific products on an approved list, or formulary, which might not include all of the approved products for a particular indication.
In the United States, no uniform policy of coverage and reimbursement for products exists among third-party payors. Third-party payors often rely upon Medicare coverage policy and payment limitations in setting their reimbursement rates, but also have their own methods and approval process apart from Medicare determinations. Therefore, coverage and reimbursement for products in the United States can differ significantly from payor to payor.
In order to secure coverage and reimbursement for any product that might be approved for sale, a company may need to conduct expensive pharmacoeconomic studies in order to demonstrate the medical necessity and cost-effectiveness of the product. A payor’s decision to provide coverage for a drug product does not imply that an adequate reimbursement rate will be approved. Third-party reimbursement may not be sufficient to maintain price levels high enough to realize an appropriate return on investment in product development.
The containment of healthcare costs also has become a priority of federal, state and foreign governments and the prices of drugs have been a focus in this effort. Governments have shown significant interest in implementing cost-containment programs, including price controls, restrictions on reimbursement and requirements for substitution of generic products. Adoption of price controls and cost-containment measures, and adoption of more restrictive policies in jurisdictions with existing controls and measures, could further limit a company’s revenue generated from
144
Table of Contents
the sale of any approved products. Coverage policies and third-party reimbursement rates may change at any time. Even if favorable coverage and reimbursement status is attained for one or more products for which a company or its collaborators receive marketing approval, less favorable coverage policies and reimbursement rates may be implemented in the future.
In the European Union, pricing and reimbursement schemes vary widely from country to country. Some countries provide that drug products may be marketed only after a reimbursement price has been agreed. Some countries may require the completion of additional studies that compare the cost-effectiveness of a particular drug candidate to currently available therapies, or so called health technology assessments, in order to obtain reimbursement or pricing approval. For example, the European Union provides options for its member states to restrict the range of drug products for which their national health insurance systems provide reimbursement and to control the prices of medicinal products for human use. European Union member states may approve a specific price for a drug product or may instead adopt a system of direct or indirect controls on the profitability of the company placing the drug product on the market. Other member states allow companies to fix their own prices for drug products, but monitor and control company profits.
The downward pressure on health care costs in general, particularly prescription drugs, has become intense and there are high barriers to the entry of new products. In addition, in some countries, cross-border imports fromlow-priced markets exert competitive pressure that may reduce pricing within a country. Any country that has price controls or reimbursement limitations for drug products may not allow favorable reimbursement and pricing arrangements.
Healthcare Law and Regulation
Healthcare providers, physicians and third-party payors play a primary role in the recommendation and prescription of drug products that are granted marketing approval. Arrangements with providers, consultants, third-party payors and customers are subject to broadly applicable fraud and abuse and other healthcare laws and regulations. Such restrictions under applicable federal and state healthcare laws and regulations, include the following:
| ∎ | the federal healthcare Anti-Kickback Statute prohibits, among other things, persons or entities from knowingly and willfully soliciting, offering, receiving or providing remuneration, directly or indirectly, in cash or in kind, to induce or reward either the referral of an individual for, or the purchase, order or recommendation of, any good or service, for which payment may be made, in whole or in part, under a federal healthcare program such as Medicare and Medicaid; |
| ∎ | the federal civil and criminal false claims laws, including the False Claims Act, and civil monetary penalties laws, which provide for civil whistleblower or qui tam actions, prohibit, among other things, individuals or entities from knowingly presenting, or causing to be presented, to the federal government, claims for payment that are false or fraudulent or making a false statement to avoid, decrease or conceal an obligation to pay money to the federal government; |
| ∎ | the federal Health Insurance Portability and Accountability Act of 1996, or HIPAA, imposes criminal and civil liability for, among other things, executing a scheme to defraud any healthcare benefit program or making false statements relating to healthcare matters; |
| ∎ | HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act and their respective implementing regulations, including the Final Omnibus Rule published in January 2013, also imposes obligations, including mandatory contractual terms, with respect to safeguarding the privacy, security and transmission of individually identifiable health information; |
| ∎ | the federal false statements statute prohibits knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false statement in connection with the delivery of or payment for healthcare benefits, items or services; |
| ∎ | the federal transparency requirements under the Affordable Care Act, known as the federal Physician Payments Sunshine Act, require manufacturers of drugs, devices, biologics and medical supplies to report to the Centers for Medicare & Medicaid Services, or CMS, within the Department of Health and Human Services, or HHS, information related to payments and other transfers of value to physicians and teaching hospitals and physician ownership and investment interests held by physicians and their immediate family members; and |
145
Table of Contents
| ∎ | analogous state and foreign laws and regulations, such as state anti-kickback and false claims laws, may apply to sales or marketing arrangements and claims involving healthcare items or services reimbursed bynon-governmental third-party payors, including private insurers. |
Some state laws require pharmaceutical companies to comply with the pharmaceutical industry’s voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government in addition to requiring drug manufacturers to report information related to payments to physicians and other health care providers or marketing expenditures. State and local laws require the registration of pharmaceutical sales representatives and state and foreign laws also govern the privacy and security of health information in some circumstances, many of which differ from each other in significant ways and often are not preempted by HIPAA, thus complicating compliance efforts.
Efforts to ensure that current and future business arrangements with third parties comply with applicable healthcare laws and regulations involves substantial costs.If operations are found to be in violation of any of these laws or any other governmental regulations that may apply to a business, the business may be subject to significant civil, criminal and administrative penalties, damages, fines, disgorgement, individual imprisonment, exclusion of products from government-funded healthcare programs, such as Medicare and Medicaid, additional reporting requirements and oversight if subject to a corporate integrity agreement or similar agreement to resolve allegations ofnon-compliance with these laws, and the curtailment or restructuring of operations.
Healthcare Reform
A primary trend in the United States healthcare industry and elsewhere is cost containment. There have been a number of federal and state proposals during the last few years regarding the pricing of pharmaceutical and biopharmaceutical products, limiting coverage and reimbursement for drugs and other medical products, government control and other changes to the healthcare system in the United States.
By way of example, the United States and state governments continue to propose and pass legislation designed to reduce the cost of healthcare. In March 2010, the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act, or collectively the Affordable Care Act, was enacted which, among other things, includes changes to the coverage and payment for products under government health care programs. Among the provisions of the Affordable Care Act of importance to potential drug candidates are:
| ∎ | an annual, nondeductible fee on any entity that manufactures or imports specified branded prescription drugs and biologic agents, apportioned among these entities according market share in certain government healthcare programs, although this fee would not apply to sales of certain products approved exclusively for orphan indications; |
| ∎ | expansion of eligibility criteria for Medicaid programs by, among other things, allowing states to offer Medicaid coverage to certain individuals with income at or below 133% of the federal poverty level, thereby potentially increasing a manufacturer’s Medicaid rebate liability; |
| ∎ | expansion of manufacturers’ rebate liability under the Medicaid Drug Rebate Program by increasing the minimum rebate for both branded and generic drugs and revising the definition of “average manufacturer price,” or AMP, for calculating and reporting Medicaid drug rebates on outpatient prescription drug prices and extending rebate liability to prescriptions for individuals enrolled in Medicare Advantage plans; |
| ∎ | a new methodology by which rebates owed by manufacturers under the Medicaid Drug Rebate Program are calculated for drugs that are inhaled, infused, instilled, implanted or injected; |
| ∎ | expanded types of entities eligible for the 340B drug discount program; |
| ∎ | establishment of the Medicare Part D coverage gap discount program by requiring manufacturers to provide a 50% (and 70% commencing January 1, 2019)point-of-sale-discount off the negotiated price of applicable brand drugs to eligible beneficiaries during their coverage gap period as a condition for the manufacturers’ outpatient drugs to be covered under Medicare Part D; |
| ∎ | establishment of a new Patient-Centered Outcomes Research Institute to oversee, identify priorities in, and conduct comparative clinical effectiveness research, along with funding for such research; |
146
Table of Contents
| ∎ | establishment of the Center for Medicare and Medicaid Innovation within CMS to test innovative payment and service delivery models to lower Medicare and Medicaid spending, potentially including prescription drug spending; and |
| ∎ | a licensure framework for follow on biologic products. |
Some of the provisions of the Affordable Care Act have yet to be implemented, and there have been judicial and Congressional challenges to certain aspects of the Affordable Care Act, as well as recent efforts by the Trump administration to repeal or replace certain aspects of the Affordable Care Act. Since January 2017, President Trump has signed two Executive Orders and other directives designed to delay the implementation of certain provisions of the Affordable Care Act or otherwise circumvent some of the requirements for health insurance mandated by the Affordable Care Act. Concurrently, Congress has considered legislation that would repeal or repeal and replace all or part of the Affordable Care Act. While Congress has not passed comprehensive repeal legislation, two bills affecting the implementation of certain taxes under the Affordable Care Act have been signed into law. The Tax Cuts and Jobs Act of 2017, or the Tax Act, includes a provision repealing, effective January 1, 2019, thetax-based shared responsibility payment imposed by the Affordable Care Act on certain individuals who fail to maintain qualifying health coverage for all or part of a year that is commonly referred to as the “individual mandate”. On January 22, 2018, President Trump signed a continuing resolution on appropriations for fiscal year 2018 that delayed the implementation of certain Affordable CareAct-mandated fees, including theso-called “Cadillac” tax on certain high cost employer-sponsored insurance plans, the annual fee imposed on certain health insurance providers based on market share, and the medical device excise tax onnon-exempt medical devices. The Bipartisan Budget Act of 2018, or the BBA, among other things, amends the Affordable Care Act, effective January 1, 2019, to close the coverage gap in most Medicare drug plans, commonly referred to as the “donut hole”. In July 2018, CMS published a final rule permitting further collections and payments to and from certain Affordable Care Act qualified health plans and health insurance issuers under the Affordable Care Act risk adjustment program in response to the outcome of federal district court litigation regarding the method CMS uses to determine this risk adjustment. On December 14, 2018, a U.S. District Court Judge in the Northern District of Texas ruled that the individual mandate is an inseverable feature of the Affordable Care Act, and therefore, because it was repealed as part of the Tax Act, the remaining provisions of the Affordable Care Act are invalid as well. While the Trump Administration and CMS have both stated that the ruling will have no immediate effect, it is unclear how this decision and subsequent appeals, if any, and other efforts to repeal and replace the Affordable Care Act will impact the Affordable Care Act.
Other legislative changes have been proposed and adopted in the United States since the Affordable Care Act was enacted. For example, in August 2011, the Budget Control Act of 2011, among other things, created measures for spending reductions by Congress. A Joint Select Committee on Deficit Reduction, tasked with recommending a targeted deficit reduction of at least $1.2 trillion for the years 2012 through 2021, was unable to reach required goals, thereby triggering the legislation’s automatic reduction to several government programs. This includes aggregate reductions of Medicare payments to providers of up to 2% per fiscal year, which went into effect in April 2013 and due to legislative amendments to the statute, including the BBA, and will remain in effect through 2027 unless additional Congressional action is taken. In January 2013, President Obama signed into law the American Taxpayer Relief Act of 2012, which, among other things, further reduced Medicare payments to several providers, including hospitals, imaging centers and cancer treatment centers, and increased the statute of limitations period for the government to recover overpayments to providers from three to five years.
Moreover, there has been heightened governmental scrutiny recently over pharmaceutical pricing practices in light of the rising cost of prescription drugs and biologics. Such scrutiny has resulted in several recent Congressional inquiries and proposed and enacted federal and state legislation designed to, among other things, bring more transparency to product pricing, review the relationship between pricing and manufacturer patient programs, and reform government program reimbursement methodologies for products. At the federal level, the Trump administration’s budget proposal for fiscal year 2019 contains further drug price control measures that could be enacted during the 2019 budget process or in other future legislation, including, for example, measures to permit Medicare Part D plans to negotiate the price of certain drugs under Medicare Part B, to allow some states to negotiate drug prices under Medicaid, and to eliminate cost sharing for generic drugs forlow-income patients.
Further, the Trump administration released a “Blueprint” to lower drug prices and reduce out-of-pocket costs of drugs that contains additional proposals to increase manufacturer competition, increase the negotiating power of
147
Table of Contents
certain federal healthcare programs, incentivize manufacturers to lower the list price of their products and reduce the out of pocket costs of drug products paid by consumers. HHS has already started the process of soliciting feedback on certain of these measures and, additionally, is immediately implementing others under its existing authority. For example, in September 2018, CMS announced that it will allow Medicare Advantage Plans the option to use step therapy for Part B drugs beginning January 1, 2019, and in October 2018, CMS proposed a new rule that would requiredirect-to-consumer television advertisements of prescription drugs and biological products, for which payment is available through or under Medicare or Medicaid, to include in the advertisement the Wholesale Acquisition Cost, or list price, of that drug or biological product. Although a number of these, and other potential, proposals will require authorization through additional legislation to become effective, Congress and the executive branch have each indicated that it will continue to seek new legislative and/or administrative measures to control drug costs. At the state level, legislatures have increasingly passed legislation and implemented regulations designed to control pharmaceutical and biological product pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access and marketing cost disclosure and transparency measures, and, in some cases, designed to encourage importation from other countries and bulk purchasing.
Additionally, on May 30, 2018, the Trickett Wendler, Frank Mongiello, Jordan McLinn, and Matthew Bellina Right to Try Act of 2017 was signed into law. The law, among other things, provides a federal framework for certain patients to access certain investigational new drug products that have completed a Phase 1 clinical trial and that are undergoing investigation for FDA approval. Under certain circumstances, eligible patients can seek treatment without enrolling in clinical trials and without obtaining FDA permission under the FDA expanded access program. There is no obligation for a drug manufacturer to make its drug products available to eligible patients as a result of the Right to Try Act.
Facilities
Our operations are conducted at Stealth Delaware, which is located in Newton, Massachusetts, where it occupies 14,446 square feet of office space. The lease expires November 30, 2020.
Employees
As of December 31, 2018, we had 57 full-time employees, 36 of whom were primarily engaged in research and development activities and 17 of whom had a Ph.D. or Pharm.D. degree. All of our full-time employees are based in the United States.
Legal Proceedings
We are not currently a party to any legal proceedings.
148
Table of Contents
Executive Officers and Directors
The following table sets forth the name and position of each of our directors of Stealth BioTherapeutics Corp and of the executive officers of Stealth Delaware and their ages as of December 31, 2018. Stealth BioTherapeutics Corp does not have any executive officers other than Reenie McCarthy, its Chief Executive Officer.
NAME | AGE | POSITION | ||||
Executive Officers | ||||||
Irene (Reenie) McCarthy | 54 | Chief Executive Officer, Director | ||||
Daniel E. Geffken | 61 | Interim Chief Financial Officer | ||||
Mark J. Bamberger, Ph.D. | 66 | Chief Scientific Officer | ||||
Brian D. Blakey, Pharm.D. | 56 | Chief Business Officer | ||||
James R. Carr, Pharm.D. | 56 | Chief Clinical Development Officer | ||||
Non-Employee Directors | ||||||
Gerald L. Chan, Sc.D. | 67 | Director, Chairman of the Board | ||||
Vincent Cheung(3) | 38 | Director | ||||
Lu Huang, M.D.(2) | 45 | Director | ||||
Francis W. Chen, Ph.D.(1)(3) | 70 | Director | ||||
Stephen Law(1)(2) | 56 | Director | ||||
Kevin F. McLaughlin(1)(3) | 62 | Director | ||||
Edward P. Owens(2) | 72 | Director | ||||
| (1) | Member of Audit Committee |
| (2) | Member of Remuneration Committee |
| (3) | Member of Nominating Committee |
Executive Officers
Irene (Reenie) McCarthy has served as Chief Executive Officer of Stealth BioTherapeutics Corp since October 2018. She has served as Chief Executive Officer of Stealth Delaware since February 2016 and as President and Secretary of Stealth Delaware since August 2015. She was appointed as a Director of Stealth BioTherapeutics Corp in June 2018. She has served as a director of Stealth Delaware since July 2009. Ms. McCarthy served as a member of Morningside Technology Advisory, LLC (and affiliates), a private advisory company, from January 2009 to April 2016. Ms. McCarthy remains a director of Morningside Technology Advisory, LLC. She has served as a director for numerous private biotechnology companies developing drugs across a broad spectrum of therapeutic focus areas. Ms. McCarthy was a director of Biovex Group, Inc., a biotechnology company developing an oncolytic vaccine for melanoma and head and neck cancer, from 2009 to 2011, when it was acquired by Amgen Inc. Prior to joining the Morningside group, Ms. McCarthy spent five years as a corporate lawyer with Richards & O’Neil LLP. She holds a J.D. from the University of Pennsylvania Law School and a B.A. in English and Political Science from Bates College. We believe that Ms. McCarthy is qualified to serve on our board of directors because of her extensive experience investing in life sciences companies, her service on several life science company boards and her almost decade of service to our company, as an investor, board member and officer.
Daniel E. Geffkenhas served as the interim Chief Financial Officer of Stealth Delaware since November 2016 through a consulting agreement entered into between the Company and Danforth Advisors LLC, or Danforth, on November 21, 2016, as amended. Mr. Geffken is a founder and managing director at Danforth, a management consulting firm, where he has served since 2011. Through Danforth, Mr. Geffken currently serves as Chief Financial Officer for Apic Bio, Inc., apre-clinical stage gene therapy company, starting in March 2018 and ProMIS Neurosciences, a biotechnology company focused on the discovery and development of antibody therapeutics for neurodegenerative diseases and listed on the Toronto Stock Exchange, starting in March 2017, and served as Chief Financial Officer for Homology Medicines, Inc., a genetic medicines company, from April 2015 to June 2017, and
149
Table of Contents
Apellis Pharmaceuticals, Inc., a biotechnology company focused on neurodevelopmental disorders, from August 2015 to August 2017. From 2013 through 2017, Mr. Geffken served on the board of directors of Alcobra Ltd., a Nasdaq-listed biotechnology company. Alcobra Ltd. later merged with Arcturus Therapeutics, Inc. and from
November 2017 until May 2018, Mr. Geffken served on the board of directors of Arcturus Therapeutics, Inc., a Nasdaq-listed company. Mr. Geffken received an M.B.A from the Harvard Business School and a B.S. in economics from The Wharton School, University of Pennsylvania.
Mark J. Bamberger, Ph.D., has served as Chief Scientific Officer of Stealth Delaware since February 2014. Prior to joining us, Dr. Bamberger worked as an independent consultant from January 2008 to February 2014, including being a consultant for Stealth Delaware pursuant to a consulting agreement dated April 1, 2011, as amended, from April 2011 to February 2014. Mr. Bamberger was the Director of Cardiovascular and Metabolic Disease Research at Pfizer, Inc., a pharmaceutical company, from January 2004 to January 2008. He holds a Ph.D. in biochemistry from the Medical College of Pennsylvania and a B.S. in biology from St. Joseph’s University.
Brian D. Blakey, Pharm.D., has served as Chief Business Officer of Stealth Delaware since February 2014. Previously, Dr. Blakey was the Chief Strategy and Operations Officer of Element Marketing Group, a medical marketing agency, from June 2010 to February 2014, and was the Vice President of Commercial Development at Salutria Pharmaceuticals, LLC (formerly AtheroGenics Inc.), a biotechnology company, from May 2006 to May 2010. He also worked in multiple roles at GlaxoSmithKline, plc, a pharmaceutical company, beginning in March 1998, ultimately serving in the position of director between July 2003 and February 2004. Dr. Blakey holds a Pharm.D. from the University of Florida.
James R. Carr, Pharm.D., has served as Chief Clinical Development Officer of Stealth Delaware since January 2017 and previously served as our Vice President, Clinical Development since March 2014. Previously, Dr. Carr was the Executive Director in the Cardiovascular Metabolic Franchiseat GlaxoSmithKline plc, a pharmaceutical company, from October 2010 to March 2014 and the Vice President of Clinical Development at ARCA biopharma, Inc., a pharmaceutical company, from May 2008 to November 2010. Dr. Carr holds a Pharm.D. and a B.S. in pharmacy from the University of Minnesota.
Non-Employee Directors
Gerald L. Chan, Sc.D., was appointed as a Director of Stealth BioTherapeutics Corp and as Chairman of the Board in June 2018. He has served as a director of Stealth Delaware since October 2007. Dr. Chanco-founded the Morningside group in 1986. He has been a member of the board of directors of Hang Lung Group Limited since 1986, and Aduro Biotech Inc., a Nasdaq listed company, since 2014. Dr. Chan received a B.S. and M.S. in engineering from the University of California, Los Angeles, and a M.S. in medical radiological physics and an Sc.D. in radiation biology from Harvard University. He did his post-doctoral training at the Dana-Farber Cancer Institute as a fellow of the Leukemia Society of America. We believe that Dr. Chan is qualified to serve on our board of directors because of his extensive experience investing in and serving on the boards of directors of life sciences companies.
Vincent Sai Sing Cheung was appointed as a Director of Stealth BioTherapeutics Corp in June 2018. Mr. Cheung is currently the Managing Director and the Chief Operating Officer of the Nan Fung Group, an international business conglomerate with global interests in property, financial investments and a diverse range of business partnerships. Mr. Cheung was appointed as aNon-executive Director of Forterra Real Estate Pte. Ltd. in August 2013. Forterra Real Estate Pte. Ltd. was acquired by Nan Fung International Holdings Limited in 2015. He also served as aNon-executive Director and Executive Director of Sino-Ocean Group Holding Limited from March 2011 to May 2014 and from May 2014 to August 2015, respectively. Mr. Cheung received a B.A. in molecular and cell biology from the University of California, Berkeley. We believe Mr. Cheung is qualified to serve on our board of directors because of his financial and business experience.
Lu Huang, M.D., was appointed as a Director of Stealth BioTherapeutics Corp in June 2018. Dr. Huang joined the Morningside group in October 2003 and leads the Morningside life science investment team in China. She has led over a dozen healthcare and life sciences investments in China and serves as a director in a number of portfolio companies including MicuRx Pharmaceuticals, Inc. Dr. Huang obtained her M.D. from Shanghai Jiao Tong University School of Medicine (formerly known as Shanghai Second Medical University) in China and subsequently worked at the Clinical Medical Centre of Shanghai Second Medical University. She holds an M.B.A. from St. John’s University.
150
Table of Contents
We believe Dr. Huang is qualified to serve on our board of directors because of her extensive experience serving on the boards of directors of life sciences companies and her medical insights.
Francis W. Chen, Ph.D., was appointed as a Director of Stealth BioTherapeutics Corp in June 2018. He has served as a director of Stealth Delaware since April 2006. In November 2011, he founded, and currently serves as the chairman of, SinoAmerican Partners Limited, an advisory services firm that specializes in cross-border transactions involving natural resources, transportation-based assets and related financial services. Dr. Chen was also a venture partner at WI Harper Group, an early-stage venture capital firm with investment activities in Silicon Valley and China from June 2009 to December 2012. He previously served on the board of directors of SPI Energy Co., Ltd. from November 2009 to August 2013. Dr. Chen has more than 20 years of prior management experience in the healthcare industry and has served on the board of directors of several private companies. Dr. Chen holds a Ph.D. in immunology from Harvard University and an M.S. and a B.S. in chemistry from Tufts University. We believe Dr. Chen is qualified to serve on our board of directors because of his extensive experience investing in and serving on the boards of directors of life science companies.
Cheuk Kin Stephen Law was appointed as a Director of Stealth BioTherapeutics Corp in June 2018. Mr. Law has over 30 years of experience in accounting, corporate finance and investment. He is currently the Managing Director of ANS Capital Limited, a company principally engaged in investment and corporate finance. He also serves as an IndependentNon-executive Director of China Everbright Limited since May 2018 and served as an Independent Non-executive Director of AAG Energy Holdings Limited, a clean energy company whose shares are listed on the Hong Kong Stock Exchange, between July 2016 and September 2018. He has been a board member of Hong Kong Business Accountants Association since August 2017. Since June 2016, Mr. Law has served as an expert consultant for the Ministry of Finance of the Peoples Republic of China to advise on finance and management accounting. Mr. Law previously served as the Finance Director and an executive director of MTR Corporation Ltd. between July 2013 and July 2016, where he was responsible for overseeing finance, investment control, treasury and other matters. Previously, he served as Chief Financial Officer at Guoco Group Limited, an investment holding company whose shares are listed on the Hong Kong Stock Exchange, from October 2012 to June 2013; as a principal and then a managing director of TPG Growth Funds, one of the largest global private equity funds, where he was responsible for private equity investments in Asia, from July 2006 to September 2012; served as a senior investment professional of Morningside Technologies Inc., a Cayman Islands company principally engaging in venture capital and private equity, from July 2000 to July 2006; and as an investment control manager of Wheelock Pacific Limited from February 1995 to July 1997 and worked in the corporate development and finance division of Wharf Cable Limited from July 1997 to July 2000. Mr. Law is a member of the Institute of Chartered Accountants in England and Wales, and of the Hong Kong Institute of Certified Public Accountants. He was a council member of Hong Kong Institute of Certified Public Accountants from 2010 to 2017. Mr. Law received a B.Sc. (Civil Engineering) from the University of Birmingham in the United Kingdom in July 1984. Mr. Law has been an adjunct professor of the Hong Kong Polytechnic University from October 2015 to August 2017. We believe Mr. Law is qualified to serve on our board of directors because of his significant investing experience, as well as his accounting and financial expertise.
Kevin F. McLaughlin was appointed as a Director of Stealth BioTherapeutics Corp in June 2018. He has served as a director of Stealth Delaware since March 2017. Mr. McLaughlin is currently Senior Vice President, Chief Financial Officer and Treasurer of Acceleron Pharma, Inc., a biotechnology company, and has been since November 2010. Mr. McLaughlin has also served on the board of directors of Vericel Corporation, a biopharmaceutical company, since January 2015. He previously served as Senior Vice President and Chief Financial Officer of Qteros, Inc., a cellulosic biofuels company, from 2009 through 2010 and asco-founder, Chief Operating Officer and director of Aptius Education, Inc., a publishing company, from 2007 through 2009. Mr. McLaughlin held several executive positions with PRAECIS Pharmaceuticals, Inc., a biopharmaceutical company, from 1996 through 2007, initially as Chief Financial Officer, before becoming Chief Operating Officer and eventually President and Chief Executive Officer, and he served as a member of the board of directors. Mr. McLaughlin began his career in senior financial roles at Prime Computer and Computervision Corporation. Mr. McLaughlin received a B.S. in business from Northeastern University and an M.B.A. from Babson College. We believe Mr. McLaughlin is qualified to serve on our board of directors because of his extensive experience managing and serving on the boards of directors of life science companies.
Edward P. Owens was appointed as a Director of Stealth BioTherapeutics Corp in June 2018. He has served as a director of Stealth Delaware since May 2017. Mr. Owens has been a Director of Ironwood Pharmaceuticals, Inc., a
151
Table of Contents
Nasdaq-listed company, since March 2013. He is a retired Partner of Wellington Management Company LLP and the founding portfolio manager of Vanguard Health Care Fund, which he managed from 1984 until his retirement at the end of 2012. Mr. Owens holds a B.S. in Physics from the University of Virginia and an M.B.A. from Harvard Business School. We believe Mr. Owens is qualified to serve on our board of directors because of his experience in serving on the board of directors of life sciences companies, as well as his investment expertise.
Corporate Governance
We are a “foreign private issuer,” as defined by the SEC. As a result, in accordance with the rules and regulations of Nasdaq, we will comply with home country governance requirements and certain exemptions thereunder rather than complying with Nasdaq corporate governance standards. While we voluntarily follow most Nasdaq corporate governance rules, we may choose to take advantage of the following limited exemptions afforded to foreign private issuers:
| ∎ | Exemption from the requirement to have independent director oversight of director nominations; |
| ∎ | Exemption from the requirements that our board of directors have a compensation committee that is composed entirely of independent directors; and |
| ∎ | Exemption from the requirement that our board of directors shall have regularly scheduled meetings at which only independent directors are present as set forth in Nasdaq Rule 5605(b)(2). |
We intend to follow our home country practices in lieu of the foregoing requirements. Although we may rely on home country corporate governance practices in lieu of certain of the rules in the Nasdaq Rule 5600 Series and Rule 5250(d), we must comply with Nasdaq’s Notification of Noncompliance requirement (Rule 5625), the Voting Rights requirement (Rule 5640) and have an audit committee that satisfies Rule 5605(c)(3), consisting of committee members that meet the independence requirements of Rule 5605(c)(2)(A)(ii). Although we currently intend to comply with the Nasdaq corporate governance rules applicable other than as noted above, we may in the future decide to use the foreign private issuer exemption with respect to some or all the other Nasdaq corporate governance rules.
In addition, as a foreign private issuer, we expect to take advantage of the following exemptions from SEC reporting obligations:
| ∎ | Exemption from filing quarterly reports on Form10-Q or provide current reports on Form8-K, disclosing significant events within four days of their occurrence. |
| ∎ | Exemption from Section 16 rules regarding sales of common shares by insiders, which will provide less data in this regard than shareholders of U.S. companies that are subject to the Exchange Act. |
Accordingly, our shareholders will not have the same protections afforded to shareholders of companies that are subject to all of the corporate governance requirements of Nasdaq and the domestic reporting requirements of the SEC. We may utilize these exemptions for as long as we continue to qualify as a foreign private issuer.
Board Composition
Our board of directors consists of Reenie McCarthy, Gerald L. Chan, Vincent Sai Sing Cheung, Dr. Lu Huang, Francis W. Chen, Cheuk Kin Stephen Law, Kevin F. McLaughlin and Edward P. Owens. Our directors will hold office until their successors have been elected and qualified or until the earlier of their resignation or removal. As a foreign private issuer, under the listing requirements and rules of Nasdaq, we are not required to have independent directors on our board of directors, except that our audit committee is required to consist fully of independent directors, subject to certainphase-in schedules. However, our board of directors has determined that, of our eight directors, six do not have a relationship that would interfere with the exercise of independent judgment in carrying out the responsibilities of director and that each of these directors is “independent” as that term is defined under Nasdaq rules.
Board Committees
Our board of directors has established audit, remuneration and nominating committees.
152
Table of Contents
Audit Committee
The members of our audit committee are Stephen Law, Francis W. Chen, and Kevin F. McLaughlin, and Kevin F. McLaughlin serves as the chair of our audit committee. Our board of directors has determined that he is an “audit committee financial expert” as defined by applicable SEC rules. Our audit committee assists our board of directors in its oversight of our accounting and financial reporting process and the audits of our financial statements. Our audit committee’s responsibilities include:
| ∎ | appointing, approving the compensation of, and assessing the independence of our registered public accounting firm; |
| ∎ | overseeing the work of our independent registered public accounting firm, including through the receipt and consideration of reports from such firm; |
| ∎ | reviewing and discussing with management and our independent registered public accounting firm our annual and quarterly financial statements and related disclosures; |
| ∎ | monitoring our internal control over financial reporting, disclosure controls and procedures, and code of business conduct and ethics; |
| ∎ | overseeing our internal audit function, if any; |
| ∎ | discussing our risk management policies; |
| ∎ | establishing procedures for the receipt and retention of accounting-related complaints and concerns; |
| ∎ | meeting independently with our internal auditing staff, our independent registered public accounting firm, and management; |
| ∎ | reviewing and approving or ratifying any related person transactions; and |
| ∎ | preparing the audit committee report required by SEC rules. |
All audit services to be provided to us and allnon-audit services, other thande minimisnon-audit services, to be provided to us by our registered public accounting firm must be approved in advance by our audit committee.
We expect to satisfy the member independence requirements for the audit committee prior to the end of the transition period provided under current Nasdaq Listing Rules and SEC rules and regulations for companies completing their initial public offering.
Remuneration Committee
The members of our remuneration committee are Edward P. Owens, Stephen Law and Dr. Lu Huang, and Edward P. Owens serves as the chair of our remuneration committee. Our remuneration committee assists our board of directors in the discharge of its responsibilities relating to the compensation of our executive officers. Our remuneration committee’s responsibilities include:
| ∎ | reviewing and approving, or making recommendations to our board of directors with respect to, the compensation of our Chief Executive Officer; |
| ∎ | reviewing and approving, or making recommendations to our board of directors with respect to, the compensation of our other executive officers; |
| ∎ | overseeing the evaluation of our senior executives; |
| ∎ | reviewing and making recommendations to our board of directors with respect to our incentive compensation and equity-based compensation plans; |
| ∎ | overseeing and administering our equity-based plans; |
| ∎ | reviewing and making recommendations to our board of directors with respect to director compensation; |
| ∎ | reviewing and discussing with management our “Compensation Discussion and Analysis” disclosure to the extent such disclosure is required by SEC rules; and |
| ∎ | preparing the remuneration committee report required by SEC rules. |
153
Table of Contents
Nominating Committee
The members of our nominating committee are Francis W. Chen, Kevin F. McLaughlin and Vincent Cheung, and Francis W. Chen serves as the chair of our nominating committee. Our nominating committee’s responsibilities include:
| ∎ | identifying individuals qualified to become members of our board of directors; |
| ∎ | recommending to our board of directors the persons to be nominated for election as directors and to each of our board of directors’ committees; |
| ∎ | developing and recommending to our board of directors corporate governance principles; and |
| ∎ | overseeing periodic evaluations of our board of directors. |
Compensation
For the year ended December 31, 2018, the aggregate compensation accrued or paid to our executive officers for services in all capacities was $1.9 million plus option awards exercisable for 416,667 ordinary shares at an exercise price of $1.20. Options for 416,667 shares expire on February 27, 2028. Except for the grant of share options to Mr. Law upon his joining the Stealth Delaware board of directors in 2018, none of ournon-employee directors received any compensation from us in the fiscal year ended December 31, 2018. The compensation that we pay to Reenie McCarthy, who is also our Chief Executive Officer, is received solely in her capacity as Chief Executive Officer.
In September 2018, we adopted a non-employee director compensation policy, to be effective upon closing of this offering, that provides to each non-employee director:
| ∎ | $40,000 per year for his or her service as a non-employee director; |
| ∎ | $8,000 per year per committee for his or her service as the audit, remuneration and/or nomination committee chair; |
| ∎ | $5,000 per year per committee for his or her service as an audit, remuneration and/or nomination committee member (other than for the committee chair); and |
| ∎ | at the discretion of the board of directors, an annual grant of options or restricted share units in respect of ordinary shares. |
The following table sets forth information concerning outstanding equity awards for each of ournon-employee directors as of December 31, 2018:
| OPTION AWARDS | ||||||||||||||||
NAME | NUMBER OF SECURITIES UNDERLYING UNEXERCISED OPTIONS EXERCISABLE (#) | NUMBER OF SECURITIES UNDERLYING UNEXERCISED OPTIONS UNEXERCISABLE (#) | OPTION EXERCISE PRICE ($) | OPTION EXPIRATION DATE | ||||||||||||
Gerald L. Chan, Sc.D. | 2,500,000 | — | $ | 0.84 | 8/26/2024 | |||||||||||
Francis W. Chen, Ph.D. | 50,000 | — | $ | 0.45 | 12/13/2022 | |||||||||||
Vincent Cheung | — | — | — | — | ||||||||||||
Lu Huang, M.D. | — | — | — | — | ||||||||||||
Stephen Law | 6,250 | 43,750 | $ | 1.53 | (1) | 06/27/2028 | ||||||||||
Kevin F. McLaughlin | 21,875 | 28,125 | $ | 1.38 | 03/15/2027 | |||||||||||
Edward P. Owens | 19,792 | 30,208 | $ | 1.38 | 05/23/2027 | |||||||||||
| (1) | In October 2018, the exercise price per share of these options was reduced from $2.22 to $1.53 per share. |
We also reimburse ournon-employee directors for reasonable travel andout-of-pocket expenses incurred in connection with attending our board of director and committee meetings.
154
Table of Contents
Agreements with our Executive Officers
We have entered into offer letters with each of our executive officers, other than Mr. Geffken, that set forth the terms of the executive officer’s compensation, including his or her initial base salary and an annual cash bonus target percentage. The offer letters provide that the executive officers are eligible to participate in company-sponsored benefit programs that are available generally to all of our employees.
In addition, our offer letters with Dr. Blakey and Dr. Carr provide for the payment of six months base salary in the event that we terminate their employment without cause, subject to the execution of a release of claims. Under the letters, cause is defined as one or more of (i) willful malfeasant, dishonest or grossly negligent conduct that relates to us and causes us harm or damage, (ii) a continued breach of conduct required by the invention andnon-disclosure agreement, including a material breach of anynon-competition,non-solicitation or confidentiality covenant or under any applicable legal principle, (iii) a material breach of duty of loyalty to us, (iv) a commission of an act of fraud, theft, misappropriation or embezzlement, (v) the commission of an act of fraud, theft, misappropriation or embezzlement or (vi) a conviction of, or pleadingnolo contendere to, a felony or any other crime involving moral turpitude. Severance payments to either of Dr. Blakey or Dr. Carr could be delayed for six months in certain circumstances for compliance with Section 409A of the Internal Revenue Code of 1986, as amended, or the Code.
The services of Mr. Geffken as interim CFO are provided pursuant to a consulting agreement with Danforth. See “Related Party Transactions—Consulting Agreement” for a further description of this agreement.
Equity andNon-Equity Incentive Plans
The three equity incentive plans described in this section are our 2006 share incentive plan, as amended to date, or the 2006 plan, our 2019 share incentive plan, or the 2019 plan and our 2019 employee share purchase plan, or ESPP. Prior to this offering, we granted awards to eligible participants under the 2006 plan. Following the closing of this offering, we expect to grant awards to eligible participants under the 2019 plan and the ESPP.
2006 Share Incentive Plan
In 2010, our board of directors adopted, and our shareholders approved, the 2006 plan. The 2006 plan provides for the grant of options, restricted shares and other awards that are valued in whole or in part by reference to, or are otherwise based on, ordinary shares or other property. Our employees, officers, directors, consultants and advisers are eligible to receive awards under our 2006 plan. Our board of directors administers the 2006 plan.
The 2006 plan provides that a maximum of 25,544,054 ordinary shares are authorized for issuance under the plan. No awards may be granted under the 2006 plan after December 15, 2019 and upon effectiveness of the 2019 plan no new awards will be granted under the 2006 plan. Our board of directors may amend, suspend or terminate the 2006 plan at any time.
In the event of any share split, reverse share split, share dividend, recapitalization, combination of shares, reclassification of shares,spin-off or other similar change in capitalization or event, or any distribution to holders of ordinary shares other than an ordinary cash dividend, we shall appropriately adjust, to the extent determined by the board of directors:
| ∎ | the number and class of securities available under the 2006 plan; |
| ∎ | the number and class of securities and exercise price per share of each outstanding option; |
| ∎ | the repurchase price per share subject to each outstanding restricted share award; and |
| ∎ | the terms of each other outstanding award under the 2006 plan. |
In the event of any merger or consolidation of our company with or into another entity as a result of which all of our ordinary shares are converted into or exchanged for the right to receive cash, securities or other property or are cancelled; an exchange of all of our ordinary shares for cash, securities or other property pursuant to a share exchange transaction; or a liquidation or dissolution of our company, our board of directors shall, on such terms as
155
Table of Contents
our board of directors determines, take any one or more of the following actions pursuant to the 2006 plan, as to some or all outstanding awards, except as to restricted share awards:
| ∎ | provide that awards shall be assumed, or substantially equivalent awards shall be substituted, by the acquiring or succeeding corporation (or an affiliate thereof); |
| ∎ | upon written notice to a plan participant, provide that the participant’s unexercised options or other awards shall be exercisable in full and will terminate immediately prior to the consummation of such event unless exercised by the participant within a specified period following the date of such notice; |
| ∎ | provide that outstanding awards shall become realizable, or deliverable, or restrictions applicable to an award shall lapse, in whole or in part prior to or upon such event; |
| ∎ | if under the terms of such event, holders of ordinary shares will receive upon consummation thereof a cash payment for each share surrendered in the event, make or provide for a cash payment to a plan participant in exchange for the termination of such awards; |
| ∎ | provide that, in connection with a liquidation of dissolution of the company, awards shall convert into the right to receive liquidation proceeds; or |
| ∎ | any combination of the foregoing. |
In regards to the restricted share awards, should one of the events described above occur, other than a liquidation or dissolution of our company, than the repurchase and other rights under the restricted share award shall inure to the benefit of our successor and shall apply to the cash, securities or other property which the ordinary shares were converted into or exchanged for pursuant to such event in the same manner and to the same extent as they applied to the ordinary shares subject to such restricted share award. Upon the occurrence of a liquidation or dissolution of our company, except to the extent specifically provided to the contrary in such instrument evidencing any restrict share award or any other agreement between a plan participant and us, all restrictions and conditions on all restricted share awards then outstanding shall automatically be deemed terminated or satisfied.
Our board of directors is not obligated under the 2006 plan to issue all awards under identical terms or treat all plan participants uniformly. Our board of directors may amend, modify or terminate any outstanding award either with the consent of the plan participant or if in the board of director’s determination such action would not materially and adversely affect the plan participant.
2019 Share Incentive Plan
In January 2019 our board of directors adopted, and our shareholders approved, the 2019 plan to become effective immediately prior to the effectiveness of the registration statement related to this offering. The 2019 plan provides for the grant of incentive share options,non-statutory share options, share appreciation rights, awards of restricted shares, restricted share units or other share-based awards. Upon the closing of this offering, the number of our ordinary shares that will be reserved for issuance under the 2019 plan will be the sum of 47,692,934 shares plus (1) the number of our ordinary shares subject to outstanding awards under our 2006 plan upon the closing of this offering that expire, terminate or are otherwise surrendered, cancelled, forfeited or repurchased by us at their original issuance price pursuant to a contractual repurchase right and (2) an annual increase, to be added the first day of each fiscal year, beginning with the fiscal year ending December 31, 2020 and continuing until, and including, the fiscal year ending December 31, 2029, equal to the lowest of 31,780,518 of our ordinary shares, 4.0% of the number of ordinary shares outstanding on the first day of the fiscal year and an amount determined by our board of directors. Our employees, officers, directors, consultants and advisors will be eligible to receive awards under the 2019 plan; however, incentive share options may only be granted to our employees.
Pursuant to the terms of the 2019 plan, our board of directors (or a committee delegated by our board of directors) administers the 2019 plan and, subject to any limitations set forth in the 2019 plan, will select the recipients of awards and determine:
| ∎ | the number of ordinary shares covered by options and the dates upon which those options become exercisable; |
156
Table of Contents
| ∎ | the type of options to be granted; |
| ∎ | the exercise price of options, which price must be at least equal to the fair market value of our ordinary shares on the date of grant; |
| ∎ | the duration of options, which may not be in excess of 10 years; |
| ∎ | the methods of payment of the exercise price of options; and |
| ∎ | the number of our ordinary shares subject to and the terms of any share appreciation rights, awards of restricted share, restricted share units or other share-based awards and the terms and conditions of such awards, including the issue price, conditions for repurchase, repurchase price and performance conditions (though the measurement price of share appreciation rights must be at least equal to the fair market value of our ordinary shares on the date of grant and the duration of such awards may not be in excess of ten years), if any. |
In the event of any share split, reverse share split, share consolidation, share dividend, recapitalization, combination of shares, reclassification of shares,spin-off or other similar change in capitalization or event, or any dividend or distribution to holders of our ordinary shares other than an ordinary cash dividend, we are required by the 2019 plan to make equitable adjustments (or make substitute awards, if applicable), in a manner determined by our board, to:
| ∎ | the number and class of securities available under the 2019 plan; |
| ∎ | the share counting rules under the 2019 plan; |
| ∎ | the number and class of shares and exercise price per share of each outstanding option; |
| ∎ | the share andper-share provisions and measurement price of each outstanding share appreciation right; |
| ∎ | the number of shares and the repurchase price per share subject to each outstanding restricted share award; and |
| ∎ | the share andper-share related provisions and purchase price, if any, of any outstanding restricted stock unit award and other share-based award. |
Upon a merger or other reorganization event (as defined in our 2019 plan), our board of directors, may, on such terms as our board determines (except to the extent specifically provided otherwise in an applicable award agreement or other agreement between the participant and us), take any one or more of the following actions pursuant to the 2019 plan, as to some or all outstanding awards, other than restricted share awards:
| ∎ | provide that all outstanding awards will be assumed or substantially equivalent awards will be substituted by the acquiring or successor corporation (or an affiliate thereof); |
| ∎ | upon written notice to a participant, provide that the participant’s unvested and/or unexercised awards will terminate or be forfeited immediately prior to the consummation of such transaction unless exercised by the participant; |
| ∎ | provide that outstanding awards will become exercisable, realizable or deliverable, or restrictions applicable to an award will lapse, in whole or in part, prior to or upon the reorganization event; |
| ∎ | in the event of a reorganization event pursuant to which holders of our ordinary shares will receive a cash payment for each share surrendered in the reorganization event, make or provide for a cash payment to the participants with respect to each award held by a participant equal to (1) the number of shares of our ordinary shares subject to the vested portion of the award (after giving effect to any acceleration of vesting that occurs upon or immediately prior to such reorganization event) multiplied by (2) the excess, if any, of the cash payment for each share surrendered in the reorganization event over the exercise, measurement or purchase price of such award and any applicable tax withholdings, in exchange for the termination of such award; |
| ∎ | provide that, in connection with a liquidation or dissolution, awards convert into the right to receive liquidation proceeds (if applicable, net of exercise, measurement or purchase price thereof and any applicable tax withholdings); or |
| ∎ | any combination of the foregoing. |
157
Table of Contents
Our board of directors is not obligated by the 2019 plan to treat all awards, all awards held by a participant, or all awards of the same type, identically.
In the case of certain outstanding restricted share units, no assumption or substitution is permitted, and the restricted share units will instead be settled in accordance with the terms of the applicable restricted share unit agreement.
Upon the occurrence of a reorganization event other than a liquidation, winding up or dissolution, the repurchase and other rights under each outstanding restricted share award will continue for the benefit of the successor company and will, unless our board of directors may otherwise determine, apply to the cash, shares, securities or other property which our ordinary shares are converted into or exchanged for pursuant to the reorganization event, unless our board of directors provided for the termination or deemed satisfaction of such repurchase or other rights under the restricted share award agreement or any other agreement between the participant and us. Upon the occurrence of a reorganization event involving a liquidation, winding up or dissolution, all restrictions and conditions on each outstanding restricted share award will automatically be deemed terminated or satisfied, unless otherwise provided in the agreement evidencing the restricted share award or in any other agreement between the participant and us.
Our board of directors may at any time provide that any award under the 2019 plan shall become immediately exercisable in whole or in part, free of some or all restrictions or conditions, or otherwise realizable in whole or in part, as the case may be.
Except with respect to certain actions requiring shareholder approval under the Nasdaq Listing Rules, the 2019 plan, and our Articles of Association, our board of directors may amend, modify or terminate any outstanding award under the 2019 plan, including but not limited to, substituting therefor another award of the same or a different type, changing the date of exercise or realization, and converting an incentive share option into a nonstatutory share option, subject to certain participant consent requirements. Unless our shareholders approve such action, the 2019 plan provides that we may not (except as otherwise permitted in connection with a change in capitalization or reorganization event):
| ∎ | amend any outstanding share option or share appreciation right granted under the 2019 plan to provide an exercise or measurement price per share that is lower than the then-current exercise or measurement price per share of such outstanding award; |
| ∎ | cancel any outstanding option or share appreciation right (whether or not granted under the 2019 plan) and grant in substitution therefor new awards under the 2019 plan (other than substitute awards permitted in connection with a merger or consolidation of an entity with us or our acquisition of property or share of another entity) covering the same or a different number of our ordinary shares and having an exercise or measurement price per share lower than the then-current exercise or measurement price per share of the cancelled award; |
| ∎ | cancel in exchange for a cash payment any outstanding option or share appreciation right with an exercise or measurement price per share above the then-current fair market value of our ordinary shares; or |
| ∎ | take any other action that constitutes a “repricing” within the meaning of the Nasdaq Listing Rules. |
No award may be granted under the 2019 plan after 10 years from the effective date of this offering, but awards previously granted may extend beyond that date. Our board of directors may amend, suspend or terminate the 2019 plan at any time, except that shareholder approval will be required to comply with applicable law or the Nasdaq Listing Rules.
2019 Employee Share Purchase Plan
In January 2019, our board of directors adopted, and our shareholders approved, the ESPP, to become effective immediately prior to the effectiveness of the registration statement related to this offering. The ESPP will be administered by our board of directors or by a committee appointed by our board of directors. The ESPP initially provides participating employees with the opportunity to purchase up to an aggregate of 3,972,565 ordinary shares. The number of ordinary shares reserved for issuance under the ESPP will automatically increase on the first day of each fiscal year, beginning with the fiscal year ending December 31, 2020 and continuing until, and including, the fiscal year ending December 31, 2030, equal to the lowest of (i) 7,945,130 ordinary shares, (ii)
158
Table of Contents
1.0% of the number of ordinary shares outstanding on the first day of the fiscal year and (iii) an amount determined by our board of directors.
All of our employees or employees of any designated subsidiary, as defined in the ESPP, are eligible to participate in the ESPP, provided that:
| ∎ | such person is customarily employed by us or a designated subsidiary for more than 20 hours a week and for more than five months in a calendar year; |
| ∎ | such person has been employed by us or by a designated subsidiary for at least three months prior to enrolling in the ESPP; and |
| ∎ | such person was our employee or an employee of a designated subsidiary on the first day of the applicable offering period under the ESPP. |
No employee may be granted an option which permits them to purchase ordinary shares under the ESPP and any of our other employee share purchase plans to accrue at a rate which exceeds $25,000 of the fair market value of our ordinary shares in any calendar year in which the option is outstanding. In addition, no employee may purchase ordinary shares under the ESPP that would result in the employee owning 5% or more of the total combined voting power or value of our shares.
We expect to make one or more offerings to our eligible employees to purchase shares under the ESPP beginning at such time as our board of directors or committee may determine. Each offering will consist of asix-month offering period during which payroll deductions will be made and held for the purchase of our ordinary shares at the end of the offering period. Our board of directors may, at its discretion, choose a different period of not more than 12 months for an offering.
On the commencement date of each offering period, each eligible employee may authorize up to a maximum of 15% of his or her compensation to be deducted by us during the offering period. Each employee who continues to be a participant in the ESPP on the last business day of the offering period will be deemed to have exercised an option to purchase from us the number of whole ordinary shares that his or her accumulated payroll deductions on such date will pay for, not in excess of the maximum numbers set forth above. Under the terms of the ESPP, the purchase price shall be determined by our board of directors for each offering period and will be at least 85% of the applicable closing price of our ordinary shares. If our board of directors does not make a determination of the purchase price, the purchase price will be 85% of the lesser of the closing price of our ordinary shares on the first business day of the offering period or on the last business day of the offering period.
An employee may for any reason withdraw from participation in an offering prior to close of business on the fifteenth business day prior to the end of an offering period and permanently draw out the balance accumulated in the employee’s account. If an employee elects to discontinue his or her payroll deductions during an offering period but does not elect to withdraw his or her funds, funds previously deducted will be applied to the purchase of ordinary shares at the end of the offering period. If a participating employee’s employment ends before the last business day of an offering period, no additional payroll deductions will be made and the balance in the employee’s account will be paid to the employee.
We will be required to make equitable adjustments to the number and class of securities available under the ESPP, the share limitations under the ESPP, and the purchase price for an offering period under the ESPP to reflect share splits, reverse share splits, share consolidation, share dividends, recapitalizations, combinations of shares, reclassifications of shares, spin-offs and other similar changes in capitalization or events or any dividends or distributions to holders of our ordinary shares other than ordinary cash dividends.
In connection with a merger or other reorganization event, as defined in the ESPP, our board of directors or a committee of our board of directors may take any one or more of the following actions as to outstanding options to purchase ordinary shares under the ESPP on such terms as our board or committee determines:
| ∎ | provide that options shall be assumed, or substantially equivalent options shall be substituted, by the acquiring or succeeding corporation (or an affiliate thereof); |
159
Table of Contents
| ∎ | upon written notice to employees, provide that all outstanding options will be terminated immediately prior to the consummation of such reorganization event and that all such outstanding options will become exercisable to the extent of accumulated payroll deductions as of a date specified by our board of directors or committee in such notice, which date shall not be less than ten days preceding the effective date of the reorganization event; |
| ∎ | upon written notice to employees, provide that all outstanding options will be cancelled as of a date prior to the effective date of the reorganization event and that all accumulated payroll deductions will be returned to participating employees on such date; |
| ∎ | in the event of a reorganization event under the terms of which holders of our ordinary shares will receive upon consummation thereof a cash payment for each share surrendered in the reorganization event, change the last day of the offering period to be the date of the consummation of the reorganization event and make or provide for a cash payment to each employee equal to (1) the cash payment for each share surrendered in the reorganization event times the number of ordinary shares that the employee’s accumulated payroll deductions as of immediately prior to the reorganization event could purchase at the applicable purchase price, where the acquisition price is treated as the fair market value of our ordinary shares on the last day of the applicable offering period for purposes of determining the purchase price and where the number of shares that could be purchased is subject to the applicable limitations under the ESPP minus (2) the result of multiplying such number of shares by the purchase price; and/or |
| ∎ | provide that, in connection with our liquidation or dissolution, options shall convert into the right to receive liquidation proceeds (net of the purchase price thereof). |
Our board of directors may at any time, and from time to time, amend or suspend the ESPP or any portion thereof. We will obtain shareholder approval for any amendment if such approval is required by Section 423 of the Code. Further, our board of directors may not make any amendment that would cause the ESPP to fail to comply with Section 423 of the Code. The ESPP may be terminated at any time by our board of directors. Upon termination, we will refund all amounts in the accounts of participating employees.
401(k) Retirement Plan
We maintain a 401(k) retirement plan that is intended to be atax-qualified defined contribution plan under Section 401(k) of the Code. In general, all of our employees are eligible to participate. The 401(k) plan includes a salary deferral arrangement pursuant to which participants may elect to reduce their current compensation by up to the statutorily prescribed limit and have the amount of the reduction contributed to the 401(k) plan. We contribute up to 3% of an employee’s salary, subject to statutory limits.
Rule10b5-1 Sales Plans
Our directors and executive officers may adopt written plans, known asRule 10b5-1 plans, in which they will contract with a broker to buy or sell ordinary shares on a periodic basis. Under aRule 10b5-1 plan, a broker executes trades pursuant to parameters established by the director or officer when entering into the plan, without further direction from the director or officer. The director or officer may amend or terminate the plan in some circumstances. Our directors and executive officers may also buy or sell additional shares outside of aRule 10b5-1 plan when they are not in possession of material, nonpublic information.
Code of Business Conduct and Ethics
In December 2018, our board of directors adopted a written code of business conduct and ethics, to be effective upon the completion of this offering, that applies to our directors, officers, and employees, including our principal executive officer, principal financial officer, principal accounting officer or controller, or persons performing similar functions. Following this offering, a copy of the code will be posted on the Corporate Governance section of our website, which is located at www.stealthbt.com/investors. If we make any substantive amendments to, or grant any waivers from, the code of business conduct and ethics for any officer or director, we will disclose the nature of such amendment or waiver on our website or in a current report onForm 6-K.
160
Table of Contents
Family Relationships
There are no family relationships among any of our directors or executive officers.
Insurance and Indemnification
Every director and officer is indemnified and secured harmless out of our assets and funds against all actions, proceedings, costs, charges, expenses, losses, damages or liabilities incurred or sustained by such director or officer (other than by reason of such director’s or officer’s own dishonesty, willful default or fraud as determined by a court of competent jurisdiction) in or about the conduct of our affairs or in the execution of such director or officer’s duties, powers, authorities or discretions, including any costs, expenses, losses or liabilities incurred by such director or officer in defending (whether successfully or otherwise) any civil proceedings concerning us or our affairs in any court whether Cayman Islands or elsewhere
Insofar as indemnification of liabilities arising under the Securities Act may be permitted to our board, executive officers, or persons controlling us pursuant to the foregoing provisions, we have been informed that, in the opinion of the SEC, such indemnification is against public policy as expressed in the Securities Act and is therefore unenforceable.
161
Table of Contents
Since January 1, 2015 we have engaged in the following transactions with our directors, executive officers or holders of more than 5% of our outstanding share capital and their affiliates, which we refer to as our related parties.
Note Issuances
Between January and April 2015, we borrowed $35.0 million from Morningside Venture (I) Investments Limited, or MVIL, pursuant to a note purchase agreement, or the 2015 Note. As of December 31, 2018, MVIL beneficially owned 98.3% of our outstanding ordinary shares.
In July 2015, we entered into an agreement with MVIL regarding the 2015 Note and other notes we previously issued to MVIL that were then outstanding, or the Conversion Notes. Under this agreement, we issued 54,333,699 Series A convertible preferred shares upon conversion of Conversion Notes in an aggregate principal amount of $115.0 million plus accrued interest. In addition, under this agreement, we issued 32,500,033 Series A convertible preferred shares to MVIL in exchange for a demand note issued to us by MVIL in an aggregate principal amount of $75.0 million, all of which was repaid between July 2015 and December 2016.
Between February and September 2017, pursuant to a note purchase agreement with MVIL, as the same was amended and restated, we issued convertible promissory notes to MVIL in an aggregate principal amount of $50.0 million, or the 2017 Shareholder Notes.
In January 2018, we entered into a note exchange agreement with MVIL pursuant to which MVIL exchanged the 2017 Shareholder Notes for a new convertible note in the principal amount of $52.4 million representing the aggregate principal amount of the 2017 Shareholder Notes plus accrued interest, or the January 2018 Shareholder Note. The January 2018 Shareholder Note accrues interest at 7% per annum, which compounds annually, and upon such compounding, is to be added to the outstanding principal amount. The January 2018 Shareholder Note is convertible upon (i) the closing of an initial public offering or (ii) a subsequent financing occurring after January 10, 2019. Effective upon the closing of a qualified financing, the outstanding principal and accrued interest plus a 25% premium, defined as the sum of principal plus interest multiplied by 25%, will automatically convert into shares of the same class and series of our share capital issued to other investors in the qualified financing. Unless the outstanding amount of the notes are earlier repaid, retired, discharged, or automatically converted into our shares, all amounts outstanding become due and payable on the later of (i) January 10, 2020 and (ii) five business days after the date on which our term loan with Hercules is repaid, terminated and discharged in full.
In October 2018, we entered into a note purchase agreement with MVIL pursuant to which we issued to MVIL three notes in the aggregate principal amount of $30.0 million in October 2018, December 2018 and January 2019. These notes have substantially the same terms as the January 2018 Shareholder Note except that a qualified financing is limited to a U.S. initial public offering.
Warrant Exercise
In December 2009, in connection with our Series A convertible preferred share financing, we issued MVIL a warrant to purchase an aggregate of 333,333 ordinary shares at an exercise price of $0.03 per share. In November 2016, MVIL fully exercised this warrant.
Investor Agreements
In April 2006, we entered into a Subscription and Shareholders Agreement with MVIL and certain other shareholders pursuant to which we agreed to issue ordinary shares and Series A convertible preferred shares and granted certain information rights and observer rights that remain in effect. The Subscription and Shareholders Agreement will terminate upon the completion of this offering. In connection with the Subscription and Shareholders Agreement, we entered into a Registration Rights Agreement with certain of our shareholders, including MVIL, in April 2006 that provided for customary registration rights to holders of our ordinary shares. The Registration Rights Agreement will terminate immediately prior to effectiveness of the registration statement of which this prospectus forms a part.
162
Table of Contents
Indications of Interest to Participate in this Offering
Our existing principal shareholder, Morningside Venture (I) Investments Limited, certain entities associated with it, certain of the holders of our outstanding convertible notes and entities associated with such holders have indicated an interest in purchasing up to an aggregate of approximately $60.0 million of ADSs in this offering at the initial public offering price and on the same terms as the other purchasers in this offering. However, because indications of interest are not binding agreements or commitments to purchase, these persons may determine to purchase fewer ADSs than they indicate an interest in purchasing or not to purchase any ADSs in this offering. It is also possible that these persons could purchase more ADSs in this offering. In addition, the underwriters could determine to sell fewer ADSs to any of these persons than they indicate an interest in purchasing or not to sell any ADSs to such persons. The underwriters will receive the same underwriting discount and commissions on these ADSs as they will on any other ADSs sold to the public in this offering.
Employment Agreements
From January 1, 2014 through March 30, 2016, the services of our former chief executive officer and our current chief executive officer were provided pursuant to an agreement between Morningside Technology Advisory, LLC and us. Pursuant to this agreement, we reimbursed Morningside Technology Advisory, LLC an aggregate of $299,860 during 2015 and $107,500 during 2016. Morningside Technology Advisory, LLC is owned by our current chief executive officer, Ms. McCarthy. Ms. McCarthy and Dr. Chan are directors of our company and Morningside Technology Advisory, LLC.
See “Management—Agreements with Our Executive Officers” for information about agreements between us and our executive officers.
Consulting Agreement
In November 2016, we entered into a consulting agreement with Danforth, an affiliate of Mr. Geffken, our interim Chief Financial Officer. Pursuant to the agreement, Danforth provides us with the CFO services of Mr. Geffken in exchange for fees payable to Danforth. In accordance with the consulting agreement, in January 2017, we issued Danforth a warrant to purchase up to 231,989 ordinary shares at an exercise price of $1.38 per share, which warrant was amended in June 2018 to be an option granted to Mr. Geffken under the 2006 plan. The consulting agreement has been amended to extend the agreement through November 2019.
Indemnification of Officers and Directors
As more fully described in our Articles of Association, our Articles of Association provide that our board of directors and officers shall be indemnified from and against all liability which they incur in execution of their duty in their respective offices out of our assets and funds, except liability incurred by reason of such director’s or officer’s dishonesty, willful deceit or fraud. See the “Management—Insurance and Indemnification” section of this prospectus for a further discussion of these arrangements.
163
Table of Contents
The following table sets forth information with respect to the beneficial ownership of the ordinary shares, as of December 31, 2018 by:
| ∎ | each of our directors; |
| ∎ | each of our executive officers; |
| ∎ | all of our directors and executive officers as a group; and |
| ∎ | each person, or group of affiliated persons, who is known by us to beneficially own more than 5% of the ordinary shares. |
The percentage ownership calculations for beneficial ownership prior to the offering are based on a total of 160,088,346 ordinary shares outstanding as of December 31, 2018, after giving effect to the conversion of all outstanding Series A convertible preferred shares upon the closing of this offering into an aggregate of 91,600,398 ordinary shares. The column entitled “Percentage of Shares Beneficially Owned—After Offering” is based on ordinary shares to be outstanding after this offering, including (i) the ordinary shares represented by the ADSs that we are selling in this offering, and (ii) the issuance of 161,732,652 ordinary shares upon the conversion of our outstanding convertible notes in an aggregate principal amount of $132.4 million, assuming an initial public offering price of $13.00 per ADS (the midpoint of the estimated price range set forth on the cover page of this prospectus).
The number of shares beneficially owned by each shareholder is determined under rules issued by the Securities and Exchange Commission and includes voting or investment power with respect to securities. Under these rules, beneficial ownership includes any shares as to which the individual or entity has sole or shared voting power or investment power. In computing the number of shares beneficially owned by an individual or entity and the percentage ownership of that person, ordinary shares subject to options or other rights held by such person that are currently exercisable or will become exercisable within 60 days of December 31, 2018 are considered outstanding, although such shares subject to options or other rights are not considered outstanding for purposes of computing the percentage ownership of any other person. Unless otherwise indicated, the address of all listed shareholders is c/o Stealth BioTherapeutics Inc., 275 Grove Street,Suite 3-107, Newton, Massachusetts 02466. Each of the shareholders listed has sole voting and investment power with respect to the shares beneficially owned by the shareholder unless noted otherwise, subject to community property laws where applicable.
Our existing principal shareholder, Morningside Venture (I) Investments Limited, certain entities associated with it, certain of the holders of our outstanding convertible notes and entities associated with such holders have indicated an interest in purchasing up to an aggregate of approximately $60.0 million of ADSs in this offering at the initial public offering price and on the same terms as other purchasers in the offering. However, because indications of interest are not binding agreements or commitments to purchase, these persons may determine to purchase fewer ADSs than they indicate an interest in purchasing or not to purchase any ADSs in this offering. It is also possible that these persons could purchase more ADSs in this offering. In addition, the underwriters could determine to sell
164
Table of Contents
fewer ADSs to any of these persons than they indicate an interest in purchasing or not to sell any ADSs to such persons. The following table does not reflect any potential purchase by these shareholders or their affiliated entities.
| SHARES BENEFICIALLY OWNED | PERCENTAGE OF SHARES BENEFICIALLY OWNED | |||||||||||
NAME OF BENEFICIAL OWNER | BEFORE OFFERING | AFTER OFFERING | ||||||||||
5% Shareholders | ||||||||||||
Morningside Venture (I) Investments Limited(1) | 157,880,373 | 98.3 | % | 65.1 | % | |||||||
Executive Officers and Directors | ||||||||||||
Reenie McCarthy(2) | 2,822,222 | 1.7 | % | * | % | |||||||
Daniel E. Geffken(3) | 231,989 | * | % | * | % | |||||||
Mark J. Bamberger, Ph.D.(4) | 661,927 | * | % | * | % | |||||||
Brian D. Blakey, Pharm.D.(5) | 1,041,236 | * | % | * | % | |||||||
James R. Carr, Pharm.D.(6) | 616,490 | * | % | * | % | |||||||
Gerald L. Chan, Sc.D.(7) | 2,500,000 | 1.5 | % | * | % | |||||||
Francis W. Chen, Ph.D.(8) | 50,000 | * | % | * | % | |||||||
Vincent Chueng | — | * | % | * | % | |||||||
Lu Huang, M.D. | — | * | % | * | % | |||||||
Stephen Law(9) | 8,333 | * | % | * | % | |||||||
Kevin F. McLaughlin(10) | 23,958 | * | % | * | % | |||||||
Edward P. Owens(11) | 21,875 | * | % | * | % | |||||||
All executive officers and directors as a group (12 persons)(12) | 7,978,031 | 4.7 | % | 2.0 | % | |||||||
| * | Less than 1%. |
| (1) | Consists of (i) 66,113,309 ordinary shares, (ii) 91,167,065 Series A convertible preferred shares, (iii) 600,000 ordinary shares issuable upon the exercise of options exercisable within 60 days after December 31, 2018 and (iv) following the completion of this offering, 100,431,318 ordinary shares issued upon conversion of convertible notes in an aggregate principal amount of $82.4 million, assuming an initial public offering price of $13.00 per ADS (the midpoint of the estimated price range set forth on the cover page of this prospectus). Louise Mary Garbarino, Jill Marie Franklin, Peter Stuart Allenby Edwards and Raymond Long Sing Tang, the directors of Morningside Venture (I) Investments Limited, or MVIL, share voting and dispositive control over the shares held by MVIL. As a result, Louise Mary Garbarino, Jill Marie Franklin, Peter Stuart Allenby Edwards and Raymond Long Sing Tang may be deemed to possess voting and investment control over, and may be deemed to have indirect beneficial ownership with respect to, all shares held by MVIL. Each of Louise Mary Garbarino, Jill Marie Franklin, Peter Stuart Allenby Edwards and Raymond Long Sing Tang disclaims beneficial ownership of such shares, except to the extent of their respective pecuniary interests therein. The address for MVIL is 2nd Floor, Le Prince de Galles,3-5 Avenue des Citronniers, MC 98000, Monaco. |
| (2) | Consists of 2,822,222 ordinary shares issuable upon the exercise of options exercisable within 60 days after December 31, 2018. |
| (3) | Consists of 231,989 ordinary shares issuable upon the exercise of options exercisable within 60 days after December 31, 2018. |
| (4) | Consists of 661,927 ordinary shares issuable upon the exercise of options exercisable within 60 days after December 31, 2018. |
| (5) | Consists of 1,041,236 ordinary shares issuable upon the exercise of options exercisable within 60 days after December 31, 2018. |
| (6) | Consists of 616,490 ordinary shares issuable upon the exercise of options exercisable within 60 days after December 31, 2018. |
| (7) | Consists of 2,500,000 ordinary shares issuable upon the exercise of options exercisable within 60 days after December 31, 2018. |
| (8) | Consists of 50,000 ordinary shares issuable upon the exercise of options exercisable within 60 days after December 31, 2018. |
| (9) | Consists of 8,333 ordinary shares issuable upon the exercise of options exercisable within 60 days after December 31, 2018. |
| (10) | Consists of 23,958 ordinary shares issuable upon the exercise of options exercisable within 60 days after December 31, 2018. |
| (11) | Consists of 21,875 ordinary shares issuable upon the exercise of options exercisable within 60 days after December 31, 2018. |
| (12) | Consists of 7,978,031 ordinary shares issuable upon the exercise of options exercisable within 60 days after December 31, 2018. |
Holdings by U.S. Shareholders
As of December 31, 2018, approximately 3.0% of our outstanding ordinary shares were held by nine record holders in the United States and less than 1% of our outstanding Series A convertible preferred shares were held by one record holder in the United States.
165
Table of Contents
DESCRIPTION OF SHARE CAPITAL AND ARTICLES OF ASSOCIATION
The following describes our issued share capital, summarizes the material provisions of our Articles of Association and highlights certain differences in corporate law in the Cayman Islands and the United States.
General
We were incorporated in April 2006 under the name of Stealth Peptides International Inc as an exempted company incorporated with limited liability under the laws of the Cayman Islands, and we changed our name in June 2015 to Stealth BioTherapeutics Corp. Our affairs are governed by our Articles of Association, the Companies Law and the common law of the Cayman Islands. The following description of our share capital and provisions of our Articles of Association are summaries and are qualified by reference to the Articles of Association that will be in effect upon the closing of this offering. We have filed copies of these documents as exhibits to our registration statement of which this prospectus forms a part.
Issued Share Capital
Following the closing of this offering, our authorized share capital will be $225,000 divided into 750,000,000 ordinary shares.
As of December 31, 2018, there were 68,487,948 ordinary shares outstanding, par value $0.0003 per share, and 91,600,398 Series A convertible preferred shares outstanding, par value $0.0003 per share.
Articles of Association
Subject to other provisions in our Articles of Association, our shareholders may by ordinary resolution increase our authorized share capital or by special resolution reduce the share capital and amend our Articles of Association.
General
All of our outstanding ordinary shares are fully paid andnon-assessable. No share certificates will be issued in connection with the offering.
The ordinary shares issued upon the completion of the offering are not entitled to any preemptive conversion or redemption rights at the sole option of the holder of ordinary shares. Our shareholders may freely hold and vote their shares (subject to certain restrictions contained in our Articles of Association, such as the process for validly appointing a proxy).
Our board of directors may provide for other classes of shares, including classes of preferred shares, out of our authorized but unissued share capital, which could be utilized for a variety of corporate purposes, including future offerings to raise capital for corporate purposes or for use in employee benefit plans. Such additional classes of shares shall have such rights, restrictions, preferences, privileges and payment obligations as determined by our board of directors. If we issue any preferred shares, the rights, preferences and privileges of holders of our ordinary shares will be subject to, and may be adversely affected by, the rights of the holders of such preferred shares. See “—Variation of rights of Shares.”
Repurchase Rights
Any repurchase of our own shares by us as may be agreed with the relevant shareholders shall be approved by our board of directors in compliance with the Companies Law and our Articles of Association, and we may make a payment in respect of such repurchase in any manner authorized by the Companies Law and our Articles of Association, including out of our capital. A payment out of capital by a Cayman Islands company is not lawful unless immediately following the date on which the payment out of capital is proposed to be made the company shall be able to pay its debts as they fall due in the ordinary course of business. Only shares that are fully paid may be repurchased, and there must be at least one share remaining in issue following the repurchase.
Voting Rights
Voting at any meeting of shareholders is by a poll. Each ordinary share is entitled to one vote.
A quorum required for a meeting of shareholders consists of at least one or more of shareholders present in person or by proxy and entitled to vote representing the holders of at least a majority of all of our issued voting share
166
Table of Contents
capital. Shareholders’ meetings are held annually and may otherwise be convened by our board of directors on its own initiative, with at least 10 days advance notice to the shareholders. Shareholders’ meetings shall also be convened on the requisition in writing of any shareholder or shareholders holding at least a majority of the issued voting share capital, subject to certain procedural requirements. Advance notice of at least 21 days is required for convening extraordinary general meetings.
Any ordinary resolution to be made by our shareholders requires the affirmative vote of a simple majority of the votes attaching to the ordinary shares cast in person or by proxy at a meeting of our shareholders. A special resolution requires the affirmative vote of not less thantwo-thirds of the votes cast in person or by proxy at a meeting of our shareholders. A special resolution is required for certain matters specified in the Companies Law as requiring approval by special resolution, including, without limitation, amending our Articles of Association, reducing our authorized share capital, changing our name, and appointing a voluntary liquidator.
An ordinary resolution or a special resolution may also be adopted by way of unanimous written resolution signed by or on behalf of each shareholder who would have been entitled to vote on such matter at a general meeting without a meeting being held.
Dividends
With the exception of section 34 of the Companies Law, there are no statutory provisions relating to the payment of dividends in the Cayman Islands. Based upon English case law, which is regarded as persuasive in the Cayman Islands, dividends may be paid only out of profits. Section 34 of the Companies Law permits, subject to a solvency test and the provisions, if any, of the company’s memorandum and articles of association, the payment of dividends and distributions out of the share premium account.
Any dividends will be paid to the custodian of the ADSs being issued in this offering and shall be subject to further distribution to you as a beneficial owner of the underlying ordinary shares by the custodian. See “Description of American Depositary Shares—Dividends and Other Distributions.”
Liquidation
On a return of capital on winding up or otherwise (other than on conversion, redemption or purchase of ordinary shares), assets available for distribution among the holders of ordinary shares shall be distributed among the holders of the ordinary shares on a pro rata basis.
Transfer of Shares
Subject to the restrictions of our Articles of Association and the Nasdaq Listing Rules or any relevant securities law, any of our shareholders may transfer all or any of his or her ordinary shares by an instrument of transfer in the usual or common form prescribed by Nasdaq or any other form approved by our board of directors.
Subject to the Nasdaq Listing Rules and any rights or restrictions for time being attached to any share, our board of directors may in their absolute discretion decline to register any transfer of shares.
Subject to our Articles of Association and the Nasdaq Listing Rules and any rights or restrictions for time being attached to any share, the registration of transfers of shares may be suspended and our register of members closed at such times and for such periods as our board of directors may from time to time determine.
Variation of Rights of Shares
The rights attached to any class of shares may, subject to any rights or restrictions attached to any class, be materially adversely varied or abrogated only with written consent of the holders of not less thantwo-thirds of the issued shares of the relevant class or with the sanction of a resolution passed at a separate meeting of the holders of the shares of such class by a majority oftwo-thirds of the votes cast at such a meeting.
The rights conferred upon the shareholders of any class (including, without limitation and for the avoidance of doubt, the ordinary shares) shall not, subject to any rights or restrictions attached to the shares of that class, be deemed to be materially adversely varied or abrogated by, among other things, the creation, allotment or issuance of further shares ranking pari passu with or subsequent to such class or the redemption or purchase of any shares of any class by us.
167
Table of Contents
Inspection of Books and Records
Holders of our ordinary shares have no general right under the Companies Law to inspect or obtain copies of our register of members or our corporate records other than our Articles of Association.
Borrowing Power
Our board of directors may exercise all powers to borrow money and to mortgage or charge our undertaking, property and uncalled capital, to provide for a security interest to be taken in such undertaking, property or uncalled capital, to issue debentures, debenture stock and other securities whenever money is borrowed or as security for any debt, liability or obligation of us or of any third party.
Share Options
As of December 31, 2018, options to purchase 15,871,229 ordinary shares at a weighted-average exercise price of $1.06 per share were outstanding, of which options to purchase 11,868,948 ordinary shares were exercisable, at a weighted-average exercise price of $0.94 per share.
Warrants
In June 2017, we issued a warrant to Hercules to purchase, at the holder’s election, $500,000 of Series A shares or securities issued in a next equity financing, which includes this offering. The exercise price is (a) $2.30769 per Series A share or (b) in the event the holder elects securities issued in this offering, $1.08 (assuming an initial public offering price of $13.00 per ADS, the midpoint of the estimated price range set forth on the cover of this prospectus). Assuming an initial public offering price of $13.00 per ADS (the midpoint of the estimated price range set forth on the cover page of this prospectus), the warrant is exercisable for 38,462 ADS, representing 461,538 ordinary shares underlying such ADSs.
Differences in Corporate Law
DELAWARE | CAYMAN ISLANDS | |||
Title of Organizational Documents | Certificate of Incorporation and Bylaws | Memorandum and Articles of Association | ||
Duties of Directors | Under Delaware law, the business and affairs of a corporation are managed by or under the direction of its board of directors. In exercising their powers, directors are charged with a fiduciary duty of care to protect the interests of the corporation and a fiduciary duty of loyalty to act in the best interests of its shareholders. The duty of care requires that directors act in an informed and deliberative manner and inform themselves, prior to making a business decision, of all material information reasonably available to them. The duty of care also requires that directors exercise care in overseeing and investigating the conduct of the corporation’s employees. The duty of loyalty may be summarized as the duty to act in good faith, not out of self-interest, and in a manner which the director reasonably believes to be in the best interests of the shareholders. | As a matter of Cayman Islands law, directors of Cayman Islands companies owe fiduciary duties to the company which include, amongst other things, a duty to act in good faith in their dealings with or on behalf of the company and exercise their powers and fulfill the duties of their office honestly. Five core duties are:
∎ a duty to act in good faith in what the directorsbona fide consider to be the best interests of the company (and in this regard, it should be noted that the duty is owed to the company and not to associate companies, subsidiaries or holding companies);
∎ a duty not to personally profit from opportunities that arise from the office of director (unless the company permits him to do so);
∎ a duty of trusteeship of the company’s assets;
∎ a duty to avoid conflicts of interest; and | ||
168
Table of Contents
DELAWARE | CAYMAN ISLANDS | |||
∎ a duty to exercise powers for the purpose for which such powers were conferred.
A director of a Cayman Islands company also owes the company a duty to act with skill, care and diligence. A director need not exhibit in the performance of his or her duties a greater degree of skill than may reasonably be expected from a person of his or her knowledge and experience. | ||||
Limitations on Personal Liability of Directors | Subject to the limitations described below, a certificate of incorporation may provide for the elimination or limitation of the personal liability of a director to the corporation or its shareholders for monetary damages for a breach of fiduciary duty as a director.
Such provision cannot limit liability for breach of loyalty, acts or omissions not in good faith, intentional misconduct, unlawful payment of dividends or unlawful share purchase or redemption. In addition, the certificate of incorporation cannot limit liability for any act or omission occurring prior to the date when such provision becomes effective. | The Companies Law has no equivalent provision to Delaware law regarding the limitation of director’s liability. However, as a matter of public policy, Cayman Islands law will not allow the limitation of a director’s liability to the extent that the liability is a consequence of the director committing a crime or of the director’s own fraud, dishonesty or willful default. | ||
Indemnification of Directors, Officers, Agents, and Others | A corporation has the power to indemnify any director, officer, employee, or agent of the corporation who was, is, or is threatened to be made a party who acted in good faith and in a manner they believed to be in the best interests of the corporation, and if with respect to a criminal proceeding, had no reasonable cause to believe his conduct would be unlawful, against amounts actually and reasonably incurred. | Cayman Islands law does not limit the extent to which a company’s articles of association may provide for indemnification of directors and officers, except to the extent any such provision may be held by the Cayman Islands Court to be contrary to public policy, such as to provide indemnification against the consequences of committing a crime, or against the indemnified person’s own fraud, dishonesty or willful default. | ||
Interested Directors | Under Delaware law, a transaction in which a director who has an interest is not void or voidable solely because such interested director is present at or participates in the meeting that authorizes the transaction if: (i) the material facts as to such interested director’s relationship or interests are disclosed or are known to the board of directors and the board in good faith authorizes the transaction by the affirmative vote of a majority of the disinterested directors, even though the disinterested directors are less than a quorum, (ii) such material facts are disclosed or are known to | Under our Articles of Association, directors who are in any way, whether directly or indirectly, interested in a contract or proposed contract with our company must declare the nature of their interest at a meeting of the board of directors. Following such declaration, a director may vote in respect of any contract or proposed contract notwithstanding his interest; provided that, in exercising any such vote, such director’s duties remain as described above. | ||
169
Table of Contents
DELAWARE | CAYMAN ISLANDS | |||
| the shareholders entitled to vote on such transaction and the transaction is specifically approved in good faith by vote of the shareholders, or (iii) the transaction is fair as to the corporation as of the time it is authorized, approved or ratified. Under Delaware law, a director could be held liable for any transaction in which such director derived an improper personal benefit. | ||||
Voting Requirements | The certificate of incorporation may include a provision requiring supermajority approval by the directors or shareholders for any corporate action.
In addition, under Delaware law, certain business combinations involving interested shareholders require approval by a supermajority of thenon-interested shareholders. | As a matter of Cayman Islands law, certain matters must be approved by special resolution of the shareholders, including amending or adopting memorandum or articles of association of a Cayman Islands company, appointment of inspectors to examine company affairs, reduction of share capital (subject, in relevant circumstances, to court approval), change of name, authorization of a plan of merger or transfer by way of continuation to another jurisdiction or consolidation, voluntary winding up of the company or the recalling of the liquidation of the company.
The Companies Law requires that a special resolution be passed by a majority of at leasttwo-thirds or such higher percentage as set forth in the articles of association, of shareholders being entitled to vote and do vote in person or by proxy at a general meeting, or by unanimous written consent of shareholders entitled to vote at a general meeting. Our Articles of Association does not provide for a higher threshold.
The Companies Law defines “special resolutions” only. A company’s articles of association can therefore tailor the definition of “ordinary resolutions” as a whole, or with respect to specific provisions. Our Articles of Association provide that an ordinary resolution is a resolution (i) passed by a simple majority of such shareholders as, being entitled to do so, vote in person (or, where proxies are allowed, by proxy) at a general meeting and regard shall be had in computing a majority to the number of votes to which each shareholder is entitled or (ii) approved in writing by all of the shareholders entitled to vote at a general meeting in one or more instruments each signed by one or more of the shareholders | ||
170
Table of Contents
DELAWARE | CAYMAN ISLANDS | |||
| and the effective date of the resolution so adopted shall be the date on which the instrument (or the last of such instruments, if more than one) is executed. | ||||
Voting for Directors | Under Delaware law, unless otherwise specified in the certificate of incorporation or bylaws of the corporation, directors shall be elected by a plurality of the votes of the shares present in person or represented by proxy at the meeting and entitled to vote on the election of directors. | Our Articles of Association provide that at an annual general meeting where a resolution for the election of directors is proposed in accordance with our Articles of Association, a plurality of the votes cast shall be sufficient to elect a director. | ||
Cumulative Voting | No cumulative voting for the election of directors unless so provided in the certificate of incorporation. | No cumulative voting for the election of directors unless so provided in the articles of association.
Our Articles of Association do not provide for cumulative voting on the election of the directors as described above. | ||
Directors’ Powers Regarding Bylaws | The certificate of incorporation may grant the directors the power to adopt, amend or repeal bylaws. | Our Articles of Association may only be amended by a special resolution of the shareholders. | ||
Nomination and Removal of Directors and Filling Vacancies on Board | Shareholders may generally nominate directors if they comply with advance notice provisions and other procedural requirements in company bylaws. Holders of a majority of the shares may remove a director with or without cause, except in certain cases involving a classified board or if the company uses cumulative voting. Unless otherwise provided for in the certificate of incorporation or bylaws, directorship vacancies are filled by a majority of the directors elected or then in office. | Nomination and removal of directors and filling of board vacancies are governed by the terms of the articles of association.
Our Articles of Association provide that a director shall hold office until such time they resign upon the expiry of a full term of three years, if they are removed from office by ordinary resolution of the shareholders or otherwise in accordance with our Articles of Association. | ||
Mergers and Similar Arrangements | Under Delaware law, with certain exceptions, a merger, consolidation, exchange or sale of all or substantially all the assets of a corporation must be approved by the board of directors and a majority of the outstanding shares entitled to vote thereon. Under Delaware law, a shareholder of a corporation participating in certain major corporate transactions may, under certain circumstances, be entitled to appraisal rights pursuant to which such shareholder may receive cash in the amount of the fair value of the shares held by such shareholder (as determined by a court) in lieu of the consideration such shareholder would otherwise receive in the transaction. | The Companies Law provides for the merger or consolidation of two or more companies into a single entity. The legislation makes a distinction between a “consolidation” and a “merger.” In a consolidation, a new entity is formed from the combination of each participating company, and the separate consolidating parties, as a consequence, cease to exist and are each stricken by the Registrar of Companies. In a merger, one company remains as the surviving entity, having in effect absorbed the other merging parties that then cease to exist.
Two or more Cayman Islands-registered companies may merge or consolidate. Cayman Islands-registered companies may | ||
171
Table of Contents
DELAWARE | CAYMAN ISLANDS | |||
Delaware law also provides that a parent corporation, by resolution of its board of directors, may merge with any subsidiary, of which it owns at least 90% of each class of capital stock without a vote by shareholders of such subsidiary. Upon any such merger, dissenting shareholders of the subsidiary would have appraisal rights. | also merge or consolidate with overseas companies provided that the laws of the foreign jurisdiction permit such merger or consolidation.
A plan of merger or consolidation shall be authorized by each constituent company by way of (i) a special resolution of the members of each such constituent company; and (ii) such other authorization, if any, as may be specified in such constituent company’s articles of association. If one of the constituent companies is an overseas company, a declaration from a director of the overseas company is required to confirm that the merger or consolidation is permitted or not prohibited by the constituent overseas company and by the laws of the jurisdiction in which the overseas company is existing, and that those constitutional documents have been or will be complied with.
Shareholder approval is not required where a parent company registered in the Cayman Islands seeks to merge with one or more of its subsidiaries registered in the Cayman Islands and a copy of the plan of merger is given to every member of each subsidiary company to be merged unless that member agrees otherwise.
Secured creditors must consent to the merger although application can be made to the Cayman Islands Court for such requirement to be waived if such secured creditor does not grant its consent to the merger. Where an overseas company wishes to merge with a Cayman Islands company, consent or approval to the transfer of any security interest granted by the overseas company to the resulting Cayman Islands entity in the transaction is required, unless otherwise released or waived by the secured party. If the merger plan is approved, it is then filed with the Cayman Islands General Registry along with a declaration by a director of each company. The Registrar of Companies will then issue a certificate of merger which shall be prima facie evidence of compliance with all requirements of the Companies Law in respect of the merger or consolidation.
The surviving or consolidated entity remains or becomes active while the other company |
172
Table of Contents
DELAWARE | CAYMAN ISLANDS | |||
or companies are automatically dissolved. Unless the shares of such shareholder are publicly listed or quoted, dissenting shareholders in a merger or consolidation of this type are entitled to payment of the fair value of their shares if such shareholder provides a written objection before the vote on such merger or consolidation. With respect to shares that are listed or quoted, a shareholder shall have similar rights only if it is required by the terms of the merger or consolidation to accept for such shares property other than (i) shares (or depositary receipts in respect thereof) in the surviving or consolidated company; (ii) listed or quoted shares (or depositary receipts in respect thereof) of another company; (iii) cash in lieu of any fractions of shares or depositary receipts described at (i) and (ii); or (iv) any combination of shares, depositary receipts or cash described in (i)—(iii).
Cayman Islands companies may also be restructured or amalgamated under supervision of the Cayman Islands Court by way of a court-sanctioned “scheme of arrangement.” A scheme of arrangement is one of several transactional mechanisms available in the Cayman Islands for achieving a restructuring. Others include share capital exchange, merger (as described above), asset acquisition or control, through contractual arrangements, of an operating business. A Cayman Islands Court scheme of arrangement requires the approval of a majority in number, of each class of shareholders and creditors with whom the arrangement is to be made and who must in addition represent three-fourths in value of each such class of shareholders or creditors, as the case may be, that are present and voting either in person or by proxy at the meeting summoned for that purpose. The convening of the meetings and subsequently the terms of the arrangement must be sanctioned by the Cayman Islands Court. While a dissenting shareholder would have the right to express to the Cayman Islands Court its view that the transaction ought not be approved, the Cayman Islands Court can |
173
Table of Contents
DELAWARE | CAYMAN ISLANDS | |||
be expected to approve the scheme of arrangement if it is satisfied that:
∎ the classes which are required to approve the scheme of arrangement have been properly constituted, so that the members of such classes are properly represented;
∎ the meetings held by the company in relation to the approval of the scheme of arrangement by such classes have been convened and held in accordance with any directions given by the Cayman Islands Court;
∎ the scheme of arrangement has been properly explained to the shareholders or creditors so that they have been able to exercise an informed vote in respect of the scheme; the scheme of arrangement is one which an intelligent and honest man, who is a member of the relevant class and properly acting might approve.
When a takeover offer is made and accepted by holders of 90% of the shares within four months, the offeror may, within atwo-month period following the expiration of the said four month period, require the holders of the remaining shares to transfer such shares on the terms of the offer. An objection may be made to the Cayman Islands Court but is unlikely to succeed unless there is evidence of fraud, bad faith or collusion. If the arrangement and reconstruction are thus approved, any dissenting shareholders would have no rights comparable to appraisal rights, which would otherwise ordinarily be available to dissenting shareholders of U.S. corporations, providing rights to receive payment in cash for the judicially determined value of the shares.
Our Articles of Association provide that we may by special resolution resolve to merge or consolidate in accordance with the Companies Law. | ||||
Shareholder Suits | Class actions and derivative actions generally are available to shareholders under Delaware law for, among other things, breach of | The rights of shareholders under Cayman Islands law are not as extensive as those under Delaware law. Class actions are | ||
174
Table of Contents
DELAWARE | CAYMAN ISLANDS | |||
| fiduciary duty, corporate waste and actions not taken in accordance with applicable law. In such actions, the court generally has discretion to permit the winning party to recover attorneys’ fees incurred in connection with such action. | generally not available to shareholders under Cayman Islands laws; historically, there have not been any reported instances of such class actions having been successfully brought before the Cayman Islands Court. In principle, we will normally be the proper plaintiff and a derivative action may be brought by a minority shareholder in only limited circumstances. In this regard, the Cayman Islands Court would ordinarily be expected to follow English case law precedent, which would permit a shareholder to commence an action in the company’s name to remedy a wrong done to the company where the act complained of cannot be ratified by the shareholders and where control of the company by the wrongdoer results in the company not pursuing a remedy itself. The case law shows that derivative actions have been permitted in respect of acts that are beyond the company’s corporate power, illegal, where the individual rights of the plaintiff shareholder have been infringed or are about to be infringed and acts that are alleged to constitute a “fraud on the minority.” The winning party in such an action generally would be able to recover a portion of attorney’s fees incurred in connection with such action. | |||
Inspection of Corporate Records | Under Delaware law, shareholders of a Delaware corporation have the right during normal business hours to inspect for any proper purpose, and to obtain copies of list(s) of shareholders and other books and records of the corporation and its subsidiaries, if any, to the extent the books and records of such subsidiaries are available to the corporation. | Shareholders of a Cayman Islands exempted company have no general right under Cayman Islands law to inspect or obtain copies of the register of members or other corporate records (other than the register of mortgages or charges) of the company. However, these rights may be provided in the company’s articles of association. Our Articles of Association provide that the holders of our ordinary shares will have no general right to inspect or obtain copies of our register of members or our corporate records other than our Articles of Association. | ||
Shareholder Proposals | Unless provided in the corporation’s certificate of incorporation or bylaws, Delaware law does not include a provision restricting the manner in which shareholders may bring business before a meeting. | The Companies Law does not provide shareholders any right to bring business before a meeting or requisition a general meeting. However, these rights may be provided in the company’s articles of association. | ||
175
Table of Contents
DELAWARE | CAYMAN ISLANDS | |||
Our Articles of Association provide for extraordinary general meeting to be convened on the requisition in writing of any shareholder(s) entitled to attend and vote at our extraordinary general meetings and to exercise at least a majority of the votes permitted to be exercised at any such meeting subject to certain procedural requirements. | ||||
Approval of Corporate Matters by Written Consent | Delaware law permits shareholders to take action by written consent signed by the holders of outstanding shares having not less than the minimum number of votes that would be necessary to authorize or take such action at a meeting of shareholders. | The Companies Law allows a special resolution to be passed in writing only if signed by all the voting shareholders (if authorized by the articles of association). | ||
Calling of Special Shareholders Meetings | Delaware law permits the board of directors or any person who is authorized under a corporation’s certificate of incorporation or bylaws to call a special meeting of shareholders. | The Companies Law does not have provisions governing the proceedings of shareholders meetings which are usually provided in the articles of association.
Our Articles of Association provide for an extraordinary general meeting to be convened on the requisition in writing of any shareholder(s) entitled to attend and vote at our extraordinary general meetings and to exercise at least a majority of the votes permitted to be exercised at any such meeting subject to certain procedural requirements. | ||
Listing on The Nasdaq Global Market
We have applied to list the ADSs on The Nasdaq Global Market under the trading symbol “MITO.”
Registrar
Our register of members, or share register, reflects only record owners of our ordinary shares. Holders of our ADSs will not be treated as one of our shareholders and their names will therefore not be entered in our share register. The depositary, the custodian or their nominees will be the holder of the shares underlying our ADSs. For further discussion on our ADSs and ADS holder rights, see “Description of American Depositary Shares” in this prospectus.
176
Table of Contents
DESCRIPTION OF AMERICAN DEPOSITARY SHARES
Description of American Depositary Shares
Citibank, N.A., or Citibank, has agreed to act as the depositary for the ADSs. Citibank’s depositary offices are located at 388 Greenwich Street, New York, New York 10013. ADSs represent ownership interests in securities that are on deposit with the depositary. ADSs may be represented by certificates that are commonly known as American Depositary Receipts, or ADRs. The depositary typically appoints a custodian to safekeep the securities on deposit. In this case, the custodian is Citibank, N.A.—Hong Kong, located at 9/F, Citi Tower, One Bay East, 83 Hoi Bun Road, Kwun Tong, Kowloon, Hong Kong.
We have appointed Citibank as depositary pursuant to a deposit agreement. A copy of the deposit agreement will be on file with the SEC under cover of a registration statement onForm F-6. You may obtain a copy of the deposit agreement from the SEC’s Public Reference Room at 100 F Street, N.E., Washington, D.C. 20549 and from the SEC’s website (www.sec.gov). Please refer to registration number 333-229509 when retrieving such copy.
We are providing you with a summary description of the material terms of the ADSs and of your material rights as an owner of ADSs. Please note that summaries by their nature lack the precision of the information summarized and the rights and obligations of an owner of ADSs will be determined by reference to the terms of the deposit agreement and not by this summary. We urge you to review the deposit agreement in its entirety. The portions of this summary that are italicized describe matters that may be relevant to ownership of ADSs but may not be contained in the deposit agreement.
Each ADS represents the right to receive, and to exercise the beneficial ownership interests in, 12 ordinary shares that are on deposit with the depositary and/or custodian. An ADS also represents the right to receive, and to exercise the beneficial interests in, any other property received by the depositary or the custodian on behalf of the owner of the ADS but that has not been distributed to the owners of ADSs because of legal restrictions or practical considerations. We and the depositary may agree to change theADS-to-ordinary shares ratio by amending the deposit agreement. This amendment may give rise to, or change, the depositary fees payable by ADS owners. The custodian, the depositary and their respective nominees will hold all deposited property for the benefit of the holders and beneficial owners of ADSs. The deposited property does not constitute the proprietary assets of the depositary, the custodian or their nominees. Beneficial ownership in the deposited property will under the terms of the deposit agreement be vested in the beneficial owners of the ADSs. The depositary, the custodian and their respective nominees will be the record holders of the deposited property represented by the ADSs for the benefit of the holders and beneficial owners of the corresponding ADSs. A beneficial owner of ADSs may or may not be the holder of ADSs. Beneficial owners of ADSs will be able to receive, and to exercise beneficial ownership interests in, the deposited property only through the registered holders of the ADSs, the registered holders of the ADSs (on behalf of the applicable ADS owners) only through the depositary, and the depositary (on behalf of the owners of the corresponding ADSs) directly, or indirectly, through the custodian or their respective nominees, in each case upon the terms of the deposit agreement.
If you become an owner of ADSs, you will become a party to the deposit agreement and therefore will be bound to its terms and to the terms of any ADR that represents your ADSs. The deposit agreement and the ADR specify our rights and obligations as well as your rights and obligations as owner of ADSs and those of the depositary. As an ADS holder you appoint the depositary to act on your behalf in certain circumstances. The deposit agreement and the ADRs are governed by New York law. However, our obligations to the holders of ordinary shares will continue to be governed by the laws of the Cayman Islands, which may be different from the laws of the United States.
In addition, applicable laws and regulations may require you to satisfy reporting requirements and obtain regulatory approvals in certain circumstances. You are solely responsible for complying with such reporting requirements and obtaining such approvals. Neither the depositary, the custodian, us or any of their or our respective agents or affiliates shall be required to take any actions whatsoever on your behalf to satisfy such reporting requirements or obtain such regulatory approvals under applicable laws and regulations.
As an owner of ADSs, we will not treat you as one of our shareholders and you will not have direct shareholder rights. The depositary will hold on your behalf the shareholder rights attached to the ordinary shares underlying your ADSs.
177
Table of Contents
As an owner of ADSs you will be able to exercise the shareholders rights for the ordinary shares represented by your ADSs through the depositary only to the extent contemplated in the deposit agreement. To exercise any shareholder rights not contemplated in the deposit agreement you will, as an ADS owner, need to arrange for the cancellation of your ADSs and become a direct shareholder.
The manner in which you own the ADSs (e.g., in a brokerage account vs. as registered holder, or as holder of certificated vs. uncertified ADSs) may affect your rights and obligations, and the manner in which, and extent to which, the depositary’s services are made available to you. As an owner of ADSs, you may hold your ADSs either by means of an ADR registered in your name, through a brokerage or safekeeping account, or through an account established by the depositary in your name reflecting the registration of uncertificated ADSs directly on the books of the depositary (commonly referred to as the direct registration system or DRS). The direct registration system reflects the uncertificated (book-entry) registration of ownership of ADSs by the depositary. Under the direct registration system, ownership of ADSs is evidenced by periodic statements issued by the depositary to the holders of the ADSs. The direct registration system includes automated transfers between the depositary and The Depository Trust Company, or DTC, the central book-entry clearing and settlement system for equity securities in the United States. If you decide to hold your ADSs through your brokerage or safekeeping account, you must rely on the procedures of your broker or bank to assert your rights as ADS owner. Banks and brokers typically hold securities such as the ADSs through clearing and settlement systems such as DTC. The procedures of such clearing and settlement systems may limit your ability to exercise your rights as an owner of ADSs. Please consult with your broker or bank if you have any questions concerning these limitations and procedures. All ADSs held through DTC will be registered in the name of a nominee of DTC. This summary description assumes you have opted to own the ADSs directly by means of an ADS registered in your name and, as such, we will refer to you as the “holder.” When we refer to “you,” we assume the reader owns ADSs and will own ADSs at the relevant time.
The registration of the ordinary shares in the name of the depositary or the custodian shall, to the maximum extent permitted by applicable law, vest in the depositary or the custodian the record ownership in the applicable ordinary shares with the beneficial ownership rights and interests in such ordinary shares being at all times vested with the beneficial owners of the ADSs representing the ordinary shares. The depositary or the custodian shall at all times be entitled to exercise the beneficial ownership rights in all deposited property, in each case only on behalf of the holders and beneficial owners of the ADSs representing the deposited property.
Dividends and Distributions
As a holder of ADSs, you generally have the right to receive the distributions we make on the securities deposited with the custodian. Your receipt of these distributions may be limited, however, by practical considerations and legal limitations. Holders of ADSs will receive such distributions under the terms of the deposit agreement in proportion to the number of ADSs held as of the specified record date, after deduction of the applicable fees, taxes and expenses.
Distributions of Cash
Whenever we make a cash distribution for the securities on deposit with the custodian, we will deposit the funds with the custodian. Upon receipt of confirmation of the deposit of the requisite funds, the depositary will arrange for the funds received in a currency other than U.S. dollars to be converted into U.S. dollars and for the distribution of the U.S. dollars to the holders, subject to the laws and regulations of the Cayman Islands.
The conversion into U.S. dollars will take place only if practicable and if the U.S. dollars are transferable to the United States. The depositary will apply the same method for distributing the proceeds of the sale of any property (such as undistributed rights) held by the custodian in respect of securities on deposit.
The distribution of cash will be made net of the fees, expenses, taxes and governmental charges payable by holders under the terms of the deposit agreement. The depositary will hold any cash amounts it is unable to distribute in anon-interest bearing account for the benefit of the applicable holders and beneficial owners of ADSs until the distribution can be effected or the funds that the depositary holds must be escheated as unclaimed property in accordance with the laws of the relevant states of the United States.
Distributions of Shares
Whenever we make a free distribution of ordinary shares for the securities on deposit with the custodian, we will deposit the applicable number of ordinary shares with the custodian. Upon receipt of confirmation of such deposit,
178
Table of Contents
the depositary will either distribute to holders new ADSs representing the ordinary shares deposited or modify theADS-to-ordinary shares ratio, in which case each ADS you hold will represent rights and interests in the additional ordinary shares so deposited. Only whole new ADSs will be distributed. Fractional entitlements will be sold and the proceeds of such sale will be distributed as in the case of a cash distribution.
The distribution of new ADSs or the modification of theADS-to-ordinary shares ratio upon a distribution of ordinary shares will be made net of the fees, expenses, taxes and governmental charges payable by holders under the terms of the deposit agreement. In order to pay such taxes or governmental charges, the depositary may sell all or a portion of the new ordinary shares so distributed.
No such distribution of new ADSs will be made if it would violate a law (e.g., the U.S. securities laws) or if it is not operationally practicable. If the depositary does not distribute new ADSs as described above, it may sell the ordinary shares received upon the terms described in the deposit agreement and will distribute the proceeds of the sale as in the case of a distribution of cash.
Distributions of Rights
Whenever we intend to distribute rights to purchase additional ordinary shares, we will give prior notice to the depositary and we will assist the depositary in determining whether it is lawful and reasonably practicable to distribute rights to purchase additional ADSs to holders.
The depositary will establish procedures to distribute rights to purchase additional ADSs to holders and to enable such holders to exercise such rights if it is lawful and reasonably practicable to make the rights available to holders of ADSs, and if we provide all of the documentation contemplated in the deposit agreement (such as opinions to address the lawfulness of the transaction). You may have to pay fees, expenses, taxes and other governmental charges to subscribe for the new ADSs upon the exercise of your rights. The depositary is not obligated to establish procedures to facilitate the distribution and exercise by holders of rights to purchase new ordinary shares other than in the form of ADSs.
The depositary will not distribute the rights to you if:
| ∎ | we do not timely request that the rights be distributed to you or we request that the rights not be distributed to you; or |
| ∎ | we fail to deliver satisfactory documents to the depositary; or |
| ∎ | it is not reasonably practicable to distribute the rights. |
The depositary will sell the rights that are not exercised or not distributed if such sale is lawful and reasonably practicable. The proceeds of such sale will be distributed to holders as in the case of a cash distribution. If the depositary is unable to sell the rights, it will allow the rights to lapse.
Elective Distributions
Whenever we intend to distribute a dividend payable at the election of shareholders either in cash or in additional shares, we will give prior notice thereof to the depositary and will indicate whether we wish the elective distribution to be made available to you. In such case, we will assist the depositary in determining whether such distribution is lawful and reasonably practicable.
The depositary will make the election available to you only if it is reasonably practicable and if we have provided all of the documentation contemplated in the deposit agreement. In such case, the depositary will establish procedures to enable you to elect to receive either cash or additional ADSs, in each case as described in the deposit agreement.
If the election is not made available to you, you will receive either cash or additional ADSs, depending on what a shareholder in the Cayman Islands would receive upon failing to make an election, as more fully described in the deposit agreement.
Other Distributions
Whenever we intend to distribute property other than cash, ordinary shares or rights to purchase additional ordinary shares, we will notify the depositary in advance and will indicate whether we wish such distribution to be made to you. If so, we will assist the depositary in determining whether such distribution to holders is lawful and reasonably practicable.
179
Table of Contents
If it is reasonably practicable to distribute such property to you and if we provide to the depositary all of the documentation contemplated in the deposit agreement, the depositary will distribute the property to the holders in a manner it deems practicable.
The distribution will be made net of fees, expenses, taxes and governmental charges payable by holders under the terms of the deposit agreement. In order to pay such taxes and governmental charges, the depositary may sell all or a portion of the property received.
The depositary willnot distribute the property to you and will sell the property if:
| ∎ | we do not request that the property be distributed to you or if we ask that the property not be distributed to you; or |
| ∎ | we do not deliver satisfactory documents to the depositary; or |
| ∎ | the depositary determines that all or a portion of the distribution to you is not reasonably practicable. |
The proceeds of such a sale will be distributed to holders as in the case of a cash distribution.
Redemption
Whenever we decide to redeem any of the securities on deposit with the custodian, we will notify the depositary in advance. If it is practicable and if we provide all of the documentation contemplated in the deposit agreement, the depositary will provide notice of the redemption to the holders.
The custodian will be instructed to surrender the shares being redeemed against payment of the applicable redemption price. The depositary will convert the redemption funds received into U.S. dollars upon the terms of the deposit agreement and will establish procedures to enable holders to receive the net proceeds from the redemption upon surrender of their ADSs to the depositary. You may have to pay fees, expenses, taxes and other governmental charges upon the redemption of your ADSs. If less than all ADSs are being redeemed, the ADSs to be retired will be selected by lot or on a pro rata basis, as the depositary may determine.
Changes Affecting Ordinary Shares
The ordinary shares held on deposit for your ADSs may change from time to time. For example, there may be a change in nominal or par value,split-up, cancellation, consolidation or any other reclassification of such ordinary shares or a recapitalization, reorganization, merger, consolidation or sale of assets of the Company.
If any such change were to occur, your ADSs would, to the extent permitted by law, represent the right to receive the property received or exchanged in respect of the ordinary shares held on deposit. The depositary may in such circumstances deliver new ADSs to you, amend the deposit agreement, the ADRs and the applicable Registration Statement(s) onForm F-6, call for the exchange of your existing ADSs for new ADSs and take any other actions that are appropriate to reflect as to the ADSs the change affecting the ordinary shares. If the depositary may not lawfully distribute such property to you, the depositary may sell such property and distribute the net proceeds to you as in the case of a cash distribution.
Issuance of ADSs upon Deposit of Ordinary Shares
Upon completion of this offering, the ordinary shares being offered pursuant to this prospectus will be deposited by us with the custodian. Upon receipt of confirmation of such deposit, the depositary will issue ADSs to the underwriters named in this prospectus.
After the closing of this offering, the depositary may create ADSs on your behalf if you or your broker deposit ordinary shares with the custodian. The depositary will deliver these ADSs to the person you indicate only after you pay any applicable issuance fees and any charges and taxes payable for the transfer of the ordinary shares to the custodian. Your ability to deposit ordinary shares and receive ADSs may be limited by the legal considerations in the United States and Cayman Islands applicable at the time of deposit.
The issuance of ADSs may be delayed until the depositary or the custodian receives confirmation that all required approvals have been given and that the ordinary shares have been duly transferred to the custodian. The depositary will only issue ADSs in whole numbers.
180
Table of Contents
When you make a deposit of ordinary shares, you will be responsible for transferring good and valid title to the depositary. As such, you will be deemed to represent and warrant that:
| ∎ | the ordinary shares are duly authorized, validly issued, fully paid,non-assessable and legally obtained; |
| ∎ | all preemptive (and similar) rights, if any, with respect to such ordinary shares have been validly waived or exercised; |
| ∎ | you are duly authorized to deposit the ordinary shares; |
| ∎ | the ordinary shares presented for deposit are free and clear of any lien, encumbrance, security interest, charge, mortgage or adverse claim, and are not, and the ADSs issuable upon such deposit will not be, “restricted securities” (as defined in the deposit agreement); |
| ∎ | the ordinary shares presented for deposit have not been stripped of any rights or entitlements; and |
| ∎ | the deposit of the ordinary shares does not violate any applicable provisions of the Cayman Islands. |
If any of the representations or warranties are incorrect in any way, we and the depositary may, at your cost and expense, take any and all actions necessary to correct the consequences of the misrepresentations.
Transfer, Combination and Split Up of ADRs
As an ADR holder, you will be entitled to transfer, combine or split up your ADRs and the ADSs evidenced thereby. For transfers of ADRs, you will have to surrender the ADRs to be transferred to the depositary and also must:
| ∎ | ensure that the surrendered ADR is properly endorsed or otherwise in proper form for transfer; |
| ∎ | provide such proof of identity and genuineness of signatures as the depositary deems appropriate; |
| ∎ | provide any transfer stamps required by the State of New York or the United States; and |
| ∎ | pay all applicable fees, charges, expenses, taxes and other government charges payable by ADR holders pursuant to the terms of the deposit agreement, upon the transfer of ADRs. |
To have your ADRs either combined or split up, you must surrender the ADRs in question to the depositary with your request to have them combined or split up, and you must pay all applicable fees, charges and expenses payable by ADR holders, pursuant to the terms of the deposit agreement, upon a combination or split up of ADRs.
Withdrawal of Ordinary Shares Upon Cancellation of ADSs
As a holder, you will be entitled to present your ADSs to the depositary for cancellation and then receive the corresponding number of underlying ordinary shares at the custodian’s offices. Your ability to withdraw the ordinary shares held in respect of the ADSs may be limited by the legal considerations in the United States and Cayman Islands applicable at the time of withdrawal. In order to withdraw the ordinary shares represented by your ADSs, you will be required to pay to the depositary the fees for cancellation of ADSs and any charges and taxes payable upon the transfer of the ordinary shares. You assume the risk for delivery of all funds and securities upon withdrawal. Once canceled, the ADSs will not have any rights under the deposit agreement.
If you hold ADSs registered in your name, the depositary may ask you to provide proof of identity and genuineness of any signature and such other documents as the depositary may deem appropriate before it will cancel your ADSs. The withdrawal of the ordinary shares represented by your ADSs may be delayed until the depositary receives satisfactory evidence of compliance with all applicable laws and regulations. Please keep in mind that the depositary will only accept ADSs for cancellation that represent a whole number of securities on deposit.
You will have the right to withdraw the securities represented by your ADSs at any time except for:
| ∎ | temporary delays that may arise because (i) the transfer books for the ordinary shares or ADSs are closed, or (ii) ordinary shares are immobilized on account of a shareholders’ meeting or a payment of dividends; |
| ∎ | obligations to pay fees, taxes and similar charges; |
| ∎ | restrictions imposed because of laws or regulations applicable to ADSs or the withdrawal of securities on deposit; and/or |
| ∎ | other circumstances specifically contemplated by Section I.A.(l) of the General Instructions toForm F-6 (as such General Instructions may be amended from time to time). |
181
Table of Contents
The deposit agreement may not be modified to impair your right to withdraw the securities represented by your ADSs except to comply with mandatory provisions of law.
Voting Rights
As a holder, you generally have the right under the deposit agreement to instruct the depositary to exercise the voting rights for the ordinary shares represented by your ADSs. The voting rights of holders of ordinary shares are described in “Description of Share Capital and Articles of Association—Articles of Association” in this prospectus.
At our request, the depositary will distribute to you any notice of shareholders’ meeting received from us together with information explaining how to instruct the depositary to exercise the voting rights of the securities represented by ADSs. In lieu of distributing such materials, the depositary may distribute to holders of ADSs instructions on how to receive such materials upon request.
If the depositary timely receives voting instructions from a holder of ADSs, it will endeavor to vote the securities (in person or by proxy) represented by the holder’s ADSs as follows:
| ∎ | The depositary will vote (or cause the custodian to vote) the ordinary shares held on deposit in accordance with the voting instructions received from the holders of ADSs. |
| ∎ | Holders of ADSs in respect of which no timely voting instructions have been received shall be deemed to have instructed the depositary to give a discretionary proxy to a person designated by us to vote the ordinary shares represented by such holders’ ADSs; provided, however, that no such discretionary proxy shall be given with respect to any matter to be voted upon as to which we inform the depositary that (a) we do not wish such proxy to be given, (b) substantial opposition exists, or (c) the rights of holders of ordinary shares may be adversely affected. |
Securities for which no voting instructions have been received will not be voted (except as otherwise contemplated in the deposit agreement). Please note that the ability of the depositary to carry out voting instructions may be limited by practical and legal limitations and the terms of the securities on deposit. We cannot assure you that you will receive voting materials in time to enable you to return voting instructions to the depositary in a timely manner.
Fees and Charges
As an ADS holder, you will be required to pay the following fees under the terms of the deposit agreement:
SERVICE | FEE | |
| Issuance of ADSs (e.g., an issuance of ADS upon a deposit of ordinary shares or upon a change in theADS(s)-to-ordinary shares ratio), excluding ADS issuances as a result of distributions of ordinary shares | Up to $0.05 per ADS issued | |
| Cancellation of ADSs (e.g., a cancellation of ADSs for delivery of deposited property or upon a change in theADS(s)-to-ordinary shares ratio) | Up to $0.05 per ADS cancelled | |
| Distribution of cash dividends or other cash distributions (e.g., upon a sale of rights and other entitlements) | Up to $0.05 per ADS held | |
| Distribution of ADSs pursuant to (i) share dividends or other free share distributions, or (ii) exercise of rights to purchase additional ADSs | Up to $0.05 per ADS held | |
| Distribution of securities other than ADSs or rights to purchase additional ADSs (e.g., upon aspin-off) | Up to $0.05 per ADS held | |
| ADS Services | Up to $0.05 per ADS held on the applicable record date(s) established by the depositary | |
182
Table of Contents
As an ADS holder you will also be responsible to pay certain charges such as:
| ∎ | taxes (including applicable interest and penalties) and other governmental charges; |
| ∎ | the registration fees as may from time to time be in effect for the registration of ordinary shares on the share register and applicable to transfers of ordinary shares to or from the name of the custodian, the depositary or any nominees upon the making of deposits and withdrawals, respectively; |
| ∎ | certain cable, telex and facsimile transmission and delivery expenses; |
| ∎ | the expenses and charges incurred by the depositary in the conversion of foreign currency; |
| ∎ | the fees and expenses incurred by the depositary in connection with compliance with exchange control regulations and other regulatory requirements applicable to ordinary shares, ADSs and ADRs; and |
| ∎ | the fees and expenses incurred by the depositary, the custodian or any nominee in connection with the servicing or delivery of deposited property. |
ADS fees and charges for (i) the issuance of ADSs, and (ii) the cancellation of ADSs are charged to the person to whom the ADSs are issued (in the case of ADS issuances) and to the person whose ADSs are cancelled (in the case of ADS cancellations). In the case of ADSs issued by the depositary into DTC, the ADS issuance and cancellation fees and charges may be deducted from distributions made through DTC, and may be charged to the DTC participant(s) receiving the ADSs being issued or the DTC participant(s) holding the ADSs being cancelled, as the case may be, on behalf of the beneficial owner(s) and will be charged by the DTC participant(s) to the account of the applicable beneficial owner(s) in accordance with the procedures and practices of the DTC participants as in effect at the time. ADS fees and charges in respect of distributions and the ADS service fee are charged to the holders as of the applicable ADS record date. In the case of distributions of cash, the amount of the applicable ADS fees and charges is deducted from the funds being distributed. In the case of (i) distributions other than cash and (ii) the ADS service fee, holders as of the ADS record date will be invoiced for the amount of the ADS fees and charges and such ADS fees and charges may be deducted from distributions made to holders of ADSs. For ADSs held through DTC, the ADS fees and charges for distributions other than cash and the ADS service fee may be deducted from distributions made through DTC, and may be charged to the DTC participants in accordance with the procedures and practices prescribed by DTC and the DTC participants in turn charge the amount of such ADS fees and charges to the beneficial owners for whom they hold ADSs.
In the event of refusal to pay the depositary fees, the depositary may, under the terms of the deposit agreement, refuse the requested service until payment is received or may set off the amount of the depositary fees from any distribution to be made to the ADS holder. Certain depositary fees and charges (such as the ADS services fee) may become payable shortly after the closing of the ADS offering. Note that the fees and charges you may be required to pay may vary over time and may be changed by us and by the depositary. You will receive prior notice of such changes. The depositary may reimburse us for certain expenses incurred by us in respect of the ADR program, by making available a portion of the ADS fees charged in respect of the ADR program or otherwise, upon such terms and conditions as we and the depositary agree from time to time.
Amendments and Termination
We may agree with the depositary to modify the deposit agreement at any time without your consent. We undertake to give holders 30 days’ prior notice of any modifications that would materially prejudice any of their substantial rights under the deposit agreement. We will not consider to be materially prejudicial to your substantial rights any modifications or supplements that are reasonably necessary for the ADSs to be registered under the Securities Act or to be eligible for book-entry settlement, in each case without imposing or increasing the fees and charges you are required to pay. In addition, we may not be able to provide you with prior notice of any modifications or supplements that are required to accommodate compliance with applicable provisions of law.
You will be bound by the modifications to the deposit agreement if you continue to hold your ADSs after the modifications to the deposit agreement become effective. The deposit agreement cannot be amended to prevent you from withdrawing the ordinary shares represented by your ADSs (except as permitted by law).
We have the right to direct the depositary to terminate the deposit agreement. Similarly, the depositary may in certain circumstances on its own initiative terminate the deposit agreement. In either case, the depositary must give
183
Table of Contents
notice to the holders at least 30 days before termination. Until termination, your rights under the deposit agreement will be unaffected.
After termination, the depositary will continue to collect distributions received (but will not distribute any such property until you request the cancellation of your ADSs) and may sell the securities held on deposit. After the sale, the depositary will hold the proceeds from such sale and any other funds then held for the holders of ADSs in anon-interest bearing account. At that point, the depositary will have no further obligations to holders other than to account for the funds then held for the holders of ADSs still outstanding (after deduction of applicable fees, taxes and expenses).
In connection with any termination of the deposit agreement, the depositary may make available to owners of ADSs a means to withdraw the ordinary shares represented by ADSs and to direct the depositary of such ordinary shares into an unsponsored American depositary share program established by the depositary. The ability to receive unsponsored American depositary shares upon termination of the deposit agreement would be subject to satisfaction of certain U.S. regulatory requirements applicable to the creation of unsponsored American depositary shares and the payment of applicable depositary fees.
Books of Depositary
The depositary will maintain ADS holder records at its depositary office. You may inspect such records at such office during regular business hours but solely for the purpose of communicating with other holders in the interest of business matters relating to the ADSs and the deposit agreement.
The depositary will maintain in New York facilities to record and process the issuance, cancellation, combination,split-up and transfer of ADSs. These facilities may be closed from time to time, to the extent not prohibited by law.
Limitations on Obligations and Liabilities
The deposit agreement limits our obligations and the depositary’s obligations to you. Please note the following:
| ∎ | We and the depositary are obligated only to take the actions specifically stated in the deposit agreement without negligence or bad faith. |
| ∎ | The depositary disclaims any liability for any failure to carry out voting instructions, for any manner in which a vote is cast or for the effect of any vote, provided it acts in good faith and without negligence and in accordance with the terms of the deposit agreement. |
| ∎ | The depositary disclaims any liability for any failure to determine the lawfulness or practicality of any action, for the content of any document forwarded to you on our behalf or for the accuracy of any translation of such a document, for the investment risks associated with investing in ordinary shares, for the validity or worth of the ordinary shares, for any tax consequences that result from the ownership of ADSs, for the credit-worthiness of any third party, for allowing any rights to lapse under the terms of the deposit agreement, for the timeliness of any of our notices or for our failure to give notice. |
| ∎ | We and the depositary will not be obligated to perform any act that is inconsistent with the terms of the deposit agreement. |
| ∎ | We and the depositary disclaim any liability if we or the depositary are prevented or forbidden from or subject to any civil or criminal penalty or restraint on account of, or delayed in, doing or performing any act or thing required by the terms of the deposit agreement, by reason of any provision, present or future of any law or regulation, or by reason of present or future provision of any provision of our Articles of Association, or any provision of or governing the securities on deposit, or by reason of any act of God or war or other circumstances beyond our control. |
| ∎ | We and the depositary disclaim any liability by reason of any exercise of, or failure to exercise, any discretion provided for in the deposit agreement or in our Articles of Association or in any provisions of or governing the securities on deposit. |
| ∎ | We and the depositary further disclaim any liability for any action or inaction in reliance on the advice or information received from legal counsel, accountants, any person presenting ordinary shares for deposit, any holder of ADSs or authorized representatives thereof, or any other person believed by either of us in good faith to be competent to give such advice or information. |
184
Table of Contents
| ∎ | We and the depositary also disclaim liability for the inability by a holder to benefit from any distribution, offering, right or other benefit that is made available to holders of ordinary shares but is not, under the terms of the deposit agreement, made available to you. |
| ∎ | We and the depositary may rely without any liability upon any written notice, request or other document believed to be genuine and to have been signed or presented by the proper parties. |
| ∎ | We and the depositary also disclaim liability for any consequential or punitive damages for any breach of the terms of the deposit agreement. |
| ∎ | No disclaimer of any Securities Act or Exchange Act liability is intended by any provision of the deposit agreement, in each case to the extent established under applicable U.S. laws. |
Nothing in the deposit agreement gives rise to a partnership or joint venture, or establishes a fiduciary relationship, among us, the depositary bank and you as ADS holder.
Nothing in the deposit agreement precludes Citibank (or its affiliates) from engaging in transactions in which parties adverse to us or the ADS owners have interests, and nothing in the deposit agreement obligates Citibank to disclose those transactions, or any information obtained in the course of those transactions, to us or to the ADS owners, or to account for any payment received as part of those transactions.
Taxes
You will be responsible for the taxes and other governmental charges payable on the ADSs and the securities represented by the ADSs. We, the depositary and the custodian may deduct from any distribution the taxes and governmental charges payable by holders and may sell any and all property on deposit to pay the taxes and governmental charges payable by holders. You will be liable for any deficiency if the sale proceeds do not cover the taxes that are due.
The depositary may refuse to issue ADSs, to deliver, transfer, split and combine ADRs or to release securities on deposit until all taxes and charges are paid by the applicable holder. The depositary and the custodian may take reasonable administrative actions to obtain tax refunds and reduced tax withholding for any distributions on your behalf. However, you may be required to provide to the depositary and to the custodian proof of taxpayer status and residence and such other information as the depositary and the custodian may require to fulfill legal obligations. You are required to indemnify us, the depositary and the custodian for any claims with respect to taxes based on any tax benefit obtained for you.
Foreign Currency Conversion
The depositary will arrange for the conversion of all foreign currency received into U.S. dollars if such conversion is practical, and it will distribute the U.S. dollars in accordance with the terms of the deposit agreement. You may have to pay fees and expenses incurred in converting foreign currency, such as fees and expenses incurred in complying with currency exchange controls and other governmental requirements.
If the conversion of foreign currency is not practical or lawful, or if any required approvals are denied or not obtainable at a reasonable cost or within a reasonable period, the depositary may take the following actions in its discretion:
| ∎ | Convert the foreign currency to the extent practical and lawful and distribute the U.S. dollars to the holders for whom the conversion and distribution is lawful and practical. |
| ∎ | Distribute the foreign currency to holders for whom the distribution is lawful and practical. |
| ∎ | Hold the foreign currency (without liability for interest) for the applicable holders. |
185
Table of Contents
Governing Law/Waiver of Jury Trial
The deposit agreement, the ADRs and the ADSs will be interpreted in accordance with the laws of the State of New York. The rights of holders of ordinary shares (including ordinary shares represented by ADSs) is governed by the laws of the Cayman Islands.
AS A PARTY TO THE DEPOSIT AGREEMENT, YOU IRREVOCABLY WAIVE YOUR RIGHT TO TRIAL BY JURY, TO THE FULLEST EXTENT PERMITTED BY APPLICABLE LAW, IN ANY LEGAL PROCEEDING ARISING OUT OF THE DEPOSIT AGREEMENT OR THE ADRs AGAINST US AND/OR THE DEPOSITARY.
186
Table of Contents
SHARES AND ADSs ELIGIBLE FOR FUTURE SALE
Prior to this offering, there has been no public market for the ordinary shares or the ADSs, and a liquid trading market for the ADSs may not develop or be sustained after this offering. Future sales of substantial amounts of the ADSs in the public market, including shares issued upon exercise of outstanding options, or the anticipation of these sales, could adversely affect market prices prevailing from time to time and could impair our ability to raise capital through sales of equity securities.
Based upon the 68,487,948 ordinary shares that were outstanding on December 31, 2018, upon the closing of this offering, we will have 396,220,998 outstanding ordinary shares, which include 74,400,000 ordinary shares represented by ADSs, after giving effect to (i) this offering, (ii) the conversion of all outstanding Series A convertible preferred shares into 91,600,398 ordinary shares upon the closing of this offering and (iii) the issuance of 161,732,652 ordinary shares upon the conversion of our outstanding convertible notes in an aggregate principal amount of $132.4 million, assuming an initial public offering price of $13.00 per ADS (the midpoint of the estimated price range set forth on the cover page of this prospectus), upon the closing of this offering.
Of the ADSs to be outstanding immediately after the closing of this offering, we expect that the ADSs to be sold in this offering will be freely tradable without restriction under the Securities Act unless purchased by our “affiliates,” as that term is defined in Rule 144 under the Securities Act. The remaining ordinary shares outstanding after this offering will be “restricted securities” under Rule 144, and we expect that substantially all of these restricted securities will be subject to the180-daylock-up period under thelock-up agreements as described below. These restricted securities may be sold in the public market only if registered or pursuant to an exemption from registration, such as Rule 144 or Rule 701 under the Securities Act.
Rule 144
In general, under Rule 144, beginning 90 days after the date of this prospectus, any person who is not our affiliate and has held their securities for at least six months, including the holding period of any prior owner other than one of our affiliates, may sell securities without restriction, subject to the availability of current public information about us. In addition, under Rule 144, any person who is not our affiliate and has not been our affiliate at any time during the preceding three months and has held their securities for at least one year, including the holding period of any prior owner other than one of our affiliates, would be entitled to sell an unlimited number of shares immediately upon the closing of this offering without regard to whether current public information about us is available.
Beginning 90 days after the date of this prospectus, a person who is our affiliate or who was our affiliate at any time during the preceding three months may sell any unrestricted securities, as well as restricted securities that the person has beneficially owned for at least six months, including the holding period of any prior owner other than one of our affiliates, under Rule 144. Affiliates selling restricted or unrestricted securities may sell a number of securities within any three-month period that does not exceed the greater of:
| ∎ | 1% of the number of ordinary shares then outstanding, which will equal approximately 3,962,210 ordinary shares, or 330,184 ADSs, immediately after this offering; and |
| ∎ | the average weekly trading volume of the ordinary shares in the form of ADSs on The Nasdaq Global Market during the four calendar weeks preceding the filing of a Notice of Proposed Sale of Securities Pursuant to Rule 144 with respect to the sale. |
Sales under Rule 144 by our affiliates are also subject to manner of sale provisions and notice requirements and to the availability of current public information about us.
Rule 701
In general, under Rule 701 of the Securities Act, any of our employees, consultants, or advisors, other than our affiliates, who purchased shares from us in connection with a qualified compensatory stock plan or other written agreement is eligible to resell these shares 90 days after the date of this prospectus in reliance on Rule 144, but without compliance with the holding period requirements of Rule 144 and without regard to the volume of such
187
Table of Contents
sales or the availability of public information about us. Rule 701 permits affiliates to sell their Rule 701 shares under Rule 144 without complying with the holding period requirements of Rule 144. Subject to the180-daylock-up period described below, approximately 41,306 ordinary shares will be eligible for sale in accordance with Rule 701.
Regulation S
Regulation S under the Securities Act provides that ordinary shares owned by any person may be sold without registration in the United States, provided that the sale is effected in an offshore transaction and no directed selling efforts are made in the United States (as these terms are defined in Regulation S), subject to certain other conditions. In general, this means that our ordinary shares may be sold in some other manner outside the United States without requiring registration in the United States.
Lock-Up Agreements
We and our directors and executive officers, and holders of substantially all of our outstanding equity securities, have agreed with the underwriters, subject to certain exceptions, not to, during the180-day period following the date of the final prospectus for this offering, offer, sell, contract to sell, pledge, grant any option to purchase, make any short sale or otherwise dispose of any ordinary shares, ADSs or any options or warrants to purchase any ordinary shares, or any securities convertible into, exchangeable for or that represent the right to receive any ordinary shares, except with the prior written consent of Jefferies LLC and Evercore Group L.L.C. on behalf of the underwriters. Jefferies LLC and Evercore Group L.L.C. may, in their sole discretion, release all or some portion of the securities subject tolock-up agreements prior to the expiration of thelock-up period.
Thelock-up restrictions and specified exceptions are described in more detail under “Underwriting.”
Share Options and Warrant
As of December 31, 2018, we had outstanding options to purchase 15,871,229 ordinary shares, of which options to purchase 11,868,948 shares were vested. Following this offering, we intend to file one or more registration statements onForm S-8 under the Securities Act to register all of the ordinary shares subject to outstanding options and options and other awards issuable pursuant to the 2019 plan, the ESPP and our 2006 plan. Shares covered by these registration statements will then be eligible for sale in the public markets, subject to vesting restrictions, any applicablelock-up agreements described above and Rule 144 limitations applicable to affiliates.
As of December 31, 2018, we had an outstanding warrant to purchase Series A convertible preferred shares or other shares issued by us in a qualified financing. This warrant will become a warrant to purchase 38,462 ADSs, representing 461,538 ordinary shares, upon closing of this offering. Any shares acquired through the exercise of this warrant will be eligible for sale subject to thelock-up agreements and securities laws described above.
188
Table of Contents
Material U.S. Federal Income Tax Considerations for U.S. Holders
The following discussion describes the material U.S. federal income tax consequences relating to the ownership and disposition of our ordinary shares or ADSs by U.S. Holders (as defined below). This discussion applies to U.S. Holders that purchase our ADSs pursuant to this offering and hold such ADSs as a capital asset (generally, property held for investment). This discussion is based on the U.S. Internal Revenue Code of 1986, as amended, or the Code, administrative pronouncements, judicial decisions, and final, temporary, and proposed U.S. Treasury Regulations, all as in effect on the date hereof and all of which are subject to change, possibly with retroactive effect. This discussion does not address all of the U.S. federal income tax consequences that may be relevant to specific U.S. Holders in light of their particular circumstances, including state and local tax consequences, estate tax consequences, alternative minimum tax consequences, and tax consequences applicable to U.S. Holders subject to special rules, such as:
| ∎ | banks, insurance companies, and certain other financial institutions; |
| ∎ | U.S. expatriates and certain former citizens or long-term residents of the United States; |
| ∎ | dealers or traders in securities who use amark-to-market method of tax accounting; |
| ∎ | persons holding ordinary shares or ADSs as part of a hedging transaction, “straddle,” wash sale, conversion transaction or integrated transaction or persons entering into a constructive sale with respect to ordinary shares or ADSs; |
| ∎ | persons whose “functional currency” for U.S. federal income tax purposes is not the U.S. dollar; |
| ∎ | brokers, dealers or traders in securities, commodities or currencies; |
| ∎ | tax-exempt entities or government organizations; |
| ∎ | S corporations, partnerships or other entities or arrangements classified as partnerships for U.S. federal income tax purposes; |
| ∎ | regulated investment companies or real estate investment trusts; |
| ∎ | persons who acquired our ordinary shares or ADSs pursuant to the exercise of any employee share option or otherwise as compensation; |
| ∎ | persons that own or are deemed to own ten percent or more of our shares; and |
| ∎ | persons holding our ordinary shares or ADSs in connection with a trade or business, permanent establishment, or fixed base outside the United States. |
If an entity treated as a partnership for U.S. federal income tax purposes holds our ordinary shares or ADSs, the U.S. federal income tax consequences relating to an investment in such ordinary shares or ADSs will depend upon the status of the partner and the activities of the partnership.
A “U.S. Holder” is a holder who, for U.S. federal income tax purposes, is a beneficial owner of ordinary shares or ADSs and is:
| ∎ | an individual who is a citizen or resident of the United States; |
| ∎ | a corporation, or other entity taxable as a corporation, created or organized in or under the laws of the United States, any state thereof, or the District of Columbia; |
| ∎ | an estate the income of which is subject to U.S. federal income tax regardless of its source; or |
| ∎ | a trust if (i) a U.S. court is able to exercise primary supervision over the administration of the trust and one or more U. S. persons have authority to control all substantial decisions of the trust or (ii) the trust has made a valid election to be treated as a U.S. person under applicable U.S. Treasury Regulations. |
Persons considering an investment in our ADSs should consult their own tax advisors as to the particular tax consequences applicable to them relating to the purchase, ownership and disposition of our ADSs, including the applicability of U.S. federal, state and local tax laws andnon-U.S. tax laws.
The discussion below assumes that the representations contained in the deposit agreement are true and that the obligations in the deposit agreement and any related agreement will be complied with in accordance with their
189
Table of Contents
terms. Generally, a holder of an ADS should be treated for U.S. federal income tax purposes as holding the ordinary shares represented by the ADS. Accordingly, no gain or loss will be recognized upon an exchange of ADSs for the underlying ordinary shares represented by such ADSs. The U.S. Treasury has expressed concerns that intermediaries in the chain of ownership between the holder of an ADS and the issuer of the security underlying the ADS may be taking actions that are inconsistent with the beneficial ownership of the underlying security. Accordingly, the creditability of foreign taxes, if any, as described below, could be affected by actions taken by intermediaries in the chain of ownership between the holders of ADSs and our company if as a result of such actions the holders of ADSs are not properly treated as beneficial owners of the underlying ordinary shares.
Passive Foreign Investment Company Rules
We are a foreign corporation, within the meaning of the Code. If we are classified as a passive foreign investment company, or PFIC, in any taxable year, a U.S. Holder will be subject to special rules generally intended to reduce or eliminate any benefits from the deferral of U.S. federal income tax that a U.S. Holder could derive from investing in anon-U.S. company that does not distribute all of its earnings on a current basis.
Anon-U.S. corporation will be classified as a PFIC for any taxable year in which, after applying certain look-through rules, either:
| ∎ | at least 75% of its gross income is “passive income” (the “PFIC income test”); or |
| ∎ | on average at least 50% of its assets, determined on a quarterly basis, are assets that produce passive income or are held for the production of passive income (the “PFIC asset test”). |
Passive income for this purpose generally includes, among other things, dividends, interest, royalties, rents, and gains from the sale or exchange of property that gives rise to passive income. Assets that produce or are held for the production of passive income generally include cash, even if held as working capital or raised in a public offering, marketable securities, and other assets that may produce passive income. Generally, in determining whether anon-U.S. corporation is a PFIC, a proportionate share of the income and assets of each corporation in which it owns, directly or indirectly, at least a 25% interest (by value) is taken into account.
Based on our estimated gross income and the average value of our gross assets, taking into account the initial public offering price of the ADSs in this offering and the expected price of the ADSs following this offering, and the nature of our business, we do not believe that we were a PFIC for our tax year ended December 31, 2017, and do not expect to be a PFIC during our tax year ending December 31, 2018. However, there can be no assurance that we will not be classified as a PFIC for the current taxable year or any prior or future taxable year. The determination of whether we are a PFIC is a fact-intensive determination made on an annual basis and the applicable law is subject to varying interpretation.
A separate determination must be made after the close of each taxable year as to whether we are a PFIC for that year. As a result, our PFIC status may change from year to year. The total value of our assets for purposes of the PFIC asset test generally will be calculated using the market price of our ordinary shares or ADSs, which may fluctuate considerably. Fluctuations in the market price of the ordinary shares or ADSs may result in our being a PFIC for any taxable year.
If we are a PFIC in any taxable year during which a U.S. Holder owns our ordinary shares or ADSs, the U.S. Holder could be liable for additional taxes and interest charges under the “PFIC excess distribution regime” upon (i) a distribution paid during a taxable year that is greater than 125% of the average annual distributions paid in the three preceding taxable years, or, if shorter, the U.S. Holder’s holding period for our ordinary shares or ADSs, and (ii) any gain recognized on a sale, exchange or other disposition, including a pledge, of our ordinary shares or ADSs, whether or not we continue to be a PFIC. Under the PFIC excess distribution regime, the tax on such distribution or gain would be determined by allocating the distribution or gain ratably over the U.S. Holder’s holding period for our ordinary shares or ADSs. The amount allocated to the current taxable year (i.e., the year in which the distribution occurs or the gain is recognized) and any year prior to the first taxable year in which we are a PFIC will be taxed as ordinary income earned in the current taxable year. The amount allocated to other taxable years will be taxed at the highest marginal rates in effect for individuals or corporations, as applicable, to ordinary income for each such taxable year, and an interest charge, generally applicable to underpayments of tax, will be added to the tax.
190
Table of Contents
If we are classified as a PFIC for any year during which a U.S. Holder holds our ordinary shares or ADSs, we must generally continue to be treated as a PFIC by that holder for all succeeding years during which the U.S. Holder holds such ordinary shares or ADSs, regardless of whether we continue to meet the tests described above, unless we cease to be a PFIC and the U.S. Holder makes a “deemed sale” election under the PFIC rules with respect to our ordinary shares or ADSs. If the “deemed sale” election is made, the U.S. Holder will be deemed to have sold our ordinary shares or ADSs it holds at their fair market value on the last day of the last taxable year in which we qualified as a PFIC, and any gain recognized from such deemed sale would be taxed under the PFIC excess distribution regime. After the deemed sale election, the U.S. Holder’s ordinary shares or ADSs would not be treated as shares of a PFIC unless we subsequently become a PFIC. If we are a PFIC for any taxable year during which a U.S. Holder holds our ordinary shares or ADSs, and one of ournon-U.S. subsidiaries is also a PFIC (i.e., a lower-tier PFIC), such U.S. Holder would be treated as owning a proportionate amount (by value) of the shares of the lower-tier PFIC and would be taxed under the PFIC excess distribution regime on distributions by the lower-tier PFIC and on gain from the disposition of shares of the lower-tier PFIC even though such U.S. Holder would not receive the proceeds of those distributions or dispositions. Any of ournon-U.S. subsidiaries that have elected to be disregarded as entities separate from us or as partnerships for U.S. federal income tax purposes would not be corporations under U.S. federal income tax law and accordingly, cannot be classified as lower-tier PFICs. However,non-U.S. subsidiaries that have not made such election may be classified as lower-tier PFICs if we are a PFIC during a U.S. Holder’s holding period and the subsidiary meets the PFIC income test or PFIC asset test.
If we are a PFIC, a U.S. Holder will not be subject to tax under the PFIC excess distribution regime on distributions or gain recognized on our ordinary shares or ADSs if a valid“mark-to-market” election is made by the U.S. Holder for our ordinary shares or ADSs, provided that the ordinary shares or ADSs are “marketable.” Our ordinary shares or ADSs will be considered marketable if they are “regularly traded” on a “qualified exchange” within the meaning of applicable U.S. Treasury Regulations. A class of stock is regularly traded during any calendar year during which such class of stock is traded, other than in de minimis quantities, on at least 15 days during each calendar quarter. Our ADSs will be marketable as long as they remain listed on The Nasdaq Global Market and are regularly traded. Amark-to-market election will not apply to our ordinary shares or ADSs for any taxable year during which we are not a PFIC, but will remain in effect with respect to any subsequent taxable year in which we become a PFIC. Such election will not apply to any of ournon-U.S. subsidiaries. Accordingly, a U.S. Holder may continue to be subject to tax under the PFIC excess distribution regime with respect to any lower-tier PFICs notwithstanding the U.S. Holder’smark-to-market election for our ordinary shares or ADSs.
An electing U.S. Holder generally must take into account as ordinary income each year an amount equal to the excess, if any, of the fair market value of our ordinary shares or ADSs held at the end of such taxable year over the adjusted tax basis of such ordinary shares or ADSs. The U.S. Holder may also claim an ordinary loss deduction for the excess, if any, of the U.S. Holder’s adjusted tax basis of such ordinary shares or ADSs over their fair market value at the end of the taxable year, but only to the extent of any netmark-to-market gains for prior years. The U.S. Holder’s tax basis in our ordinary shares or ADSs would be adjusted to reflect any income or loss recognized as a result of themark-to-market election. Any gain from a sale, exchange or other disposition of our ordinary shares or ADSs in any taxable year in which we are a PFIC would be treated as ordinary income and any loss from such sale, exchange or other disposition would be treated first as ordinary loss (to the extent of any netmark-to-market gains for prior years) and thereafter as capital loss. If, after having been a PFIC for a taxable year, we cease to be classified as a PFIC because we no longer meet the PFIC income or PFIC asset test, the U.S. Holder would not be required to take into account any latent gain or loss in the manner described above and any gain or loss recognized on the sale or exchange of the ordinary shares or ADSs would be classified as a capital gain or loss. Once made, the election cannot be revoked without the consent of the Internal Revenue Service, or the IRS, unless the ADSs cease to be marketable.
The tax consequences that would apply if we are a PFIC would also be different from those described above if a U.S. Holder were able to make a valid qualified electing fund, or QEF, election. As we do not expect to provide U.S. Holders with the information necessary for a U.S. Holder to make a QEF election, prospective investors should assume that a QEF election will not be available.
Unless otherwise provided by the U.S. Treasury, each U.S. shareholder of a PFIC is required to file an annual report containing such information as the U.S. Treasury may require. A U.S. Holder’s failure to file the annual report will
191
Table of Contents
cause the statute of limitations for such U.S. Holder’s U.S. federal income tax return to remain open with regard to the items required to be included in such report until three years after the U.S. Holder files the annual report, and, unless such failure is due to reasonable cause and not willful neglect, the statute of limitations for the U.S. Holder’s entire U.S. federal income tax return will remain open during such period.
Distributions
While we do not expect to pay any dividends in the near future, in the event any dividends are paid, subject to the discussion above under “Passive Foreign Investment Company Rules,” a U.S. Holder that receives a distribution with respect to our ordinary shares or ADSs generally will be required to include the gross amount of such distribution in gross income as a dividend when actually or constructively received to the extent of the U.S. Holder’s pro rata share of our current and/or accumulated earnings and profits (as determined under U.S. federal income tax principles). To the extent a distribution received by a U.S. Holder is not a dividend because it exceeds the U.S. Holder’s pro rata share of our current and accumulated earnings and profits, it will be treated first as atax-free return of capital and reduce (but not below zero) the adjusted tax basis of the U.S. Holder’s ordinary shares or ADSs. To the extent the distribution exceeds the adjusted tax basis of the U.S. Holder’s ordinary shares or ADSs, the remainder will be taxed as capital gain. Because we may not account for our earnings and profits in accordance with U.S. federal income tax principles, U.S. Holders should expect all distributions to be reported to them as dividends. Subject to applicable limitations, dividends paid to certainnon-corporate U.S. Holders may be taxable at preferential rates applicable to “qualified dividend income.” However, the qualified dividend income treatment may not apply if we are treated as a PFIC with respect to the U.S. Holder. Distributions on our ordinary shares or ADSs that are treated as dividends generally will constitute income from sources outside the United States for foreign tax credit purposes and generally will constitute passive category income. Such dividends will not be eligible for the “dividends received’’ deduction generally allowed to corporate shareholders with respect to dividends received from U.S. corporations.
Dividends will be included in a U.S. Holder’s income on the date of the Depositary’s receipt of the dividend. The amount of any dividend income paid in foreign currency will be the U.S. dollar amount calculated by reference to the exchange rate in effect on the date of actual or constructive receipt, regardless of whether the payment is in fact converted into U.S. dollars. If the dividend is converted into U.S. dollars on the date of receipt, a U.S. Holder should not be required to recognize foreign currency gain or loss with respect to the dividend income. A U.S. Holder may have foreign currency gain or loss if the dividend is converted into U.S. dollars after the date of receipt.
Sale, Exchange or Other Disposition of Our Ordinary Shares or ADSs
Subject to the discussion above under “Passive Foreign Investment Company Rules,’’ a U.S. Holder generally will recognize capital gain or loss for U.S. federal income tax purposes upon the sale, exchange or other disposition of our ordinary shares or ADSs in an amount equal to the difference, if any, between the amount realized (i.e., the amount of cash plus the fair market value of any property received) on the sale, exchange or other disposition and such U.S. Holder’s adjusted tax basis in the ordinary shares or ADSs. Such capital gain or loss generally will be long-term capital gain taxable at a reduced rate fornon-corporate U.S. Holders or long-term capital loss if, on the date of sale, exchange or other disposition, the ordinary shares or ADSs were held by the U.S. Holder for more than one year. Any capital gain of anon-corporate U.S. Holder that is not long-term capital gain is taxed at ordinary income rates. The deductibility of capital losses is subject to limitations. Any gain or loss recognized from the sale or other disposition of our ordinary shares or ADSs will generally be gain or loss from sources within the United States for U.S. foreign tax credit purposes.
Medicare Tax
Certain U.S. Holders that are individuals, estates or trusts and whose income exceeds certain thresholds generally are subject to a 3.8% tax on all or a portion of their net investment income, which may include their gross dividend income and net gains from the disposition of our ordinary shares or ADSs.
Information Reporting and Backup Withholding
U.S. Holders may be required to file certain U.S. information reporting returns with the IRS with respect to an investment in our ordinary shares or ADSs, including, among others, IRS Form 8938 (Statement of Specified Foreign Financial Assets). As described above under “Passive Foreign Investment Company Rules,” each U.S. Holder who is a shareholder of a PFIC must file an annual report containing certain information. U.S. Holders paying more than $100,000 for our ordinary shares or ADSs may be required to file IRS Form 926 (Return by a U.S. Transferor of
192
Table of Contents
Property to a Foreign Corporation) reporting this payment. Substantial penalties may be imposed upon a U.S. Holder that fails to timely comply with the required information reporting.
Dividends on and proceeds from the sale or other disposition of our ADSs may be reported to the IRS unless the U.S. Holder establishes a basis for exemption. Backup withholding may apply to amounts subject to reporting if the holder (i) fails to provide an accurate U.S. taxpayer identification number or otherwise establish a basis for exemption, or (ii) is described in certain other categories of persons. However, U.S. Holders that are corporations generally are excluded from these information reporting and backup withholding tax rules.
Backup withholding is not an additional tax. Any amounts withheld under the backup withholding rules generally will be allowed as a refund or a credit against a U.S. Holder’s U.S. federal income tax liability if the required information is furnished by the U.S. Holder on a timely basis to the IRS.
Cayman Islands Taxation
Prospective investors should consult their professional advisers on the possible tax consequences of buying, holding or selling any ADSs under the laws of their country of citizenship, residence or domicile.
The following is a discussion on certain Cayman Islands income tax consequences of an investment in the ADSs. The discussion is a general summary of present law, which is subject to prospective and retroactive change. It is not intended as tax advice, does not consider any investor’s particular circumstances, and does not consider tax consequences other than those arising under Cayman Islands law.
No stamp duty, capital duty, registration or other issue or documentary taxes are payable in the Cayman Islands on the creation, issuance or delivery of the ADSs. The Cayman Islands currently have no form of income, corporate or capital gains tax and no estate duty, inheritance tax or gift tax. There are currently no Cayman Islands’ taxes or duties of any nature on gains realized on a sale, exchange, conversion, transfer or redemption of the ADSs. Payments of dividends and capital in respect of the ADSs or ordinary shares will not be subject to taxation in the Cayman Islands and no withholding will be required on the payment of interest and principal or a dividend or capital to any holder of the ADSs, nor will gains derived from the disposal of the ADSs be subject to Cayman Islands income or corporation tax as the Cayman Islands currently have no form of income or corporation taxes.
Pursuant to section 6 of the Tax Concessions Law (2018 Revision) of the Cayman Islands, we have obtained an undertaking from theGovernor-in-Cabinet:
| ∎ | that no law which is enacted in the Cayman Islands imposing any tax to be levied on profits, income, gains or appreciation shall apply to us or our operations; and |
| ∎ | that no such tax or any tax in the nature of estate duty or inheritance tax shall be payable on or in respect of the ADSs or ordinary shares, debentures or other obligations of ours. |
The undertaking for the Company is for a period of twenty years from April 11, 2006.
193
Table of Contents
Subject to the terms and conditions set forth in the underwriting agreement, dated , 2019 between us and Jefferies LLC, Evercore Group L.L.C. and BMO Capital Markets Corp. as the representatives of the underwriters named below and the joint book-running managers of this offering, we have agreed to sell to the underwriters, and each of the underwriters has agreed, severally and not jointly, to purchase from us, the respective number of ADSs shown opposite its name below:
UNDERWRITER | NUMBER OF ADSs | |||
Jefferies LLC | ||||
Evercore Group L.L.C. | ||||
BMO Capital Markets Corp. | ||||
Nomura Securities International, Inc. | ||||
|
| |||
Total | 6,200,000 | |||
|
| |||
The underwriting agreement provides that the obligations of the several underwriters are subject to certain conditions precedent such as the receipt by the underwriters of officers’ certificates and legal opinions and approval of certain legal matters by their counsel. The underwriting agreement provides that the underwriters will purchase all of the ADSs if any of them are purchased. If an underwriter defaults, the underwriting agreement provides that the purchase commitments of the nondefaulting underwriters may be increased or the underwriting agreement may be terminated. We have agreed to indemnify the underwriters and certain of their controlling persons against certain liabilities, including liabilities under the Securities Act, and to contribute to payments that the underwriters may be required to make in respect of those liabilities.
Our existing principal shareholder, Morningside Venture (I) Investments Limited, certain entities associated with it, certain of the holders of our outstanding convertible notes and entities associated with such holders have indicated an interest in purchasing up to an aggregate of approximately $60.0 million of ADSs in this offering at the initial public offering price and on the same terms as the other purchasers in this offering. However, because indications of interest are not binding agreements or commitments to purchase, these persons may determine to purchase fewer ADSs than they indicate an interest in purchasing or not to purchase any ADSs in this offering. It is also possible that these persons could purchase more ADSs in this offering. In addition, the underwriters could determine to sell fewer ADSs to any of these persons than they indicate an interest in purchasing or not to sell any ADSs to such persons. The underwriters will receive the same underwriting discount and commissions on these ADSs as they will on any other ADSs sold to the public in this offering. Any ADSs not so purchased will be offered by the underwriters to the general public on the same terms as the other ADSs offered by this prospectus.
The underwriters have advised us that, following the completion of this offering, they currently intend to make a market in the ADSs as permitted by applicable laws and regulations. However, the underwriters are not obligated to do so, and the underwriters may discontinue any market-making activities at any time without notice in their sole discretion. Accordingly, no assurance can be given as to the liquidity of the trading market for the ADSs, that you will be able to sell any of the ADSs held by you at a particular time or that the prices that you receive when you sell will be favorable.
The underwriters are offering the ADSs subject to their acceptance of the ADSs from us and subject to prior sale. The underwriters reserve the right to withdraw, cancel or modify offers to the public and to reject orders in whole or in part. Certain of the underwriters may offer and sell the ADSs through one or more of their respective affiliates or selling agents. In addition, the underwriters have advised us that they do not intend to confirm sales to any account over which they exercise discretionary authority.
Commission and Expenses
The underwriters have advised us that they propose to offer the ADSs to the public at the initial public offering price set forth on the cover page of this prospectus and to certain dealers, which may include the underwriters, at that
194
Table of Contents
price less a concession not in excess of $ per ADS. After the offering, the initial public offering price, concession and reallowance to dealers may be reduced by the representatives. No such reduction will change the amount of proceeds to be received by us as set forth on the cover page of this prospectus.
The following table shows the public offering price, the underwriting discounts and commissions that we are to pay the underwriters and the proceeds, before expenses, to us in connection with this offering. Such amounts are shown assuming both no exercise and full exercise of the underwriters’ option to purchase additional ADSs.
| PER ADS | TOTAL | |||||||||||||||
| WITHOUT OPTION TO PURCHASE ADDITIONAL ADSs | WITH OPTION TO PURCHASE ADDITIONAL ADSs | WITHOUT OPTION TO PURCHASE ADDITIONAL ADSs | WITH OPTION TO PURCHASE ADDITIONAL ADSs | |||||||||||||
Public offering price | $ | $ | $ | $ | ||||||||||||
Underwriting discounts and commissions paid by us | $ | $ | $ | $ | ||||||||||||
Proceeds to us, before expenses | $ | $ | $ | $ | ||||||||||||
We estimate expenses payable by us in connection with this offering, other than the underwriting discounts and commissions referred to above, will be approximately $2.0 million. We have also agreed to reimburse the underwriters for certain expenses, including an amount not to exceed $40,000 in connection with the clearance of this offering with the Financial Industry Regulatory Authority, Inc. as set forth in the underwriting agreement.
Determination of Offering Price
Prior to this offering, there has not been a public market for our ADSs. Consequently, the initial public offering price for our ADSs will be determined by negotiations between us and the representatives. Among the factors to be considered in these negotiations will be prevailing market conditions, our financial information, market valuations of other companies that we and the underwriters believe to be comparable to us, estimates of our business potential, the present state of our development and other factors deemed relevant.
We offer no assurances that the initial public offering price will correspond to the price at which the ADSs will trade in the public market subsequent to the offering or that an active trading market for the ADSs will develop and continue after the offering.
Listing
We have applied to have our ADSs listed on the Nasdaq Global Market under the trading symbol “MITO”.
Option to Purchase Additional ADSs
We have granted to the underwriters an option, exercisable for 30 days from the date of this prospectus, to purchase, from time to time, in whole or in part, up to an aggregate of 930,000 ADSs from us at the public offering price set forth on the cover page of this prospectus, less underwriting discounts and commissions. If the underwriters exercise this option, each underwriter will be obligated, subject to specified conditions, to purchase a number of additional ADSs proportionate to that underwriter’s initial purchase commitment as indicated in the table above. This option may be exercised only if the underwriters sell more ADSs than the total number set forth on the cover page of this prospectus.
No Sales of Similar Securities
We, our officers, directors and holders of all or substantially all our equity securities have agreed, subject to specified exceptions, not to directly or indirectly:
| ∎ | sell, offer, contract or grant any option to sell (including any short sale), pledge, transfer, establish an open “put equivalent position” within the meaning of Rule16a-l(h) under the Securities Exchange Act of 1934, as amended, or |
195
Table of Contents
| ∎ | otherwise dispose of any ordinary shares, options or warrants to acquire ordinary shares or ADSs, or securities exchangeable or exercisable for or convertible into ordinary shares or ADSs currently or hereafter owned either of record or beneficially, or |
| ∎ | enter into any swap, hedge or similar arrangement or agreement that transfers, in whole or in part, the economic risk of ownership of our ordinary shares or ADSs, or of options or warrants to ordinary shares or ADSs, or securities or rights exchangeable or exercisable for or convertible into ordinary shares or ADSs, |
| ∎ | make any demand for, or exercise any right with respect to, the registration under the Securities Act of the offer and sale of any ordinary shares or ADSs, or of options or warrants to ordinary shares or ADSs, or securities or rights exchangeable or exercisable for or convertible into ordinary shares or ADSs, or cause to be filed a registration statement, prospectus or prospectus supplement (or an amendment or supplement thereto) with respect to any such registration, or |
| ∎ | publicly announce an intention to do any of the foregoing for a period of 180 days after the date of this prospectus. |
This restriction terminates after the close of trading of the ADSs on and including the 180th day after the date of this prospectus.
Jefferies LLC and Evercore Group L.L.C. may, in their sole discretion and at any time or from time to time before the termination of the180-day period release all or any portion of the securities subject tolock-up agreements. There are no existing agreements between the underwriters and any of our shareholders who will execute alock-up agreement, providing consent to the sale of ordinary shares or ADSs prior to the expiration of thelock-up period.
Stabilization
The underwriters have advised us that they, pursuant to Regulation M under the Securities Exchange Act of 1934, as amended, certain persons participating in the offering may engage in short sale transactions, stabilizing transactions, syndicate covering transactions or the imposition of penalty bids in connection with this offering. These activities may have the effect of stabilizing or maintaining the market price of our ADSs at a level above that which might otherwise prevail in the open market. Establishing short sales positions may involve either “covered” short sales or “naked” short sales.
“Covered” short sales are sales made in an amount not greater than the underwriters’ option to purchase additional ADSs in this offering. The underwriters may close out any covered short position by either exercising their option to purchase additional ADSs or purchasing ADSs in the open market. In determining the source of ADSs to close out the covered short position, the underwriters will consider, among other things, the price of ADSs available for purchase in the open market as compared to the price at which they may purchase ADSs through the option to purchase additional ADSs.
“Naked” short sales are sales in excess of the option to purchase additional ADSs. The underwriters must close out any naked short position by purchasing ADSs in the open market. A naked short position is more likely to be created if the underwriters are concerned that there may be downward pressure on the price of the ADSs in the open market after pricing that could adversely affect investors who purchase in this offering.
A stabilizing bid is a bid for the purchase of ADSs on behalf of the underwriters for the purpose of fixing or maintaining the price of the ADSs. A syndicate covering transaction is the bid for or the purchase of ADSs on behalf of the underwriters to reduce a short position incurred by the underwriters in connection with the offering. Similar to other purchase transactions, the underwriter’s purchases to cover the syndicate short sales may have the effect of raising or maintaining the market price of our ADSs or preventing or retarding a decline in the market price of our ADSs. As a result, the price of our ADSs may be higher than the price that might otherwise exist in the open market. A penalty bid is an arrangement permitting the underwriters to reclaim the selling concession otherwise accruing to a syndicate member in connection with the offering if the ADSs originally sold by such syndicate member are purchased in a syndicate covering transaction and therefore have not been effectively placed by such syndicate member.
Neither we nor any of the underwriters make any representation or prediction as to the direction or magnitude of any effect that the transactions described above may have on the price of our ADSs. The underwriters are not obligated to engage in these activities and, if commenced, any of the activities may be discontinued at any time.
196
Table of Contents
The underwriters may also engage in passive market making transactions in our ADSs on The Nasdaq Global Market in accordance with Rule 103 of Regulation M during a period before the commencement of offers or sales of ADSs in this offering and extending through the completion of distribution. A passive market maker must display its bid at a price not in excess of the highest independent bid of that security. However, if all independent bids are lowered below the passive market maker’s bid that bid must then be lowered when specified purchase limits are exceeded.
Electronic Distribution
A prospectus in electronic format may be made available bye-mail or on the web sites or through online services maintained by one or more of the underwriters or their affiliates. In those cases, prospective investors may view offering terms online and may be allowed to place orders online. The underwriters may agree with us to allocate a specific number of ADSs for sale to online brokerage account holders. Any such allocation for online distributions will be made by the underwriters on the same basis as other allocations. Other than the prospectus in electronic format, the information on the underwriters’ web sites and any information contained in any other web site maintained by any of the underwriters is not part of this prospectus, has not been approved and/or endorsed by us or the underwriters and should not be relied upon by investors.
Other Activities and Relationships
The underwriters and certain of their affiliates are full service financial institutions engaged in various activities, which may include securities trading, commercial and investment banking, financial advisory, investment management, investment research, principal investment, hedging, financing and brokerage activities. The underwriters and certain of their affiliates have, from time to time, performed, and may in the future perform, various commercial and investment banking and financial advisory services for us and our affiliates, for which they received or will receive customary fees and expenses.
In the ordinary course of their various business activities, the underwriters and certain of their affiliates may make or hold a broad array of investments and actively trade debt and equity securities (or related derivative securities) and financial instruments (including bank loans) for their own account and for the accounts of their customers, and such investment and securities activities may involve securities or instruments issued by us and our affiliates. If the underwriters or their respective affiliates have a lending relationship with us, they routinely hedge their credit exposure to us consistent with their customary risk management policies. The underwriters and their respective affiliates may hedge such exposure by entering into transactions which consist of either the purchase of credit default swaps or the creation of short positions in our securities or the securities of our affiliates, including potentially the ADSs offered hereby. Any such short positions could adversely affect future trading prices of the ADSs offered hereby. The underwriters and certain of their respective affiliates may also communicate independent investment recommendations, market color or trading ideas and publish or express independent research views in respect of such securities or instruments and may at any time hold, or recommend to clients that they acquire, long or short positions in such securities and instruments.
Selling Restrictions
Australia
This prospectus is not a disclosure document for the purposes of Australia’s Corporations Act 2001 (Cth) of Australia, or Corporations Act, has not been lodged with the Australian Securities & Investments Commission and is only directed to the categories of exempt persons set out below. Accordingly, if you receive this prospectus in Australia:
You confirm and warrant that you are either:
| ∎ | a “sophisticated investor” under section 708(8)(a) or (b) of the Corporations Act; |
| ∎ | a “sophisticated investor” under section 708(8)(c) or (d) of the Corporations Act and that you have provided an accountant’s certificate to the Company which complies with the requirements of section 708(8)(c)(i) or (ii) of the Corporations Act and related regulations before the offer has been made; |
| ∎ | a person associated with the Company under Section 708(12) of the Corporations Act; or |
| ∎ | a “professional investor” within the meaning of section 708(11)(a) or (b) of the Corporations Act. |
197
Table of Contents
To the extent that you are unable to confirm or warrant that you are an exempt sophisticated investor, associated person or professional investor under the Corporations Act, any offer made to you under this prospectus is void and incapable of acceptance.
You warrant and agree that you will not offer any of the ADSs issued to you pursuant to this prospectus for resale in Australia within 12 months of those ADSs being issued unless any such resale offer is exempt from the requirement to issue a disclosure document under section 708 of the Corporations Act.
Cayman Islands
No invitation, whether directly or indirectly, may be made to the public in the Cayman Islands to subscribe for securities of the company, and no such invitation is hereby made.
Pursuant to the Companies Law, no invitation may be made to the public in the Cayman Islands to subscribe for the ordinary shares by or on behalf of the company unless at the time of such invitation the company is listed on the Cayman Islands Stock Exchange.
European Economic Area
In relation to each member state of the European Economic Area which has implemented the Prospectus Directive (each, a “Relevant Member State”), an offer to the public of any common shares which are the subject of the offering contemplated by this prospectus supplement and the accompanying prospectus may not be made in that Relevant Member State except that an offer to the public in that Relevant Member State of any common shares may be made at any time under the following exemptions under the Prospectus Directive, if they have been implemented in that Relevant Member State:
| ∎ | to any legal entity which is a “qualified investor” as defined in the Prospectus Directive; |
| ∎ | to fewer than 100 or, if the Relevant Member State has implemented the relevant provision of the 2010 PD Amending Directive, 150, natural or legal persons (other than qualified investors as defined in the Prospectus Directive), as permitted under the Prospectus Directive, subject to obtaining the prior consent of the underwriters or the underwriters nominated by us for any such offer; or |
| ∎ | in any other circumstances falling within Article 3(2) of the Prospectus Directive, |
provided that no such offer of common shares shall require us or any of the underwriters to publish a prospectus pursuant to Article 3 of the Prospectus Directive or supplement a prospectus pursuant to Article 16 of the Prospectus Directive.
For the purposes of this provision, the expression an “offer to the public of common shares” in relation to the common shares or ADSs in any Relevant Member State means the communication in any form and by any means of sufficient information on the terms of the offer and the common shares or ADSs to be offered so as to enable an investor to decide to purchase or subscribe to the common shares or ADSs, as the same may be varied in that Relevant Member State by any measure implementing the Prospectus Directive in that Relevant Member State and the expression “Prospectus Directive” means Directive 2003/71/EC (and amendments thereto, including the 2010 PD Amending Directive, to the extent implemented in the Relevant Member State), and includes any relevant implementing measure in the Relevant Member State and the expression “2010 PD Amending Directive” means Directive 2010/73/EU.
Hong Kong
No securities have been offered or sold, and no securities may be offered or sold, in Hong Kong, by means of any document, other than to persons whose ordinary business is to buy or sell shares or debentures, whether as principal or agent; or to “professional investors” as defined in the Securities and Futures Ordinance (Cap. 571) of Hong Kong (“SFO”) and any rules made under that Ordinance; or in other circumstances which do not result in the document being a “prospectus” as defined in the Companies Ordinance (Cap. 32) of Hong Kong (“CO”) or which do not constitute an offer or invitation to the public for the purpose of the CO or the SFO. No document, invitation or advertisement relating to the securities has been issued or may be issued or may be in the possession of any person for the purpose of issue (in each case whether in Hong Kong or elsewhere), which is directed at, or the contents of which are likely to be accessed or read by, the public of Hong Kong (except if permitted under the securities laws of Hong Kong) other than with respect to securities which are or are intended to be disposed of only to persons outside Hong Kong or only to “professional investors” as defined in the SFO and any rules made under that Ordinance.
198
Table of Contents
This prospectus has not been registered with the Registrar of Companies in Hong Kong. Accordingly, this prospectus may not be issued, circulated or distributed in Hong Kong, and the securities may not be offered for subscription to members of the public in Hong Kong. Each person acquiring the securities will be required, and is deemed by the acquisition of the securities, to confirm that he is aware of the restriction on offers of the securities described in this prospectus and the relevant offering documents and that he is not acquiring, and has not been offered any securities in circumstances that contravene any such restrictions.
Japan
The offering has not been and will not be registered under the Financial Instruments and Exchange Law of Japan (Law No. 25 of 1948 of Japan, as amended), or FIEL, and the underwriters will not offer or sell any securities, directly or indirectly, in Japan or to, or for the benefit of, any resident of Japan (which term as used herein means any person resident in Japan, including any corporation or other entity organized under the laws of Japan), or to others forre-offering or resale, directly or indirectly, in Japan or to, or for the benefit of, any resident of Japan, except pursuant to an exemption from the registration requirements of, and otherwise in compliance with, the FIEL and any other applicable laws, regulations and ministerial guidelines of Japan.
Singapore
This prospectus has not been and will not be lodged or registered as a prospectus with the Monetary Authority of Singapore. Accordingly, this prospectus and any other document or material in connection with the offer or sale, or invitation for subscription or purchase of the securities may not be issued, circulated or distributed, nor may the securities be offered or sold, or be made the subject of an invitation for subscription or purchase, whether directly or indirectly, to persons in Singapore other than (i) to an institutional investor under Section 274 of the Securities and Futures Act, Chapter 289 of Singapore (the “SFA”), (ii) to a relevant person pursuant to Section 275(1), or any person pursuant to Section 275(1A), and in accordance with the conditions specified in Section 275, of the SFA, or (iii) otherwise pursuant to, and in accordance with the conditions of, any other applicable provision of the SFA.
Where the securities are subscribed or purchased under Section 275 of the SFA by a relevant person which is:
| ∎ | a corporation (which is not an accredited investor (as defined in Section 4A of the SFA)) the sole business of which is to hold investments and the entire share capital of which is owned by one or more individuals, each of whom is an accredited investor; or |
| ∎ | a trust (where the trustee is not an accredited investor) whose sole purpose is to hold investments and each beneficiary of the trust is an individual who is an accredited investor, |
securities (as defined in Section 239(1) of the SFA) of that corporation or the beneficiaries’ rights and interest (howsoever described) in that trust shall not be transferred within six months after that corporation or that trust has acquired the securities pursuant to an offer made under Section 275 of the SFA except:
| ∎ | to an institutional investor or to a relevant person defined in Section 275(2) of the SFA, or to any person arising from an offer referred to in Section 275(1A) or Section 276(4)(i)(B) of the SFA; |
| ∎ | where no consideration is or will be given for the transfer; |
| ∎ | where the transfer is by operation of law; |
| ∎ | as specified in Section 276(7) of the SFA; or |
| ∎ | as specified in Regulation 32 of the Securities and Futures (Offers of Investments) (Shares and Debentures) Regulations 2005 of Singapore. |
Switzerland
The securities may not be publicly offered in Switzerland and will not be listed on the SIX Swiss Exchange (SIX), or on any other stock exchange or regulated trading facility in Switzerland. This prospectus has been prepared without regard to the disclosure standards for issuance prospectuses under art. 652a or art. 1156 of the Swiss Code of Obligations or the disclosure standards for listing prospectuses under art. 27 ff. of the SIX Listing Rules or the listing rules of any other stock exchange or regulated trading facility in Switzerland. Neither this prospectus nor any other offering or marketing material relating to the securities or the offering may be publicly distributed or otherwise made publicly available in Switzerland.
199
Table of Contents
Neither this prospectus nor any other offering or marketing material relating to the offering, us or the securities have been or will be filed with or approved by any Swiss regulatory authority. In particular, this prospectus will not be filed with, and the offer of securities will not be supervised by, the Swiss Financial Market Supervisory Authority FINMA, and the offer of securities has not been and will not be authorized under the Swiss Federal Act on Collective Investment Schemes (“CISA”). The investor protection afforded to acquirers of interests in collective investment schemes under the CISA does not extend to acquirers of securities.
United Kingdom
This prospectus is only being distributed to, and is only directed at, persons in the United Kingdom that are qualified investors within the meaning of Article 2(1)(e) of the Prospectus Directive that are also (i) investment professionals falling within Article 19(5) of the Financial Services and Markets Act 2000 (Financial Promotion) Order 2005, as amended (the “Order”) and/or (ii) high net worth entities falling within Article 49(2)(a) to (d) of the Order and other persons to whom it may lawfully be communicated (each such person being referred to as a “relevant person”).
This prospectus and its contents are confidential and should not be distributed, published or reproduced (in whole or in part) or disclosed by recipients to any other persons in the United Kingdom. Any person in the United Kingdom that is not a relevant person should not act or rely on this document or any of its contents.
United Arab Emirates
The offering contemplated hereunder has not been approved or licensed by the Central Bank of the United Arab Emirates (UAE), the Securities and Commodities Authority of the UAE and/or any other relevant licensing authority in the UAE including any licensing authority incorporated under the laws and regulations of any of the free zones established and operating in the territory of the UAE, in particular the Dubai Financial Services Authority, or DFSA, a regulatory authority of the Dubai International Financial Centre (DIFC). This offering does not constitute a public offer of shares in the UAE, DIFC and/or any other free zone in accordance with the Commercial Companies Law, Federal Law No. 8 of 1984 (as amended), or the DFSA Markets Rules, accordingly, or otherwise. The ADSs may not be offered to the public in the UAE and/or any of the free zones.
The ADSs may be offered and issued only to a limited number of investors in the UAE or any of its free zones who qualify as sophisticated investors under the relevant laws and regulations of the UAE or the free zone concerned. We represent and warrant that the ADSs will not be offered, sold, transferred or delivered to the public in the UAE or any of its free zones.
Dubai International Financial Centre
This document relates to an Exempt Offer in accordance with the Markets Rules of the Dubai Financial Services Authority. This document is intended for distribution only to Persons of a type specified in those rules to whom Exempt Offers can be made. It must not be delivered to, or relied on by, any other Person. The Dubai Financial Services Authority has no responsibility for reviewing or verifying any documents in connection with Exempt Offers. The Dubai Financial Services Authority has not approved this document nor taken steps to verify the information set out in it, and has no responsibility for it. The ADSs to which this document relates may be illiquid and/or subject to restrictions on their resale. Prospective purchasers of the ADSs offered should conduct their own due diligence on the ADSs. If you do not understand the contents of this document you should consult an authorized financial adviser.
Canada
(A) Resale Restrictions
The distribution of ADSs in Canada is being made only in the provinces of Ontario, Quebec, Alberta and British Columbia on a private placement basis exempt from the requirement that we prepare and file a prospectus with the securities regulatory authorities in each province where trades of these securities are made. Any resale of the ADSs in Canada must be made under applicable securities laws which may vary depending on the relevant jurisdiction, and which may require resales to be made under available statutory exemptions or under a discretionary exemption granted by the applicable Canadian securities regulatory authority. Purchasers are advised to seek legal advice prior to any resale of the securities.
200
Table of Contents
(B) Representations of Canadian Purchasers
By purchasing ADSs in Canada and accepting delivery of a purchase confirmation, a purchaser is representing to us and the dealer from whom the purchase confirmation is received that:
| ∎ | the purchaser is entitled under applicable provincial securities laws to purchase the ADSs without the benefit of a prospectus qualified under those securities laws as it is an “accredited investor” as defined under National Instrument45-106—Prospectus Exemptions, |
| ∎ | the purchaser is a “permitted client” as defined in National Instrument31-103—Registration Requirements, Exemptions and Ongoing Registrant Obligations, |
| ∎ | where required by law, the purchaser is purchasing as principal and not as agent, and |
| ∎ | the purchaser has reviewed the text above under Resale Restrictions. |
(C) Conflicts of Interest
Canadian purchasers are hereby notified that the underwriters are relying on the exemption set out in section 3A.3 or 3A.4, if applicable, of National Instrument33-105—Underwriting Conflicts from having to provide certain conflict of interest disclosure in this document.
(D) Statutory Rights of Action
Securities legislation in certain provinces or territories of Canada may provide a purchaser with remedies for rescission or damages if the offering memorandum (including any amendment thereto) such as this document contains a misrepresentation, provided that the remedies for rescission or damages are exercised by the purchaser within the time limit prescribed by the securities legislation of the purchaser’s province or territory. The purchaser of these securities in Canada should refer to any applicable provisions of the securities legislation of the purchaser’s province or territory for particulars of these rights or consult with a legal advisor.
(E) Enforcement of Legal Rights
All of our directors and officers as well as the experts named herein may be located outside of Canada and, as a result, it may not be possible for Canadian purchasers to effect service of process within Canada upon us or those persons. All or a substantial portion of our assets and the assets of those persons may be located outside of Canada and, as a result, it may not be possible to satisfy a judgment against us or those persons in Canada or to enforce a judgment obtained in Canadian courts against us or those persons outside of Canada.
(F) Taxation and Eligibility for Investment
Canadian purchasers of ADSs should consult their own legal and tax advisors with respect to the tax consequences of an investment in the ADSs in their particular circumstances and about the eligibility of the ADSs for investment by the purchaser under relevant Canadian legislation.
Israel
This document does not constitute a prospectus under the Israeli Securities Law, 5728-1968, or the Securities Law, and has not been filed with or approved by the Israel Securities Authority. In Israel, this prospectus is being distributed only to, and is directed only at, and any offer of the ADSs is directed only at, (i) a limited number of persons in accordance with the Israeli Securities Law and (ii) investors listed in the first addendum, or the Addendum, to the Israeli Securities Law, consisting primarily of joint investment in trust funds, provident funds, insurance companies, banks, portfolio managers, investment advisors, members of the Tel Aviv Stock Exchange, underwriters, venture capital funds, entities with equity in excess of NIS 50 million and “qualified individuals,” each as defined in the Addendum (as it may be amended from time to time), collectively referred to as qualified investors (in each case, purchasing for their own account or, where permitted under the Addendum, for the accounts of their clients who are investors listed in the Addendum). Qualified investors are required to submit written confirmation that they fall within the scope of the Addendum, are aware of the meaning of same and agree to it.
201
Table of Contents
The following table indicates the expenses to be incurred in connection with the offering described in this registration statement, other than underwriting discounts and commissions, all of which will be paid by us. All amounts are estimated except the SEC registration fee, the Financial Industry Regulatory Authority, Inc., or FINRA, filing fee and The Nasdaq Global Market listing fee.
| AMOUNT | ||||
Securities and Exchange Commission registration fee | $ | 12,099 | ||
FINRA filing fee | 15,473 | |||
Nasdaq Global Stock Market listing fee | 130,000 | |||
Accountants’ fees and expenses | 290,000 | |||
Legal fees and expenses | 1,250,000 | |||
Transfer agent’s fees and expenses | 4,000 | |||
Printing and engraving expenses | 290,000 | |||
Miscellaneous | 6,319 | |||
|
| |||
Total expenses | $ | 1,997,891 | ||
|
| |||
202
Table of Contents
Legal matters with respect to U.S. federal and New York state law in connection with this offering will be passed upon for us by Wilmer Cutler Pickering Hale and Dorr LLP, New York, New York. Certain legal matters with respect to Cayman Islands law in connection with the validity of the ADSs being offered by this prospectus and other legal matters will be passed upon for us by Walkers, George Town, Cayman Islands. Cooley LLP, New York, New York is serving as counsel for the underwriters in connection with this offering.
The consolidated financial statements of Stealth BioTherapeutics Corp and subsidiaries as of December 31, 2016 and 2017 and for the years then ended, included in this prospectus, have been audited by Deloitte & Touche LLP, an independent registered public accounting firm, as stated in their report appearing herein (which report expresses an unqualified opinion on the consolidated financial statements and includes an explanatory paragraph referring to our ability to continue as a going concern). Such consolidated financial statements have been so included in reliance upon the report of such firm given upon their authority as experts in accounting and auditing.
The registered business address of Deloitte & Touche LLP is 200 Berkeley Street, Boston, Massachusetts 02116.
ENFORCEMENT OF CIVIL LIABILITIES
Our agent for service of process in the United States is Stealth Delaware, and the executive offices of Stealth Delaware are located at 275 Grove Street, Suite3-107, Newton, MA 02466, and the telephone number there is (617)600-6888.
We are incorporated under the laws of the Cayman Islands. We have been advised that there is some doubt as to the enforceability in the Cayman Islands, in original actions or in actions for enforcement of judgments of the U.S. courts, of civil liabilities based solely on the federal securities laws of the United States. In addition, awards for punitive damages in actions brought in the United States, or elsewhere may be unenforceable in the Cayman Islands. An award for monetary damages under the U.S. securities laws would be considered punitive if it does not seek to compensate the claimant for loss or damage suffered and is intended to punish the defendant. The enforceability of any judgment in the Cayman Islands will depend on the particular facts of the case as well as the laws and treaties in effect at the time. The United States and the Cayman Islands do not currently have a treaty providing for recognition and enforcement of judgments (other than arbitration awards) in civil and commercial matters.
We have been advised by our Cayman Islands legal counsel that the Cayman Islands Court is unlikely (i) to recognize or enforce against us judgments of the courts of the United States predicated upon the civil liability provisions of the federal securities laws of the United States or any state; and (ii) in original actions brought in the Cayman Islands, to impose liabilities against us predicated upon the civil liability provisions of the federal securities laws of the United States or any state, so far as the liabilities imposed by those provisions are penal in nature. In certain circumstances, although there is no statutory enforcement in the Cayman Islands of judgments obtained in the United States, the Cayman Islands Court will recognize and enforce a foreign money judgment of a foreign court of competent jurisdiction without retrial on the merits and based on the principle that a judgment of a competent foreign court imposes upon the judgment debtor an obligation to pay the sum for which judgment has been given provided certain conditions are met. For a foreign judgment to be enforced in the Cayman Islands, such judgment must be final and conclusive and for a liquidated sum, and must not be in respect of taxes or a fine or penalty , inconsistent with a Cayman Islands judgment in respect of the same matter, impeachable on the grounds of fraud or obtained in a manner, and or be of a kind the enforcement of which is, contrary to natural justice or the public policy of the Cayman Islands (awards of punitive or multiple damages may well be held to be contrary to public policy). The Cayman Islands Court may stay enforcement proceedings if concurrent proceedings are being brought elsewhere.
203
Table of Contents
WHERE YOU CAN FIND MORE INFORMATION
We have filed with the SEC a registration statement on FormF-1, including relevant exhibits and schedules under the Securities Act with respect to underlying ordinary shares represented by the ADSs, to be sold in this offering. A related registration statement onF-6 has been filed with the SEC to register the ADSs. This prospectus, which constitutes a part of the registration statement, does not contain all of the information contained in the registration statement. You should read the registration statement and its exhibits and schedules for further information with respect to us and our ADSs.
Immediately upon the completion of this offering, we will become subject to periodic reporting and other informational requirements of the Exchange Act as applicable to foreign private issuers. Accordingly, we will be required to file reports, including annual reports on Form20-F, and other information with the SEC. All information filed with the SEC can be inspected and copied at the public reference facilities maintained by the SEC at 100 F Street, N.E., Washington, D.C. 20549. You can request copies of these documents upon payment of a duplicating fee, by writing to the SEC. Please call the SEC at1-800-SEC-0330 for further information on the operation of the public reference rooms. The SEC maintains an internet site at http://www.sec.gov that contains reports, proxy and information statements and other information regarding issuers that file electronically with the SEC.
As a foreign private issuer, we are exempt under the Exchange Act from, among other things, the rules prescribing the furnishing and content of proxy statements, and our executive officers, directors and principal shareholders are exempt from the reporting and short-swing profit recovery provisions contained in Section 16 of the Exchange Act. In addition, we will not be required under the Exchange Act to file periodic reports and financial statements with the SEC as frequently or as promptly as U.S. companies whose securities are registered under the Exchange Act. However, we intend to furnish the depositary with our annual reports, which will include a review of operations and annual audited consolidated financial statements prepared in conformity with U.S. GAAP, and all notices of shareholders’ meeting and other reports and communications that are made generally available to our shareholders. The depositary will make such notices, reports and communications available to holders of ADSs and will mail to all record holders of ADSs the information contained in any notice of a shareholders’ meeting received by the depositary from us.
204
Table of Contents
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS
Index to Consolidated Financial Statements as of December 31, 2016 and 2017 and for the Years Ended December 31, 2016 and 2017
| PAGE | ||||
| F-2 | ||||
| F-3 | ||||
| F-4 | ||||
Consolidated Statements of Convertible Preferred Shares and Shareholders’ Deficit | F-5 | |||
| F-6 | ||||
| F-7 | ||||
Index to Unaudited Interim Condensed Consolidated Financial Statements as of December 31, 2017 and September 30, 2018 and for the Nine Month Periods Ended September 30, 2017 and 2018 | ||||
| F-24 | ||||
| F-25 | ||||
Condensed Consolidated Statements of Convertible Preferred Shares and Shareholders’ Deficit | F-26 | |||
| F-27 | ||||
| F-28 | ||||
F-1
Table of Contents
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Shareholders and Board of Directors of Stealth BioTherapeutics Corp
Opinion on the Financial Statements
We have audited the accompanying consolidated balance sheets of Stealth BioTherapeutics Corp and its subsidiaries (the “Company”) as of December 31, 2016 and 2017, the related consolidated statements of operations, convertible preferred shares and shareholders’ deficit, and cash flows, for each of the years then ended, and the related notes (collectively referred to as the “financial statements”). In our opinion, the financial statements present fairly, in all material respects, the financial position of the Company as of December 31, 2016 and 2017, and the results of its operations and its cash flows for the years then ended, in conformity with accounting principles generally accepted in the United States of America.
Going Concern
The accompanying financial statements have been prepared assuming that the Company will continue as a going concern. As discussed in Note 1 to the financial statements, the Company’s recurring losses from operations, cash used in operations, and accumulated shareholders’ deficit raise substantial doubt about its ability to continue as a going concern. Management’s plans concerning these matters are also discussed in Note 1 to the financial statements. The financial statements do not include any adjustments that might result from the outcome of this uncertainty.
Basis for Opinion
These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on the Company’s financial statements based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (PCAOB) and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. As part of our audits, we are required to obtain an understanding of internal control over financial reporting but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion.
Our audits included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audits provide a reasonable basis for our opinion.
/s/ Deloitte & Touche LLP
Boston, Massachusetts
October 25, 2018 (December 28, 2018 as to the effects of the reverse share split described in Note 18)
We have served as the Company’s auditor since 2014.
F-2
Table of Contents
STEALTH BIOTHERAPEUTICS CORP
| DECEMBER 31, | ||||||||
| 2016 | 2017 | |||||||
Assets | ||||||||
Current assets: | ||||||||
Cash and cash equivalents | $ | 9,709,732 | $ | 4,118,804 | ||||
Prepaid expenses and other current assets | 1,728,393 | 1,801,203 | ||||||
|
|
|
| |||||
Total current assets | 11,438,125 | 5,920,007 | ||||||
Property and equipment, net | 999,530 | 795,940 | ||||||
Othernon-current assets | 884,598 | 438,982 | ||||||
|
|
|
| |||||
Total assets | $ | 13,322,253 | $ | 7,154,929 | ||||
|
|
|
| |||||
Liabilities, convertible preferred shares and shareholders’ deficit | ||||||||
Current liabilities: | ||||||||
Accounts payable | $ | 2,909,247 | $ | 7,454,569 | ||||
Accrued expenses and other current liabilities | 8,866,732 | 12,520,020 | ||||||
Accrued interest payable | — | 2,525,685 | ||||||
Current portion of long-term debt | — | 2,094,295 | ||||||
|
|
|
| |||||
Total current liabilities | 11,775,979 | 24,594,569 | ||||||
|
|
|
| |||||
Convertible notes payable to shareholder | — | 50,000,000 | ||||||
Long-term debt, less current portion | — | 11,956,867 | ||||||
Warrant liability | — | 512,618 | ||||||
|
|
|
| |||||
Total liabilities | 11,775,979 | 87,064,054 | ||||||
|
|
|
| |||||
Commitments and contingencies (Note 13) | ||||||||
Series A convertible preferred shares, $0.0003 par value; 106,666,667 shares authorized; 91,600,398 issued and outstanding at December 31, 2016 and 2017; aggregate liquidation preference of $211,376,929 at December 31, 2016 and 2017 | 211,376,929 | 211,376,929 | ||||||
Shareholders’ deficit: | ||||||||
Ordinary shares, $0.0003 par value; 203,333,333 shares authorized at December 31, 2016 and 2017; 68,458,475 and 68,474,614 shares issued and outstanding at December 31, 2016 and 2017, respectively | 20,538 | 20,542 | ||||||
Additionalpaid-in capital | 36,795,750 | 38,250,174 | ||||||
Accumulated deficit | (246,646,943 | ) | (329,556,770 | ) | ||||
|
|
|
| |||||
Total shareholders’ deficit | (209,830,655 | ) | (291,286,054 | ) | ||||
|
|
|
| |||||
Total liabilities, convertible preferred shares and shareholders’ deficit | $ | 13,322,253 | $ | 7,154,929 | ||||
|
|
|
| |||||
See the accompanying notes to these consolidated financial statements.
F-3
Table of Contents
STEALTH BIOTHERAPEUTICS CORP
CONSOLIDATED STATEMENTS OF OPERATIONS
| YEAR ENDED DECEMBER 31, | ||||||||
| 2016 | 2017 | |||||||
Operating expenses: | ||||||||
Research and development | $ | 48,445,173 | $ | 63,219,537 | ||||
General and administrative | 13,403,332 | 16,500,875 | ||||||
|
|
|
| |||||
Total operating expenses | 61,848,505 | 79,720,412 | ||||||
|
|
|
| |||||
Loss from operations | (61,848,505 | ) | (79,720,412 | ) | ||||
|
|
|
| |||||
Other income (expense): | ||||||||
Interest income | 799,023 | 56,843 | ||||||
Interest expense | — | (3,281,715 | ) | |||||
Change in valuation of warrant liability | — | 35,457 | ||||||
|
|
|
| |||||
Total other income (expense), net | 799,023 | (3,189,415 | ) | |||||
|
|
|
| |||||
Net loss attributable to ordinary shareholders | $ | (61,049,482 | ) | $ | (82,909,827 | ) | ||
|
|
|
| |||||
Net loss per share attributable to ordinary shareholders—basic and diluted | $ | (0.90 | ) | $ | (1.21 | ) | ||
|
|
|
| |||||
Weighted average ordinary shares used in net loss per share attributable to ordinary shareholders—basic and diluted | 68,165,325 | 68,472,262 | ||||||
|
|
|
| |||||
Pro forma net loss per share attributable to ordinary shareholders—basic and diluted (unaudited) | $ | (0.43 | ) | |||||
|
| |||||||
Pro forma weighted average ordinary shares used in net loss per share attributable to ordinary shareholders—basic and diluted (unaudited) | 188,261,368 | |||||||
|
| |||||||
See the accompanying notes to these consolidated financial statements
F-4
Table of Contents
STEALTH BIOTHERAPEUTICS CORP
CONSOLIDATED STATEMENTS OF CONVERTIBLE PREFERRED SHARES AND SHAREHOLDERS’ DEFICIT
| SERIES A CONVERTIBLE PREFERRED SHARES | SHAREHOLDER DEMAND NOTE RECEIVABLE | ORDINARY SHARES | ADDITIONAL PAID-IN CAPITAL | ACCUMULATED DEFICIT | TOTAL SHAREHOLDERS’ DEFICIT | |||||||||||||||||||||||||||||||||||
| SHARES | AMOUNT | SHARES | AMOUNT | |||||||||||||||||||||||||||||||||||||
Balance at January 1, 2016 | 91,600,398 | $ | 211,376,929 | $ | (50,739,404 | ) | 68,125,142 | $ | 20,438 | $ | 34,952,859 | $ | (185,597,461 | ) | $ | (150,624,164 | ) | |||||||||||||||||||||||
Proceeds from shareholder demand note receivable | — | — | 50,739,404 | — | — | — | — | — | ||||||||||||||||||||||||||||||||
Exercise of warrant | — | — | — | 333,333 | 100 | 9,900 | — | 10,000 | ||||||||||||||||||||||||||||||||
Share-based compensation expense | — | — | — | — | — | 1,832,991 | — | 1,832,991 | ||||||||||||||||||||||||||||||||
Net loss | — | — | — | — | — | — | (61,049,482 | ) | (61,049,482 | ) | ||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||||||||||||
Balance at December 31, 2016 | 91,600,398 | 211,376,929 | — | 68,458,475 | 20,538 | 36,795,750 | (246,646,943 | ) | (209,830,655 | ) | ||||||||||||||||||||||||||||||
Exercise of share options | — | — | — | 16,139 | 4 | 10,471 | — | 10,475 | ||||||||||||||||||||||||||||||||
Share-based compensation expense | — | — | — | — | — | 1,286,970 | — | 1,286,970 | ||||||||||||||||||||||||||||||||
Issuance of warrant for ordinary shares | — | — | — | — | — | 156,983 | — | 156,983 | ||||||||||||||||||||||||||||||||
Net loss | — | — | — | — | — | — | (82,909,827 | ) | (82,909,827 | ) | ||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||||||||||||
Balance at December 31, 2017 | 91,600,398 | $ | 211,376,929 | $ | — | 68,474,614 | $ | 20,542 | $ | 38,250,174 | $ | (329,556,770 | ) | $ | (291,286,054 | ) | ||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||||||||||||
See the accompanying notes to these consolidated financial statements
F-5
Table of Contents
STEALTH BIOTHERAPEUTICS CORP
CONSOLIDATED STATEMENTS OF CASH FLOWS
| YEAR ENDED DECEMBER 31, | ||||||||
| 2016 | 2017 | |||||||
Cash flows from operating activities: | ||||||||
Net loss | $ | (61,049,482 | ) | $ | (82,909,827 | ) | ||
Adjustments to reconcile net loss to net cash used in operating activities: | ||||||||
Depreciation and amortization | 312,537 | 346,872 | ||||||
Change in fair value of warrant liability | — | (35,457 | ) | |||||
Issuance of warrant for ordinary shares | — | 156,983 | ||||||
Amortization of debt discount | — | 192,020 | ||||||
Write-off of deferred financing costs | 457,652 | |||||||
Non-cash interest expense | — | 2,525,685 | ||||||
Share-based compensation | 1,832,991 | 1,286,970 | ||||||
Loss on disposal of asset | — | 17,670 | ||||||
Changes in operating assets and liabilities: | ||||||||
Prepaid expenses and other current assets | 1,563,817 | (72,810 | ) | |||||
Accounts payable | 767,838 | 4,545,322 | ||||||
Accrued expenses and other current liabilities | 2,552,366 | 3,653,288 | ||||||
|
|
|
| |||||
Net cash used in operating activities | (54,019,933 | ) | (69,835,632 | ) | ||||
|
|
|
| |||||
Cash flows from investing activities: | ||||||||
Purchase of property and equipment | (287,883 | ) | (160,952 | ) | ||||
Changes in other assets | 105,362 | (12,036 | ) | |||||
|
|
|
| |||||
Net cash used in investing activities | (182,521 | ) | (172,988 | ) | ||||
|
|
|
| |||||
Cash flows from financing activities: | ||||||||
Proceeds from issuance of convertible notes payable to shareholder | — | 50,000,000 | ||||||
Proceeds from venture debt issuance | — | 14,633,000 | ||||||
Payment of venture issuance costs | — | (225,783 | ) | |||||
Proceeds from repayment of shareholder demand note receivable | 50,739,404 | — | ||||||
Payment of deferred financing costs | (457,652 | ) | — | |||||
Proceeds from exercise of share options and warrant | 10,000 | 10,475 | ||||||
|
|
|
| |||||
Net cash provided by financing activities | 50,291,752 | 64,417,692 | ||||||
|
|
|
| |||||
Net decrease in cash and cash equivalents | (3,910,702 | ) | (5,590,928 | ) | ||||
Cash and cash equivalents, beginning of period | 13,620,434 | 9,709,732 | ||||||
|
|
|
| |||||
Cash and cash equivalents, end of period | $ | 9,709,732 | $ | 4,118,804 | ||||
|
|
|
| |||||
Supplemental disclosure of noncash investing and financing activity: | ||||||||
Noncash items: | ||||||||
Fair value of warrants issued in connection with term loan | $ | — | $ | 548,075 | ||||
|
|
|
| |||||
Supplemental cash flow information-cash paid for interest | $ | — | $ | 564,010 | ||||
|
|
|
| |||||
See the accompanying notes to these consolidated financial statements.
F-6
Table of Contents
STEALTH BIOTHERAPEUTICS CORP
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
1. Organization and Operations
The Company
Stealth BioTherapeutics Corp was incorporated in Grand Cayman, Cayman Islands as Stealth Peptides International, Inc. in April 2006. Its wholly owned subsidiary, Stealth BioTherapeutics Inc., was incorporated in Delaware as Stealth Peptides Inc. in October 2007. In addition, a wholly owned subsidiary, Stealth BioTherapeutics (HK) Limited, was incorporated in Hong Kong in September 2017. In May 2018, Stealth BioTherapeutics (Shanghai) Limited was formed as a wholly foreign owned enterprise in China. Hereinafter, Stealth BioTherapeutics Corp, Stealth BioTherapeutics Inc., Stealth BioTherapeutics (HK) Limited, and Stealth BioTherapeutics (Shanghai) Limited are referred to as the “Company.” The Company is a clinical stage biotechnology company focused on the discovery and development of novel pharmaceutical agents to treat patients suffering from diseases involving mitochondrial dysfunction through its mitochondrial medicine platform. The consolidated financial statements include the assets and liabilities and operating results of the Company and its wholly owned subsidiaries. Since inception, the Company has devoted substantially all of its efforts to research and development, business planning, acquiring operating assets, seeking intellectual property protection for its technology and product candidates, and raising capital.
Since inception, the Company has entered into numerous debt and equity issuances with Morningside Venture (I) Investments Limited (the “Shareholder”). As of December 31, 2017, the Shareholder held approximately 98% of the Company’s outstanding shares. See Notes 7 and 8. Since inception, the Company has incurred net losses and negative cash flows from operations and had an accumulated deficit of $246.6 million and $329.6 million as of December 31, 2016 and 2017, respectively. The Company has financed its operations to date from the issuance of preferred shares, ordinary shares and convertible debt substantially to the Shareholder, as well as term debt.
Liquidity and Going Concern
These consolidated financial statements have been prepared on a going concern basis, which assumes the realization of assets and settlement of liabilities in the normal course of business. Since its inception, the Company has incurred recurring losses, including a net loss of $82.9 million for the year ended December 31, 2017. The Company expects to continue to incur operating losses in the foreseeable future.
Management believes that cash and cash equivalents of $4.1 million at December 31, 2017, together with proceeds of $5.0 million received in 2018 under our term loan facility (Note 6), proceeds of $50.0 million received under the January 2018 note purchase agreement (Note 7) and proceeds of $15.0 million received in October 2018 under the October note purchase agreement (Note 7), along with an additional borrowing capacity of $15 million (Note 7), will be sufficient to fund operating expenses into the first quarter of 2019. The Company may seek to obtain financing through equity and debt issuances, collaborative agreements, and grants from government and private sponsors. Because the ability to obtain additional financing is outside of the Company’s control, the foregoing conditions raise substantial doubt in regard to the Company’s ability to continue as a going concern. If the Company is unable to obtain additional funding when needed, or to the extent needed, it may be necessary to scale back operations or halt certain research and development activities, which could prevent the Company from successfully executing on its operating plan. The consolidated financial statements do not include any adjustments related to the recoverability and classification of recorded assets or liabilities that might be necessary should the Company be unable to continue its operations.
2. Summary of Significant Accounting Policies
Basis of Presentation and Use of Estimates
The accompanying consolidated financial statements have been prepared in conformity with accounting principles generally accepted in the United States of America (“GAAP”). Any reference in these notes to applicable guidance is meant to refer to authoritative GAAP, as found in the Accounting Standards Codification (“ASC”) and Accounting Standards Update (“ASU”) of the Financial Accounting Standards Board (“FASB”). The preparation of financial statements in conformity with GAAP requires management to make estimates and assumptions that affect the
F-7
Table of Contents
amounts reported in the financial statements and accompanying notes. On an ongoing basis, the Company’s management evaluates its estimates related to, but not limited to, estimates related to fair value of ordinary share, share-based compensation expense, recoverability of the Company’s net deferred tax asset-related valuation allowances, and certain prepaid expenses and accrued expenses. The Company bases its estimates on historical experience and other market-specific or other relevant assumptions that it believes to be reasonable under the circumstances. Actual results may differ materially from those estimates or assumptions.
The Company utilizes significant estimates and assumptions in determining the fair value of its ordinary shares. The Company utilized various valuation methodologies in accordance with the framework of the 2004 and 2014 American Institute of Certified Public Accountants Technical Practice Aids,Valuation of Privately-held Company Equity Securities Issued as Compensation, to estimate the fair value of its ordinary shares. Each valuation methodology includes estimates and assumptions that require the Company’s judgment. These estimates and assumptions include a number of objective and subjective factors, including external market conditions affecting the biotechnology industry sector, the prices at which the Company sold preferred shares, the superior rights and preferences of securities senior to the Company’s ordinary shares at the time and the likelihood of achieving a liquidity event, such as an initial public offering (“IPO”) or sale of the Company. Significant changes to the key assumptions used in the valuations could result in different fair values of ordinary shares at each valuation date and materially affect the consolidated financial statements.
Principles of Consolidation
All intercompany balances and transactions have been eliminated in consolidation.
Segment Information
Operating segments are defined as components of an enterprise about which separate discrete information is available for evaluation by the chief operating decision maker, or decision-making group, in deciding how to allocate resources and assess performance. Management views the Company’s operations and manages its business as a single operating segment.
Cash Equivalents
Cash equivalents include highly liquid investments maturing within 90 days from the date of purchase. Cash equivalents consist primarily of U.S. government treasury funds at December 31, 2016 and 2017 and are valued at cost, which approximates fair value.
Concentrations of Credit Risk
Financial instruments, which potentially subject the Company to concentrations of credit risk, consist principally of money market funds and U.S. treasury funds. The Company places these investments in highly rated financial institutions and limits the amount of credit exposure to any one financial institution. These amounts at times may exceed federally insured limits. The Company has not experienced any credit losses in such accounts and does not believe it is exposed to any significant credit risk on these funds.
Fair Value
Fair value is defined as the exchange price that would be received for an asset or paid to transfer a liability (an exit price) in the principal or most advantageous market for the asset or liability in an orderly transaction between market participants on the measurement date. Valuation techniques used to measure fair value are performed in a manner to maximize the use of observable inputs and minimize the use of unobservable inputs. The accounting standard describes a fair value hierarchy based on three levels of inputs, of which the first two are considered observable and the last unobservable, that may be used to measure fair value, which are the following:
Level 1—Quoted prices in active markets that are accessible at the market date for identical unrestricted assets or liabilities.
Level 2—Inputs other than Level 1 that are observable, either directly or indirectly, such as quoted prices for similar assets or liabilities; quoted prices in markets that are not active; or other inputs for which all significant inputs are observable or can be corroborated by observable market data for substantially the full term of the assets or liabilities.
Level 3—Unobservable inputs that are supported by little or no market activity and that are significant to the fair value of the assets or liabilities.
F-8
Table of Contents
The Company’s financial instruments consist of cash equivalents, principally U.S. government securities, accounts payable, accrued expenses, term debt and a warrant liability.
Management believes that the carrying amounts of the Company’s cash equivalents, accounts payable and accrued expenses approximate the fair value due to the short term nature of those instruments. The Company has classified these financial instruments as Level I. Cash equivalents as of December 31, 2016 and 2017 were $5.2 million and $4.0 million, respectively.
The Company believes that its debt obligations bear interest at rates which approximate prevailing market rates for instruments with similar characteristics and, accordingly, the carrying values for these instruments approximate fair value. The debt fair value measurements are considered Level 2 in the fair value hierarchy.
The Company’s warrant liability is carried at fair value determined according to the fair value hierarchy described above and classified as a Level 3 measurement (see Note 6).
As of December 31, 2017, the Company has a term loan outstanding, the fair value of which is measured using Level 2 inputs and warrant liability, which is measured using Level 3 inputs (see Note 6). The Company evaluates transfers between levels at the end of each reporting period. There were no transfers of financial instruments between levels during the years ended December 31, 2016 and 2017. The change in fair value of the warrant is included in other income (expense).
Property and Equipment
Property and equipment are stated at cost, net of accumulated depreciation and amortization. Major improvements are capitalized as additions to property and equipment, whereas expenditures for maintenance and repairs, which do not improve or extend the life of the respective assets, are charged to operating expenses as incurred.
Depreciation and amortization is recorded using the straight line method over the estimated useful lives of the respective assets, which are as follows:
ASSET | ESTIMATED USEFUL LIFE | |
Computer equipment and software | 3 years | |
Furniture, fixtures, and other | 5 years | |
Laboratory equipment | 5 years | |
Leasehold improvements | Shorter of useful life or term of lease |
Impairment of Long-lived Assets
The Company reviews long-lived assets for impairment whenever events or changes in circumstances indicate that the carrying amount of the asset may not be recoverable. When such events occur, the Company compares the carrying amounts of the assets to the undiscounted expected future cash flows the assets are expected to generate and recognizes an impairment loss equal to the excess of the carrying value over the fair value of the related asset. For the years ended December 31, 2016 and 2017, no impairments have been recorded.
Operating Leases
The Company leases facilities under anon-cancelable operating lease agreement. The lease agreement contains free or escalating rent payment provisions. The Company recognizes rent expense under such leases on a straight-line basis over the term of the lease with the difference between the expense and the payments recorded as deferred rent on the consolidated balance sheets. Any reimbursements by the landlord for tenant improvements are considered lease incentives, the balance of which is recorded as a lease incentive obligation within deferred rent on the consolidated balance sheets and amortized over the life of the lease. Lease renewal periods are considered in determining the lease term.
F-9
Table of Contents
Convertible Preferred Shares
The Company classifies convertible preferred shares as temporary equity in the consolidated balance sheets due to certain change in control clauses that are outside of the Company’s control, including liquidation, sale, or transfer of control of the Company, as holders of the convertible preferred shares could cause redemption of the shares in these situations.
Research and Development Costs
Costs incurred in connection with research and development activities are expensed as incurred. Research and development expenses include (i) employee-related expenses, including salaries, benefits, travel and share-based compensation expense; (ii) external research and development expenses incurred under arrangements with contract research organizations and contract manufacturing organizations, investigational sites and consultants, including share-based compensation expense for consultants; (iii) the cost of acquiring, developing and manufacturing clinical study materials; and (iv) costs associated with preclinical and clinical activities and regulatory operations.Non-refundable advance payments for goods or services to be received in the future for use in research and development activities are capitalized and recorded in the accompanying consolidated balance sheets as prepaid research and development. The capitalized amounts are expensed as the related goods are delivered or the services are performed. If expectations change such that the Company does not expect it will need the goods to be delivered or the services to be rendered, capitalizednon-refundable advance payments would be charged to expense.
The Company enters into consulting, research and other agreements with commercial entities, researchers, universities and others for the provision of goods and services. Under such agreements, the Company may pay for services on an hourly, monthly, quarterly, project or other basis. Such arrangements are generally cancellable upon reasonable notice and payment of costs incurred. Costs are considered incurred based on an evaluation of the progress to completion of specific tasks under each contract using information and data provided by the Company’s clinical sites and vendors. These costs consist of direct and indirect costs associated with specific projects, as well as fees paid to various entities that perform certain research on behalf of the Company.
Depending upon the timing of payments to the service providers, the Company recognizes prepaid expenses or accrued expenses related to these costs. These accrued or prepaid expenses are based on management’s estimates of the work performed under service agreements, milestones achieved and experience with similar contracts. The Company monitors each of these factors and adjusts estimates accordingly.
Share-based Compensation
The Company accounts for share-based compensation awards as compensation expense based on their grant date fair values. For share-based awards granted to employees, the Company allocates share-based compensation expense on a straight-line basis over the associated service or vesting period. Fornon-employees the compensation expense is generally recognized during the period in which services are rendered. At the end of each financial reporting period prior to completion of the service, the fair value of these awards is remeasured using the then current fair value of the Company’s ordinary shares and updated assumption inputs in the Black-Scholes option-pricing model (“Black-Scholes”). The Company recognizes compensation expense for the portion of awards that have vested each period. Share-based compensation is classified in the accompanying consolidated statements of operations within research and development or general and administrative operating expenses depending on where the related services are provided.
The Company estimates the fair value of its share options using Black-Scholes, which requires the input of subjective assumptions, including (a) expected share price volatility, (b) expected term of the award, (c) risk-free interest rate, (d) expected dividends and (e) estimated fair value of its ordinary shares on the measurement date. Due to the lack of a public market for the trading of its ordinary shares and a lack of Company specific historical and implied volatility data, the Company has based its estimate of expected volatility on the historical volatility of a group of similar companies, but which are publicly traded. When selecting these public companies on which it has based its expected share price volatility, the Company selected companies with comparable characteristics to it, including enterprise value, risk profiles, position within the industry and with historical share price information sufficient to meet the expected term of the share-based awards. The Company computes historical volatility data using the daily closing prices for the selected companies’ shares during the equivalent period of the calculated expected term of the share-based awards. The Company will continue to apply this process until a sufficient amount of historical
F-10
Table of Contents
information regarding the volatility of its own share price becomes available. The expected term of options granted represents the weighted average of previously transacted awards plus the minimum and maximum expected life of the outstanding awards based on vesting and expiry. The expected term for nonemployee awards is the remaining contractual term of the option. The risk-free interest rates are based on the U.S. Treasury securities with a maturity date commensurate with the expected term of the associated award. The Company has never paid and does not expect to pay dividends in the foreseeable future.
The Company estimates forfeitures at the time of grant and revises those estimates in subsequent periods if actual forfeitures differ from its estimates. The Company uses historical plan data to estimate forfeitures and records share-based compensation expense only for those awards that are expected to vest. Share-based compensation expense recognized in the consolidated financial statements is based on awards that are ultimately expected to vest.
Income Taxes
Deferred income taxes are recorded using an asset and liability approach. The Company records deferred tax assets and liabilities based on differences between financial reporting and tax bases of assets and liabilities which are measured using the enacted tax rates and laws that will be in effect when the differences are expected to reverse. Deferred tax assets are reduced by a valuation allowance if it is more likely than not that some portion or all of the deferred tax asset will not be realized.
When uncertain tax positions exist, the Company recognizes the tax benefit of tax positions to the extent that the benefit will more likely than not be realized, which is based upon the technical merits of the tax position as well as consideration of the available facts and circumstances. As of December 31, 2016 and 2017, the Company does not have any material uncertain tax positions.
Guarantees and Indemnification
The Company indemnifies its officers and directors for certain events or occurrences that happen by reason of the relationship with, or position held at, the Company. The Company has not experienced any losses related to these indemnification obligations, and no claims were outstanding.
Comprehensive Loss
Comprehensive loss is defined as the change in equity of a business enterprise during a period from transactions and other events and circumstances fromnon-owner sources. Comprehensive loss is equal to net loss for all periods presented.
Net Loss Per Share Attributable to Ordinary Shareholders
Basic net loss per share attributable to ordinary shareholders is calculated by dividing net loss attributable to ordinary shareholders by the weighted average shares outstanding during the period, without consideration for ordinary shares equivalents. During periods of income, the Company allocates participating securities a proportional share of income determined by dividing total weighted average participating securities by the sum of the total weighted average ordinary shares and participating securities (the“two-class method”). The Company’s convertible preferred shares participate in any dividends declared by the Company and are, therefore, considered to be participating securities. Participating securities have the effect of diluting both basic and diluted earnings per share during periods of income. During periods of loss, the Company allocates no loss to participating securities because they have no contractual obligation to share in the losses of the Company. Diluted net loss per share attributable to ordinary shareholders is calculated by adjusting weighted average shares outstanding for the dilutive effect of ordinary share equivalents outstanding for the period, determined using the treasury-share andif-converted methods. For purposes of the diluted net loss per share attributable to ordinary shareholders’ calculation, convertible preferred shares, share options, warrants and convertible notes are considered to be ordinary share equivalents, but have been excluded from the calculation of diluted net loss per share attributable to ordinary shareholders, as their effect would be anti-dilutive for all periods presented. Therefore, basic and diluted net loss per share are the same for all periods presented.
Unaudited Pro Forma Loss per Share
Unaudited pro forma net loss per share applicable to ordinary shareholders is computed using the weighted-average number of ordinary shares outstanding after giving effect to the conversion of all outstanding convertible preferred shares and convertible debt into ordinary shares as if such conversion had occurred on January 1, 2017, or the date of original issuance, if later.
F-11
Table of Contents
Recent Accounting Pronouncements
In March 2016, the FASB issued ASUNo. 2016-09Improvements to Employee Share-Based Payment Accounting (“ASU2016-09”), which simplifies share-based payment accounting through a variety of amendments. The standard was effective for annual periods beginning after December 15, 2016 and for interim periods within those fiscal years. The changes resulting from the adoption of this standard impact the accounting for income taxes, accounting for forfeitures, statutory tax withholding and the presentation of statutory tax withholding on the statement of cash flows. The Company adopted this standard on January 1, 2017. Under guidance within ASU2016-09, excess tax benefits and deficiencies are to be recognized as income tax expense or benefit in the statement of operations in the period in which they occur rather than as an increase or decrease in stockholders’ equity (deficit). Since the Company maintains a full valuation allowance on its net deferred tax asset, there is no net impact to its accumulated deficit or its net loss resulting from the adoption of this standard. Also under the guidance in ASU2016-09, an entity may elect to account for forfeitures as they occur or continue to estimate the total number of awards that are vested or expected to vest. The Company has elected to continue to estimate its forfeitures. The adoption of this standard did not have a material impact on the Company’s financial position, results of operations or statement of cash flows.
In February 2016, the FASB issued ASU2016-02,Leases (Topic 842) (“ASU2016-02”). The new guidance most significantly impacts lessee accounting and disclosures but also requires enhanced disclosures for lessors. The guidance requires lessees to identify arrangements that should be accounted for as leases. For lease arrangements exceeding a12-month term, aright-of-use asset and lease obligation is recorded by the lessee for all leases, whether operating or financing, while the statement of operations reflects lease expense for operating leases and amortization and interest expense for financing leases. Leases with a term of 12 months or less will be accounted for similar to existing guidance for operating leases. In addition, the new lease guidance requires the use of the modified retrospective method. The guidance is effective for private companies for fiscal years beginning after December 15, 2019. The Company is evaluating the impact of this new standard on its consolidated financial statements and related disclosures.
In August 2016, the FASB issued ASUNo. 2016-15,Statement of Cash Flows (Topic 230) (“ASU2016-15”):Classification of Certain Cash Receipts and Cash Payments. This update addresses eight specific cash flow issues with the objective of reducing the existing diversity in practice. The ASU is effective for private companies for fiscal years and interim periods within those fiscal years beginning after December 15, 2018. The Company does not believe that the adoption of ASUNo. 2016-15 will have a material impact on its consolidated financial statements and related disclosures.
In May 2017, the FASB issued ASUNo. 2017-09,Compensation—Stock Compensation (Topic 718): Scope of Modification Accounting (“ASUNo. 2017-09”), which clarifies when to account for a change to the terms or conditions of a share-based payment award as a modification. Under the new guidance, modification accounting is required only if the fair value, the vesting conditions, or the classification of the award (as equity or liability) changes as a result of the change in terms or conditions. The standard is effective for annual periods beginning after December 15, 2017, including interim periods within those fiscal years. Early adoption is permitted. The Company is evaluating the impact of this new standard on its consolidated financial statements and related disclosures.
In June 2018, the FASB issued ASUNo. 2018-07,Compensation—Stock Compensation (Topic 718): Improvements to Nonemployee Share-Based Payment Accounting (“ASUNo. 2018-07”). These amendments expand the scope of Topic 718, Compensation—Stock Compensation (which currently only includes share-based payments to employees) to include share-based payments issued to nonemployees for goods or services. Consequently, the accounting for share-based payments to nonemployees and employees will be substantially aligned. The ASU supersedes Subtopic505-50, Equity—Equity-Based Payments toNon-Employees. This standard is effective for private companies for annual periods beginning after December 15, 2019, including interim periods within those fiscal years, with early adoption permitted as long as ASUNo. 2014-09 has been adopted by the Company. The Company is evaluating the impact of this new standard on its consolidated financial statements and related disclosures.
F-12
Table of Contents
3. Prepaid Expenses and Other Current Assets
Prepaid expenses and other current assets consist of the following:
| AS OF DECEMBER 31, | ||||||||
| 2016 | 2017 | |||||||
Research and development | $ | 1,541,341 | $ | 1,527,711 | ||||
Other | 187,052 | 273,492 | ||||||
|
|
|
| |||||
Total | $ | 1,728,393 | $ | 1,801,203 | ||||
|
|
|
| |||||
4. Property and Equipment, Net
Property and equipment, net consists of the following:
| AS OF DECEMBER 31, | ||||||||
| 2016 | 2017 | |||||||
Computer equipment and software | $ | 330,070 | $ | 354,903 | ||||
Furniture, fixtures and other | 644,756 | 718,955 | ||||||
Laboratory equipment | 409,336 | 376,806 | ||||||
Leasehold improvements | 336,178 | 374,097 | ||||||
|
|
|
| |||||
| 1,720,340 | 1,824,761 | |||||||
Accumulated depreciation | (720,810 | ) | (1,028,821 | ) | ||||
|
|
|
| |||||
Property and equipment, net | $ | 999,530 | $ | 795,940 | ||||
|
|
|
| |||||
Depreciation expense for the years ended December 31, 2016 and 2017 was $312,537 and $346,872, respectively.
5. Accrued Expenses and Other Current Liabilities
Accrued expenses and other current liabilities consist of the following:
| AS OF DECEMBER 31, | ||||||||
| 2016 | 2017 | |||||||
Research and development | $ | 5,798,917 | $ | 9,272,095 | ||||
Employee compensation costs | 1,555,968 | 2,060,991 | ||||||
Consulting and professional services | 489,258 | 542,436 | ||||||
Legal expenses | 660,474 | 407,923 | ||||||
Deferred rent | 196,537 | 165,373 | ||||||
Other | 165,578 | 71,202 | ||||||
|
|
|
| |||||
Total | $ | 8,866,732 | $ | 12,520,020 | ||||
|
|
|
| |||||
F-13
Table of Contents
6. Debt
Term Loan
In June 2017, the Company entered into a Loan and Security Agreement, (“LSA”), with a lender which permits the Company to borrow up to an aggregate principal amount of $40.0 million through a multiple tranche term loan (“Loan”). The tranche advances are based on the Company achieving certain performance milestones as defined in the LSA. Upon closing of the Loan, the Company drew the first tranche less expenses, which resulted in net proceeds of $12.1 million. In September 2017, the Company drew the second tranche advance of $2.5 million upon achieving the first milestone, bringing the total gross amount borrowed to $15.0 million as of December 31, 2017.
The Loan included a $200,000 facility charge, which was paid to the lender on the closing date. The Company paid a $30,000 due diligence fee prior to the Loan closing, and the Company incurred additional cash expenses of $362,783 related to the Loan. These three amounts were all recorded as a debt discount and are being amortized as interest expense using the effective interest method over the life of the Loan. The Loan also includes an end of term charge equal to the greater of $750,000 or 5% of the aggregate principal amount of all advances. The end of term charge is being accrued and recorded to interest expense over the life of the Loan using the effective interest method.
The Loan bears interest at the greater of (i) the prime rate plus 5.5% or (ii) 9.5%. As of December 31, 2017, the interest rate was 10.0%. Interest accrues from the closing date and interest payments are due monthly in arrears on the first of the month. Payments under the Loan are interest only for the first twelve months after closing followed by a30-month amortization period of principal and interest through the scheduled maturity date of January 1, 2021. Principal and interest payments will commence on August 1, 2018. However, if certain milestones are met, the date may be extended to February 1, 2019 or August 1, 2019, depending on the milestone achievement. During 2018, the Loan was amended to, among other things, delay the principal payments to December 1, 2018 and possibly further to April 30, 2019 depending upon the achievement of certain milestones.
The Company’s obligations to the lender are secured by a first priority security interest in substantially all of its assets, excluding intellectual property (“IP”). The lender maintains a negative pledge on IP with a security interest in the proceeds of the sale of the IP. The Loan contains certain covenants related to restrictions on payments for certain investments, additional debt, distributions and transfers.
As consideration for the Loan, the Company and the lender entered into a Warrant Agreement (“Warrant”), pursuant to which the lender, as Warrant holder, has the right to purchase a quantity of shares equal to the quotient derived by dividing (a) the Warrant coverage by (b) the exercise price. Warrant coverage means the greater of (a) $312,500 plus 2.5% of future tranche advances in the event all or part of the tranches are funded or (b) $375,000. The exercise price is (a) the purchase price of Series A preferred shares, $2.30769 per share, or (b) the price per share paid in the next equity round of financing of ordinary shares or preferred shares, which results in aggregate gross proceeds of at least $30 million. As of December 31, 2017, the exercise price, share type and amount of shares had not been fully defined. The Warrant is exercisable beginning in June 2017, in whole or in part, and expires in ten years.
The estimated Warrant shares were initially valued on June 30, 2017, using the Black-Scholes model with the following assumptions: volatility of 64.5%, expected term of ten years, risk-free interest rate of 2.3%, fair value of Series A preferred shares of $2.43 and a zero dividend yield. The resulting estimated Warrant fair value of $548,075 has been recorded as a debt discount and is being amortized through interest expense using the effective interest method through the scheduled maturity date of January 1, 2021. At December 31, 2017, the following assumptions were used: volatility of 67.3%, expected term of 9.5 years, risk-free interest rate of 2.4%, fair value of Series A preferred shares of $2.28 and a zero dividend yield.
F-14
Table of Contents
Certain estimates and judgments were used by management to estimate future funding from the Loan and the associated probabilities of occurrence, and volatility, amongst others. The warrant is recorded at fair value on our consolidated balance sheet as a liability and subject to revaluation at each balance sheet date, and any changes in value are recorded as a component of gain or loss from valuation of warrant liability, until the earlier of their exercise or expiration or upon the completion of a liquidation event. Activity related to the Warrant liability for the year ended December 31, 2017 is as follows:
Fair value at January 1, 2017 | $ | — | ||
|
| |||
Issuance of warrant | 548,075 | |||
Change in fair value of warrant liability | (35,457 | ) | ||
|
| |||
Fair value at December 31, 2017 | $ | 512,618 | ||
|
|
In addition, the lender can declare a material adverse effect while monitoring our business, operations, properties, assets or financial condition. A material adverse effect is considered an event of default under the LSA. In the event of default, repayment of amounts due under the Loan may be accelerated by the lender.
Future principal payments under the Loan as of December 31, 2017 are as follows:
2018 | $ | 2,242,136 | ||
2019 | 5,781,667 | |||
2020 | 6,378,089 | |||
2021 | 598,108 | |||
|
| |||
Total future principal payments | 15,000,000 | |||
|
| |||
Less unamortized debt discount | 948,838 | |||
|
| |||
Total balance as depicted on the balance sheet | $ | 14,051,162 | ||
|
| |||
Term loan—current portion | 2,094,295 | |||
Termloan—non-current portion | 11,956,867 | |||
|
| |||
Total balance as depicted on the balance sheet | $ | 14,051,162 | ||
|
|
Interest expense related to the Loan for the year ended December 31, 2017 was $1,035,493. Accrued interest as of December 31, 2017 was $279,463.
In March 2018, the Company drew the third tranche advance of $5.0 million upon achieving the third milestone, bringing the total gross amount borrowed to $20.0 million. During 2018, the Loan was amended to, among other things, delay the principal payments to December 1, 2018 and possibly further to April 30, 2019 depending upon the achievement of certain milestones. For consideration of the amendments, the Company agreed to pay an additional end of term charge of $250,000 at maturity which is being accrued and recorded to interest expense over the life of the loan using the effective interest method.
7. Convertible Notes Payable and Shareholder Demand Note Receivable
For the year ended December 31, 2016, the Company recorded $763,995 of interest income from a Shareholder Demand Note Receivable that was paid in full during 2016.
In connection with the issuance of a note in December 2009, the Company issued a warrant to the Shareholder to purchase 333,333 ordinary shares at $0.03 per share. The warrant was fully exercised in November 2016 for $10,000.
F-15
Table of Contents
During the year ended December 31, 2017, the Company issued six convertible promissory notes payable to the Shareholder, resulting in proceeds of $50.0 million (the “2017 Shareholder Notes”). The notes accrue interest at 8% per annum. Effective upon the closing of a qualified financing, as defined, the outstanding principal and accrued interest will automatically convert into shares of the same class and series of our shares issued to other investors in the qualified financing. The Shareholder also has the right to convert some or all of the outstanding amount into shares of Series A preferred shares at a conversion price of $2.30769 after December 31, 2018.
Interest expense related to the convertible notes for the year ended December 31, 2017 was $2,246,222, which was recorded as accrued interest payable on the accompanying consolidated balance sheet.
In January 2018, the Company entered into a note exchange agreement with the Shareholder in the amount of $52.4 million, which represents the total principal and accrued interest of the 2017 Shareholder Notes at the time of the execution of the note exchange agreement. The exchange terminated the 2017 Shareholder Notes and created a new convertible note under substantially the same terms as the notes described in the following paragraph.
In January 2018, the Company entered into a note purchase agreement with new investors (as amended, the “2018 Agreement”), whereby the Company may borrow an aggregate principal amount of $30.0 million in exchange for notes convertible into ordinary shares of the Company. In April 2018, the note purchase agreement was amended to allow the Company to borrow up to $65.0 million in the aggregate. Under the 2018 Agreement, between January and May 2018, the Company issued notes in an aggregate principal amount of $50.0 million (the “2018 New Investor Notes”). The 2018 New Investor Notes accrue interest at 7% per annum. Accrued interest on the 2018 New Investor Notes compounds annually, and upon such compounding, shall be added to the outstanding principal amount. The 2018 New Investor Notes, as amended, are convertible upon (i) the closing of an initial public offering or (ii) a subsequent financing occurring after January 10, 2019. Effective upon the closing of a qualified financing, as defined, the outstanding principal and accrued interest plus a 25% premium, defined as the sum of principal plus interest multiplied by 25%, will automatically convert into shares of the same class and series of our shares issued to other investors in the qualified financing. Unless the outstanding amount of the 2018 New Investor Notes are earlier repaid, retired, discharged, or automatically converted into shares of the Company upon the occurrence of events discussed below, all amounts outstanding become due and payable on the later of (i) January 10, 2020 and (ii) five business days after the date on which the term loan is repaid, terminated and discharged in full.
In October 2018, the Company entered into an additional note purchase agreement with the Shareholder (the “2018 Shareholder Note”), whereby the Company may borrow an aggregate principal amount of up to $30.0 million, of which it has borrowed $15.0 million. The notes contain similar terms as the notes described in the preceding paragraph. The 2018 Shareholder Note is convertible upon a qualified initial public offering of our ordinary shares in the United States at the initial public offering price per share. Effective upon the closing of a qualified financing, the outstanding principal and accrued interest plus a 25% premium of such principal and interest will automatically convert into shares of the same class and series of our shares issued to other investors in the qualified financing. The 2018 Shareholder Note accrues interest at 7% per annum and accrued interest compounds annually, and upon such compounding, is added to the outstanding principal amount. Unless earlier converted into shares, the 2018 Shareholder Note becomes due and payable on the later of (i) October 3, 2020 and (ii) five business days after the date on which the Loan is repaid, terminated and discharged in full.
8. Convertible Preferred Shares
At December 31, 2016 and 2017, the Company had authorized 106,666,667 shares of Series A preferred, $0.0003 par value, and there were 91,600,398 shares issued and outstanding.
The rights and preferences of the Series A preferred shares are as follows:
Conversion—At any time at the holder’s request and automatically upon the closing of a qualified IPO or sale of the Company, Series A preferred shares is convertible into ordinary shares at a ratio which is computed by dividing the original issue price by the applicable conversion price. A qualified IPO is defined under our articles of association as a fully underwritten public offering of ordinary shares in which aggregate gross proceeds equal or exceed $35 million pursuant to an effective registration statement under the Securities Act or in a jurisdiction
F-16
Table of Contents
outside of the United States. The initial conversion price of $2.30769 may be adjusted if and whenever the Company subsequently issues or sells ordinary shares or Series A preferred shares at a per share price that is less than the conversion price in effect at that time. At December 31, 2017, the applicable conversion ratio was 1:1.
Dividends—Series A preferred shareholders are entitled to receive, when and as declared by the board of directors, preferential cash dividends at a rate at least equal to 8% of the original issue price. Such dividends are not cumulative. No dividends have been declared.
Redemption Rights—Series A preferred shareholders do not have any stated redemption rights.
Liquidation Rights—In the event of a liquidation, dissolution, orwinding-up of the Company, Series A preferred shareholders shall be paid an amount first out of legally available funds available for distribution to holders of the Company’s capital share an amount equal to $2.30769 per share, plus all declared but unpaid dividends with respect to each such shares, as adjusted for any share dividend, share split, recapitalization, or other similar event. After payment of all preferential amounts, any assets and funds of the Company that remain available shall be distributed on a pro rata basis among the holders of ordinary shares.
Voting Rights—Series A preferred shareholders are entitled to the number of votes equal to the number of ordinary shares into which the Series A preferred shares are convertible. Preferred and ordinary shareholders vote together as a single class except for the election of the Company’s board of directors. For such election, holders of Series A preferred shares have the right to elect two directors and the holders of ordinary shares have a right to appoint one director.
9. Shareholders’ Equity
Ordinary Shares
At December 31, 2016 and 2017, the Company had 203,333,333 ordinary shares, $0.0003 par value, authorized for issuance, and there were 68,458,475 and 68,474,614 ordinary shares issued and outstanding, respectively.
In January 2017, the Company issued a warrant to purchase 231,989 ordinary shares to an affiliate of its interim Chief Financial Officer of Stealth BioTherapeutics Inc. at an exercise price of $1.38 per share. The warrant was fully vested as of December 31, 2017 and expires in January 2022. The Company recorded an expense of $156,983 within general and administrative expenses in the accompanying consolidated statement of operations for the year ended December 31, 2017. In June 2018, the warrant was amended and restated to be treated as an option agreement under the 2006 plan.
The voting, dividend and liquidation rights of holders of ordinary shares are subject to and qualified by the rights, powers and preferences of holders of Series A preferred shares. The rights and preferences of ordinary shares are as follows:
Voting—Holders are entitled to one vote for each ordinary share held at all meetings of shareholders and written action in lieu of meetings; there is no cumulative voting.
Dividends—Holders are entitled to receive dividends, if and when declared by the board of directors. Cash dividends may not be declared or paid to holders until paid on Series A preferred shares in accordance with its terms. No dividends have been declared.
Liquidation—After payment to the holders of Series A preferred shares of its liquidation preference, the holders of ordinary shares are entitled to share in the Company’s assets available for distribution on a pro rata basis, in the event of any voluntary or involuntary liquidation, dissolution or winding up of the Company or upon the occurrence of a deemed liquidation event.
F-17
Table of Contents
The Company has reserved for future issuances the following number of ordinary shares as of December 31, 2017:
2006 Share Incentive Plan | 25,516,081 | |||
Conversion of Series A preferred shares | 91,600,398 | |||
Exercise of ordinary share warrant | 231,989 | |||
Conversion of preferred share warrant | 162,500 | |||
|
| |||
Total | 117,510,968 | |||
|
|
10. Share Option Plan
The Company’s 2006 Share Incentive Plan, as amended, (the “2006 Plan”), provides for the grant of share options or other awards to employees, directors, advisers, and consultants for the purchase of up to 25,544,054 ordinary shares. Share options vest over varying schedules as determined by the Company’s board of directors and typically expire 10 years from the date of grant. Certain options provide for accelerated vesting if there is a change in control, as defined in the 2006 Plan. At December 31, 2017, there were 10,727,050 shares available for future grant.
In determining the exercise prices for options granted, the Company’s board of directors has considered the fair value of ordinary shares as of the grant date, based upon a variety of factors, including the results obtained from a third-party valuation, its financial position and financial performance, the status of technological developments of its proposed products, the composition and ability of the current scientific and management team, an evaluation or benchmark of its competition, the illiquid nature of the ordinary shares, sales of capital share including convertible preferred shares, the effect of the rights and preferences of Series A preferred shares, and the prospects of a liquidity event.
Total share-based compensation expense is as follows:
| YEAR ENDED DECEMBER 31, | ||||||||
| 2016 | 2017 | |||||||
Research and development | $ | 378,045 | $ | 722,277 | ||||
General and administrative | 1,454,946 | 564,693 | ||||||
|
|
|
| |||||
Total | $ | 1,832,991 | $ | 1,286,970 | ||||
|
|
|
| |||||
As of December 31, 2017, total unrecognized compensation expense related tonon-vested share options, net of related forfeiture estimates, was $1,827,032. The Company expects to recognize its remaining unrecognized share-based compensation expense over a weighted-average period of approximately 2.6 years.
The fair value of each share option granted to employees and directors was estimated on the date of grant using the following assumptions:
| YEAR ENDED DECEMBER 31, | ||||||||
| 2016 | 2017 | |||||||
Risk free interest rate | 1.23% - 2.42 | % | 1.89% - 2.83 | % | ||||
Expected dividend yield | — | — | ||||||
Expected term (in years) | 6.4 | 6.0 | ||||||
Expected volatility | 50% | 57% | ||||||
Underlying fair value of ordinary shares | $1.14 | $1.38 | ||||||
F-18
Table of Contents
The following table summarizes share option plan activity for the year ended December 31, 2017:
| NUMBER OF SHARES | WEIGHTED- AVERAGE EXERCISE PRICE | AVERAGE REMAINING CONTRACTUAL LIFE (IN YEARS) | AGGREGATE INTRINSIC VALUE | |||||||||||||
Outstanding at January 1, 2017 | 10,953,667 | $ | 0.87 | 7.9 | $ | 5,599,435 | ||||||||||
Granted | 4,301,900 | $ | 1.38 | |||||||||||||
Exercised | (16,139 | ) | $ | 0.66 | ||||||||||||
Cancelled or forfeited | (450,396 | ) | $ | 1.17 | ||||||||||||
|
| |||||||||||||||
Outstanding at December 31, 2017 | 14,789,032 | $ | 1.02 | 7.5 | $ | 3,580,527 | ||||||||||
|
| |||||||||||||||
Exercisable at December 31, 2017 | 10,265,876 | $ | 0.87 | 6.9 | $ | 3,442,241 | ||||||||||
|
| |||||||||||||||
Vested and expected to vest at December 31, 2017 | 13,161,820 | $ | 0.96 | 7.3 | $ | 3,557,007 | ||||||||||
|
| |||||||||||||||
The weighted average grant date fair value per share for awards granted during the years ended December 31, 2016 and December 31, 2017 was $0.58 and $0.74, respectively.
11. 401(k) Savings Plan
In 2014, the Company adopted atax-qualified employee savings and retirement 401(k) Plan, covering all qualified employees. Eligible employees may make pretax contributions to the 401(k) Plan up to statutory limits. The Company contributes up to 3% of an employee’s annual salary, within statutory limits. During the years ended December 31, 2016 and 2017, the Company contributed $228,422 and $267,989, respectively.
12. License Agreements
In 2006, the Company entered into a license agreement, as amended, with Cornell University and a research institute (collectively “licensor”) for certain intellectual property rights, and subsequently entered into four additional license agreements with Cornell. Under the terms of the original license agreement, the Company issued an aggregate of 666,667 ordinary shares to Cornell between 2006 and 2009. The Company has also paid $60,000 in license fees. The Company is also required to pay royalties on the commercial sale of products that result from the licensed intellectual property, as well as a percentage of any sublicensing revenue. Subject to specified reductions and royalty offset, such royalties are calculated as a tiered,low-to-mid single digit percentage of net sales of licensed products under each of the license agreements, except that for licensed products under the original agreement, such royalties are calculated as a tiered, low single-digit tosub-teen percentage of net sales, depending on patent coverage, amount of net sales and type of licensed product. Under this license agreement, if the Company fails to commercialize a product by December 31, 2020, the licensor may terminate the license, subject to specified exceptions for causes due to scientific, regulatory and other events over which we cannot exert direct control.
13. Commitments and Contingencies
Lease commitments
The Company’s U.S. subsidiary currently leases office space in Newton, Massachusetts under a lease that expires in November 2020 and the Company’s U.S. subsidiary has made a security deposit of $325,000, which is classified in other assets on the accompanying consolidated balance sheets.
The Company has accounted for the lease as an operating lease. Rent expense was $564,895 for each of the years ended December 31, 2016 and 2017. The expense is being recorded on a straight-line basis over the term of the lease. Incentives received from the landlord related to the operating lease are recorded as deferred rent. As of December 31, 2016 and 2017, the Company recorded deferred rent of $196,537 and $165,373, respectively, which is included in accrued expenses and other current liabilities on the accompanying consolidated balance sheet.
F-19
Table of Contents
Future minimum payments payable under all operating leases as of December 31, 2017 are as follows:
YEAR ENDING DECEMBER 31, | ||||
2018 | $ | 607,939 | ||
2019 | 622,385 | |||
2020 | 582,659 | |||
|
| |||
Total minimum lease payments | $ | 1,812,983 | ||
|
| |||
14. Income Taxes
As a Cayman Islands entity, Stealth BioTherapeutics Corp is not currently subject to taxation. Stealth BioTherapeutics Inc. is subject to U.S. income tax and certain state income taxes.
The following table presents domestic and foreign components of loss before income tax benefit for the periods presented:
| YEAR ENDED DECEMBER 31, | ||||||||
| 2016 | 2017 | |||||||
Domestic | $ | 480,149 | $ | 1,598,933 | ||||
Foreign | 60,569,333 | 81,310,894 | ||||||
|
|
|
| |||||
Loss before income tax benefit | $ | 61,049,482 | $ | 82,909,828 | ||||
|
|
|
| |||||
A reconciliation setting forth the differences between the Company’s effective tax rate and the U.S. statutory tax rate is as follows:
| YEAR ENDED DECEMBER 31, | ||||||||
| 2016 | 2017 | |||||||
Income tax benefit at federal statutory rate | $ | 162,567 | $ | 557,206 | ||||
State and local income taxes net of federal tax benefit | 334,773 | 254,703 | ||||||
Federal credits | 881,381 | 1,298,890 | ||||||
Federal rate change | — | (280,090 | ) | |||||
Nondeductible/nontaxable permanent items | (15,353 | ) | (11,849 | ) | ||||
Other | 21,169 | 1,406 | ||||||
Change in valuation allowance | (1,384,537 | ) | (1,820,266 | ) | ||||
|
|
|
| |||||
Income tax benefit | $ | — | $ | — | ||||
|
|
|
| |||||
Effective tax rate | 0.0 | % | 0.0 | % | ||||
|
|
|
| |||||
F-20
Table of Contents
The significant components of the Company’s deferred tax assets are as follows:
| YEAR ENDED DECEMBER 31, | ||||||||
| 2016 | 2017 | |||||||
Deferred tax assets: | ||||||||
Federal and state net operating loss carryforwards | $ | 606,265 | $ | 620,007 | ||||
Credits | 1,227,570 | 2,871,521 | ||||||
Deferred rent | 71,941 | 39,817 | ||||||
Other accrued liabilities | — | 55,961 | ||||||
Depreciation | — | 2,245 | ||||||
|
|
|
| |||||
Total deferred tax assets | 1,905,776 | 3,589,551 | ||||||
|
|
|
| |||||
Deferred tax liabilities: | ||||||||
Other accrued liabilities | 94,493 | — | ||||||
Depreciation | 41,998 | — | ||||||
|
|
|
| |||||
Total deferred tax liabilities | 136,491 | — | ||||||
|
|
|
| |||||
Valuation allowance | 1,769,285 | 3,589,551 | ||||||
|
|
|
| |||||
Net deferred tax liability | $ | — | $ | — | ||||
|
|
|
| |||||
As of December 31, 2017, Stealth BioTherapeutics Inc. had federal and state net operating loss carryforwards of $2,623,358 and $788,499, respectively. The net operating loss carryforwards expire at various dates beginning in 2034 through 2036 for U.S. and state tax purposes.
Realization of the future tax benefits is dependent on many factors, including the Company’s ability to generate taxable income within the net operating loss carryforward period. As of December 31, 2017, the Company maintains a full valuation allowance for its deferred tax assets due to uncertainty regarding their realization. Adjustments could be required in the future if the Company estimates that the amount of deferred tax assets to be realized is more or less than the net amount the Company has recorded. The valuation allowance increased $1,820,266 during the year ended December 31, 2017 due primarily to the generation of net operating losses during the period and the recognition of potential research and development tax credits.
The Company is not currently under any income tax examinations. Due to the Company’s net operating losses, all tax years generally remain open in each jurisdiction. No interest or penalties have been recorded on any unrecognized tax benefits since its inception. The Company does not believe material uncertain tax positions have arisen to date.
Under the provisions of Section 382 of the Internal Revenue Code of 1986, certain substantial changes in the Company’s ownership, including a sale of the Company, or significant changes in ownership due to sales of equity, may have limited, or may limit in the future, the amount of net operating loss carryforwards and tax credits, which could be used annually to offset future taxable income.
On December 22, 2017, The Tax Cuts and Jobs Act (the “Act)” was enacted. The Act significantly revised the U.S. corporate income tax law by lowering the corporate Federal income tax rate from 35% to 21%. As of December 31, 2017, the Company has assessed the effects of the corporate rate reduction on its existing deferred tax balances which resulted in a $280,090 reduction in the deferred tax assets. Since the Company maintains a full valuation allowance on its deferred tax assets, a corresponding reduction in the valuation allowance equal to the effect of the rate reduction on the ending deferred tax asset was also reflected. In addition to the rate reduction, the Act also requires companies with foreign subsidiaries to pay aone-time transition tax on earnings that were previously tax deferred. As of December 31, 2017, the Company does not have previously deferred foreign earnings subject to the transition tax.
F-21
Table of Contents
15. Net Loss Per Share Attributable to Ordinary Shareholders
Basic and diluted net loss per ordinary share are calculated as follows:
| YEAR ENDED DECEMBER 31, | ||||||||
| 2016 | 2017 | |||||||
Numerator: | ||||||||
Net loss attributable to ordinary shareholders—basic and diluted | $ | (61,049,482 | ) | $ | (82,909,827 | ) | ||
|
|
|
| |||||
Denominator: | ||||||||
Weighted-average ordinary shares used in net loss per share attributable to ordinary shareholders—basic and diluted | 68,165,325 | 68,472,262 | ||||||
|
|
|
| |||||
Net loss per share attributable to ordinary shareholders—basic and diluted | $ | (0.90 | ) | $ | (1.21 | ) | ||
|
|
|
| |||||
The following ordinary share equivalents, presented on an as converted basis, were excluded from the calculation of net loss per share for the periods presented, as their effect is anti-dilutive:
| YEAR ENDED DECEMBER 31, | ||||||||
| 2016 | 2017 | |||||||
Convertible preferred shares | 91,600,398 | 91,600,398 | ||||||
Preferred share warrants | — | 162,500 | ||||||
Ordinary share warrants | — | 231,989 | ||||||
Convertible notes payable to shareholder and accrued interest | — | 22,640,052 | ||||||
Outstanding share options | 10,953,667 | 14,789,032 | ||||||
|
|
|
| |||||
Total | 102,554,065 | 129,423,971 | ||||||
|
|
|
| |||||
Unaudited Pro Forma Net Loss Per Share
The unaudited pro forma basic and diluted net loss per share attributable to ordinary shareholders for the year ended December 31, 2017 has been prepared to give effect to adjustments arising upon the completion of a qualified IPO. The unaudited pro forma net loss attributable to ordinary shareholders used in the calculation of unaudited pro forma basic and diluted net loss per share attributable to ordinary shareholders does not include the effects of preferred share dividends because the calculation gives effect to the automatic conversion of all preferred shares and convertible debt outstanding as of December 31, 2017, respectively, into ordinary shares as if the proposed IPO had occurred on the later of January 1, 2017, or the issuance date of the preferred shares.
F-22
Table of Contents
The unaudited pro forma basic and diluted weighted-average ordinary shares outstanding used in the calculation of unaudited basic and diluted net loss per share attributable to ordinary shareholders for the year ended December 31, 2017 has been prepared to give effect, upon a qualified IPO, to the automatic conversion of all outstanding convertible preferred shares and convertible debt into ordinary shares as if the proposed IPO had occurred on the later of January 1, 2017, or the issuance date of the preferred shares. Pro forma basic and diluted net loss per share attributable to ordinary shareholders was calculated as follows:
IN THOUSANDS, EXCEPT SHARE AND PER SHARE DATA | YEAR ENDED DECEMBER 31, 2017 | |||
Numerator: | ||||
Net loss attributable to ordinary shareholders—basic and diluted | $ | (82,910 | ) | |
Add: Interest on convertible notes | 2,246 | |||
|
| |||
Pro forma net loss attributable to ordinary shareholders—basic and diluted | $ | (80,664 | ) | |
|
| |||
Denominator: | ||||
Weighted-average ordinary shares outstanding—basic and diluted | 68,472,262 | |||
Pro forma adjustment to reflect automatic conversion of convertible preferred shares to ordinary shares upon the completion of the proposed initial public offering | 91,600,398 | |||
Pro forma adjustment to reflect automatic conversion of convertible debt to ordinary shares upon the completion of the proposed initial public offering | 28,188,708 | |||
|
| |||
Pro forma weighted-average ordinary shares outstanding—basic and diluted | 188,261,368 | |||
|
| |||
Pro forma net loss per share attributable to ordinary shareholders—basic and diluted | $ | (0.43 | ) | |
|
| |||
16. Related Party
For the year ended December 31, 2016, the Company paid $107,500 for services provided by an entity affiliated with its Chief Executive Officer for services provided as its Chief Executive Officer. For the year ended December 31, 2016 and 2017, the Company paid $2,868 and $193,523, respectively, for services provided by an entity affiliated with its interim Chief Financial Officer for services provided as its Chief Financial Officer.
Except as disclosed elsewhere in the notes to the accompanying consolidated financial statements, there were no other material transactions with related parties.
17. Subsequent Events
The Company has completed an evaluation of all subsequent events through October 25, 2018 (December 28, 2018 for Note 18), the date these financial statements were available to be issued. Except as disclosed in Notes 1, 6, 7, 9 and 18, the Company has concluded that no subsequent events have occurred that require disclosure.
18. Reverse Share Split
The Company’s board of directors and shareholders approved a three for one reverse share split of its issued and outstanding ordinary shares and share options and a proportional adjustment to the existing conversion ratios for the Company’s preferred shares through a consolidation of its share capitalization effective as of December 28, 2018. Accordingly, all share and per share amounts for all periods presented in the accompanying financial statements and notes thereto have been retroactively adjusted, where applicable, to reflect the reverse share split.
F-23
Table of Contents
CONDENSED CONSOLIDATED BALANCE SHEETS
(unaudited)
| DECEMBER 31, | SEPTEMBER 30, | PRO FORMA SEPTEMBER 30, | ||||||||||
| 2017 | 2018 | 2018 | ||||||||||
Assets | ||||||||||||
Current assets: | ||||||||||||
Cash and cash equivalents | $ | 4,118,804 | $ | 4,078,286 | $ | 4,078,286 | ||||||
Prepaid expenses and other current assets | 1,801,203 | 951,775 | 951,775 | |||||||||
|
|
|
|
|
| |||||||
Total current assets | 5,920,007 | 5,030,061 | 5,030,061 | |||||||||
Property and equipment, net | 795,940 | 572,472 | 572,472 | |||||||||
Deferred offering costs | — | 5,621,698 | 5,621,698 | |||||||||
Othernon-current assets | 438,982 | 405,494 | 405,494 | |||||||||
|
|
|
|
|
| |||||||
Total assets | $ | 7,154,929 | $ | 11,629,725 | $ | 11,629,725 | ||||||
|
|
|
|
|
| |||||||
Liabilities, convertible preferred shares and shareholders’ deficit | ||||||||||||
Current liabilities: | ||||||||||||
Accounts payable | $ | 7,454,569 | $ | 8,826,256 | $ | 8,826,256 | ||||||
Accrued expenses and other current liabilities | 12,520,020 | 15,313,272 | 15,313,272 | |||||||||
Accrued interest payable | 2,525,685 | 5,024,558 | 634,473 | |||||||||
Current portion of long-term debt | 2,094,295 | 6,893,160 | 6,893,160 | |||||||||
|
|
|
|
|
| |||||||
Total current liabilities | 24,594,569 | 36,057,246 | 31,667,161 | |||||||||
|
|
|
|
|
| |||||||
Convertible notes payable | 50,000,000 | 78,142,465 | — | |||||||||
Long-term debt, less current portion | 11,956,867 | 12,467,422 | 12,467,422 | |||||||||
Derivative liability | — | 33,652,582 | — | |||||||||
Warrant liability | 512,618 | 386,349 | 386,349 | |||||||||
|
|
|
|
|
| |||||||
Total liabilities | 87,064,054 | 160,706,064 | 44,520,932 | |||||||||
|
|
|
|
|
| |||||||
Commitments and contingencies | ||||||||||||
Series A convertible preferred shares, $.0003 par value; 106,666,667 shares authorized; 91,600,398 issued and outstanding at December 31, 2017 and September 30, 2018; aggregate liquidation preference of $211,376,929 at December 31, 2017 and September 30, 2018; no shares issued and outstanding as of September 30, 2018 (pro forma) | 211,376,929 | 211,376,929 | — | |||||||||
Shareholders’ deficit: | ||||||||||||
Ordinary shares, $.0003 par value; 203,333,333 shares authorized and 68,474,614 shares issued and outstanding at December 31, 2017 and September 30, 2018; 750,000,000 shares authorized and 283,245,110 shares issued and outstanding at September 30, 2018 (pro forma) | 20,542 | 20,542 | 84,974 | |||||||||
Additionalpaid-in capital | 38,250,174 | 39,205,914 | 366,703,543 | |||||||||
Accumulated deficit | (329,556,770 | ) | (399,679,724 | ) | (399,679,724 | ) | ||||||
|
|
|
|
|
| |||||||
Total shareholders’ deficit | (291,286,054 | ) | (360,453,268 | ) | (32,891,207 | ) | ||||||
|
|
|
|
|
| |||||||
Total liabilities, convertible preferred shares and shareholders’ deficit | $ | 7,154,929 | $ | 11,629,725 | $ | 11,629,725 | ||||||
|
|
|
|
|
| |||||||
See the accompanying notes to these condensed consolidated financial statements.
F-24
Table of Contents
CONDENSED CONSOLIDATED STATEMENTS OF OPERATIONS
(unaudited)
| NINE MONTHS ENDED SEPTEMBER 30, | ||||||||
| 2017 | 2018 | |||||||
Operating expenses: | ||||||||
Research and development | $ | 46,212,164 | $ | 41,757,884 | ||||
General and administrative | 12,937,339 | 12,541,068 | ||||||
|
|
|
| |||||
Total operating expenses | 59,149,503 | 54,298,952 | ||||||
|
|
|
| |||||
Loss from operations | (59,149,503 | ) | (54,298,952 | ) | ||||
|
|
|
| |||||
Other income (expense): | ||||||||
Interest income | 26,394 | 140,783 | ||||||
Interest expense | (1,710,941 | ) | (14,422,008 | ) | ||||
Change in valuation of warrant liability | (5,964 | ) | 126,269 | |||||
Change in valuation of derivative liability | — | (1,669,046 | ) | |||||
|
|
|
| |||||
Total other income (expense), net | (1,690,511 | ) | (15,824,002 | ) | ||||
|
|
|
| |||||
Net loss attributable to ordinary shareholders | $ | (60,840,014 | ) | $ | (70,122,954 | ) | ||
|
|
|
| |||||
Net loss per share attributable to ordinary shareholders — basic and diluted | $ | (0.89 | ) | $ | (1.02 | ) | ||
|
|
|
| |||||
Weighted average ordinary shares used in net loss per share attributable to ordinary shareholders—basic and diluted | 68,471,469 | 68,474,614 | ||||||
|
|
|
| |||||
Pro forma net loss per share attributable to ordinary shareholders —basic and diluted | $ | (0.24 | ) | |||||
|
| |||||||
Pro forma weighted-average ordinary shares used in net loss per share attributable to ordinary shareholders—basic and diluted | 238,105,715 | |||||||
|
| |||||||
See the accompanying notes to these unaudited condensed consolidated financial statements
F-25
Table of Contents
CONDENSED CONSOLIDATED STATEMENTS OF CONVERTIBLE PREFERRED SHARES AND SHAREHOLDERS’ DEFICIT
(unaudited)
| SERIES A CONVERTIBLE PREFERRED SHARES | ORDINARY SHARES | ADDITIONAL PAID-IN CAPITAL | ACCUMULATED DEFICIT | TOTAL SHAREHOLDERS’ DEFICIT | ||||||||||||||||||||||||||||
| SHARES | AMOUNT | SHARES | AMOUNT | |||||||||||||||||||||||||||||
Balance at January 1, 2017 | 91,600,398 | 211,376,929 | 68,458,475 | 20,538 | 36,795,750 | (246,646,943 | ) | (209,830,655 | ) | |||||||||||||||||||||||
Exercise of share options | — | — | 16,139 | 4 | 10,471 | — | 10,475 | |||||||||||||||||||||||||
Share-based compensation expense | — | — | — | — | 977,643 | — | 977,643 | |||||||||||||||||||||||||
Issuance of warrant for ordinary shares | — | — | — | — | 156,983 | — | 156,983 | |||||||||||||||||||||||||
Net loss | — | — | — | — | — | (60,840,014 | ) | (60,840,014 | ) | |||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||||||
Balance at September 30, 2017 | 91,600,398 | $ | 211,376,929 | 68,474,614 | $ | 20,542 | $ | 37,940,847 | $ | (307,486,956 | ) | $ | (269,525,567 | ) | ||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||||||
Balance at December 31, 2017 | 91,600,398 | $ | 211,376,929 | 68,474,614 | $ | 20,542 | $ | 38,250,174 | $ | (329,556,770 | ) | $ | (291,286,054 | ) | ||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||||||
Share-based compensation expense | 955,740 | 955,740 | ||||||||||||||||||||||||||||||
Net loss | — | — | — | — | (70,122,954 | ) | (70,122,954 | ) | ||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||||||
Balance at September 30, 2018 | 91,600,398 | $ | 211,376,929 | 68,474,614 | $ | 20,542 | $ | 39,205,914 | $ | (399,679,724 | ) | $ | (360,453,268 | ) | ||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||||||
See the accompanying notes to these unaudited condensed consolidated financial statements
F-26
Table of Contents
CONDENSED CONSOLIDATED STATEMENTS OF CASH FLOWS
(unaudited)
| NINE MONTHS ENDED SEPTEMBER 30, | ||||||||
| 2017 | 2018 | |||||||
Cash flows from operating activities: | ||||||||
Net loss | $ | (60,840,014 | ) | $ | (70,122,954 | ) | ||
Adjustments to reconcile net loss to net cash used in operating activities: | ||||||||
Depreciation and amortization | 262,061 | 235,120 | ||||||
Change in fair value of warrant liability | 5,964 | (126,269 | ) | |||||
Change in fair value of derivative liability | — | 1,669,046 | ||||||
Issuance of warrant for ordinary shares | 156,983 | — | ||||||
Amortization of debt discount | 94,825 | 8,155,768 | ||||||
Write-off of deferred financing costs | 457,652 | — | ||||||
Non-cash interest expense | 1,288,807 | 4,808,463 | ||||||
Share-based compensation | 977,643 | 955,740 | ||||||
Changes in operating assets and liabilities: | ||||||||
Prepaid expenses and other current assets | (905,977 | ) | 861,063 | |||||
Accounts payable | 1,680,818 | 1,371,686 | ||||||
Accrued expenses, accrued interest payable and other current liabilities | 5,455,173 | 1,277,811 | ||||||
|
|
|
| |||||
Net cash used in operating activities | (51,366,065 | ) | (50,914,526 | ) | ||||
|
|
|
| |||||
Cash flows from investing activities: | ||||||||
Purchase of property and equipment | (160,952 | ) | (11,652 | ) | ||||
Changes in other assets | 21,451 | — | ||||||
|
|
|
| |||||
Net cash used in investing activities | (139,501 | ) | (11,652 | ) | ||||
|
|
|
| |||||
Cash flows from financing activities: | ||||||||
Proceeds from issuance of convertible notes payable from shareholder | 50,000,000 | — | ||||||
Proceeds from issuance of convertible notes payable | — | 50,000,000 | ||||||
Proceeds from long term debt issuance | 14,633,000 | 5,000,000 | ||||||
Payment of long term debt issuance costs | (225,783 | ) | — | |||||
Payment of convertible debt issuance costs | — | (55,826 | ) | |||||
Proceeds from repayment of shareholder demand note receivable | — | — | ||||||
Payment of deferred financing costs | — | (4,058,514 | ) | |||||
Proceeds from exercise of share options and warrant | 10,475 | — | ||||||
|
|
|
| |||||
Net cash provided by financing activities | 64,417,692 | 50,885,660 | ||||||
|
|
|
| |||||
Net decrease in cash and cash equivalents | 12,912,126 | (40,518 | ) | |||||
Cash and cash equivalents, beginning of period | 9,709,732 | 4,118,804 | ||||||
|
|
|
| |||||
Cash and cash equivalents, end of period | $ | 22,621,858 | $ | 4,078,286 | ||||
|
|
|
| |||||
Supplemental disclosure of noncash investing and financing activity: | ||||||||
Noncash items: | ||||||||
Fair value of warrants issued in connection with term loan | $ | 548,075 | $ | — | ||||
|
|
|
| |||||
Fair value of derivatives recorded in connection with the 2018 Shareholder Note and 2018 New Investor Notes | $ | — | $ | 31,983,535 | ||||
|
|
|
| |||||
Noncash conversion of accrued interest due to Shareholder into new convertible notes payable to Shareholder | $ | — | $ | 2,357,333 | ||||
|
|
|
| |||||
Deferred financing costs included in accrued expenses | $ | — | $ | 1,563,184 | ||||
|
|
|
| |||||
Supplemental cash flow information-Cash paid for interest | $ | 213,281 | $ | 1,410,035 | ||||
|
|
|
| |||||
See the accompanying notes to these unaudited condensed consolidated financial statements.
F-27
Table of Contents
NOTES TO UNAUDITED CONDENSED CONSOLIDATED FINANCIAL STATEMENTS
Nine months ended September 30, 2017 and 2018
1. Organization and Operations
The Company
Stealth BioTherapeutics Corp was incorporated in Grand Cayman, Cayman Islands as Stealth Peptides International, Inc. in April 2006. Its wholly owned subsidiary, Stealth BioTherapeutics Inc., was incorporated in Delaware as Stealth Peptides Inc. in October 2007. In addition, a wholly owned subsidiary, Stealth BioTherapeutics (HK) Limited, was incorporated in Hong Kong in September 2017. In May 2018, Stealth BioTherapeutics (Shanghai) Limited was formed as a wholly foreign owned enterprise in China. Hereinafter, Stealth BioTherapeutics Corp, Stealth BioTherapeutics Inc., Stealth BioTherapeutics (HK) Limited, and Stealth BioTherapeutics (Shanghai) Limited are referred to as the “Company.” The Company is a clinical stage biotechnology company focused on the discovery and development of novel pharmaceutical agents to treat patients suffering from diseases involving mitochondrial dysfunction through its mitochondrial medicine platform. The condensed consolidated financial statements include the assets and liabilities and operating results of the Company and its wholly owned subsidiaries. Since inception, the Company has devoted substantially all of its efforts to research and development, business planning, acquiring operating assets, seeking intellectual property protection for its technology and product candidates, and raising capital.
The Company has entered into numerous debt and equity issuances with Morningside Venture (I) Investments Limited (the “Shareholder”). As of September 30, 2018, the Shareholder held approximately 98% of the Company’s outstanding shares. See Notes 8 and 9. The Company has incurred net losses and negative cash flows from operations and had an accumulated deficit of $399.7 million as of September 30, 2018. The Company has financed its operations to date from the issuance of preferred shares, ordinary shares, convertible debt, as well as long term debt.
Liquidity and Going Concern
These condensed consolidated financial statements have been prepared on a going concern basis, which assumes the realization of assets and settlement of liabilities in the normal course of business. Since its inception, the Company has incurred recurring losses, including net losses of $70.1 million for the nine months ended September 30, 2018. The Company expects to continue to incur operating losses in the foreseeable future.
Management believes that cash and cash equivalents of $4.1 million at September 30, 2018, together with the proceeds of $25.0 million received in October and December 2018 under the 2018 Shareholder Note (Note 8), along with an additional borrowing availability of $5.0 million (Note 8), will be sufficient to fund operating expenses into the first quarter of 2019. The Company may seek to obtain financing through equity and debt issuances, collaborative agreements, and grants from government and private sponsors. Because the ability to obtain additional financing is outside of the Company’s control, the foregoing conditions raise substantial doubt in regard to the Company’s ability to continue as a going concern. If the Company is unable to obtain additional funding when needed, or to the extent needed, it may be necessary to scale back operations or halt certain research and development activities, which could prevent the Company from successfully executing on its operating plan. The condensed consolidated financial statements do not include any adjustments related to the recoverability and classification of recorded assets or liabilities that might be necessary should the Company be unable to continue its operations.
2. Summary of Significant Accounting Policies
Basis of Presentation and Use of Estimates
The Company’s significant accounting policies are disclosed in the audited consolidated financial statements for the year ended December 31, 2017, included elsewhere in this prospectus. Since the date of those financial statements, there have been no changes to its significant accounting policies.
F-28
Table of Contents
Unaudited Interim Financial Information
The accompanying unaudited condensed consolidated financial statements have been prepared by the Company in accordance with accounting principles generally accepted in the United States, or GAAP, for interim financial reporting and as required by Regulation S-X, Rule 10-01. The unaudited condensed consolidated financial statements have been prepared on the same basis as the audited annual financial statements and, in the opinion of management, reflect all adjustments, which include only normal recurring adjustments, necessary for a fair statement of the Company’s financial position as of September 30, 2018 and the results of its operations and its cash flows for the nine months ended September 30, 2017 and 2018. The financial data and other information disclosed in these notes related to the nine months ended September 30, 2017 and 2018 are unaudited. The results for the nine months ended September 30, 2018 are not necessarily indicative of results to be expected for the year ending December 31, 2018, any other interim periods, or any future year or period.
Unaudited Pro Forma Information
Upon the completion of the Company’s initial public offering (“IPO”), all outstanding Series A convertible preferred shares and the outstanding aggregate principal amount of, and all accrued and unpaid interest on, the Company’s outstanding convertible notes will each automatically convert into the Company’s ordinary shares. The accompanying unaudited pro forma balance sheet information has been prepared assuming (1) the automatic conversion of the Series A convertible preferred shares outstanding into 91,600,398 ordinary shares of the Company upon the completion of the IPO and (2) the automatic conversion of an aggregate principal amount of $102.4 million and all accrued and unpaid interest on the Company’s outstanding convertible promissory notes into 123,170,098 ordinary shares upon the closing of the IPO.
The pro forma net loss per share applicable to ordinary shareholders is computed using the weighted-average number of ordinary shares outstanding after giving effect to the conversion of all outstanding convertible preferred shares and convertible debt into ordinary shares as if such conversion had occurred on January 1, 2018, or the date of original issuance, if later.
The Company believes that the unaudited pro forma net income (loss) per share disclosure provides material information to investors because the conversion of the convertible preferred shares and the convertible notes into ordinary shares is expected to occur upon the closing of the IPO and, therefore, that the disclosure of pro forma net income (loss) per share provides a measure of net income (loss) per share that is comparable to what will be reported as a public company.
Deferred Offering Costs
The Company capitalizes certain legal, professional accounting and other third-party fees that are directly associated within-process equity financings as deferred offering costs until such financings are consummated. After consummation of the equity financing, these costs are recorded in shareholders’ (deficit) equity as a reduction of proceeds generated as a result of the offering.
Should a planned equity financing be abandoned, the deferred offering costs would be expensed immediately as a charge to operating expenses in the consolidated statement of operations. The Company recorded deferred offering costs of $5.6 million as of September 30, 2018 and are included in othernon-current assets.
F-29
Table of Contents
3. Fair Value of Financial Assets and Liabilities
Fair Value Hierarchy
Fair value is defined as the exchange price that would be received for an asset or paid to transfer a liability (an exit price) in the principal or most advantageous market for the asset or liability in an orderly transaction between market participants on the measurement date. Valuation techniques used to measure fair value are performed in a manner to maximize the use of observable inputs and minimize the use of unobservable inputs. The accounting standard describes a fair value hierarchy based on three levels of inputs, of which the first two are considered observable and the last unobservable, that may be used to measure fair value, which are the following:
Level 1—Quoted prices in active markets that are accessible at the market date for identical unrestricted assets or liabilities.
Level2—lnputs other than Level 1 that are observable, either directly or indirectly, such as quoted prices for similar assets or liabilities; quoted prices in markets that are not active; or other inputs for which all significant inputs are observable or can be corroborated by observable market data for substantially the full term of the assets or liabilities.
Level3—Unobservable inputs that are supported by little or no market activity and that are significant to the fair value of the assets or liabilities.
The following table presents information about the Company’s financial assets and liabilities measured at fair value on a recurring basis and indicate the level of the fair value hierarchy utilized to determine such fair values as of December 31, 2017 and September 30, 2018:
| FAIR VALUE MEASUREMENTS AS OF DECEMBER 31, 2017 USING | ||||||||||||||||
| LEVEL 1 | LEVEL 2 | LEVEL 3 | TOTAL | |||||||||||||
Assets: | ||||||||||||||||
Short-term U.S. Treasury securities | $ | 4,118,804 | — | — | $ | 4,118,804 | ||||||||||
|
|
|
|
|
|
|
| |||||||||
Total financial assets | $ | 4,118,804 | — | — | $ | 4,118,804 | ||||||||||
|
|
|
|
|
|
|
| |||||||||
Liabilities: | ||||||||||||||||
Warrant liability | $ | — | $ | — | $ | 512,618 | $ | 512,618 | ||||||||
|
|
|
|
|
|
|
| |||||||||
Total financial liabilities | $ | — | $ | — | $ | 512,618 | $ | 512,618 | ||||||||
|
|
|
|
|
|
|
| |||||||||
| FAIR VALUE MEASUREMENTS AS OF SEPTEMBER 30, 2018 USING | ||||||||||||||||
| LEVEL 1 | LEVEL 2 | LEVEL 3 | TOTAL | |||||||||||||
Assets: | ||||||||||||||||
Short-term U.S. Treasury securities | $ | 4,078,286 | — | — | $ | 4,078,286 | ||||||||||
|
|
|
|
|
|
|
| |||||||||
Total financial assets | $ | 4,078,286 | $ | — | $ | — | $ | 4,078,286 | ||||||||
|
|
|
|
|
|
|
| |||||||||
Liabilities: | ||||||||||||||||
Derivative liability | $ | — | $ | — | $ | 33,652,582 | $ | 33,652,582 | ||||||||
Warrant liability | — | — | $ | 386,349 | $ | 386,349 | ||||||||||
|
|
|
|
|
|
|
| |||||||||
Total financial liabilities | $ | — | $ | — | $ | 34,038,931 | $ | 34,038,931 | ||||||||
|
|
|
|
|
|
|
| |||||||||
As of December 31, 2017 and September 30, 2018, the carrying amounts of cash, accounts payable, and accrued expenses approximated their estimated fair values because of the short-term nature of these financial instruments. The Company’s cash equivalents, which are in money market funds and U.S. treasury securities, are classified within Level 1 of the fair value hierarchy because they are valued using quoted prices as of December 31, 2017 and September 30, 2018.
F-30
Table of Contents
As of December 31, 2017 and September 30, 2018, the outstanding debt from Loan (Note 7) and convertible debt obligations (Note 8) bear interest at rates which approximate prevailing market rates for instruments with similar characteristics and, accordingly, the carrying values for these instruments approximate fair value.
Warrant Liability
As consideration for the Company’s Term Loan (see Note 7), the Company and the lender entered into a Warrant Agreement. The warrant was recorded as a liability at fair value upon issuance. The warrant is recorded at fair value on our condensed consolidated balance sheet as a liability and discount to the Loan. It is subject to revaluation at each balance sheet date, and any changes in value are recorded as a component of gain or loss from valuation of warrant liability, until the earlier of their exercise or expiration or upon the completion of a liquidation event.
The estimated fair value of the Warrant was remeasured as of September 30, 2017, using a Black-Scholes model with the following assumptions: volatility of 66.7%, expected term of 9.75 years, risk-free interest rate of 2.3%, fair value of Series A preferred of $2.43 and a zero dividend yield. The resulting estimated fair value of the warrant liability was $554,039.
In 2018, the Company revised its valuation model for the Warrant to consider various liquidity scenarios. The scenarios were based on the probability and estimated timing of a liquidity event including short term IPO, long term IPO, equity financing or a sale of the Company. The Company then used a Black-Scholes model which incorporates assumptions and estimates, to value the warrant under the various liquidity scenarios. The estimated fair value of the Warrant as of September 30, 2018, used the following assumptions: volatility of 74%, expected term of 8.25 years, risk-free interest rate of 2.9%, fair value of Series A preferred of $2.97 and a zero dividend yield. The resulting estimated fair value of the warrant liability was $386,349.
The following table presents our warrant liability measured at fair value using unobservable inputs (Level 3) as of the nine months ended September 30, 2017 and 2018:
Fair value at January 1, 2017 | $ | — | ||
Initial fair value of warrant liability | 548,075 | |||
Change in fair value of warrant liability | 5,964 | |||
|
| |||
Fair value at September 30, 2017 | $ | 554,039 | ||
|
| |||
Fair value at December 31, 2017 | $ | 512,618 | ||
Change in fair value of warrant liability | (126,269 | ) | ||
|
| |||
Fair value at September 30, 2018 | $ | 386,349 | ||
|
|
Significant increases or decreases in any of the probabilities of success or changes in expected timelines for achievement of any of these scenarios could result in a significantly higher or lower fair value of the liability.
Derivative Liability
The Company evaluated the 2018 New Investor Notes Note (see Note 8 for description of convertible notes issued) and concluded that certain of the redemption and conversion features met the bifurcation criteria under ASC 815, Derivatives and Hedging, that should be accounted for separately from the debt (“Derivative Liability”). The Derivative Liability is recorded at fair value on our consolidated balance sheet as a liability and subject to revaluation at each balance sheet date, and any changes in value are recorded as a component of gain or loss in the change in valuation of derivative liability on the statements of operations.
In January 2018, upon the issuance of the first note in the amount of $15.0 million as well as the exchange note of $52.4 million, the identified embedded derivatives were initially valued using a Monte Carlo simulation. The simulation took into consideration the probability of four scenarios: subsequent financing at 10% probability, short term IPO at 20% probability, long term IPO at 50% probability, and change of control at a 20% probability. Other assumptions included a forecast horizon of 2.0 years, the present value of the Company’s equity, and expected volatility of 82%. The resulting fair value of the derivatives was $19.3 million.
F-31
Table of Contents
In April 2018, upon the issuance of the second note in the amount of $5.0 million, the embedded derivative was initially valued using a Monte Carlo simulation. The simulation took into consideration the probability of four scenarios: subsequent financing at 10% probability, short term IPO at 30% probability, long term IPO at 40% probability, and change of control at a 20% probability. Other assumptions included a forecast horizon of 1.8 years, the present value of the Company’s equity, and expected volatility of future equity of 83%. The resulting derivative fair value is $1.4 million.
In May 2018, upon the issuance of additional notes in the amount of $30.0 million, the embedded derivatives were initially valued using a Monte Carlo simulation. The simulation took into consideration the probability of four scenarios: subsequent financing at 10% probability, short term IPO at 40% probability, long term IPO at 30% probability, and change of control at a 20% probability. Other assumptions included a forecast horizon of 1.6 years, the present value of the Company’s equity, and expected volatility of future equity of 79%. The resulting derivative fair value is $11.2 million.
As of September 30, 2018, the fair value of the Derivative Liability wasre-measured using the Monte Carlo simulation. The simulation took into consideration the probability of four scenarios: subsequent financing at 10% probability, short term IPO at 20% probability, long term IPO at 50% probability, and change of control at a 20% probability. Other assumptions included a forecast horizon of 2.0 years, the present value of the Company’s equity, and expected volatility of future equity of 63%. The resulting fair value of the derivative was $33.7 million.
The following table presents our Derivative Liability measured at fair value using unobservable inputs (Level 3) as of the nine months ended September 30, 2018:
Fair value at January 1, 2018 | $ | — | ||
Initial fair value of Derivative Liability | 31,983,535 | |||
Change in fair value of Derivative Liability | 1,669,047 | |||
|
| |||
Fair value at September 30, 2018 | $ | 33,652,582 | ||
|
|
Significant increases or decreases in any of the probabilities of success or changes in expected timelines for achievement of any of these scenarios could result in a significantly higher or lower fair value of the liability.
There have been no transfers between fair value measure levels during the year ended December 31, 2017 and for the nine months ended September 30, 2018.
4. Prepaid Expenses and Other Current Assets
Prepaid expenses and other current assets consist of the following:
| AS OF DECEMBER 31, | AS OF SEPTEMBER 30, | |||||||
| 2017 | 2018 | |||||||
Research and development | $ | 1,527,711 | $ | 592,242 | ||||
Prepaid insurance | 49,013 | 117,639 | ||||||
Other | 224,479 | 241,894 | ||||||
|
|
|
| |||||
Total | $ | 1,801,203 | $ | 951,775 | ||||
|
|
|
| |||||
F-32
Table of Contents
5. Property and Equipment, Net
Property and equipment, net consists of the following:
| AS OF DECEMBER 31, | AS OF SEPTEMBER 30, | |||||||
| 2017 | 2018 | |||||||
Computer equipment and software | $ | 354,903 | $ | 366,555 | ||||
Furniture, fixtures and other | 718,955 | 718,955 | ||||||
Laboratory equipment | 376,806 | 376,806 | ||||||
Leasehold improvements | 374,097 | 374,097 | ||||||
|
|
|
| |||||
| 1,824,761 | 1,836,413 | |||||||
Accumulated depreciation | (1,028,821 | ) | (1,263,941 | ) | ||||
|
|
|
| |||||
Property and equipment, net | $ | 795,940 | $ | 572,472 | ||||
|
|
|
| |||||
Depreciation expense for the nine months ended September 30, 2017 and 2018 was $262,061 and $235,120, respectively.
6. Accrued Expenses and Other Current Liabilities
Accrued expenses and other current liabilities consist of the following:
| AS OF DECEMBER 31, | AS OF SEPTEMBER 30, | |||||||
| 2017 | 2018 | |||||||
Research and development | $ | 9,272,095 | $ | 9,672,416 | ||||
Employee compensation costs | 2,060,991 | 2,037,398 | ||||||
Consulting and professional services | 542,436 | 2,729,687 | ||||||
Legal expenses | 407,923 | 513,221 | ||||||
Deferred rent | 165,373 | 133,993 | ||||||
Other | 71,202 | 226,557 | ||||||
|
|
|
| |||||
Total | $ | 12,520,020 | $ | 15,313,272 | ||||
|
|
|
| |||||
7. Debt
Term Loan
In June 2017, the Company entered into a Loan and Security Agreement (the “LSA”) with a lender which permits the Company to borrow up to an aggregate principal amount of $40.0 million through a multiple tranche term loan (the “Loan”). The tranche advances are based on the Company achieving certain performance milestones as defined in the LSA. Upon closing of the Loan, the Company drew the first tranche less expenses, which resulted in net proceeds of $12.1 million. In September 2017, the Company drew the second tranche advance of $2.5 million upon achieving the first milestone. In March 2018, the Company drew the third tranche advance of $5.0 million upon achieving a second milestone, bringing the total gross amount borrowed to $20.0 million as of September 30, 2018.
The Loan included a $200,000 facility charge, which was paid to the lender on the closing date. The Company paid a $30,000 due diligence fee prior to the Loan closing, and the Company incurred additional cash expenses of $362,783 related to the Loan. These three amounts were all recorded as a debt discount and are being amortized as interest expense using the effective interest method over the life of the Loan. The Loan also includes an end of term charge equal to the greater of $750,000 or 5% of the aggregate principal amount of all advances. The end of term charge is being accrued and recorded to interest expense over the life of the Loan using the effective interest method.
F-33
Table of Contents
The Loan bears interest at the greater of (i) the prime rate plus 5.5% or (ii) 9.5%. As of September 30, 2018, the interest rate was 10.75%. Interest accrues from the closing date and interest payments are due monthly in arrears on the first of the month. Payments under the Loan are interest only for the first twelve months after closing followed by a30-month amortization period of principal and interest that were scheduled to begin on August 1, 2018 and continue through the scheduled maturity date of January 1, 2021. During 2018, the Loan was amended to, among other things, postpone the principal payments to December 1, 2018 and possibly further to April 30, 2019 depending upon the achievement of certain milestones. These amendments to the Loan were accounted for as a debt modification. For consideration of the amendments, the Company agreed to pay an additional end of term charge of $250,000 at maturity which is being accrued and recorded to interest expense over the life of the loan using the effective interest method.
The Company’s obligations to the lender are secured by a first priority security interest in substantially all of its assets, excluding intellectual property (“IP”). The lender maintains a negative pledge on IP with a security interest in the proceeds of the sale of the IP. The Loan contains certain covenants related to restrictions on payments for certain investments, additional debt, distributions and transfers.
As consideration for the Loan, the Company and the lender entered into a Warrant Agreement (“Warrant”), pursuant to which the lender, as Warrant holder, has the right to purchase a quantity of shares equal to the quotient derived by dividing (a) the Warrant coverage by (b) the exercise price. Warrant coverage means the greater of (a) $312,500 plus 2.5% of future tranche advances in the event all or part of the tranches are funded or (b) $375,000. The exercise price is (a) the purchase price of Series A preferred shares (“Series A preferred”), $2.30769 per share, or (b) the price per share paid in the next equity round of financing of ordinary shares or preferred shares, which results in aggregate gross proceeds of at least $30 million. As of September 30, 2018, the exercise price, share type and amount of shares had not been fully defined. The Warrant was exercisable beginning in June 2017, in whole or in part, and expires in ten years. The Warrant was recorded as a liability and a discount to the debt. The discount on the debt is being amortized through interest expense using the effective interest rate method over the remaining term of the Loan. See Note 3 for fair value considerations and disclosures.
In addition, the lender can declare a material adverse effect while monitoring our business, operations, properties, assets or financial condition. A material adverse effect is considered an event of default under the LSA. In the event of default, repayment of amounts due under the Loan may be accelerated by the lender.
Future principal payments under the Loan as of September 30, 2018 are as follows:
2018 | $ | 686,547 | ||
2019 | 8,710,804 | |||
2020 | 9,706,175 | |||
2021 | 896,474 | |||
|
| |||
Total future principal payments | 20,000,000 | |||
|
| |||
Less unamortized debt discount | 639,418 | |||
|
| |||
Total balance as depicted on the balance sheet | $ | 19,360,582 | ||
|
| |||
Term loan—current portion | 6,893,160 | |||
Termloan—non-current portion | 12,467,422 | |||
|
| |||
Total balance as depicted on the balance sheet | $ | 19,360,582 | ||
|
|
Interest expense related to the Loan for the nine months ended September 30, 2017 and 2018 was $486,941 and $2,074,466, respectively. Accrued interest as of September 30, 2018 was $634,473.
F-34
Table of Contents
8. Convertible Notes Payable and Shareholder Demand Note Receivable
During the year ended December 31, 2017, the Company issued six convertible promissory notes payable to the Shareholder, resulting in proceeds of $50.0 million (the “2017 Shareholder Notes”).The notes accrue interest at 8% per annum. Effective upon the closing of a qualified financing, as defined, the outstanding principal and accrued interest will automatically convert into shares of the same class and series of our shares issued to other investors in the qualified financing. The Shareholder also has the right to convert some or all of the outstanding amount into shares of Series A preferred shares at a conversion price of $2.30769 after December 31, 2018. In January 2018, the Company entered into a note exchange agreement with the Shareholder in the amount of $52.4 million, which represents the total principal and accrued interest of the 2017 Shareholder Notes at the time of the execution of the note exchange agreement. The exchange terminated the 2017 Shareholder Notes and created a new convertible note under substantially the same terms as the notes described in the following paragraph. The note exchange agreement was accounted for as a debt extinguishment and resulted in no gain or loss upon recognition of the new debt.
In January 2018, the Company entered into a note purchase agreement with new investors (as amended, the “2018 Agreement”), whereby the Company may borrow an aggregate principal amount of $30.0 million in exchange for notes convertible into ordinary shares of the Company. In April 2018, the note purchase agreement was amended to allow the Company to borrow up to $65.0 million in the aggregate. Under the 2018 Agreement, between January and May 2018, the Company issued notes in an aggregate principal amount of $50.0 million (the “2018 New Investor Notes”). The 2018 New Investor Notes accrue interest at 7% per annum. Accrued interest on the 2018 New Investor Notes compounds annually. The 2018 New Investor Notes, as amended, are convertible upon (i) the closing of an initial public offering or (ii) a subsequent financing occurring after January 10, 2019. Effective upon the closing of a qualified financing, as defined, the outstanding principal and accrued interest plus a 25% premium, defined as the sum of principal plus interest multiplied by 25%, will automatically convert into shares of the same class and series of our shares issued to other investors in the qualified financing. Unless the outstanding amount of the 2018 New Investor Notes are earlier repaid, retired, discharged, or automatically converted into shares of the Company upon the occurrence of events discussed below, all amounts outstanding become due and payable on the later of (i) January 10, 2020 and (ii) five business days after the date on which the term loan is repaid, terminated and discharged in full.
The Company evaluated the 2018 New Investor Notes as well as the exchange agreement and concluded that certain of the redemption and conversion features met the bifurcation criteria under ASC 815,Derivatives and Hedging, that should be accounted for separately from the debt.
The Derivative Liability is recorded at fair value on our consolidated balance sheet as a liability and subject to revaluation at each balance sheet date, and any changes in value are recorded as a component of gain or loss in the change in valuation of derivative liability on the statements of operations. The initial values of the derivative, along with legal fees, were recorded as a debt discount and are being amortized as interest expense using the effective interest method over the life of the note. See Note 3 for fair value considerations and disclosures.
In October 2018, the Company entered into an additional note purchase agreement with the Shareholder (the “2018 Shareholder Note”), whereby the Company may borrow an aggregate principal amount of up to $30.0 million, of which it has borrowed $25.0 million. The notes contain similar terms as the notes described in the paragraph above describing the 2018 New Investor Notes. The 2018 Shareholder Note is convertible upon a qualified initial public offering of our ordinary shares in the United States at the initial public offering price per share. Effective upon the closing of a qualified financing, the outstanding principal and accrued interest plus a 25% premium of such principal and interest will automatically convert into shares of the same class and series of our shares issued to other investors in the qualified financing. The 2018 Shareholder Note accrues interest at 7% per annum and accrued interest compounds annually, and upon such compounding, is added to the outstanding principal amount. Unless earlier converted into shares, the 2018 Shareholder Note becomes due and payable on the later of (i) October 3, 2020 and (ii) five business days after the date on which the Loan is repaid, terminated and discharged in full.
Interest expense for the nine months ended September 30, 2017 and 2018 was $1,224,000 and $12,347,543, respectively.
F-35
Table of Contents
9. Convertible Preferred Shares
At December 31, 2017 and September 30, 2018, the Company had authorized 106,666,667 shares of Series A preferred, $0.0003 par value, and there were 91,600,398 shares issued and outstanding.
The rights and preferences of the Series A preferred are as follows:
Conversion—At any time at the holder’s request and automatically upon the closing of a qualified IPO or sale of the Company, Series A preferred is convertible into ordinary shares at a ratio which is computed by dividing the original issue price by the applicable conversion price. A qualified IPO is defined under our articles of association as a fully underwritten public offering of ordinary shares in which aggregate gross proceeds equal or exceed $35 million pursuant to an effective registration statement under the Securities Act or in a jurisdiction outside of the United States. The initial conversion price of $2.30769 may be adjusted if and whenever the Company subsequently issues or sells ordinary shares or Series A preferred at a per share price that is less than the conversion price in effect at that time. At September 30, 2018, the applicable conversion ratio was 1:1.
Dividends—Series A preferred is entitled to receive, when and as declared by the board of directors, preferential cash dividends at a rate at least equal to 8% of the original issue price. Such dividends are not cumulative. No dividends have been declared.
Redemption Rights—Series A preferred does not have any stated redemption rights.
Liquidation Rights—In the event of a liquidation, dissolution, orwinding-up of the Company, Series A preferred shall be paid an amount first out of legally available funds available for distribution to holders of the Company’s capital share an amount equal to $2.30769 per share, plus all declared but unpaid dividends with respect to each such shares, as adjusted for any share dividend, share split, recapitalization, or other similar event. After payment of all preferential amounts, any assets and funds of the Company that remain available shall be distributed on a pro rata basis among the holders of ordinary shares.
Voting Rights—Series A preferred is entitled to the number of votes equal to the number of ordinary shares into which the Series A preferred is convertible. Preferred and ordinary shareholders vote together as a single class except for the election of the Company’s board of directors. For such election, holders of Series A preferred have the right to elect two directors and the holders of ordinary shares have a right to appoint one director.
10. Shareholders’ Equity
Ordinary Shares
At December 31, 2017 and September 30, 2018, 203,333,333 ordinary shares, $0.0003 par value, were authorized for issuance, and 68,474,614 ordinary shares were issued and outstanding.
In January 2017, the Company issued a warrant to purchase 231,989 ordinary shares to an affiliate of the interim Chief Financial Officer of Stealth BioTherapeutics Inc. at an exercise price of $1.38 per share. The warrant was fully vested as of December 31, 2017 and expires in January 2022. The Company recorded an expense of $156,983 and $0 within general and administrative expenses in the accompanying condensed consolidated statement of operations for the nine months ended September 30, 2017 and 2018, respectively. In June 2018, the warrant was amended and restated to be treated as an option agreement under the Company’s 2006 Share Incentive Plan.
F-36
Table of Contents
The voting, dividend and liquidation rights of holders of ordinary shares are subject to and qualified by the rights, powers and preferences of holders of Series A preferred. The rights and preferences of ordinary shares are as follows:
Voting—Holders are entitled to one vote for each ordinary share held at all meetings of shareholders and written action in lieu of meetings; there is no cumulative voting.
Dividends—Holders are entitled to receive dividends, if and when declared by the board of directors. Cash dividends may not be declared or paid to holders until paid on Series A preferred in accordance with its terms. No dividends have been declared.
Liquidation—After payment to the holders of Series A preferred of its liquidation preference, the holders of ordinary shares are entitled to share in the Company’s assets available for distribution on a pro rata basis, in the event of any voluntary or involuntary liquidation, dissolution or winding up of the Company or upon the occurrence of a deemed liquidation event.
The Company has reserved for future issuances the following number of ordinary shares as of September 30, 2018:
2006 Share Incentive Plan | 25,516,081 | |||
Conversion of Series A preferred | 91,600,398 | |||
Conversion of Series A preferred warrant | 216,667 | |||
|
| |||
Total | 117,333,146 | |||
|
|
11. Share Option Plan
The Company’s 2006 Share Incentive Plan, as amended, (the “2006 Plan”), provides for the grant of share options or other awards to employees, directors, advisers, and consultants for the purchase of up to 25,544,054 ordinary shares. Share options vest over varying schedules as determined by the Company’s board of directors and typically expire 10 years from the date of grant. Certain options provide for accelerated vesting if there is a change in control, as defined in the 2006 Plan. At September 30, 2018, there were 9,965,096 shares available for future grant.
In determining the exercise prices for options granted, the Company’s board of directors has considered the fair value of ordinary shares as of the grant date, based upon a variety of factors, including the results obtained from a third-party valuation, its financial position and financial performance, the status of technological developments of its proposed products, the composition and ability of the current scientific and management team, an evaluation or benchmark of its competition, the illiquid nature of the ordinary shares, sales of capital share including convertible preferred shares, the effect of the rights and preferences of Series A preferred shares, and the prospects of a liquidity event.
Total share-based compensation expense is as follows:
| NINE MONTHS ENDED SEPTEMBER 30, | ||||||||
| 2017 | 2018 | |||||||
Research and development | $ | 558,787 | $ | 438,352 | ||||
General and administrative | 418,856 | 517,388 | ||||||
|
|
|
| |||||
Total | $ | 977,643 | $ | 955,740 | ||||
|
|
|
| |||||
As of September 30, 2018, total unrecognized compensation expense related tonon-vested share options, net of related forfeiture estimates, was $1,980,935. The Company expects to recognize its remaining unrecognized share-based compensation expense over a weighted-average period of approximately 2.5 years.
F-37
Table of Contents
The fair value of each share option granted to employees and directors was estimated on the date of grant using the following assumptions:
| NINE MONTHS ENDED SEPTEMBER 30, | ||
| 2018 | ||
Risk free interest rate | 2.65% - 3.02% | |
Expected dividend yield | — | |
Expected term (in years) | 6.1 | |
Expected volatility | 59% |
The following table summarizes share option plan activity for the nine months ended September 30, 2018:
| NUMBER OF SHARES | WEIGHTED- AVERAGE EXERCISE PRICE | AVERAGE REMAINING CONTRACTUAL LIFE (IN YEARS) | AGGREGATE INTRINSIC VALUE | |||||||||||||
Outstanding at December 31, 2017 | 14,789,032 | $ | 1.02 | 7.5 | $ | 3,580,527 | ||||||||||
Granted | 1,756,572 | $ | 1.20 | |||||||||||||
Cancelled or forfeited | (994,618 | ) | $ | 1.29 | ||||||||||||
|
| |||||||||||||||
Outstanding at September 30, 2018 | 15,550,986 | $ | 1.05 | 6.9 | $ | 7,781,308 | ||||||||||
|
| |||||||||||||||
Exercisable at September 30, 2018 | 11,427,608 | $ | 0.81 | 6.3 | $ | 6,884,182 | ||||||||||
|
| |||||||||||||||
Vested and expected to vest at September 30, 2018 | 14,297,882 | $ | 1.02 | 6.7 | $ | 7,529,751 | ||||||||||
|
| |||||||||||||||
The weighted average grant date fair value per share for awards granted during the nine months ended September 30, 2018 was $0.82.
12. Income Taxes
During the year ended December 31, 2017 and nine months ended September 30, 2018, the Company recorded a full valuation allowance on federal and state deferred tax assets since management does not forecast the Company to be in a profitable position in the near future.
13. Net Loss Per Share Attributable to Ordinary Shareholders
Basic and diluted net loss per ordinary share are calculated as follows:
| NINE MONTHS ENDED SEPTEMBER 30, | ||||||||
| 2017 | 2018 | |||||||
Numerator: | ||||||||
Net loss attributable to ordinary shareholders—basic and diluted | $ | (60,840,014 | ) | $ | (70,122,954 | ) | ||
|
|
|
| |||||
Denominator: | ||||||||
Weighted-average ordinary shares used in net loss per share attributable to ordinary shareholders—basic and diluted | 68,471,469 | 68,474,614 | ||||||
|
|
|
| |||||
Net loss per share attributable to ordinary shareholders—basic and diluted | $ | (0.89 | ) | $ | (1.02 | ) | ||
|
|
|
| |||||
F-38
Table of Contents
The following ordinary share equivalents, presented on an as converted basis, were excluded from the calculation of net loss per share for the periods presented, as their effect is anti-dilutive:
| NINE MONTHS ENDED SEPTEMBER 30, | ||||||||
| 2017 | 2018 | |||||||
Convertible preferred Series A | 91,600,398 | 91,600,398 | ||||||
Preferred Series A share warrants | 162,500 | 216,667 | ||||||
Outstanding share options | 14,945,849 | 15,550,986 | ||||||
|
|
|
| |||||
Total | 106,708,747 | 107,368,051 | ||||||
|
|
|
| |||||
Unaudited Pro Forma Net Loss Per Share
The unaudited pro forma basic and diluted net loss per share attributable to ordinary shareholders for the nine months ended September 30, 2018 has been prepared to give effect to adjustments arising upon the completion of a qualified IPO. The unaudited pro forma net loss attributable to ordinary shareholders used in the calculation of unaudited pro forma basic and diluted net loss per share attributable to ordinary shareholders does not include the effects of preferred share dividends because the calculation gives effect to the automatic conversion of all preferred shares and convertible debt outstanding as of September 30, 2018, respectively, into ordinary shares as if the proposed IPO had occurred on the later of January 1, 2018, or the issuance date of the preferred shares.
The unaudited pro forma basic and diluted weighted-average ordinary shares outstanding used in the calculation of unaudited pro forma basic and diluted net loss per share attributable to ordinary shareholders for the nine months ended September 30, 2018 has been prepared to give effect, upon a qualified IPO, to the automatic conversion of all outstanding convertible preferred shares and convertible debt into ordinary shares as if the proposed IPO had occurred on the later of January 1, 2018, or the issuance date of the preferred shares. Pro forma basic and diluted net loss per share attributable to ordinary shareholders was calculated as follows:
| In thousands, except share and per share data | NINE MONTHS ENDED | |||
Numerator: | ||||
Net loss attributable to ordinary shareholders—basic and diluted | $ | (70,123 | ) | |
Add: Interest on convertible notes | 12,347 | |||
Add: Loss on change in fair value of derivative liability | 1,670 | |||
|
| |||
Pro forma net loss attributable to ordinary shareholders—basic and diluted | $ | (56,106 | ) | |
|
| |||
Denominator: | ||||
Weighted-average ordinary shares outstanding—basic and diluted | 68,474,614 | |||
Pro forma adjustment to reflect automatic conversion of convertible preferred shares to ordinary shares upon the completion of the proposed initial public offering | 91,600,398 | |||
Pro forma adjustment to reflect automatic conversion of convertible debt to ordinary shares upon the completion of the proposed initial public offering | 78,030,703 | |||
|
| |||
Pro forma weighted-average ordinary shares outstanding—basic and diluted | 238,105,715 | |||
|
| |||
Pro forma net loss per share attributable to ordinary shareholders—basic and diluted | $ | (0.24 | ) | |
|
| |||
14. Related Party
For the nine months ended September 30, 2017 and 2018, the Company paid $186,858 and $203,828, respectively, for consulting services provided by an entity affiliated with its interim Chief Financial Officer.
F-39
Table of Contents
Except as disclosed elsewhere in the notes to the accompanying condensed consolidated financial statements, there were no other material transactions with related parties.
15. Subsequent Events
The Company has completed an evaluation of all subsequent events through December 28, 2018 (and January 25, 2019 for the additional shareholder note borrowing), the date these financial statements were available to be issued. Except as disclosed in Notes 1, 8 and 16, the Company has concluded that no subsequent events have occurred that require disclosure.
In December 2018 and January 2019, the Company borrowed an additional $15.0 million from the Shareholder pursuant to the 2018 Shareholder Note.
16. Reverse Share Split
The Company’s board of directors and shareholders approved a three for one reverse share split of its issued and outstanding ordinary shares and share options and a proportional adjustment to the existing conversion ratios for the Company’s preferred shares through a consolidation of its share capitalization effective as of December 28, 2018. Accordingly, all share and per share amounts for all periods presented in the accompanying financial statements and notes thereto have been retroactively adjusted, where applicable, to reflect the reverse share split.
F-40
Table of Contents
6,200,000 American Depositary Shares
Representing 74,400,000 Ordinary Shares
Joint Book-Running Managers
Jefferies
Evercore ISI
BMO Capital Markets
Lead Manager
Nomura
Table of Contents
PART II
INFORMATION NOT REQUIRED IN PROSPECTUS
Item 6. Indemnification of Directors and Officers.
Every director and officer is indemnified and secured harmless out of the assets and funds of the Company against all actions, proceedings, costs, charges, expenses, losses, damages or liabilities incurred or sustained by such director or officer in or about the conduct of the Company’s affairs or in the execution of such director or officer’s duties, powers, authorities or discretions, including any costs, expenses, losses or liabilities incurred by such director or officer in defending (whether successfully or otherwise) any civil proceedings concerning the Company or its affairs in any court whether Cayman Islands or elsewhere.
Item 7. Recent Sales of Unregistered Securities.
Set forth below is information regarding ordinary shares, preferred shares, share options, and warrants to purchase shares issued by us within the past three years that were not registered under the Securities Act. Also included is the consideration received by us for such securities and information relating to the section of the Securities Act, or rule of the Securities and Exchange Commission, under which exemption from registration was claimed. All of the securities described below are deemed restricted securities for purposes of the Securities Act. All certificates representing the issued shares of share capital described in this Item 7 included appropriate legends setting forth that the securities have not been registered and the applicable restrictions on transfer.
Except as otherwise indicated herein or as the context otherwise requires, references below to “Stealth,” “the Company,” “we,” “us” and “our” refer to Stealth BioTherapeutics Corp and its consolidated subsidiaries, or any one or more of them as the context may require.
Since January 1, 2016, we have issued the following unregistered securities:
(a) Share option grants and option exercises
We granted options to purchase an aggregate of 8,764,139 ordinary shares, with exercise prices ranging from $1.14 to $2.22 per share, pursuant to our 2006 share incentive plan, as amended. We issued an aggregate of 16,139 ordinary shares upon the exercise of options for aggregate consideration of $10,476.
In October 2018, we reduced the exercise price per share of an aggregate of 385,833 options granted in June 2018 from $2.22 per share to $1.53 per share.
No underwriters were involved in the foregoing issuances of securities. The issuances of share options and the ordinary shares issued upon the exercise of the options described in this paragraph (a) of Item 7 were issued pursuant to written compensatory plans or arrangements with our employees, directors and consultants, in reliance on the exemption provided by Rule 701 promulgated under the Securities Act, or pursuant to Section 4(a)(2) under the Securities Act, relative to transactions by an issuer not involving any public offering, to the extent an exemption from such registration was required. All recipients either received adequate information about us or had access, through employment or other relationships, to such information.
(b) Convertible Promissory Note Issuances
Between February 2017 and January 2019, we issued convertible notes in an aggregate principal amount of $132.4 million. The notes are convertible into shares of our preferred shares or ordinary shares upon the occurrence of certain qualified financings.
No underwriters were involved in the issuance of these securities. The convertible securities described in this paragraph (b) of Item 7 were issued to investors in reliance upon the exemption from the registration requirements of the Securities Act provided under Regulation D promulgated under the Securities Act, or pursuant to Section 4(a)(2) under the Securities Act, relating to transactions by an issuer not involving any public offering. Each recipient of the security in the transaction described above represented that it was an accredited investor and was acquiring the security for its own account for investment purposes only and not with a view to the public resale or distribution thereof and that it could bear the risks of the investment and could hold the security for an indefinite period of time, and appropriate legends were affixed to the instrument representing the security issued in such transaction.
II-1
Table of Contents
(c) Warrant Issuances
In January 2017, we issued a warrant to purchase up to 231,989 ordinary shares to a consultant at an exercise price of $1.38 per share.
In June 2017, in connection with our entry into a loan agreement, we issued to a lender a warrant, which was amended and restated in June 2018. The warrant is exercisable for that number of our shares equal to the quotient determined by dividing (a) $500,000 plus an amount equal to 2.5% of any amount drawn under specified tranches of the loan agreement by (b) an exercise price equal to (i) $2.30769 in the event the shares issuable are Series A preferred shares or (ii) if the shares issuable are next round securities, the price per share of such next round securities. The warrant holder may elect whether to exercise the warrant for shares of Series A convertible preferred shares or next round securities.
No underwriters were involved in the issuance of these warrants. The issuance of the warrants described in this paragraph (c) of Item 7 were issued to investors in reliance upon the exemption from the registration requirements of the Securities Act provided under Regulation D promulgated under the Securities Act, or pursuant to Section 4(a)(2) under the Securities Act, relating to transactions by an issuer not involving any public offering. Each recipient of the security in the transaction described above represented that it was an accredited investor and was acquiring the security for its own account for investment purposes only and not with a view to the public resale or distribution thereof and that it could bear the risks of the investment and could hold the security for an indefinite period of time, and appropriate legends were affixed to the instrument representing the security issued in such transaction.
(d) Warrant Exercise
In December 2009, in connection with our preferred share financing, we issued a warrant to purchase an aggregate of 333,333 ordinary shares. In November 2016, the holder exercised this warrant, pursuant to which 333,333 ordinary shares were issued for an aggregate exercise price of $10,000.
No underwriters were involved in the foregoing issuance of securities. The issuance of the warrant described in this paragraph (d) of Item 7 was issued to an investor in reliance upon the exemption from the registration requirements of the Securities Act provided under Regulation D promulgated under the Securities Act, or pursuant to Section 4(a)(2) under the Securities Act, relating to transactions by an issuer not involving any public offering. The recipient of securities in the transaction described above represented that it was an accredited investor and was acquiring the securities for its own account for investment purposes only and not with a view to the public resale or distribution thereof and that it could bear the risks of the investment and could hold the securities for an indefinite period of time, and appropriate legends were affixed to the instrument representing such securities issued in such transaction.
Item 8. Exhibits and Financial Statement Schedules.
(a) Exhibits.
The exhibits to the registration statement are listed in the Exhibit Index attached hereto and incorporated by reference herein.
(b) Financial Statement Schedules.
No financial statement schedules are provided because the information called for is not required or is shown either in the financial statements or notes.
Item 9. Undertakings.
(a) The undersigned registrant hereby undertakes to provide to the underwriter, at the closing specified in the underwriting agreement, certificates in such denominations and registered in such names as required by the underwriter to permit prompt delivery to each purchaser.
(b) Insofar as indemnification for liabilities arising under the Securities Act may be permitted to directors, officers and controlling persons of the registrant pursuant to the foregoing provisions, or otherwise, the registrant has been advised that in the opinion of the Securities and Exchange Commission such indemnification is against public policy as expressed in the Securities Act and is, therefore, unenforceable. In the event that a claim for indemnification against such liabilities (other than the payment by the registrant of expenses incurred or paid by a director, officer, or controlling person of the registrant in the successful defense of any action, suit or proceeding) is asserted by such director, officer, or controlling person in connection with the securities being registered, the registrant will, unless in
II-2
Table of Contents
the opinion of its counsel the matter has been settled by controlling precedent, submit to a court of appropriate jurisdiction the question whether such indemnification by it is against public policy as expressed in the Securities Act and will be governed by the final adjudication of such issue.
(c) The undersigned hereby undertakes that:
(1) For purposes of determining any liability under the Securities Act of 1933, the information omitted from the form of prospectus filed as part of this registration statement in reliance upon Rule 430A and contained in a form of prospectus filed by the registrant pursuant to Rule 424(b)(1) or (4) or 497(h) under the Securities Act shall be deemed to be part of this registration statement as of the time it was declared effective.
(2) For the purpose of determining any liability under the Securities Act of 1933, each post-effective amendment that contains a form of prospectus shall be deemed to be a new registration statement relating to the securities offered therein, and the offering of such securities at that time shall be deemed to be the initialbona fide offering thereof.
II-3
Table of Contents
EXHIBIT INDEX
II-4
Table of Contents
EXHIBIT NUMBER | DESCRIPTION OF EXHIBIT | |
| 23.2 | Consent of Walkers (included in Exhibit 5.1) | |
| 23.3 | Consent of Wilmer Cutler Pickering Hale and Dorr LLP (included in Exhibit 8.1) | |
| 24.1** | ||
| ** | Previously filed. |
| † | Confidential treatment requested as to certain portions, which portions have been omitted and filed separately with the Securities and Exchange Commission. |
II-5
Table of Contents
Pursuant to the requirements of the Securities Act of 1933, the registrant certifies that it has reasonable grounds to believe that it meets all of the requirements for filing on FormF-1 and has duly caused this Amendment No. 2 to Registration Statement to be signed on its behalf by the undersigned, thereunto duly authorized, in the City of Newton, Massachusetts on this 6th day of February, 2019.
| STEALTH BIOTHERAPEUTICS CORP | ||
| By: | /s/ Irene P. McCarthy | |
| Irene P. McCarthy | ||
| Chief Executive Officer | ||
II-6
Table of Contents
Pursuant to the requirements of the Securities Act of 1933, this Amendment No. 2 to Registration Statement has been signed by the following persons in the capacities and on the dates indicated.
SIGNATURE | TITLE | DATE | ||
/s/ Irene P. McCarthy Irene P. McCarthy | Chief Executive Officer and Director (principal executive officer, principal financial officer and principal accounting officer) | February 6, 2019 | ||
* Francis W. Chen, Ph.D. | Director | February 6, 2019 | ||
* Gerald L. Chan, Sc.D. | Director | February 6, 2019 | ||
* Kevin F. McLaughlin | Director | February 6, 2019 | ||
* Vincent Sai Sing Cheung | Director | February 6, 2019 | ||
* Lu Huang | Director | February 6, 2019 | ||
* Cheuk Kin Stephen Law | Director | February 6, 2019 | ||
* Edward P. Owens | Director | February 6, 2019 | ||
Stealth BioTherapeutics, Inc. Authorized Representative in the United States | ||||
| * | By: | /s/ Irene P. McCarthy | ||
| Name: | Irene P. McCarthy | |||
| Title: | Chief Executive Officer | |||
II-7