UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
[Mark One]
x | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended October 31, 2012
OR
o | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15 (d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from to
Commission file number 0-15266
BIO-REFERENCE LABORATORIES, INC.
New Jersey | | 22-2405059 |
(State of incorporation) | | (I.R.S. Employer |
| | Identification No.) |
481 Edward H. Ross Drive, Elmwood Park, New Jersey 07407
(Address of principal executive offices)
Registrant’s telephone number 201-791-2600
Securities registered pursuant to Section 12(b) of the Act: None
Securities registered pursuant to Section 12(g) of the Act: | | Name of Exchange on Which Registered |
Common Stock, $.01 par value | | NASDAQ Global Market |
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes o No x.
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or 15(d) of the Act. Yes o No x.
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes x No o.
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§ 232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes x No o. [not required]
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of the registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or in any amendment to this Form 10-K. o
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of “large accelerated filer.” “accelerated filer,” and “smaller reporting company” in Rule 12b-2 of the Exchange Act. (Check one):
Large accelerated filer o | | Accelerated filer x |
| | |
Non-Accelerated filer o | | Smaller reporting company o |
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes o No x.
The aggregate market value of the voting stock of Bio-Reference Laboratories, Inc. (consisting of Common Stock, $.01 par value) held by non-affiliates of the registrant was approximately $619,778,775 based upon the last sale price for the Common Stock on April 30, 2012, the last trading date of the registrant’s most recently completed second quarter, as reported on the NASDAQ Global Market System.
On January 9, 2013, there were 27,709,382 shares of Common Stock issued and outstanding.
PART I
Forward Looking Statements
Statements included in this Annual Report on Form 10-K (Annual Report) that are not historical in nature, are intended to be, and are hereby identified as “forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995, many of which are beyond our ability to control or predict. Forward-looking statements may be identified by words such as “expects,” “anticipates,” “intends,” “plans,” “believes,” “seeks,” “estimates,” “will” or words of similar meaning and include, but are not limited to, statements about the expected future business and financial performance of Bio-Reference Laboratories, Inc. and its subsidiaries. Statements looking forward in time are included in this report pursuant to the “safe harbor” provisions of the Private Securities Litigation Reform Act of 1995. Such statements involve known and unknown risks and uncertainties that may cause the Company’s actual results in future periods to be materially different from any future performance suggested herein.
The preparation of financial statements in conformity with accounting principles generally accepted in the United States requires us to make estimates and assumptions that affect the reported amounts of revenues and expenses during the reporting period. While many aspects of our business are subject to complex federal, state and local regulations, the accounting for our business is generally straightforward. Our revenues are primarily comprised of a high volume of relatively low dollar transactions, and about 39% of all our costs consist of employee compensation and benefits. Revenues are recognized at the time the services are performed and are reported at the estimated net realizable amounts from patients, third-party payors and others for services rendered including prospectively determined adjustments under reimbursement agreements with third-party payors. These adjustments are accrued on an estimated basis in the period the services are rendered and adjusted in future periods as final settlements are determined. These estimates are reviewed and adjusted, if warranted, by senior management on a monthly basis. We believe that our estimates and assumptions are correct. Several factors could cause actual results to differ materially from those currently anticipated due to a number of factors in addition to those discussed under “Risk Factors” as well as elsewhere herein including:
Loss or suspension of a license or imposition of a fine or penalties under, or future changes in, the law or regulations of CLIA, or those of state laboratory licensing laws;
Failure to comply with HIPAA, which could negatively impact profitability and cash flows;
FDA regulation of Laboratory Developed Tests and clinical laboratories;
Failure to comply with federal and state anti-kickback laws;
Failure to maintain the security of patient-related information;
Failure to comply with the Federal Occupational Safety and Health Administration requirements and Needlestick Safety and Prevention Act;
Failure to comply with federal and state laws and regulations related to submission of claims for our services;
Changes in regulation and policies, including increasing downward pressure on health care reimbursement;
Efforts by third-party payors to reduce utilization and reimbursement for clinical testing services;
Failure to timely or accurately bill for our services;
Our failure to integrate newly acquired businesses and the costs related to such integration;
Increased competition, including price competition;
Our ability to attract and retain experienced and qualified personnel;
Our failure to obtain and retain new clients and business partners, or a reduction in tests ordered or specimens submitted by existing clients;
Adverse litigation results; and
Failure to establish, and perform to, appropriate quality standards to assure that the highest level of quality is observed in the performance of our testing services.
Item. 1. — Business
Overview
We are a clinical testing laboratory offering testing, information and related services to physician offices, clinics, hospitals, employers and governmental units. We believe that we are the fourth largest full-service laboratory in the United States and the largest independent regional laboratory in the Northeastern market. We offer a comprehensive list of laboratory testing services utilized by healthcare providers in the detection, diagnosis, evaluation, monitoring and treatment of diseases. We primarily focus on esoteric testing, molecular diagnostics, anatomical pathology, genetics, women’s health and correctional health care.
We currently process approximately 7.8 million laboratory test requisitions each year. A requisition form accompanies a patient specimen, indicating the tests to be performed and the party to be invoiced for the tests. We have a network of approximately 116 patient service centers located in the Northeast (primarily in New York metropolitan super-regional area) for collection of patient specimens. We currently conduct business in most New York State counties, as well as in most of New Jersey and Maryland as well as some parts of Pennsylvania, Delaware and Connecticut. We primarily offer laboratory services to physician offices in these areas with an infrastructure that includes a comprehensive logistical department, extensive phlebotomy services and phlebotomy draw stations scattered around our geographic area. In October 2012, we launched Laboratorio Buena Salud, the first national testing laboratory dedicated to serving Spanish-speaking populations in the United States. All business will be conducted in Spanish, including patient and physician interactions.
In addition to our clinical testing operations, we operate a clinical knowledge management service through our PSIMedica business unit. This system uses customer data from laboratory results, pharmaceutical data, claims data and other data sources to provide administrative and clinical decision support systems that enable our customers to provide quality and efficient healthcare to their populations.
We also operate a web-based connectivity portal solution for laboratories and physicians through our CareEvolve subsidiary. We use this portal ourselves to provide laboratory ordering and results as well as connectivity to our physician customers. We also market and license this connectivity solution to other laboratories throughout the country.
We are a New Jersey corporation. We are the successor to Med-Mobile, Inc., a New Jersey corporation that was organized in 1981. Our executive offices are located at 481 Edward H. Ross Drive, Elmwood Park, NJ 07407, and our telephone number is 201-791-2600. In this Form 10-K, we may at times refer to ourselves and our subsidiaries as “we,” “us” or “the Company.”
The Clinical Laboratory Testing Market in the United States
We believe that the U.S. market for clinical laboratory testing generated approximately $68 billion in annual revenue in 2012. Nearly all laboratory tests are performed by one of three types of laboratories: hospital laboratories, physician office laboratories or independent clinical laboratories. We believe approximately 60% of the clinical laboratory tests done in the United States are currently performed in a hospital laboratory, approximately 35% performed by an independent clinical laboratory and the balance in a physician office or other laboratory.
Commencing with the advent of managed care cost containment in the 1990s, the industry has been impacted by the rapid growth of managed care arrangements, increasingly stringent government regulation and escalating numbers of investigations into fraud and abuse. Among other things, these factors have led to revenue and profit declines for many smaller and mid-sized clinical laboratories, and industry consolidations. As a result, fewer but larger commercial clinical laboratories have emerged with greater economies of scale, more effective compliance with government billing regulations and other laws and a better approach to pricing their services. These changes have resulted in improved profitability for these larger commercial laboratories. In addition, new and emerging technologies continue to provide greater testing opportunities for clinical laboratories.
2
We believe that the clinical laboratory testing industry will continue to experience growth in testing volume due to the following factors:
the aging of the population of the United States;
patient awareness of the value of laboratory tests;
a decrease in the cost of tests;
the development of sophisticated and specialized tests for early detection of disease and disease management;
the diagnosis and monitoring of infectious diseases, such as AIDS and Hepatitis C;
increased recognition of early detection and prevention as a means of reducing healthcare costs;
the emergence of employer-sponsored wellness programs; and
additional research and development in genomics.
In addition, new and emerging technologies continue to provide greater testing opportunities for clinical laboratories. As the result of health insurance coverage to uninsured Americans under the Patient Protection and Affordable Care Act as amended by health Care and Education Reconciliation Act, each enacted in March 2010 (the “Health Care Reform Law”) the demand for our services may increase.
Business Strengths and Focus
We operate as a national oncology laboratory through our GenPath business unit. Our expertise in cancer pathology and diagnostics as well as molecular diagnostics has enabled GenPath to grow as a national provider.
Our innovative technology platform for sexually transmitted infections has enabled us to expand from a regional service offering to a national offering with specimens coming from throughout the contiguous 48 states in the area of Women’s Health, through our GenPath business unit.
GeneDx, our wholly owned subsidiary, is our genetics laboratory and is typically recognized as the leading national laboratory for testing of rare and ultra-rare genetic diseases.
We have one of the largest regional marketing staffs of any laboratory in the country, with approximately 265 managers and sales and service representatives working for us. We have groups dedicated to the Metropolitan regional market, the Oncology market, the Women’s Health market, the Genetic testing market and the Correctional Health market. We are currently building a new marketing group that will cross over into the genetics and Women’s Health groups to market to physicians who offer pre-natal testing.
We believe that our large marketing staff and strong infrastructure within our designated area can be leveraged to bring new technologies to physicians and healthcare providers. Over the past year, our volume of testing in the area of molecular diagnostics has increased by approximately 35%.
We believe that laboratory data has great value in managing the healthcare of a population, but can only be properly utilized when combined with medical claims and pharmacy data. Our medical information unit, PSIMedica, seeks to combine laboratory data with these other data elements in order to provide actionable analytics designed to help to improve the quality and efficiency of healthcare.
Strategy
We seek to continue our strong growth not only through our marketing organization, new technologies and superior service, but also by providing value-added analytics in conjunction with laboratory results. Our mission is to be recognized by our clients as the best provider of clinical laboratory testing, information and related services. The principal components of our strategy to achieve our mission are as follows:
capitalize on our position within the clinical market;
lead in providing medical information;
provide the highest quality service; and
pursue strategic growth opportunities, both through development of new testing services and through acquisitions.
Our Testing Services
Our laboratory testing business consists of routine testing and esoteric testing. Routine testing generates approximately 40% and esoteric testing generates approximately 60% of our net revenues.
Routine Testing
Routine tests measure various health parameters, such as the functions of the heart, kidney, liver, thyroid and other organs. Below is an abbreviated list of some commonly ordered routine tests:
Blood cell counts
Cholesterol levels
Pregnancy
Substance abuse
Urinalysis
We perform these tests at our main processing facility in Elmwood Park, New Jersey. We operate 24 hours a day, 365 days a year. We perform and report most routine tests within 24 hours. Tests results are delivered via driver or electronically.
Esoteric Tests
We also perform esoteric tests that require sophisticated equipment and materials, highly skilled personnel and professional attention. These tests are ordered less frequently than routine tests. They are also generally priced higher than routine tests. Esoteric tests are typically related to the following medical fields:
Endocrinology (the study of glands and their hormone secretions)
Genetics (the study of chromosomes, genes and their protein products)
Immunology (the study of the immune system)
Microbiology (the study of microscopic forms of life)
HIV-related tests
Molecular diagnostics (the study of genetic content for disease information)
Oncology (the study of abnormal cell growth)
Serology (the study of body fluids)
Toxicology (the study of chemicals and drugs and their effects on the body)
3
We perform cancer cytogenetic testing at our leased facilities in at our main processing facility in Elmwood Park, Smithtown, NY, Clarksburg, MD and Milford, MA and genetic testing at our GeneDx leased facility in Gaithersburg, MD, as well as at our Elmwood Park facility. We perform cytology testing in Frederick, MD, Milford, MA, Columbus, OH, Houston, TX and at our Elmwood Park facility.
PSIMedica—Medical Information
Our PSIMedica business unit is based on a clinical knowledge management, or CKM, system that uses data derived from various disparate sources to provide both administrative and clinical analysis of a population. The source data consists of enrollment (demographic) data, claims data, pharmacy data, laboratory data and any other data that may be available. The system uses sophisticated algorithms to cleanse and configure the data to facilitate comprehensive and meaningful analysis. The data is maintained on multiple levels enabling review of data from the global level to the granular transactional detail. The system includes a base set of queries that provide basic functionality and also provides on-line real-time ad hoc query capability enabling the user to customize analysis to the needs of the user’s organization. In addition to the basic queries provided by the system, PSIMedica Quality Indicators, or PQI, provide comprehensive, disease-state-oriented queries that disclose the quality and efficiency of the care and service. These indicators have been designed to provide the user with standards and outcome predictors on a medical standards basis. We are using PSIMedica to market value-added clinical laboratory services to bulk purchasers of clinical laboratory solutions, as well as marketing our PSIMedica programs to businesses such as health plans, integrated delivery networks, disease management companies, insurers, clinical trial companies and other healthcare providers that benefit from the ability of the system to combine both clinical and administrative analysis.
CareEvolve—Connectivity Solutions
Through our CareEvolve subsidiary, we offer a physician-based connectivity solution. This system provides a complex, sophisticated portal for ordering laboratory services and delivering laboratory results, along with ancillary connectivity services. The system is designed to be physician-centric and to provide a highly flexible, scalable, comprehensive desktop solution for physicians to manage their day-to-day practice needs, as well as to handle their clinical laboratory ordering and reporting. This product has been designed to work as a platform with plug and play capability that can easily be used by other laboratories that also need a web-based solution for their physician customers.
Payors and Clients
We provide laboratory services to a range of healthcare providers. A “payor” is the party who pays for the tests while the “client” is the party that refers the tests to us. An organization that has a contract with us, such as a clinic or governmental agency, may be both a payor and a client. Some states, such as New York and New Jersey, prohibit us from billing physician clients. During fiscal year 2012, no single client accounted for more than 10% of our net revenues.
The following table reflects our estimate of the breakdown of net revenue by type of payor for the fiscal years ended October 31, 2010, 2011, and 2012.
| | Fiscal Year Ended October 31, | |
| | 2012 | | 2011 | | 2010 | |
| | | | | | | |
Direct Patient Billing | | 2 | % | 2 | % | 3 | % |
Commercial Insurance | | 62 | % | 61 | % | 53 | % |
Professional Billing | | 17 | % | 17 | % | 20 | % |
Medicare | | 18 | % | 19 | % | 22 | % |
Medicaid | | 1 | % | 1 | % | 2 | % |
| | 100 | % | 100 | % | 100 | % |
Physicians who order clinical tests for their patients represent one of the primary sources of our testing volume. Fees invoiced to patients and third parties are based on our fee schedule, which may be subject to limitations imposed by third-party payors. Fees invoiced to federal health care programs such as Medicare and Medicaid, are based on fee schedules set by applicable governmental authorities, such as the Cents for Medicare and Medicaid Services (“CMS”).
We provide laboratory services to governmental agencies and large employer groups. We believe that we are the largest regional laboratory providing laboratory testing services to correctional facilities in the United States. All of these clients are charged on a contractual basis.
Billing
Billing for laboratory services is extremely complicated. We must bill various payors, such as patients, the Medicare program and state Medicaid programs, insurance companies and employer groups, all of which have different billing requirements. Compliance with applicable laws and regulations as well as internal compliance procedures adds complexity to this process.
Our bad debt expense is not the result of credit-related issues, as is the case in most industries. Our bad debt expense is due primarily to missing or incorrect demographic and billing information on our requisitions. We depend on the healthcare provider to supply us with this information. We perform the tests and report the test results as requested on the requisition regardless of whether the demographic and billing information is correct or even missing altogether. We then attempt to obtain missing and to correct incorrect information. This adds to the complexity, slows the invoicing process and generally increases the aging of our accounts receivable. When all issues are not resolved in a timely manner, the item is written-off to bad debt expense through the allowance for doubtful accounts. Other items such as pricing differences and payor disputes also complicate billing. Adjustments to receivables as a result of these types of matters are accounted for as revenue adjustments and are not written-off to bad debt expense.
Sales and Marketing
We employ full and part-time sales and marketing representatives. With approximately 265 managers and sales and service representatives working for us, we have groups dedicated to the New York metropolitan regional market, the oncology market, the women’s health market, the genetic testing market and the correctional health market. We are currently building a new marketing group that will cross over into the genetics and women’s health groups to market to physicians who offer pre-natal testing.
All of our sales and marketing personnel operate in a dual capacity, as both marketing and client support representatives. This ensures that all of our salespersons are intimately involved with the client. We believe that this is extremely helpful in client retention, since it provides a strong connection between our physician clients and us.
Client Service Coordinators
We utilize the services of full and part-time client service coordinators at our Elmwood Park, Clarksburg and Gaithersburg facilities, all of whom are trained in medical and laboratory terminology. This staff is used as an interface with physicians and nurses and supplements the client support provided by our sales force. They also report highly abnormal and life threatening results to the ordering physician via telephone in order to assist speedy medical resolution of patient problems.
4
Logistical Support
We employ full and part-time couriers. Our couriers pick up patient specimens from and deliver printed reports to physician offices, nursing homes, clinics and correctional facilities.
Acquisitions
On March 2, 2010, we acquired Lenetix Medical Screening Laboratory, Inc., a clinical testing laboratory located in Mineola, New York. The laboratory performs both clinical laboratory diagnostic testing and genetic testing.
On August 5, 2011, we acquired The Genetics Center, Inc., a New York corporation engaged in the clinical laboratory business with its principal place of business in Smithtown, New York.
We retained the staffs of these laboratories and continue to operate at the same locations.
On April 27, 2012, we entered into an agreement pursuant to which we purchased preferred shares of IncellDx, Inc. (“IncellDx”), a Delaware corporation. Information about IncellDx and the agreement may be found in our Current Report on Form 8-K, filed on May 1, 2012 and in note 18 to our consolidated financial statements.
On December 21, 2012, a date subsequent to our year end, we entered into an agreement pursuant to which we agreed to purchase all of the authorized, issued and outstanding shares of Meridian Clinical Laboratory, Corp. (“Meridian”), a Florida corporation. Information about Meridian and the agreement may be found in the Current Report on Form 8-K,we filed on December 27, 2012.
On December 31, 2012, a date subsequent to our year end, we entered into an agreement pursuant to which we agreed to purchase all of the authorized, issued and outstanding shares of Florida Clinical Laboratory, Inc. (“FCL”), a Florida corporation. Information about FCL and the agreement may be found in the Form 8-K we filed on January 4, 2013.
Competition
We compete with three types of providers in a highly fragmented and competitive industry: hospital laboratories, physician-office laboratories and other independent clinical laboratories. Our major competitors in the New York metropolitan area are two of the largest national laboratories, Quest Diagnostics (DGX) and Laboratory Corporation of America (LH). Although we are much smaller than these national laboratories, we believe that we compete successfully with them in our region due to our innovative testing services and our level of service. We believe our responses to medical consultation are faster and more personalized than those of the national laboratories. Our client service staff deals only with basic technical questions and those that have medical or scientific significance are referred directly to our senior scientists and medical staff.
Quality Assurance
In order to provide accurate and precise clinical information to the physician, it is essential that we maintain a well structured and vigorous quality assurance program. We hold the required Federal and state licenses necessary for the operation of a clinical laboratory at our facilities in New Jersey, New York, Maryland, Massachusetts, Texas and Ohio. We submit to vigorous proficiency tests (or surveys) for all tests that we perform. We are also subject to unannounced inspections from the various state and federal licensing agencies.
Our laboratories are accredited by the College of American Pathologists, or CAP. This accreditation includes on-site inspections and participation in the CAP (or equivalent) proficiency testing program. CAP is an independent organization of board certified pathologists approved by the Center for Medicare and Medicaid Services (CMS), to inspect clinical laboratories in order to determine compliance with the standards required by the Clinical Laboratory Improvement Amendments of 1988, or CLIA.
We have a Quality Assurance Committee, headed by a Quality Assurance Coordinator and composed of supervisors from all of our departments. The Committee meets each day to assess and evaluate our laboratory quality. Based on the information received from the Committee, recommendations are made to correct conditions that have led to errors. Management, department supervisors and members of the Committee continually monitor laboratory quality. Depending on the test, two or three levels of quality control materials are run in each analytical assay to enhance precision and accuracy. Patient population statistics are evaluated each day. Testing of highly abnormal samples is repeated to maximize accuracy.
We believe that all of these procedures are necessary, not only in maintaining Federal and state licensing, but also in assuring a quality product. We believe that our high standards of quality are an important factor in client retention.
Regulation of Our Clinical Laboratory Operations
The clinical laboratory industry is highly regulated and subjected to significant and changing Federal and state laws and regulations. These laws and regulations affect key aspects of our business, including licensure and operations, billing and payment for laboratory services, sales and marketing interactions with ordering physicians, security and confidentiality of health information, and environmental and occupational safety. Oversight by government officials includes regular inspections and audits. Failure to comply with applicable requirements, which are sometimes vague or indefinite, may result in substantial fines, criminal penalties, or other enforcement actions, such as suspension or revocation of a clinical laboratory’s license. Changes in regulations often increase the cost of testing or processing claims. Also, these laws may be interpreted or applied by a prosecutorial, regulatory or judicial authority in a manner that could require us to make changes in our operations, including in our pricing, billing and/or marketing practices in a manner that could adversely affect operations. We seek to and believe that we do conduct our business in compliance with all applicable laws and regulations. Set forth below are highlights of the key regulatory areas applicable to our business.
Reimbursement for Laboratory Services
We typically bill third party payors such as Medicare, Medicaid, Governmental programs and private insurers for our services. Billing for clinical testing services is very complicated, and our payors often have different coverage, billing and reimbursement requirements, and change those requirements on an ongoing basis. Also, submissions of our claims are particularly complex because we provide both anatomic pathology services and clinical laboratory tests, which generally are paid using different reimbursement principals. The clinical laboratory tests are often paid under a clinical laboratory fee schedule, and the anatomic pathology services are often paid under a physician fee schedule. If ordering physician requisitions contain incorrect or incomplete information, we may also be unable to collect reimbursement from payors. The increased use of electronic ordering reduces, but does not eliminate, the incidence of missing or incorrect information.
In addition, both government and private sector payors have engaged in ongoing efforts in recent years to contain or reduce health care costs, including reimbursement for clinical laboratory services. The combination of complex billing requirements and ongoing pressure with respect to reimbursement levels, presents substantial challenges to the clinical laboratory business. Through the Health Care Reform Law substantial changes are being made to the current system for paying for healthcare in the United States, including programs to extend medical benefits to millions of individuals who currently lack insurance coverage, coupled with measures to cut Medicare spending for most health care services, including clinical laboratories. The changes contemplated by the Health Care Reform Law are subject to rule-making and implementation timelines that extend for several years, and this uncertainty limits our ability to forecast changes that may occur in the future.
5
The U.S. Congress has considered, at least yearly in conjunction with budgetary legislation, changes to one or both of the Medicare fee schedules under which we receive reimbursement, which include the physician fee schedule for anatomical pathology services, and the clinical laboratory fee schedule for our clinical laboratory services. For example, currently there is no copayment or coinsurance required for clinical laboratory services, although there is for our physician services. However, Congress has periodically considered imposing a 20 percent coinsurance on laboratory services. If enacted, this would require us to attempt to collect this amount from patients, although in many cases the costs of collection would exceed the amount actually received.
For most of the tests performed for Medicare or Medicaid beneficiaries, laboratories are required to bill Medicare or Medicaid directly, and to accept Medicare or Medicaid reimbursement as payment in full. Part B of the Medicare program contains fee schedule payment methodologies for clinical laboratory services, and the Medicare approach and reimbursement levels often serve as a benchmark for commercial payors. Payment under Medicare is generally the lesser of billed charges, the local fee for a geographic area, and a national limitation amount that is set at a percent of the median of all local fee schedule amounts for each laboratory test code. Each year, subject to federal legislation, fees may be updated for inflation based on the percentage change in the Consumer Price Index, or CPI. From 2004 through 2008 the clinical laboratory fee schedule remained frozen, with no CPI increases. Then, for the first time in five years, as of January 1, 2009 laboratories received a 4.5% across the board increase in reimbursements. For 2010, the clinical laboratory fee schedule was decreased by 1.9 percent. For 2011, under the Health Care Reform Law, it was decreased by 1.75 percent, the first of a series of such annual reductions effective from 2011 to 2015, and in 2011, certain “productivity adjustments were instituted that have functioned to decrease rate increases under the CPI update. For 2012, the clinical laboratory fee schedule was increased by .65%, and in February 2012, Congress passed legislation that reduced payment rates under the clinical laboratory fee schedule by 2%, effective January 1, 2013 and an additional 2% reduction in Medicare rates is scheduled to take effect on March 1, 2013 under a “sequestration” mandate, unless Congress acts to prevent this reduction.
Under the CMS framework, the national limitation amount for clinical laboratory services had been reduced in a number of instances over the past several years to a present level equal to 74% of the national median of laboratory charges, and a number of proposals for legislation or regulation are under discussion which could have the effect of substantially reducing reimbursements to clinical laboratories through reduction of the present allowable percentage or through other means. We are unable to predict the outcome of these discussions. Depending upon the nature of congressional and/or regulatory action, if any, which is taken and the content of legislation, if any, which is adopted, we could experience a significant decrease in revenues from CMS, which could have a material adverse effect on us.
Also, CMS and other payors have expressed some concern regarding “billed charges” reporting by large clinical laboratories, in light of the common practice, among major clinical laboratories, of providing discounted pricing to certain clients that order testing services on a “bulk” basis, such as certain physicians, hospitals, and other institutions, resulting in economies of scale and relatively low administrative costs, as compared with the higher fees charged to individual patients and third party payors, including Medicare, who generally require separate bills or claims for each patient encounter and which involve relatively high administrative costs). If this issue were decided in a manner that required the downward adjustment of billed charges reporting, it could adversely affect the Company.
Clinical Laboratory Improvement Amendments of 1988 (“CLIA”)
CLIA extends Federal licensing requirements to all clinical laboratories (regardless of the location, size or type of laboratory), including those operated by physicians in their offices, based on the complexity of the tests they perform. CLIA also establishes a stringent proficiency testing program for laboratories and includes substantial sanctions, such as suspension, revocation or limitation of a laboratory’s CLIA certificate (which is necessary to conduct business), cancellation or suspension of the laboratory’s approval to receive Medicare and Medicaid reimbursement, and significant fines and/or criminal penalties.
CLIA, and its implementing regulations, includes quality standards (establishing Federal quality standards for all clinical laboratories); application and user fee requirements; and enforcement procedures. The quality standard regulations establish varying levels of regulatory scrutiny depending upon the complexity of testing performed. Under these regulations, a laboratory that performs only one or more of routine “waived” tests may apply for a waiver from most requirements of CLIA. We believe that most tests performed by physician office laboratories will fall into either the “waived” or the “moderately complex” category. The latter category applies to simple or automated tests and generally permits existing personnel in physicians’ offices to continue to perform testing under the implementation of systems that insure the integrity and accurate reporting of results, establishment of quality control systems, proficiency testing by approved agencies, and biannual inspection.
Under CLIA, the company remains subject to state and local laboratory regulations. CLIA provides that a state may adopt laboratory regulations that are more stringent than those under federal law, and some states require additional personnel qualifications, quality control, record maintenance and other requirements.
Our laboratory completed its first CLIA inspection under CLIA guidelines and received its certificate of compliance effective February 7, 1996. It has been reinspected since on a bi-annual basis and found to be in compliance. We believe the Company is in compliance with all applicable federal and state laboratory requirements.
Compliance Program
The Office of Inspector General has published a Model Compliance Program for the clinical laboratory industry. This is a voluntary program for laboratories to demonstrate to the Federal government that they are responsible providers. In addition, certain states, such as New York, require that health care providers, such as clinical laboratories, that engage in substantial business under the state Medicaid program have a compliance program that general adheres to the standards set forth in the Model Compliance Program. Also, under the Health Care Reform Law, the U.S. Department of Health and Human Services, or HHS, will require suppliers, such as the Company, to adopt, as a condition of Medicare participation, compliance programs that meet a core set of requirements. This mandate has not yet been implemented with respect to clinical laboratories, and HHS has not yet provided a time frame for implementation. We have implemented a comprehensive voluntary compliance program adhering to the standards set forth in the Model Compliance Program.
Health Insurance Portability and Accountability Act of 1996, as amended (“HIPAA”)
Both as a health care provider of clinical laboratory services, and in connection with the services we furnish to health plans and others as a business associate though medical information services, we are required to comply with federal and state laws that protect the privacy and security of certain healthcare and personal information. These include HIPAA, which establishes comprehensive standards with respect to the privacy and security of medical information, including requirements for safeguarding electronic protected health information, and comprehensive standards regarding uses and disclosures of protected health information. The HIPAA standards create a complex regulatory framework, including penalties for non-compliance, requirements to respond to patient requests to review and amend their medical records, certain limitations regarding the use of patient information, and notification obligations in the event of certain breaches of patient information. In addition to HIPAA, we are required to abide by various state laws protecting healthcare information, that impose standards that are stricter than those of HIPAA, such as state laws governing sensitive health information regarding HIV status and genetic testing.
HIPAA provides for significant fines as well as substantial criminal penalties for violations of the Act. The federal Health Information Technology for Economic and Clinical Health, or HITCH, Act, strengthened and expanded HIPAA, including to require certain breach notification
6
obligations, to extend a number of HIPAA requirements directly to business associates, to heighten penalties and enforcement provisions (including requiring HHS to conduct periodic audits to confirm compliance), and to extend enforcement authority over HIPAA to state attorney generals.
In addition, the HITECH Act established a program of Medicare and Medicaid incentive payments available to certain health care providers including, among others, physicians and dentists, if they meaningfully use certified electronic health record technology (“EHR”). Also, eligible providers that fail to adopt certified EHR systems may be subject to Medicare reimbursement reductions beginning in 2015. Qualification for the incentive payments requires the use of EHRs that are certified as having certain capabilities for meaningful use pursuant to standards adopted by the Department of Health and Human Services. Initial (“stage one”) standards addressed criteria for periods beginning in 2011. CMS has also issued a final rule with “stage two” criteria, for periods beginning in 2014, which are more demanding, and new, incrementally more rigorous criteria are expected to be issued for stage three compliance, however final standards have not yet been issued and so these criteria are not yet certain. Certain of our businesses involve the marketing and distribution of certified EHR products, and these products must maintain compliance with these evolving governmental criteria.
In addition, HIPAA requires health care providers, such as clinical laboratories, and other covered entities, to use certain transaction and code set rules for specified electronic transactions, such as transactions involving claims submissions. The Company believes it is in compliance in all material respects with the current rules. With respect to these rules, commencing July 1, 2012, CMS required that all HIPAA-covered entities, such as the Company, conduct electronic claim submissions and related electronic transactions under a new HIPAA transaction standard, called Version 5010. CMS is required this upgrade in connection with another new requirement applicable to the industry, the implementation of new diagnostic code sets to be used in claims submission. The new diagnostic code sets are called the ICD-10-CM, and are to be implemented on October 1, 2014. The Company has been aware of these changes for some time, and believes it is prepared to timely adopt the new standards. However, it is expected that these changes, in particular the adoption of new diagnostic codes — which must be provided to us accurately by referring physicians in order for us to receive payment from payors, such as Medicare — will result in a degree of disruption and confusion, which may adversely affect Company operations, including reimbursement rates.
Laboratory Developed Tests (LDTs)
The federal Food and Drug Administration, or FDA, has regulatory responsibility over, among other areas, instruments, test kits reagents and other medical devices used by clinical laboratories to perform diagnostic testing. High complexity and CLIA-certified laboratories, such as ours, frequently develop internal testing procedures to provide diagnostic results to customers. These tests are referred to as laboratory developed tests, or LDTs. LTD’s are subject to CMS oversight through its enforcement of CLIA. The FDA has also claimed regulatory authority over all LDTs, but has exercised enforcement discretion with regard to most LDTs offered by high complexity CLIA-certified laboratories, and has not subjected these tests to the panoply of FDA rules and regulations governing medical devices. However, the FDA has been considering changes in the way laboratories are allowed to offer these LDTs, and during 2010 publicly announced that it will be exercising regulatory authority over LDTS, using a risk-based approach that will direct more resources to tests with the highest risk of injury. The FDA has not announced a framework or timetable for implementing its announced approach and in its 2013 Work Plan, the U.S. Department of Health & Human Services Office of Inspector General announced that it would examine the oversight of the clinical effectiveness of LDTs given the current approaches by CMS and FDA with respect to LDTs. Depending upon the manner in which the FDA’s new regulatory framework is implemented, there may be an adverse affect on Company operations.
Fraud and Abuse Regulations
Since we supply services that are reimbursed by federal health care programs such as Medicare and Medicaid, our activities are also subject to regulation by CMS and enforcement by the Office of Inspector General, or OIG, within the HHS. A provision of the U.S. Social Security Act known as the “Anti-Kickback Law” prohibits providers and others from directly or indirectly soliciting, receiving, offering or paying any remuneration with the intent of generating referrals or orders for services or items covered by a federal health care program. Many states have similar laws. Courts have interpreted this law very broadly, including holding that a violation has occurred if even one purpose of the remuneration is to generate referrals, even if there are other lawful purposes. There are statutory and regulatory exceptions (known as safe harbors) that outline arrangements that are deemed lawful. However, the fact that an arrangement does not fall within a safe harbor does not necessarily render the conduct illegal under the Anti-Kickback Law. In sum, even legitimate business arrangements between the Company and referral sources, such as physicians, could lead to scrutiny by government enforcement agencies, and require extensive company resources to respond to government investigations. Violations of the Anti-Kickback Law may be punished by civil and criminal penalties and/or exclusion from participation in federal health care programs, including Medicare and Medicaid. The Health Care Reform Law strengthened provisions of the Anti-Kickback Law.
The federal “Stark Law” or “self-referral” prohibition, subject to certain exceptions, prohibits payment under Medicare or Medicaid for certain designated health services, including, among others, clinical laboratory services, where the referring physician has a financial relationships with the entity that furnishes the clinical laboratory service. The applicable exceptions permitting federal reimbursement generally require written agreements and fair market value payments that do not vary based upon the volume or value of referrals. Many states have similar self-referral laws that regulate the financial relationships between referring physicians and clinical laboratories, which extend to all referrals, not only referrals for services reimbursed by Medicare or Medicaid. Another federal law, known as the “Anti-Markup Rule,” and similar state laws, address the practice of an independent clinical laboratory performing and then billing to the ordering physician a component of a diagnostic test, such as diagnostic pathology services, where the ordering physician bills the test to Medicare. In this circumstance, penalties may apply to the physician if Medicare or other payor is billed at a rate that exceeds the laboratory’s charges to the physician, and the laboratory could be at risk under false claims laws, described below, for causing the submission of a false claim, if it advised the physician to submit claims to payors in violation of these provisions.
The federal False Claims Act, or FCA, is violated by any entity that “presents or causes to be presented” knowingly false claims for payment to the federal government and many states have similar laws that apply to governmental and private payors. In addition, the Health Care Reform Law amended the FCA to create a cause of action against any person who knowingly makes a false statement material to an obligation to pay money to the government, or knowingly conceals or improperly decreases an obligation to pay or transmit money or property to the government. For the purposes of these recent amendments, an “obligation” includes an overpayment, which is defined broadly to include “any funds that a person receives or retains under Medicare and Medicaid to which the person, after applicable reconciliation, is not entitled . . . .”
The FCA is commonly used to sue those who submit allegedly false Medicare or Medicaid claims, as well as those who induce or assist others to submit a false claim. Courts and government officials have found that “false claims” can result not only from noncompliance with the express requirements of applicable governmental reimbursement programs, such as Medicare and Medicaid, but also from noncompliance with other laws, such as provisions of the Food, Drug and Cosmetic Act, or laws that require quality care in service delivery. In addition, the Health Care Reform Law amended the FCA to specify that a claim to federal health care programs that includes items or services resulting from a violation of the Anti-Kickback Law constitutes a false claim under the FCA. The qui tam or whistleblower provisions of the FCA allow private individuals to bring actions on behalf of the government alleging that the government was defrauded, with tremendous potential financial gain to private citizens in the event they prevail. When a private party brings a whistleblower action under the FCA, the defendant is not made aware of the lawsuit until the government starts its own investigation or makes a decision on whether it will intervene. Many states have enacted similar laws that also apply to claims submitted to commercial insurance companies. The bringing of any FCA action could require us to devote resources to investigate and defend the action. Violations of the FCA could result in enormous economic liability. The law provides that all damages are trebled, and each false claim submitted is subject to a penalty of up to $11,000.
Historically, the clinical laboratory industry has been the focus of major governmental enforcement initiatives, and within the past few years federal and state governments continue to strengthen their enforcement efforts, such as through new laws that increase funding, powers and remedies to pursue suspected cases of fraud and abuse. We believe we operate lawfully within these statutes; however, we cannot predict if some of our practices may be interpreted as violating these statutes and regulations.
7
Waste Management, Health and Safety
We are subject to federal and state laws and regulations regarding the protection of the environment, the health and safety of employees, and the handling, transportation and disposal of medical specimens, and infectious and hazardous wastes. For example, federal regulations require licensure of interstate transporters of medical waste. In New Jersey, we are subject to the Comprehensive Medical Waste Management Act, or CMWMA, which requires us to register as a generator of special medical waste. All of our medical waste is disposed of by a licensed interstate hauler. The hauler provides a manifest of the disposition of the waste products as well as a certificate of incineration which is retained by us. These records are audited by the State of New Jersey on a yearly basis. We are also subject to the Federal Hazardous Materials Transportation Law, 49 U.S.C. 5101 et seq., and the Hazardous Materials Regulations, or HMR, 49 CFR parts 171-180. In addition, the federal Occupational Safety and Health Administration, or OSHA, has established extensive requirements relating specifically to workplace programs to protect workers from exposure to blood-borne pathogens, such as HIV and the hepatitis B virus, including work practice controls, protective clothing and equipment, training, vaccinations and other measures designed to minimize hazardous exposures.
Intellectual Property Rights
The Company relies on a combination of patents, trademarks, copyrights, trade secrets and nondisclosure and non-competition agreements to establish and protect its proprietary technology. The Company believes, however, that no single patent, technology, trademark, intellectual property asset or license is material to its business as a whole.
Insurance
We maintain professional liability insurance. We believe that our present insurance coverage is sufficient to cover currently estimated exposures, but we cannot assure that we will not incur liabilities in excess of the policy limits. In addition, although we believe that we will be able to continue to obtain adequate insurance coverage, we cannot assure that we will be able to do so at acceptable cost.
Employees
At October 31, 2012, we had 2,726 full-time and 838 part-time employees serving in executive positions, as technicians and technologists (including physicians, pathologists and PhDs), in marketing, in logistics and in bookkeeping, clerical and administrative positions. None of our employees are represented by a labor union. We regard relations with our employees as satisfactory.
Available Information
Our Internet website address is www.bioreference.com. Our Annual Reports on Form 10-K, Quarterly Reports on Form 10-Q, Current Reports on Form 8-K, and amendments to those reports filed or furnished pursuant to section 13(a) or 15(d) of the Exchange Act are available free of charge through our website as soon as reasonably practicable after we electronically file with or furnish them to the Securities and Exchange Commission, or SEC, and are available in print to any stockholder who requests a copy. Additionally, the charters of the standing committees of our board of directors are available on our website under “Board Committee Charters”. Information on our website shall not be deemed incorporated into, or to be a part of, this Annual Report on Form 10-K.
The public may also read and copy any materials that we file with the SEC at the SEC’s Public Reference Room at 100 F Street, NE, Washington, DC 20549. You may obtain information on the operation of the Public Reference Room by calling the SEC at 1-800-SEC-0330. Additionally, the SEC maintains a website that contains reports, proxy statements, information statements and other information regarding issuers, including us, that file electronically with the SEC at www.sec.gov.
Item 1A. Risk Factors
You should carefully consider each of the following risk factors and all other information set forth in this report. Any of the following risks could materially and adversely affect our business, financial condition or results of operations. They are not, however, the only risks we face. Additional risks and uncertainties not presently known to us or that we currently believe not to be material may also adversely affect our business, financial condition or results of operations. This report also includes forward-looking statements that involve risks or uncertainties. Our results could differ materially from those anticipated in these forward-looking statements as a result of certain factors, including the risks we face described below and elsewhere. See “Special Note Regarding Forward Looking Statements”.
Our business could be harmed from the loss or suspension of a license or imposition of a fine or penalties under, or future changes in, or interpretations of CLIA or state laboratory licensing laws to which we are subject.
The clinical laboratory testing industry is subject to extensive federal and state regulation, and many of these statutes and regulations have not been interpreted by the courts. CLIA extends federal licensing requirements to virtually all clinical laboratories (regardless of the location, size or type of laboratory), including those operated by physicians in their offices, by requiring that they be certified by the federal government or by a federally approved accreditation agency. The sanction for failure to comply with CLIA requirements may be suspension, revocation or limitation of a laboratory’s CLIA certificate, which is necessary to conduct business, as well as significant fines and/or criminal penalties. In addition, we are subject to regulation under state law. State laws may require that laboratories and/or laboratory personnel meet certain qualifications, specify certain quality controls or require maintenance of certain records.
We cannot assure you that applicable statutes and regulations will not be interpreted or applied by a prosecutorial, regulatory or judicial authority in a manner that would adversely affect our business. Potential sanctions for violation of these statutes and regulations include significant fines and the suspension or loss of various licenses, certificates and authorizations, which could have a material adverse effect on our business. In addition, compliance with future legislation could impose additional requirements on us, which may be costly.
Failure to comply with HIPAA, including regarding the use of new “standard transactions,” may negatively impact our profitability and cash flows.
Pursuant to HIPAA, we must comply with comprehensive privacy and security standards with respect to the use and disclosure of protected health information, as well as standards for electronic transactions, including specified transaction and code set rules. Under recent HITECH amendments to HIPAA, the law was expanded, including to require certain data breach notification, direct patient access to laboratory records, the extension of certain HIPAA privacy and security standards directly to business associates, and to heighten penalties for noncompliance, and enforcement efforts. While the Company maintains policies and procedures to comply with HIPAA, HHS has not yet issued final regulations to implement all HITECH requirements, and while the Company believes compliance will increase Company costs, it is difficult to predict precisely the costs involved.
8
In addition, the HIPAA transaction standards are complex, and subject to differences in interpretation by payors. For instance, some payors may interpret the standards to require us to provide certain types of information, including demographic information not usually provided to us by physicians. As a result of inconsistent application of transaction standards by payors or the our inability to obtain certain billing information not usually provided to us by physicians, we could face increased costs and complexity, a temporary disruption in receipts and ongoing reductions in reimbursements and net revenues. In addition, new requirements for additional standard transactions, such as claims attachments, Version 5010 of the HIPAA Transaction Standards and the ICD-10-CM Code Set, could prove technically difficult, time-consuming or expensive to implement. We are working closely with our payors to establish acceptable protocols for claim submission and with our trade association and an industry coalition to present issues and problems as they arise to the appropriate regulators and standards setting organizations.
FDA regulation of Laboratory Developed Tests (“LDTs”) and clinical laboratories may result in significant change, and our business could be adversely impacted if we fail to adapt.
High complexity, CLIA-certified laboratories, such as ours, frequently develop testing procedures to provide diagnostic results to customers. These tests have been traditionally offered by nearly all complex laboratories for the last few decades and LDTs are subject to CMS oversight through its enforcement of CLIA. The FDA, which regulates the development and use of medical devices, has claimed that it has regulatory authority over LDTs, but has not exercised enforcement with respect to most LDTs offered by high complexity laboratories, and not sought to require these laboratories to comply with FDA regulations regarding medical devices. During 2010, the FDA publicly announced that it has decided to exercise regulatory authority over these LDTs, and that it plans to issue guidance to the industry regarding its regulatory approach. At that time, the FDA indicated that it would use a risk-based approach to regulation and would direct more resources to tests with wider distribution and with the highest risk of injury, but that it will be sensitive to the need to not adversely impact patient care or innovation. To date, the FDA has not announced a framework or timetable for implementing a new regulatory approach, and in its 2013 Work Plan, the U.S. Department of Health & Human Services Office of Inspector General announced that it would examine the oversight of the clinical effectiveness of LDTs given the current approaches by CMS and FDA with respect to LDTs. If adopted, such a regulatory approach by the FDA may lead to an increased regulatory burden, including additional costs and delays in introducing new tests. While the ultimate impact of the FDA’s approach is unknown, it may be extensive and may result in significant change. Our failure to adapt to these changes could have a material adverse effect on our business.
Some of our activities may subject us to risks under federal and state laws prohibiting “kickbacks” and other laws designed to prohibit payments for referrals.
Federal and state anti-kickback and similar laws prohibit payment, or offers of payment, in exchange for referrals of products and services for which reimbursement may be made by Medicare or other federal and state healthcare programs. Some state laws contain similar prohibitions that apply without regard to the payor of reimbursement for the services. Under a federal statute, known as the “Stark Law” or “self-referral” prohibition, physicians, subject to certain exceptions, are prohibited from referring their Medicare or Medicaid program patients to clinical laboratories with which the physicians or their immediate family members have a financial relationship, and the laboratories are prohibited from billing for services rendered in violation of Stark Law referral prohibitions. Violations of the federal Anti-Kickback Law and Stark Law may be punished by civil and criminal penalties, and/or exclusion from participation in federal health care programs, including Medicare and Medicaid. States may impose similar penalties. The Health Care Reform Law significantly strengthened provisions of the Federal False Claims Act and Anti-Kickback Law provisions, and other health care fraud provisions, leading to the possibility of greatly increased qui tam suits by relators for perceived violations of these laws. There can be no assurance that our activities will not come under the scrutiny of regulators and other government authorities or that our practices will not be found to violate applicable laws, rules and regulations or prompt lawsuits by private citizen “relators” under federal or state false claims laws.
Federal officials responsible for administering and enforcing the healthcare laws and regulations have made a priority of eliminating healthcare fraud, and through a number of legislative measures, including the recent Health Care Reform Law, federal funding available for combating health care fraud and abuse has increased. While we seek to conduct our business in compliance with all applicable laws and regulations, many of the laws and regulations applicable to our business, particularly those relating to billing and reimbursement of tests and those relating to relationships with physicians, hospitals and patients, contain language that has not been interpreted by courts. We must rely on our interpretation of these laws and regulations based on the advice of our counsel and regulatory or law enforcement authorities may not agree with our interpretation of these laws and regulations and may seek to enforce legal remedies or penalties against us for violations. From time to time we may need to change our operations, particularly pricing or billing practices, in response to changing interpretations of these laws and regulations or regulatory or judicial determinations with respect to these laws and regulations. These occurrences, regardless of their outcome, could damage our reputation and harm important business relationships that we have with healthcare providers, payors and others. Furthermore, if a regulatory or judicial authority finds that we have not complied with applicable laws and regulations, we would be required to refund amounts that were billed and collected in violation of such laws and regulations. In addition, we may voluntarily refund amounts that were alleged to have been billed and collected in violation of applicable laws and regulations. In either case, we could suffer civil and criminal damages, fines and penalties, exclusion from participation in governmental healthcare programs and the loss of licenses, certificates and authorizations necessary to operate our business, as well as incur liabilities from third-party claims, all of which could harm our operating results and financial condition. Moreover, regardless of the outcome, if we or physicians or other third parties with whom we do business are investigated by a regulatory or law enforcement authority we could incur substantial costs, including legal fees, and our management may be required to divert a substantial amount of time to an investigation.
To enhance compliance with applicable health care laws, and mitigate potential liability in the event of noncompliance, regulatory authorities, such as the United States Health and Human Services Department Office of Inspector General (“OIG”), have recommended the adoption and implementation of a comprehensive health care compliance program that generally contains the elements of an effective compliance and ethics program described in Section 8B2.1 of the United States Sentencing Commission Guidelines Manual, and for many years the OIG has made available a model compliance program targeted to the clinical laboratory industry. In addition, certain states, such as New York, require that health care providers, such as clinical laboratories, that engage in substantial business under the state Medicaid program have a compliance program that general adheres to the standards set forth in the Model Compliance Program. Also, , under the Health Care Reform Law, the U.S. Department of Health and Human Services, or HHS, will require suppliers, such as the Company, to adopt, as a condition of Medicare participation, compliance programs that meet a core set of requirements. This mandate has not yet been implemented with respect to clinical laboratories, and HHS has not yet provided a time frame for implementation. While we have adopted U.S. healthcare compliance and ethics programs that generally incorporate the OIG’s recommendations, and train our applicable employees in such compliance, having such a program can be no assurance that we will avoid any compliance issues.
9
Failure to maintain the security of patient-related information or compliance with security requirements could damage our reputation with customers, cause it to incur substantial additional costs and become subject to litigation.
Pursuant to HIPAA, and certain similar state laws, we must comply with comprehensive privacy and security standards with respect to the use and disclosure of protected health information. Under recent HITECH amendments to HIPAA, HIPAA was expanded to require certain data breach notification, to extend certain HIPAA privacy and security standards directly to business associates, and to heighten penalties for noncompliance, and enhance enforcement efforts.
We receive certain personal and financial information about our clients and their patients. In addition, we depend upon the secure transmission of confidential information over public networks. A compromise in our security systems that results in client or patient personal information being obtained by unauthorized persons or our failure to comply with security requirements for financial transactions could adversely affect our reputation with our clients and others, as well as our results of operations, financial condition and liquidity. It could also result in litigation against us or the imposition of penalties.
Failure to comply with environmental, health and safety laws and regulations, including the federal Occupational Safety and Health Administration Act, the Needlestick Safety and Prevention Act and the Comprehensive Medical Waste Management Act, could result in fines and penalties and loss of licensure, and have a material adverse effect upon our business.
The clinical laboratory industry is highly regulated and subjected to significant federal and state regulation. This includes inspections and audits by governmental agencies. These agencies may impose fines, criminal penalties, or other enforcement actions to enforce laws and regulations. These penalties can include revocation of a clinical laboratory’s license. Changes in regulations may increase the cost of testing or processing claims.
We are subject to licensing and regulation under federal, state and local laws and regulations relating to the protection of the environment and human health and safety, including laws and regulations relating to the handling, transportation and disposal of medical specimens, infectious and hazardous waste and radioactive materials, as well as regulations relating to the safety and health of laboratory employees. The federal Occupational Safety and Health Administration has established extensive requirements relating to workplace safety for health care employers, including clinical laboratories, whose workers may be exposed to blood-borne pathogens such as HIV and the hepatitis B virus. These requirements, among other things, require work practice controls, protective clothing and equipment, training, medical follow-up, vaccinations and other measures designed to minimize exposure to, and transmission of, blood-borne pathogens. In addition, the Needlestick Safety and Prevention Act requires, among other things, that we include in our safety programs the evaluation and use of engineering controls such as safety needles if found to be effective at reducing the risk of needlestick injuries in the workplace.
Waste management is subject to federal and state regulations governing the transportation and disposal of medical waste including bodily fluids. Federal regulations require licensure of interstate transporters of medical waste. In New Jersey, we are subject to the Comprehensive Medical Waste Management Act (“CMWMA”), which requires us to register as a generator of special medical waste. All of our medical waste is disposed of by a licensed interstate hauler. The hauler provides a manifest of the disposition of the waste products as well as a certificate of incineration, which is retained by us. These records are audited by the State of New Jersey on a yearly basis. We are also subject to the Federal Hazardous materials transportation law, 49 U.S.C. 5101 et seq., and the Hazardous Materials Regulations (HMR), 49 CFR parts 171-180. The federal government has classified hazardous medical waste as hazardous materials for the purpose of regulation. These regulations preempt state regulation, which must be “substantively the same,” “the non-federal requirement must conform “in every significant respect to the federal requirement. Editorial and other similar de minimis changes are permitted,” 49 CFR 107.202(d).
Failure to comply with federal, state and local laws and regulations could subject us to denial of the right to conduct business, fines, criminal penalties and/or other enforcement actions, any of which would have a material adverse effect on our business. In addition, compliance with future legislation could impose additional requirements us, which may be costly.
We conduct our clinical laboratory testing business in a heavily regulated industry and changes in regulations or violations of regulations could, directly or indirectly, harm our operating results and financial condition.
The clinical laboratory testing industry is highly regulated and there can be no assurance that the regulatory environment in which we operate will not change significantly and adversely in the future. Areas of the regulatory environment that may affect our ability to conduct business include, without limitation:
federal and state laws applicable to billing and claims payment;
federal and state laboratory anti-mark-up laws;
federal and state anti-kickback laws;
federal and state false claims laws;
federal and state self-referral and financial inducement laws, including the federal physician anti-self-referral law, or the Stark Law;
coverage and reimbursement levels by Medicare and other governmental payors and private insurers;
federal and state laws governing laboratory licensing and testing, including CLIA;
federal and state laws governing the development, use and distribution of diagnostic medical tests known as laboratory developed tests or “LDTs”;
HIPAA, along with the revisions to HIPPA as a result of the HITECH Act, and analogous state laws;
federal, state and foreign regulation of privacy, security, electronic transactions and identity theft;
federal, state and local laws governing the handling, transportation and disposal of medical and hazardous waste;
Occupational Safety and Health Administration rules and regulations;
changes to laws, regulations and rules as a result of the Health Care Reform Law; and
changes to other federal, state and local laws, regulations and rules, including tax laws.
These laws and regulations are extremely complex and in many instances, there are no significant regulatory or judicial interpretations of these laws and regulations. Any determination that we have violated these laws or regulations, or the public announcement that we are being investigated for
10
possible violations of these laws or regulations, could harm our operating results and financial condition. In addition, a significant change in any of these laws or regulations may require us to change our business model in order to maintain compliance with these laws or regulations, which could harm our operating results and financial condition.
Failure to comply with complex federal and state laws and regulations related to submission of claims for clinical laboratory services could result in significant monetary damages and penalties and exclusion from the Medicare and Medicaid programs.
We are subject to extensive federal and state laws and regulations relating to the submission of claims for payment for clinical laboratory services, including those that relate to coverage of our services under Medicare, Medicaid and other governmental health care programs, the amounts that may be billed for our services and to whom claims for services may be submitted. These rules may also affect the Company in light of the practice management products that we market, to the extent that these products are considered to affect the manner in which our customers’ submit their own claims for services. Submission of our claims is particularly complex because we provide both anatomic pathology services and clinical laboratory tests, which generally are paid using different reimbursement principles. The clinical laboratory tests are often paid under a clinical laboratory fee schedule, and the anatomic pathology services are often paid under a physician fee schedule.
Our failure to comply with applicable laws and regulations could result in our inability to receive payment for our services or result in attempts by third-party payors, such as Medicare and Medicaid, to recover payments from us that have already been made. Submission of claims in violation of certain statutory or regulatory requirements can result in penalties, including substantial civil money penalties for each item or service billed to Medicare in violation of the legal requirement, and exclusion from participation in Medicare and Medicaid. Government authorities may also assert that violations of laws and regulations related to submission or causing the submission of claims violate the federal False Claims Act (“FCA”) or other laws related to fraud and abuse, including submission of claims for services that were not medically necessary. Violations of the FCA could result in enormous economic liability. The FCA provides that all damages are trebled, and each false claim submitted is subject to a penalty of up to $11,000. For example, we could be subject to FCA liability if it was determined that the services we provided were not medically necessary and not reimbursable, particularly if it were asserted that we contributed to the physician’s referrals of unnecessary services to us. It is also possible that the government could attempt to hold us liable under fraud and abuse laws for improper claims submitted by an entity for services that we performed if we were found to have knowingly participated in the arrangement that resulted in submission of the improper claims.
Changes in regulation and policies, including increasing downward pressure on health care reimbursement, may adversely affect reimbursement for diagnostic services and could have a material adverse impact on our business.
Reimbursement levels for health care services are subject to continuous and often unexpected changes in policies, and we face a variety of efforts by government payors to reduce utilization and reimbursement for diagnostic testing services. Changes in governmental reimbursement may result from statutory and regulatory changes, retroactive rate adjustments, administrative rulings, competitive bidding initiatives, and other policy changes.
The Health Care Reform Law includes two separate reductions in the reimbursement rates for our clinical laboratory services under the clinical laboratory fee schedule. First, it includes a “productivity adjustment” (which was 1.2 percent for 2012). Second, it includes an additional 1.75 percent reduction, the first of a series of such annual reductions effective from 2011 to 2015, which would reduce the annual Consumer Price Index-based update that would otherwise determine our reimbursement for clinical laboratory services. These reimbursement cuts could adversely affect our business.
The U.S. Congress has considered, at least yearly in conjunction with budgetary legislation, changes to one or both of the Medicare fee schedules under which we receive reimbursement, which include the physician fee schedule for anatomical pathology services, and the clinical laboratory fee schedule for our clinical laboratory services. For example, currently there is no copayment or coinsurance required for clinical laboratory services, although there is for our physician services. However, Congress has periodically considered imposing a 20 percent coinsurance on laboratory services. If enacted, this would require us to attempt to collect this amount from patients, although in many cases the costs of collection would exceed the amount actually received.
Our reimbursement for our pathology services is paid primarily under the physician fee schedule of Medicare and Medicaid and is therefore governed by a complex formula, referred to as the Sustainable Growth Rate, or SGR. As the use of this formula could result in a significant reduction in reimbursement for all physician services, Congress usually acts each year to prevent the full amount of such reductions from taking effect. In 2010, Congress acted to prevent reductions in reimbursement through December 31, 2011, and Congress acted again in 2011 to prevent significant reductions for 2012, and on January 1, 2013, Congress acted to prevent significant reductions for 2013. If Congress fails to take such action in the future, implementation of this formula could adversely affect our business.
The Center for Medicare and Medicaid Services (CMS) pays laboratories on the basis of a fee schedule that is reviewed and re-calculated on an annual basis. CMS may change the fee schedule upward or downward on billing codes that we submit for reimbursement on a regular basis; our revenue and business may be adversely affected if the reimbursement rates associated with such codes are reduced. Even when reimbursement rates are not reduced, policy changes add to our costs by increasing the complexity and volume of administrative requirements. Medicaid reimbursement, which varies by state, is also subject to administrative and billing requirements and budget pressures. Recently, state budget pressures have caused states to consider several policy changes that may impact our financial condition and results of operations, such as delaying payments, reducing reimbursement, restricting coverage eligibility and service coverage, and imposing taxes on our services.
Other legislative changes have been proposed since the passage of the Health Care Reform Law that could also affect reimbursement for our services. For example, the Budget Control Act of 2011 created a Joint Select Committee on Deficit Reduction, which was tasked with recommending proposals to reduce spending. Since that Joint Committee was unable to achieve a targeted deficit reduction of at least $1.2 trillion for the years 2013 through 2021, absent further Congressional action, an automatic reduction in federal spending, or “sequestration” is to be triggered, which, combined with the expiration of certain tax cuts on December 31, 2012, has typically been known as the Fiscal Cliff. While Congress did agree to a package of tax and federal spending proposals on January 1, 2013, these did not eliminate “sequestration” threat, but moved it back to March 1, 2013. These automatic cuts include Medicare, and, unless legislative action is taken, it will result in approximately 2% aggregate reductions to Medicare payments to providers starting on March 1, 2013.
Change in the Billing/Reimbursement procedures by the Federal government could affect our ability to be paid as we have in the past for services rendered.
CMS has changed or discussed making changes to certain types of reimbursement which could affect our rate of reimbursement. Certain cases
11
are comprised of both a technical component (TC) and a professional component (PC). In certain specified areas of testing, primarily in the area of anatomic pathology, CMS has determined that some providers have over-utilized these testing procedures and CMS has introduced changes in reimbursement policies to discourage over-utilization. While the Company does not currently over-utilize services for self-gain and does not perform any significant amounts revenue for the areas of testing currently being changed by CMS, we are always subject to review by CMS and cannot be certain that CMS won’t interpret our practices differently than we do. In addition, CMS may extend this logic and approach to other areas of testing that might affect work performed by us.
CMS has announced planned changes in the area of Molecular Diagnostics’ reimbursement, primarily designed to improve transparency in billing. Molecular Diagnostics is a rapidly changing and evolving area of clinical testing. Whereas other areas of clinical testing are well vetted and established with specific codes for reimbursement, Molecular Diagnostics has moved at a faster pace than CMS can proceed. Clinical laboratories accordingly use a process called cross-walking to get reimbursed by CMS. Cross-walking requires that the clinical laboratory identify the individual processes used to process the patient’s specimen and identify diagnostic results that are already reimbursed in established tests. CMS seeks to specifically identify the testing routine being done and reimburse providers universally for the test actually being performed. CMS has not established all of the molecular diagnostic tests that will be included in this revised schedule for reimbursement and it has not determined how much will be reimbursed to providers for these tests. We expect CMS to implement fair and reasonable reimbursement for such tests, but until such pricing decisions are disclosed we cannot be certain what CMS will finally implement.
Effective July 1, 2012, CMS eliminated an exemption that had been in place since 1999, which allowed commercial laboratories to bill for certain diagnostic tests performed on in-patient and certain outreach recipients by commercial laboratories. From 1999 through July 1, 2012, commercial laboratories were allowed to bill CMS for such tests despite the fact that the recipient was a hospital patient as long as the hospital had been submitting such tests for diagnosis to commercial laboratories prior to 1999. Upon termination of the exemption, we are required to find out from the hospital submitting the test whether the recipient’s bill for diagnostic testing will be reimbursed by the hospital or should be billed to CMS. We have systems in place to manage this change, but these systems are dependent upon our getting proper information from the hospital clients.
The Federal Government is faced with significant economic decisions in the coming years. Some solutions being offered in the government could substantially change the way laboratory testing is reimbursed by government entities. We cannot be certain what or how any such government changes may affect our business.”
Healthcare plans have taken steps to control the utilization and reimbursement of healthcare services, including clinical test services.
We also face efforts by non-governmental third-party payors, including healthcare plans, to reduce utilization and reimbursement for clinical testing services.
The healthcare industry has experienced a trend of consolidation among healthcare insurance plans, resulting in fewer but larger insurance plans with significant bargaining power to negotiate fee arrangements with healthcare providers, including clinical testing providers. These healthcare plans, and independent physician associations, may demand that clinical testing providers accept discounted fee structures or assume all or a portion of the financial risk associated with providing testing services to their members through capped payment arrangements. In addition, some healthcare plans have been willing to limit the PPO or POS laboratory network to only a single national laboratory to obtain improved fee-for-service pricing. There are also an increasing number of patients enrolling in consumer driven products and high deductible plans that involve greater patient cost-sharing.
The increased consolidation among healthcare plans also has increased the potential adverse impact of ceasing to be a contracted provider with any such insurer. The Health Care Reform Law includes provisions, including ones regarding the creation of healthcare exchanges, which may encourage healthcare insurance plans to increase exclusive contracting.
We expect continuing efforts to reduce reimbursements, to impose more stringent cost controls and to reduce utilization of clinical test services. These efforts, including future changes in third-party payor rules, practices and policies, or ceasing to be a contracted provider to a healthcare plan, may have a material adverse effect on our business.
Failure to timely or accurately bill for our services could have a material adverse effect on our business
Billing for clinical testing services is extremely complicated and is subject to extensive and non-uniform rules and administrative requirements. Depending on the billing arrangement and applicable law, we bill various payors, such as patients, insurance companies, Medicare, Medicaid, physicians, hospitals and employer groups. Changes in laws and regulations could increase the complexity and cost of our billing process. Additionally, auditing for compliance with applicable laws and regulations as well as internal compliance policies and procedures adds further cost and complexity to the billing process. Further, our billing systems require significant technology investment and, as a result of marketplace demands, we need to continually invest in our billing systems.
Missing or incorrect information on requisitions adds complexity to and slows the billing process, creates backlogs of unbilled requisitions, and generally increases the aging of accounts receivable and bad debt expense. We believe that much of our bad debt expense in recent years is attributable to the lack of, or inaccurate, billing information. Failure to timely or correctly bill may lead to our not being reimbursed for our services or an increase in the aging of our accounts receivable, which could adversely affect our results of operations and cash flows. Failure to comply with applicable laws relating to billing government healthcare programs could lead to various penalties, including: (1) exclusion from participation in CMS and other government programs; (2) asset forfeitures; (3) civil and criminal fines and penalties; and (4) the loss of various licenses, certificates and authorizations necessary to operate our business, any of which could have a material adverse effect on our results of operations or cash flows.
There have been times when our accounts receivable have increased at a greater rate than revenue growth and, therefore, have adversely affected our cash flows from operations. We have taken steps to implement systems and processing changes intended to improve billing procedures and related collection results. We believe that we have made progress by reorganizing our accounts receivable and billing functions and that our allowance for doubtful accounts is adequate. However, we cannot assure that our ongoing assessment of accounts receivable will not result in the need for additional provisions. Such additional provisions, if implemented, could have a material adverse effect on our operating results.
12
Failure of us, third-party payors or physicians to comply with Version 5010 Transactions and the ICD-10-CM Code Set, and our failure to comply with other emerging electronic transaction standards could adversely impact our business.
We are within the assessment and inventory phase to adopt Version 5010 Transactions and to adopt the ICD-10-CM Code Set issued by HHS on January 16, 2009. Compliance with Version 5010 was required by July 1, 2012; the compliance date for ICD-10-CM Code Set is currently October 1, 2014. The Company will continue its assessment of information systems, applications and processes for compliance with these requirements. Clinical laboratories are typically required to submit health care claims with diagnosis codes to third party payors. The diagnosis codes must be obtained from the ordering physician. The failure of us, third party payors or physicians to transition within the required timeframe could have an adverse impact on reimbursement, days sales outstanding and cash collections.
Also, the failure of our IT systems to keep pace with technological advances may significantly reduce our revenues or increase our expenses. Public and private initiatives to create healthcare information technology (“HCIT”) standards and to mandate standardized clinical coding systems for the electronic exchange of clinical information, including test orders and test results, could require costly modifications to our existing HCIT systems. While we do not expect HCIT standards to be adopted or implemented without adequate time to comply, if we fail to adopt or delay in implementing HCIT standards, we could lose customers and business opportunities.
We may be unable to obtain, maintain or enforce our intellectual property rights and may be subject to intellectual property litigation that could adversely impact our business
We may be unable to obtain or maintain adequate patent or other proprietary rights for our products and services or to successfully enforce our proprietary rights. In addition, we may be subject to intellectual property litigation and we may be found to infringe on the proprietary rights of others, which could force us to do one or more of the following:
cease developing, performing or selling products or services that incorporate the challenged intellectual property;
obtain and pay for licenses from the holder of the infringed intellectual property right;
redesign or reengineer our tests;
change our business processes; or
pay substantial damages, court costs and attorneys’ fees, including potentially increased damages for any infringement held to be willful.
The Company believes that no single patent, technology, trademark, intellectual property asset or license is material to its business as a whole.
Discontinuation or recalls of existing testing products; failure to develop, or acquire, licenses for new or improved testing technologies; or our clients using new technologies to perform their own tests could adversely affect our business.
From time to time, manufacturers discontinue or recall reagents, test kits or instruments used by us to perform laboratory testing. Such discontinuations or recalls could adversely affect our costs, testing volume and revenue.
The clinical laboratory industry is subject to changing technology and new product introductions. Our success in maintaining a leadership position in genomic and other advanced testing technologies will depend, in part, on its ability to develop, acquire or license new and improved technologies on favorable terms and to obtain appropriate coverage and reimbursement for these technologies. We may not be able to negotiate acceptable licensing arrangements and it cannot be certain that such arrangements will yield commercially successful diagnostic tests. If we are unable to license these testing methods at competitive rates, our research and development costs may increase as a result. In addition, if we are unable to license new or improved technologies to expand our esoteric testing operations, our testing methods may become outdated when compared with our competition and testing volume and revenue may be materially and adversely affected.
In addition, advances in technology may lead to the development of more cost-effective technologies such as point-of-care testing equipment that can be operated by physicians or other healthcare providers in their offices or by patients themselves without requiring the services of freestanding clinical laboratories. Development of such technology and its use by our clients could reduce the demand for its laboratory testing services and negatively impact its revenues.
Currently, most clinical laboratory testing is categorized as “high” or “moderate” complexity, and thereby is subject to extensive and costly regulation under CLIA. The cost of compliance with CLIA makes it impractical for most physicians to operate clinical laboratories in their offices, and other laws limit the ability of physicians to have ownership in a laboratory and to refer tests to such a laboratory. Manufacturers of laboratory equipment and test kits could seek to increase their sales by marketing point-of-care laboratory equipment to physicians and by selling test kits approved for home or physician office use to both physicians and patients. Diagnostic tests approved for home use are automatically deemed to be “waived” tests under CLIA and may be performed in physician office laboratories as well as by patients in their homes with minimal regulatory oversight. Other tests meeting certain FDA criteria also may be classified as “waived” for CLIA purposes. The FDA has regulatory responsibility over instruments, test kits, reagents and other devices used by clinical laboratories and has taken responsibility from the Centers for Disease Control for classifying the complexity of tests for CLIA purposes. Increased approval of “waived” test kits could lead to increased testing by physicians in their offices or by patients at home, which could affect our market for laboratory testing services and negatively impact our revenues.
Clinicians or patients using our services may sue us, and our insurance may not sufficiently cover all claims brought against us, which will increase our expenses.
The development, marketing, sale and performance of healthcare services expose us to the risk of litigation, including professional negligence. Damages assessed in connection with, and the costs of defending, any legal action could be substantial. We may be faced with litigation claims that exceed our insurance coverage or are not covered under any of our insurance policies. In addition, litigation could have a material adverse effect on our business if it impacts our existing and potential customer relationships, creates adverse public relations, diverts management resources from the operation of the business, or hampers our ability to otherwise conduct our business.
13
A failure to integrate newly acquired businesses and the costs related to such integration could have a material adverse impact on our net revenues and profitability.
The successful integration of any business that we may acquire entails numerous risks, including, among others:
issues related to revenue recognition and/or cash collections;
loss of key customers or employees;
difficulty in consolidating redundant facilities and infrastructure and in standardizing information and other systems;
failure to maintain quality of services that we and any such acquired companies have historically provided;
coordination of geographically separated facilities and workforces; and
diversion of management’s attention from our day-to-day business.
We cannot assure you that current or future acquisitions, if any, or any related integration efforts will be successful, or that our business will not be adversely affected by any future acquisitions. Even if we are able to successfully integrate the operations of companies or businesses that we may acquire in the future, we may not be able to realize the benefits that we expect to result from such integration, including projected cost savings.
Our operations may be adversely impacted by the effects of extreme weather conditions, natural disasters such as hurricanes and earthquakes, health pandemics, hostilities or acts of terrorism and other criminal activities.
Our operations were adversely impacted by the effects of Hurricane Sandy, and may continue to be adversely impacted by the after-effects of Hurricane Sandy, and by other extreme weather conditions, natural disasters, health pandemics, hostilities or acts of terrorism or other criminal activities. Such events may result in a temporary decline in the number of patients who seek clinical testing services or in our employees’ ability to perform their job duties. In addition, such events may temporarily interrupt our ability to transport specimens, to receive materials from our suppliers or otherwise to provide our services.
Increased competition, including price competition, could have a material adverse impact on our net revenues and profitability.
We operate in a business that is characterized by intense competition. Our major competitors in the New York metropolitan area, Quest Diagnostics and Laboratory Corporation of America, are large national laboratories that possess greater name recognition, larger customer bases, significantly greater financial resources and employ substantially more personnel than we do. Many of our competitors have long established relationships. We cannot assure you that we will be able to compete successfully with such entities in the future.
The clinical laboratory business is intensely competitive both in terms of price and service. Pricing of laboratory testing services is often one of the most significant factors used by health care providers and third-party payors in selecting a laboratory. As a result of the clinical laboratory industry undergoing significant consolidation, larger clinical laboratory providers are able to increase cost efficiencies afforded by large-scale automated testing. This consolidation results in greater price competition. We may be unable to increase cost efficiencies sufficiently, if at all, and as a result, our net earnings and cash flows could be negatively impacted by such price competition. We may also face increased competition from companies that do not comply with existing laws or regulations or otherwise disregard compliance standards in the industry. Additionally, we may also face changes in fee schedules, competitive bidding for laboratory services or other actions or pressures reducing payment schedules as a result of increased or additional competition.
Additional competition, including price competition, could have a material adverse impact on our net revenues and profitability.
An inability to attract and retain experienced and qualified personnel could adversely affect our business.
The loss of key management personnel or the inability to attract and retain experienced and qualified employees at our clinical laboratories and research centers could adversely affect our business. Our success is dependent in part on the efforts of key members of our management team, including Marc D. Grodman, M.D., our founder, president and chief executive officer. Success in maintaining our leadership position in genomic and other advanced testing technologies will depend in part on our ability to attract and retain skilled research professionals. In addition, the success of our clinical laboratories also depends on employing and retaining qualified and experienced laboratory professionals, including specialists, who perform clinical laboratory testing services. In the future, if competition for the services of these professionals increases, we may not be able to continue to attract and retain individuals in its markets. Our net revenues and earnings could be adversely affected if a significant number of professionals terminate their relationship with us or become unable or unwilling to continue their employment.
Our outstanding debt may impair our financial and operating flexibility.
As of October 31, 2012, we had approximately $4,149 million of debt outstanding. Our debt agreements contain various restrictive covenants. These restrictions could limit our ability to use operating cash flow in other areas of our business because we must use a portion of these funds to make principal and interest payments on our debt.
We or our subsidiaries may incur additional indebtedness in the future. Our ability to make principal and interest payments will depend on our ability to generate cash in the future. If we incur additional debt, a greater portion of our cash flows may be needed to satisfy our debt service obligations and if we do not generate sufficient cash to meet our debt service requirements, we may need to seek additional financing. In that case, it may be more difficult, or we may be unable, to obtain financing on terms that are acceptable to us. As a result, we would be more vulnerable to general adverse economic, industry and capital markets conditions as well as the other risks associated with indebtedness
Possible volatility in our stock price could negatively affect us and our stockholders.
The trading price of our common stock on the NASDAQ Global Market has fluctuated significantly in the past. During the period from November 1, 2009 through October 31, 2012, the trading price of our common stock fluctuated from a high of $32.42 per share to a low of $11.41per share. In the past, we have experienced a drop in stock price following an announcement of disappointing earnings or earnings guidance. Any such announcement in the future could lead to a similar drop in stock price. The price of our common stock could also be subject to wide fluctuations in the future as a result of a number of other factors, including the following:
14
changes in expectations as to future financial performance or buy/sell recommendations of securities analysts;
our, or a competitor’s, announcement of new products or services, or significant acquisitions, strategic partnerships, joint ventures or capital commitments;
the operating and stock price performance of other comparable companies; and adverse publicity.
In addition, the U.S. securities markets have experienced significant price and volume fluctuations. These fluctuations often have been unrelated to the operating performance of companies in these markets. Broad market and industry factors may lead to volatility in the price of our common stock, regardless of our operating performance. Moreover, our stock has limited trading volume, and this illiquidity may increase the volatility of our stock price.
In the past, following periods of volatility in the market price of an individual company’s securities, securities class action litigation often has been instituted against that company. The institution of similar litigation against us could result in substantial costs and a diversion of management’s attention and resources, which could negatively affect our business, results of operations or financial condition.
Certain provisions of our charter, by-laws and New Jersey law may delay or prevent a change of control of our company.
Our certificate of incorporation, as amended, requires the approval of 80% of our outstanding shares for any merger or consolidation unless the business combination has been approved or authorized by our board of directors. As a New Jersey corporation with a class of securities registered with the SEC, we are governed by certain provisions of the New Jersey Business Corporation Act that also restrict business combinations with shareholders owning 10% or more of our outstanding shares (or other “interested stockholders” as the term is defined by the New Jersey Shareholders’ Protection Act) for a period of five years after such interested shareholder achieves such status unless the business combination is approved by our board of directors prior to the shareholder becoming an interested shareholder. The New Jersey Shareholders’ Protection Act also restricts business combinations with an interested shareholder after the five-year period unless the transaction receives the approval of two-thirds of the shares outstanding, exclusive of the shares held by the interested shareholder or the transaction satisfies certain fair price requirements. In addition, with certain limited exceptions, federal regulations prohibit a person or company or a group of persons deemed to be “acting in concert” from, directly or indirectly, acquiring more than 10% (5% if the acquirer is a bank holding company) of any class of our voting stock or obtaining the ability to control in any manner the election of a majority of our directors or otherwise direct the management or policies of our company without prior notice or application to and the approval of the Federal Reserve.
A failure to obtain and retain new clients and business partners, a loss of existing clients or material contracts, or a reduction in tests ordered or specimens submitted by existing clients, could impact our ability to successfully grow our business.
To offset efforts by payors to reduce the cost and utilization of clinical laboratory services, we need to obtain and retain new clients and business partners. In addition, a reduction in tests ordered or specimens submitted by existing clients, without offsetting growth in our client base, could impact our ability to successfully grow our business and could have a material adverse impact on our net revenues and profitability. We compete primarily on the basis of the quality of testing, reporting and information systems, reputation in the medical community, the pricing of services and ability to employ qualified personnel. Our failure to successfully compete on any of these factors could result in the loss of clients and a reduction in our ability to expand our customer base.
Adverse results in material litigation matters could have a material adverse effect upon our business.
We may become subject in the ordinary course of business to material legal action related to, among other things, intellectual property disputes, professional liability and employee-related matters, as well as inquiries from governmental agencies and Medicare or Medicaid carriers requesting comment on allegations of billing irregularities that are brought to their attention through billing audits or third parties. Legal actions could result in substantial monetary damages as well as damage to our reputation with clients, which could have a material adverse effect upon our business.
Failure in our information technology systems could significantly increase testing turn-around time or billing processes and otherwise disrupt our operations.
Our laboratory operations depend, in part, on the continued performance of our information technology systems. Our information technology systems are potentially vulnerable to physical or electronic break-ins, computer viruses and similar disruptions. In addition, we are in the process of integrating the information technology systems of our recently acquired subsidiaries, and we may experience system failures or interruptions as a result of this process. Sustained system failures or interruption of our systems in one or more of our laboratory operations could disrupt our ability to process laboratory requisitions, perform testing, provide test results in a timely manner and/or bill the appropriate party. Breaches with respect to protected health information could result in violations of HIPAA and analogous state laws, and risk the imposition of significant fines and penalties. Failure of our information technology systems could adversely affect our business, profitability and financial condition.
A significant deterioration in the economy could negatively impact testing volumes, cash collections and the availability of credit.
Our operations are dependent upon ongoing demand for diagnostic testing services by patients, physicians, hospitals and others. A significant downturn in the economy could negatively impact the demand for diagnostic testing as well as the ability of patients and other payors to pay for services ordered. In addition, uncertainty in the credit markets could reduce the availability of credit and impact our ability to meet our financing needs in the future.
Failure to establish, and perform to, appropriate quality standards to assure that the highest level of quality is observed in the performance of our testing services and in the design, manufacture and marketing of our products could adversely affect the results of our operations and adversely impact our reputation.
The provision of clinical testing services, including anatomic pathology services, and related services, and the design, manufacture and marketing of diagnostic products involve certain inherent risks. The services that we provide and the products that we design, manufacture and market are intended to provide information for healthcare providers in providing patient care. Therefore, users of our services and products may have a greater sensitivity to errors than the users of services or products that are intended for other purposes.
15
Manufacturing or design defects, unanticipated use of our products, or inadequate disclosure of risks relating to the use of the products can lead to injury or other adverse events. These events could lead to recalls or safety alerts relating to our products (either voluntary or required by governmental authorities) and could result, in certain cases, in the removal of a product from the market. Any recall could result in significant costs as well as negative publicity that could reduce demand for our products. Personal injuries relating to the use of our products can also result in product liability claims being brought against us. In some circumstances, such adverse events could also cause delays in new product approvals.
Similarly, negligence in performing our services can lead to injury or other adverse events. We may be sued under physician liability or other liability law for acts or omissions by our pathologists, laboratory personnel and hospital employees who are under the supervision of our hospital-based pathologists. We are subject to the attendant risk of substantial damages awards and risk to our reputation.
Item 1B. - Unresolved Staff Comments
None.
Item 2. - Properties
We operate through a regional network of laboratories. The table below summarizes certain information as to our principal facilities as of October 31, 2012.
Location | | Purpose | | Type of
Occupancy |
Clarksburg, MD | | Pathology Laboratory | | Leased |
Elmwood Park, NJ | | Main Laboratory | | Leased |
Elmwood Park, NJ | | Corporate Headquarters | | Leased |
Gaithersburg, MD | | Genetics Laboratory | | Leased |
Houston, TX | | Pathology Laboratory | | Leased |
Milford, MA | | Oncology Laboratory | | Leased |
Poughkeepsie, NY | | Pathology Laboratory | | Leased |
We believe that each of these facilities as presently equipped has the production capacity for its currently foreseeable level of operations. We also lease additional space for patient service centers throughout the New York metropolitan area to collect specimens from physician-referred patients for testing at our processing facilities.
Item 3. - Legal Proceedings
In the normal course of business, we have been named, from time to time, as a defendant in various legal actions, which may include lawsuits alleging negligence or other similar legal claims, which could involve claims for substantial compensatory and/or punitive damages or claims for indeterminate amounts of damages, and could have an adverse impact on our client base and reputation. We are also involved, from time to time, in other reviews, investigations and proceedings by governmental agencies regarding our business, and as a health care provider and in connection with health care billing-related products, the Company may also be named from time to time in suits brought under the qui tam provisions of the False Claims Act and comparable state laws in which allegations may be made that the Company has submitted or cause to be submitted false claims in connection with claims for payment from federal or state health care programs. In addition, the Company has, from time to time, received subpoenas from state agencies and from the Office of the Inspector General of the U.S. Department of Health and Human Services seeking documents relating to the Company’s billing-related activities. These types of legal proceedings could result in adverse judgments, including substantial monetary settlements, significant fines and penalties, as well as injunctions or other relief.
At October 31, 2012 and at the date of this Report, we were not involved in any material legal proceedings, and management believes that established reserves and present insurance coverage are sufficient to cover any estimated exposures. However, the clinical laboratory testing industry is subject to extensive and evolving regulation and increasing enforcement activity, making such estimates uncertain, and potential violation of these extensive and changing statutes and regulations could result in adverse judgments, including substantial monetary settlements, significant fines and penalties, as well as injunctions or other relief, such as the loss of various licenses, certificates and authorizations. There can be no assurance, therefore, that applicable statutes and regulations will not be interpreted or applied by a prosecutorial, regulatory or judicial authority in a manner that would adversely affect the Company, and that estimates regarding potential losses associated with such claims will prove adequate.
Item 4. — Not Applicable.
16
PART II
Item 5. - Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities
Market Information
Our Common Stock is listed for trading on The NASDAQ Global Market System under the symbol “BRLI.”
The following table sets forth the range of high and low closing prices on the NASDAQ Stock Market for our Common Stock for the periods indicated.
Fiscal Year | | Prices ($) | |
2011 | | High | | Low | |
First Quarter (11/1/2010-1/31/2011) | | 24.02 | | 20.53 | |
Second Quarter (2/1/2011-4/30/2011) | | 25.21 | | 20.82 | |
Third Quarter (5/1/2011-7/31/2011) | | 25.24 | | 19.65 | |
Fourth Quarter (8/1/2011-10/31/2011) | | 20.77 | | 16.97 | |
2012 | | High | | Low | |
First Quarter (11/1/2011-1/31/2012) | | 20.02 | | 11.41 | |
Second Quarter (2/1/2012-4/30/2012) | | 24.28 | | 18.58 | |
Third Quarter (5/1/2012-7/31/2012) | | 28.28 | | 18.29 | |
Fourth Quarter (8/1/2012-10/31/2012) | | 32.86 | | 24.76 | |
On January 4, 2013 the last sale price for the Common Stock on NASDAQ was $29.40 per share.
Stockholders
At January 4, 2013, the number of record owners of the Common Stock was 266. Such number of record owners was determined from our shareholder records and does not include beneficial owners whose shares are held in nominee accounts with brokers, dealers, banks and clearing agencies.
Dividends
We have not paid any dividends on our Common Stock since our inception and, do not contemplate or anticipate paying any dividends in the foreseeable future. Furthermore, our loan agreement with PNC Bank prohibits us from paying any cash dividends or making any cash distributions with respect to shares of our Common Stock.
Recent Sales of Unregistered Securities
In 2010, we entered into an employment agreement with Wendy Chung. Upon execution of the employment agreement, 11,432 shares of Common Stock were issued to Ms. Chung and another 34,293 shares were held in escrow, to be released subject to certain terms and conditions set forth in the employment agreement. Certain terms and conditions of the employment agreement were met as of December 1, 2011 and on February 3, 2012, another 11,431 shares of Common Stock were delivered to Ms. Chung. The terms and conditions of Ms. Chung’s employment agreement were met again on December 1, 2012 and, on December 14, 2012, another 11,431 shares of Common Stock were delivered to her. The final quarter of the shares of Common Stock, or 11,431 shares, remain in escrow.
Issuer Purchases of Equity Securities
On November 11, 2011, the Company announced that its board of directors has approved a Stock Repurchase Program authorizing the repurchase of up to 1,000,000 shares of its Common Stock in the over-the-counter market at prevailing market prices over the period ending October 31, 2012. As of October 31, 2012 the Company repurchased 274,018 shares at a cost of $5,193. On December 6, 2012, the Company announced that its board of directors has approved a new Stock Repurchase Program authorizing the buyback of up to 714,550 shares of its Common Stock in the over-the-counter market at prevailing market prices through October 31, 2013.
We have presented below the cumulative total return to our stockholders during the period from November 1, 2007, through October 31, 2012 in comparison to the cumulative return on the S&P 500 Index and a customized peer group of eight companies during that same period.
We have changed our peer group in fiscal 2012 from fiscal 2011. The change in our peer group from 2011 is the omission of Bioclinica, Inc. and Psychemedics Corporation because we do not believe that these companies are our peers, the omission of Genoptix, Inc., as it was purchased by Novartis AG on March 7, 2011 and the omission of MEDTOX Scientific, Inc. and Orchid Cellmark Inc., as they were acquired by Laboratory Corporation of America Holdings on August 1, 2012 and December 16, 2011, respectively.
17
New Peer Group | | Old Peer Group |
Covance Inc | | BioClinica Inc |
Enzo Biochem Inc. | | Genoptix Inc (Included through 3/7/11 when it was acquired by Novartis AG) |
Genomic Health Inc | | Laboratory Corporation of America Holdings |
Laboratory Corporation of America Holdings | | MEDTOX Scientific Inc (Included through 7/31/12 when it was acquired by Laboratory Corp of America Holdings) |
Myriad Genetics Inc | | Neogenomics Inc |
Neogenomics Inc | | Orchid Cellmark Inc (Included through 12/16/11 when it was acquired by Laboratory Corp of America Holdings) |
Quest Diagnostics Inc | | Psychemedics Corp |
Response Genetics Inc | | Quest Diagnostics Inc |
| | Response Genetics Inc |
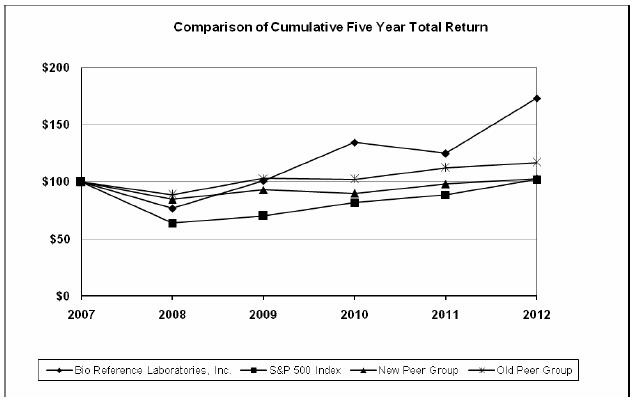
The results assume that $100 (with reinvestment of all dividends) was invested in our common stock, in the peer group, and in the index on October 31, 2007 and its relative performance tracked through October 31, 2012. The comparisons are based on historical data and are not indicative of, nor intended to forecast, the future performance of our common stock. The performance graph set forth below shall not be deemed incorporated by reference into any filing by us under the Securities Act of 1933 or the Securities Exchange Act of 1934 except to the extent that we specifically incorporate such information by reference, and shall not otherwise be deemed filed under such Acts.
18
Item 6. - Selected Financial Data
The following is a summary of our historical consolidated financial data for the periods ended and at the dates indicated below. You are encouraged to read this information together with our audited consolidated financial statements and the related footnotes and “Management’s Discussion and Analysis of Financial Condition and Results of Operations” included elsewhere in this Annual Report.
The historical consolidated financial data for the years ended October 31, 2012, 2011, and 2010 and as of October 31, 2009 and 2008 has been derived from our audited consolidated financial statements, which are included elsewhere in this Annual Report. The historical consolidated financial data for the years ended October 31, 2008 and 2009 and as of October 31, 2010, 20011, has been derived from our audited consolidated financial statements, which are not included in this Annual Report.
We believe that the comparability of our financial results between the periods presented in the table below is significantly impacted by factors which are more fully described in “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and the Consolidated Financial Statements and the notes thereto included elsewhere in this Annual Report.
| | Fiscal Years Ended October 31, | |
| | 2012 | | 2011 | | 2010 | | 2009 | | 2008 | |
| | [In Thousands Except Per Share Data] | |
Operating Data: | | | | | | | | | | | |
Net Revenues | | $ | 661,661 | | $ | 558,642 | | $ | 458,024 | | $ | 362,654 | | $ | 301,071 | |
Cost of Services | | 337,644 | | 287,853 | | 232,252 | | 183,524 | | 153,831 | |
Gross Profit | | 324,017 | | 270,789 | | 225,772 | | 179,130 | | 147,240 | |
General and Administrative Expenses | | 247,886 | | 211,015 | | 177,394 | | 140,808 | | 118,683 | |
Income From Operations | | 76,131 | | 59,774 | | 48,378 | | 38,322 | | 28,557 | |
Other Expenses [Income] - Net | | 1,615 | | (5,072 | ) | 1,415 | | (267 | ) | 1,866 | |
Provision for Income Tax Expense | | 32,360 | | 28,487 | | 20,582 | | 16,739 | | 11,074 | |
Net Income | | $ | 42,156 | | $ | 36,359 | | $ | 26,381 | | $ | 21,850 | | $ | 15,617 | |
Net Income Per Share - Basic | | $ | 1.52 | | $ | 1.30 | | $ | 0.95 | | $ | 0.79 | | $ | 0.57 | |
Net Income Per Share - Diluted | | $ | 1.51 | | $ | 1.29 | | $ | 0.94 | | $ | 0.78 | | $ | 0.56 | |
Other Data: | | | | | | | | | | | |
Net Cash - Operating Activities | | $ | 53,098 | | $ | 30,946 | | $ | 14,305 | | $ | 24,366 | | $ | 18,876 | |
Net Cash - Investing Activities | | $ | (21,390 | ) | $ | (15,542 | ) | $ | (18,411 | ) | $ | (10,807 | ) | $ | (9,901 | ) |
Net Cash - Financing Activities | | $ | (29,056 | ) | $ | (11,170 | ) | $ | 5,790 | | $ | (9,260 | ) | $ | (8,176 | ) |
| | As of October 31, | |
| | 2012 | | 2011 | | 2010 | | 2009 | | 2008 | |
Balance Sheet Data: | | | | | | | | | | | |
Total Assets | | $ | 312,347 | | $ | 283,259 | | $ | 244,131 | | $ | 197,390 | | $ | 171,311 | |
Total Long-Term Liabilities | | $ | 13,626 | | $ | 10,978 | | $ | 8,405 | | $ | 8,378 | | $ | 8,781 | |
Total Liabilities | | $ | 85,100 | | $ | 93,492 | | $ | 91,743 | | $ | 72,867 | | $ | 69,771 | |
Working Capital | | $ | 151,625 | | $ | 124,266 | | $ | 89,459 | | $ | 75,984 | | $ | 58,561 | |
Shareholder’s Equity | | $ | 227,247 | | $ | 189,767 | | $ | 152,388 | | $ | 124,523 | | $ | 101,540 | |
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations.
You are encouraged to read the following discussion and analysis of our financial condition and results of operations together with our audited consolidated financial statements and related footnotes included at the end of this Annual Report. This discussion and analysis contains forward-looking statements that involve risks and uncertainties. See “Risk Factors” included elsewhere in this Annual Report for a discussion of some of the important factors that could cause actual results to differ materially from those described or implied by the forward-looking statements contained in the following discussion and analysis. See “Special Note Regarding Forward-Looking Statements” included elsewhere in this Annual Report.
All amounts are presented in thousands, except share and per share amounts and per patient data.
Overview
We are a national clinical diagnostic laboratory located in northeastern New Jersey. We are a national laboratory in certain focused areas of laboratory testing and a full service laboratory in the New York super-region. We have developed a national reputation for our expertise in certain focused areas of clinical testing. GenPath, the name by which we are known for our cancer and oncology services, is recognized for the superior hematopathology services it provides throughout the country. Our Women’s Health initiative, through which we provide dedicated services for obstetrics and gynecology practices, including a unique, technically advanced multiplex process for identifying sexually transmitted infections, is also offered as GenPath. Our regional footprint lays within the New York City metropolitan area and the surrounding areas of New Jersey and southern New York State as well eastern Pennsylvania and some areas of western Connecticut; we also provide services further into New York State, Pennsylvania, Delaware and Maryland. As a regional provider, we are a full-service laboratory that primarily services physician office practices; our drivers pick up samples and deliver reports and supplies, we provide sophisticated technical support, phlebotomy services or patient service centers where appropriate, and electronic communication services in many cases. Physicians outside of our regional footprint send samples to our laboratory in order to take advantage of the expertise that we are able to provide in blood-based cancer pathology and associated diagnostics or to take advantage of the superior service, support and technologically
19
advanced testing we offer in our Women’s Health initiative. These accounts frequently send routine testing to us for processing along with specialized testing in order to simplify their diagnostic ordering and review procedures and to take advantage of our outstanding capability, service and support. Our correctional healthcare services are used throughout the country at prisons and jails. The focused markets we serve on a national basis outside of our regional footprint do not require many of the logistical and other ancillary support services required within the region. Even within our regional footprint, we provide the same services that we provide on a national basis as well as some regional focused diagnostic services, such as histology and pathology support services, substance abuse testing, fertility testing, hemostasis testing, women’s health testing, and molecular diagnostics that are unavailable from many of the smaller regional competitors; testing in some of these areas may be provided outside of physician offices. In October 2012, we launched Laboratorio Buena Salud, the first national testing laboratory dedicated to serving Spanish-speaking populations in the United States. All business will be conducted in Spanish, including patient and physician interactions.
Over the last few years, there have been fundamental changes in the laboratory services industry. In the 1990s, the industry was negatively impacted by the growth of managed care, increased government regulation, and investigations into fraud and abuse. These factors led to revenue and profit declines and industry consolidations, especially among commercial laboratories. There are currently only three US publicly traded full service laboratories operating primarily in the U.S. While that means that the two national mega-laboratories and Bio-Reference Laboratories are the only remaining publicly traded full service commercial laboratories, there are numerous hospital outreach programs and smaller reference laboratories that compete for the commercial clinical laboratory business scattered throughout the country. Clinical laboratories have had to improve efficiency, leverage economies of scale, comply with government regulations and other laws and develop more profitable approaches to pricing. Moreover, there has been a proliferation of technology advancements in clinical diagnostics over the last decade that has created significant opportunities for new testing and growth.
As a full service clinical laboratory, we are constantly looking for new technologies and new methodologies that will help us to grow. Since the turn of the century, our size alone has made us attractive to companies that are driving the advances in technology. We represent a significant opportunity for these companies to market their products with a nationally recognized specialty provider in our focused areas of specialty or in one of the major population centers of the world—the New York Metropolitan area. We have had several successful strategic relationships with such technology opportunities. In addition to new technology opportunities, we have an extremely seasoned and talented management staff that has been able to identify emerging laboratory markets that are under-served or under-utilized. We have recently developed programs for cardiology, histology and women’s health to go along with our existing hemostasis, hematopathology and correctional healthcare initiatives which have already been established and in which we have been increasing our market share for the past several years. We are currently preparing to launch a comprehensive pre-natal program to leverage our presence in the women’s health environment and we will continue to vigilantly seek focused diagnostic marketing opportunities where we can provide information, technology, service or support that expand and grow our clinical laboratory.
On March 2, 2010, we completed the purchase of Lenetix Medical Screening Laboratory, Inc. (“Lenetix”) from Lenetix and its sole stockholder. These assets were utilized in Lenetix’s operation of a clinical testing laboratory located in Mineola, New York. The laboratory performs both clinical laboratory diagnostic testing and genetic testing.
On August 5, 2011, we acquired all of the authorized, issued and outstanding shares of The Genetics Center, Inc. (“GCI”), a New York corporation engaged in the clinical laboratory business with principal place of business in Smithtown, New York.
On April 27, 2012, we entered into an agreement pursuant to which we purchased preferred shares of IncellDx, Inc. (“IncellDx”), a Delaware corporation. Information about IncellDx and the agreement may be found in the Current Report on Form 8-K we filed on May 1, 2012 and in note 18 to our consolidated financial statements.
On December 21, 2012, a date subsequent to our year end, we entered into an agreement pursuant to which we agreed to purchase all of the authorized, issued and outstanding shares of Meridian Clinical Laboratory, Corp. (“Meridian”), a Florida corporation. Information about Meridian and the agreement may be found in the Form 8-K we filed.
On December 31, 2012, a date subsequent to our year end, we entered into an agreement pursuant to which we agreed to purchase all of the authorized, issued and outstanding shares of Florida Clinical Laboratory, Inc. (“FCL”), a Florida corporation. Information about FCL and the agreement may be found in the Form 8-K we filed on January 4, 2013.
While we recognize that we are a clinical laboratory that processes samples, we also understand that we are an information company that needs to effectively communicate the results of our efforts back to healthcare providers. Laboratory results play a major role in the implementation of physician healthcare. Laboratory results are used to diagnose, monitor and classify health concerns. In many cases, laboratory results represent the confirming data in diagnosing complicated health issues. Since laboratory results play such an important role in routine physician care, we have developed informatics solutions that leverage our role in healthcare. We built a web-based solution to quickly, accurately, conveniently and competitively collect ordering information and deliver results. That solution is called CareEvolve. CareEvolve has been essential to our own operations. We license the technology to other laboratories throughout the country that they utilize to more effectively compete against the national laboratories. These other laboratories licensing our technology are typically not our competitors since they are outside our regional footprint.
We have also created our PSIMedica business unit that has developed a Clinical Knowledge Management (CKM) System that takes data from enrollment, claims, pharmacy, laboratory results and any other available electronic source to provide both administrative and clinical analysis of a population. The system uses proprietary algorithms to cleanse and configure the data and transfer the resulting information into a healthcare data repository. Using advanced cube technology methodologies, the data can be analyzed from a myriad of views and from highly granular transactional detail to global trended overview. Events such as the Katrina disaster in Louisiana and general pressures from the government have made development of an electronic medical record system and Pay-for Performance reimbursement priority goals in the healthcare industry. A large portion of an individual’s medical record consists of laboratory data and a key performance indicator in any Pay-for-Performance initiative is laboratory result data. Our CKM system is a mature, full functioning solution that will allow us to play a role in these important national initiatives.
To date, neither our PSIMedica business unit nor CareEvolve has produced significant revenues relative to the primary laboratory operations.
Results of Operations
Fiscal Year 2012 Compared to Fiscal Year 2011
NET REVENUES:
Net revenues for the year ended October 31, 2012 were $661,661 as compared to $558,642 for the year ended October 31, 2011; this represents an 18% increase in net revenues. This increase is due to a 16% increase in patients serviced and a 2% increase in net revenue per patient. Our laboratory operations had net revenues of $657,158 in fiscal 2012 and $554,281 in fiscal 2011.
The number of patients serviced during the year ended October 31, 2012 was 7,801, which was 16% greater when compared to the prior fiscal year. Net revenue per patient for the year ended October 31, 2012 was $84.24 compared to net revenue per patient for the year ended October 31, 2011 of $82.25, an increase of 2% as a result of increases in esoteric testing.
During the fiscal year ended October 31, 2012, we increased our sales force by approximately 12%, mostly in the specialty testing services that we market nationally. We believe that this increase in sales personnel accounted for a majority of the 16% increase in our patient volume. This
20
allowed us to expand or increase our presence in a number of markets and we expect this trend to continue.
While there is always uncertainty as to the sustainability of such growth in the future, we believe that our historical performance of 20% compound annual growth rate for the past 18 years, the current demand for our services and our continued corporate focus on strategic growth, together with our expertise in the industry, should enable us to sustain continued strong growth in the near term. Going beyond that, however, our revenues and patient counts could be adversely affected by a number of factors including, but not limited to an extended downturn in general or healthcare economic conditions, an unexpected reduction in reimbursement rates, increased market penetration by our competitors, or a substantial adverse change in federal regulatory requirements governing our industry as well as a failure to continue the sizeable annual percentage increase in base business from significantly higher levels after 17 years of sustained growth.
Our net revenues for the fourth quarter of fiscal 2012 and cumulative results for the fiscal 2012 as well as operating results during the first quarter of fiscal 2013 have been affected by the adverse weather conditions associated with the hurricane Sandy. Based on actual revenues and expenses from the period immediately preceding the storm as well as the analysis of the period following the storm, management has calculated the damage from, the hurricane Sandy resulted in a loss of net revenues of approximately $5,000 for the fourth quarter of fiscal 2012 and approximately $3,000 for the first quarter of fiscal 2013.
COST OF SERVICES:
Cost of services for the year ended October 31, 2012 was $337,644 as compared to $287,853 for the year ended October 31, 2011, an increase of 17% as compared to an 18% increase in net revenues. The Company’s medical supplies expense increased by 34% due to the higher cost of specialty testing supplies. Our medical equipment repair costs increased by 26% year over year due to higher equipment utilization rate. We expect these trends to continue.
GROSS PROFIT:
Gross profit on net revenues increased to $324,017 for the year ended October 31, 2012 from $270,789 for the year ended October 31, 2011; an increase of $53,328 (20%), primarily attributable to the increase in net revenues. Gross profit margins increased to 49% for fiscal 2012 from fiscal 2011 rate of 48%.
GENERAL AND ADMINISTRATIVE EXPENSES:
General and administrative expenses for the year ended October 31, 2012 were $247,886 as compared to $211,015 for the year ended October 31, 2011, an increase of $36,871 or 17%. This is basically in line with the increase in net revenues. We expect this trend to continue in the near future.
INTEREST EXPENSE:
Interest expense decreased from $1,747 during the year ended October 31, 2011 to $1,455 during the year ended October 31, 2012; a decrease of $292 or 17%. This decrease is due to a decrease in utilization of the PNC Bank line of credit. Management believes that this trend will continue in the near term due to the decrease in utilization of this credit facility.
NET INCOME:
We realized net income of $42,156 for the twelve month period ended October 31, 2012 as compared to $36,359 for the twelve month period ended October 31, 2011, an increase of 16%.
Pre-tax income for the period ended October 31, 2012 was $74,516, as compared to $64,846 for the period ended October 31, 2011, an increase of $9,670 (15%) and was caused primarily by an increase in net revenues. The provision for income taxes increased from $28,487 for the period ended October 31, 2011, to $32,360 (14%) for the current twelve month period.
Our diluted net income per share went from $1.16 on a pro-forma basis (without taking into account the following non-recurring items: the New Jersey sales tax refund, the loss on sale of corporate aircraft and the New York excess laboratory fee refund) in fiscal 2011 to $1.51in fiscal 2012.
Our operating results for the fourth quarter of fiscal 2012 and cumulative results for the fiscal 2012 as well as operating results during the first quarter of fiscal 2013 have been affected by hurricane Sandy. Based on actual revenues and expenses from the period immediately preceding the storm as well as the analysis of the period following the storm, Management has calculated the damage from the storm resulted in a loss of earnings approximately $0.06 per share for the fourth quarter of fiscal 2012 and approximately $0.03 per share for the first quarter of fiscal 2013.
Fiscal Year 2011 Compared to Fiscal Year 2010
NET REVENUES:
Net revenues for the year ended October 31, 2011 were $558,642 as compared to $458,024 for the year ended October 31, 2010; this represents a 22% increase in net revenues. This increase is due to a 20% increase in patients serviced and a 2% increase in net revenue per patient. Our laboratory operations had net revenues of $454,308 in fiscal 2010 and $554,281 in fiscal 2011.
The number of patients serviced during the year ended October 31, 2011 was 6,739, which was 20% greater when compared to the prior fiscal year. Net revenue per patient for the year ended October 31, 2011 was $82.25 compared to net revenue per patient for the year ended October 31, 2010 of $81.03, an increase of $1.22 or 2% as a result of increases in esoteric testing.
During the fiscal year ended October 31, 2011, we increased our sales force by approximately 19% in the specialty testing services that we market nationally. This increase occurred in two phases: one in January 2011 and one in July of the same year. We believe that this increase in sales personnel accounted for a majority of the 20% increase in our patient volume. This allowed us to expand or increase our presence in sixteen states and we expect this trend to continue.
While there is always uncertainty as to the sustainability of such growth in the future, we believe that our historical performance of 20% compound annual growth rate for the past 17 years, the current demand for our services and our continued corporate focus on strategic growth, together with our expertise in the industry, should enable us to sustain continued strong growth in the near term. Going beyond that, however, the Company’s revenues and patient counts could be adversely affected by a number of factors including, but not limited to an extended downturn in general or healthcare economic conditions, an unexpected reduction in reimbursement rates, increased market penetration by our competitors, or a substantial adverse change in federal regulatory requirements governing our industry as well as a failure to continue the sizeable annual percentage increase in base business from significantly higher levels after 17 years of sustained growth.
21
COST OF SERVICES:
Cost of Services for the year ended October 31, 2011 was $287,853 as compared to $232, 252 for the year ended October 31, 2010, an increase of 24% as compared to a 22% increase in net revenues. The Company’s reagents and laboratory supplies expense increased by 29% due to the higher cost of specialty testing reagents. Our vehicle operating expenses also increased by 25% due to the higher cost of fuel. Our medical equipment repair costs increased by 44% year over year due to higher equipment utilization rate. We expect these trends to continue.
GROSS PROFIT:
Gross profit on net revenues increased to $270,789 for the year ended October 31, 2011 from $225,772 for the year ended October 31, 2010; an increase of $45,017 (20%), primarily attributable to the increase in net revenues. Gross profit margins decreased to 48% for fiscal 2011 from fiscal 2010 rate of 49%.
GENERAL AND ADMINISTRATIVE EXPENSES:
General and administrative expenses for the year ended October 31, 2011 were $211,015 as compared to $177,394 for the year ended October 31, 2010, an increase of $33,621 or 19%. This is basically in line with the increase in net revenues. Marketing expenses increased by 25% due to increases in our sales force together with substantial investment in marketing materials and we expect this trend to continue in the near future.
INTEREST EXPENSE:
Interest expense increased from $1,566 during the year ended October 31, 2010 to $1,747 during the year ended October 31, 2011; an increase of $181 or 12%. This increase is due to an increase in utilization of the PNC Bank line of credit, acquisition debt and capital leases. Management believes that this trend will continue in the near term due to the increase in utilization rates.
NET INCOME:
We realized net income of $36,359 for the twelve month period ended October 31, 2011 as compared to $26,381 for the twelve month period ended October 31, 2010, an increase of 38%.
Pre-tax income for the period ended October 31, 2011 was $64,846, as compared to $46,963 for the period ended October 31, 2010, an increase of $17,883 (38%) and was caused primarily by an increase in net revenues. The provision for income taxes increased from $20,582 for the period ended October 31, 2010, to $28,487 (38%) for the current twelve month period.
Our diluted net income per share went from $0.94 in fiscal 2010 to $1.29 in fiscal 2011, or $1.16 on a pro-forma basis (without taking into account the following non-recurring items: the New Jersey sales tax refund, the loss on sale of corporate aircraft and the New York excess laboratory fee refund).
Liquidity and Capital Resources
Our working capital at October 31, 2012 was approximately $151,625 as compared to approximately $124,266 at October 31, 2011, an increase of $27,359 (22%). Our cash position increased by approximately $2,652 during the current twelve month period. We decreased our short term borrowing by approximately $19,110 and approximately $2,076 in long term debt. We had current liabilities of approximately $71,474 at October 31, 2012. We generated approximately $53,098 in cash from operations, an increase of approximately $22,152 as compared to the year ended October 31, 2011.
Accounts receivable, net of allowance for doubtful accounts, totaled approximately $153,247 at October 31, 2012, an increase of approximately $5,187 from October 31, 2011, or 4%. This increase was primarily attributable to increased revenue. Cash collected over the twelve month period ended October 31, 2012 increased 22% over the prior twelve month period.
Net service revenues on the statements of operations are as follows:
| | October, 31 | |
| | 2012 | | 2011 | | 2010 | |
| | | | | | | |
Gross Revenues | | $ | 3,052,431 | | $ | 2,482,349 | | $ | 1,902,573 | |
| | | | | | | |
Contractual Adjustments and Discounts: | | | | | | | |
Medicare/Medicaid Portion | | 320,697 | | 293,874 | | 281,002 | |
All Other Third Party and Direct Payors* | | 2,070,073 | | 1,629,833 | | 1,163,547 | |
Total Contractual Adjustments and Discounts | | 2,390,770 | | 1,923,707 | | 1,444,549 | |
| | | | | | | |
Net Service Revenues | | $ | 661,661 | | $ | 558,642 | | $ | 458,024 | |
| | | | | | | |
Percent of Contractual Adjustments and Discounts To Gross Revenues | | 78.3 | % | 77.5 | % | 75.9 | % |
* All Other Third Party and Direct Payors consists of almost eight hundred distinct payors, including commercial health insurers and administrators as well as professionally billed accounts such as physicians, hospitals, clinics and other direct billed accounts.
The table above illustrates the relationship between contractual adjustments and gross revenues for the fiscal years 2012, 2011, and 2010. Between 2011 and 2012, contractual adjustments increased approximately 80 basis points. For example, the average “across the board” collection
22
percent for fiscal year 2007 was 26%, while the rate for fiscal year 2012 was 17%, a decrease in our collection rate of 9%, or a 35% reduction in the collection rate. In the aggregate, this has resulted in a change of our contractual rate, leading to larger contractual allowances and lower net revenues when computed as a percentage of gross revenues. Although individual collection rates may vary from period to period or payor to payor, based on the specific historical data analyzed, this is consistent with the current state of the economy as well as the ongoing trends in health care reimbursement.
Credit risk with respect to accounts receivable is generally diversified due to the large number of patients comprising our client base. We have significant receivable balances with government payors and various insurance carriers. Generally, we do not require collateral or other security to support customer receivables. However, we continually monitor and evaluate our client acceptance and collection procedures to minimize potential credit risks associated with our accounts receivable and to establish an allowance for uncollectible accounts. As a consequence, we believe that our accounts receivable credit risk exposure beyond such allowance is not material to the financial statements.
A number of proposals for legislation continue to be under discussion which could substantially reduce Medicare and Medicaid (CMS) reimbursements to clinical laboratories. Depending upon the nature of regulatory action, and the content of legislation, we could experience a significant decrease in revenues from Medicare and Medicaid (CMS), which could have a material adverse effect on us. We are unable to predict, however, the extent to which such actions will be taken.
LABORATORY GROSS RECEIVABLES BY PAYOR GROUP
| | ($)
FY 2012 | |
| | 30 DAYS | | % | | 60 DAYS | | % | | 90 DAYS | | % | | >90 DAYS | | % | | TOTAL | | % | |
Self Pay | | 9,620 | | 18 | % | 10,633 | | 20 | % | 9,474 | | 18 | % | 24,202 | | 44 | % | 53,929 | | 100 | % |
Medicare | | 25,898 | | 56 | % | 6,550 | | 14 | % | 2,992 | | 6 | % | 11,186 | | 24 | % | 46,626 | | 100 | % |
Medicaid | | 4,881 | | 23 | % | 3,804 | | 18 | % | 3,829 | | 18 | % | 8,714 | | 41 | % | 21,228 | | 100 | % |
Pro Bill | | 17,697 | | 64 | % | 4,706 | | 17 | % | 1,771 | | 6 | % | 3,657 | | 13 | % | 27,832 | | 100 | % |
Commercial Insurance | | 154,294 | | 47 | % | 53,097 | | 17 | % | 24,752 | | 8 | % | 88,747 | | 28 | % | 320,889 | | 100 | % |
Total | | 212,390 | | 45 | % | 78,790 | | 17 | % | 42,818 | | 9 | % | 136,507 | | 29 | % | 470,505 | | 100 | % |
| | | |
| | FY 2011 | |
| | 30 DAYS | | % | | 60 DAYS | | % | | 90 DAYS | | % | | >90 DAYS | | % | | TOTAL | | % | |
Self Pay | | 7,790 | | 16 | % | 8,614 | | 18 | % | 8,475 | | 18 | % | 22,526 | | 48 | % | 47,405 | | 100 | % |
Medicare | | 25,991 | | 45 | % | 11,082 | | 19 | % | 4,501 | | 8 | % | 15,858 | | 28 | % | 57,433 | | 100 | % |
Medicaid | | 5,664 | | 24 | % | 3,476 | | 14 | % | 3,419 | | 14 | % | 11,534 | | 48 | % | 24,093 | | 100 | % |
Pro Bill | | 18,304 | | 63 | % | 4,925 | | 17 | % | 1,691 | | 6 | % | 4,341 | | 15 | % | 29,260 | | 100 | % |
Commercial Insurance | | 134,372 | | 49 | % | 47,903 | | 18 | % | 27,542 | | 10 | % | 62,768 | | 23 | % | 272,585 | | 100 | % |
Grand Total | | 192,121 | | 45 | % | 76,000 | | 18 | % | 45,629 | | 11 | % | 117,027 | | 27 | % | 430,776 | | 100 | % |
Billing for laboratory services is complicated and we must bill various payors, such as the individual, the insurance company, the government (federal or state), the private company or the health clinic. Other factors that may complicate billing include:
Differences between fee schedules and reimbursement rates;
Incomplete or inaccurate billing information as provided by the physician;
Disparity in coverage and information requirements;
Disputes with payors; and
Internal and external compliance policies and procedures.
Significant costs are incurred as a result of our participation in government programs since billing and reimbursement for laboratory tests are subject to complex regulations. We perform the requested tests and report the results whether the information is correct or not or even missing. This adds to the complexity and slows the collection process and increases the aging of our accounts receivable (“A/R”). When patient invoices are not collected in a timely manner the item is written off to the allowance.
Days Sales Outstanding (“DSO”) for fiscal years 2011 and 2012 were 91 and 80, respectively, a decrease of approximately 12%. These changes are due to constant vigilance on the part of management and internal changes to collection practices. However, when you compare our DSO lag to our collectible net revenues as reported on our financial statements for the periods in question, it varies between 98% to 102%, depending on the period.
Overall, the components of A/R as shown above for the two most recently completed fiscal years under review have not varied much year over year. The percent of A/R over 90 days has increased to 29% as of October 31, 2012 as compared to 27% as of October 31, 2011, an increase of only 2%.
See Note 5 and Note 6 to our consolidated financial statements for information regarding outstanding loans.
See Note 18 to our consolidated financial statements describing our merger and acquisition activities.
The weighted average interest rate on short-term borrowings outstanding as of October 31, 2012 was 3.25% and as of 2011 was approximately 3.25%.
We intend to expand our laboratory operations through aggressive marketing while also attempting to diversify into related medical fields through acquisitions. These acquisitions may involve cash, notes, Common Stock, and/or combinations thereof.
23
Contractual Obligations
The following table summarizes our significant contractual obligations as of October 31, 2012:
| | Total ($) | | FY 2013 ($) | | FY 2014 ($) | | FY 2015 ($) | | FY 2016 ($) | | FY 2017 ($) | | Thereafter ($) | |
Long-Term Debt | | 4,627 | | 458 | | 486 | | 518 | | 551 | | 585 | | 2,029 | |
Capital Leases | | 5,395 | | 1,200 | | 1,199 | | 1,199 | | 1,199 | | 598 | | — | |
Operating Leases | | 15,250 | | 7,127 | | 3,680 | | 1,608 | | 1,049 | | 429 | | 1,357 | |
Purchase Obligations | | 91,073 | | 23,758 | | 22,365 | | 19,943 | | 17,441 | | 7,566 | | — | |
Long-Term Liabilities under Employment and Consultant Contracts | | 16,961 | | 4,982 | | 4,302 | | 3,654 | | 2,780 | | 1,243 | | — | |
No one supplier who is counterparty to any particular supply agreement is contracted to provide more than one percent of our Cost of Services in any future period. Such contracts are made in the ordinary course of business. No directors, officers, promoters, voting trustees or individuals known to be Bio-Reference Laboratories, Inc (“BRLI”) security holders are counterparties to these agreements. Management does not believe that BRLI is substantially dependent upon these supply agreements, as the goods may be obtained from different suppliers or wholesalers, if needed. None of these agreements are leases or call for the acquisition or sale of property, plant and equipment.
Our cash balances at October 31, 2012 totaled approximately $24,665 as compared to approximately $22,013 at October 31, 2011. We believe that our cash position, the anticipated cash generated from future operations, and the availability of our credit line with PNC Bank, will meet our anticipated cash needs in fiscal 2013.
Off-Balance Sheet Arrangements
As of October 31, 2012, we did not have any off-balance sheet items.
Impact of Inflation
To date, inflation has not had a material effect on our operations.
Critical Accounting Policies
The preparation of financial statements in conformity with U.S. generally accepted accounting principles requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the reported periods.
Accounting for Intangible and Other Long-Lived Assets
We evaluate the possible impairment of our long-lived assets, including intangible assets. We review the recoverability of our long-lived assets on an annual basis or earlier if events or changes in circumstances occur that indicate that the carrying value of the asset may not be recoverable. Evaluation of possible impairment is based on our ability to recover the asset from the expected future pretax cash flows (undiscounted and without interest charges) of the related operations. If the expected undiscounted pretax cash flows are less than the carrying amount of such asset, an impairment loss is recognized for the difference between the estimated fair value and the carrying amount of the asset.
Accounting for Revenue
Service revenues are principally generated from laboratory testing services including chemical diagnostic tests such as blood analysis, urine analysis and genetic testing among others. Net service revenues are recognized at the time the testing services are performed and are reported at their estimated net realizable amounts.
Net service revenues are determined utilizing gross service revenues net of contractual allowances. Even though it is the responsibility of the patient to pay for laboratory service bills, most individuals in the United States have an agreement with a third party payor such as Medicare, Medicaid or a commercial insurance provider to pay all or a portion of their healthcare expenses; the majority of services provided by BRLI are to patients covered under a third party payor contract. In certain cases, the individual has no insurance or does not provide insurance information and in other cases tests are performed under contract to a professional organization (such as physicians, hospitals, and clinics) which reimburse BRLI directly; in the remainder of the cases, BRLI is provided the third party billing information and seeks payment from the third party under the terms and conditions of the third party payor for health service providers like BRLI. Each of these third party payors may differ not only with regard to rates, but also with regard to terms and conditions of payment and providing coverage (reimbursement) for specific tests. Estimated revenues are established based on a series of highly complex procedures and judgments that require industry specific healthcare experience and an understanding of payor methods and trends. We review our calculations on a monthly basis in order to make certain that we are properly allowing for the uncollectable portion of our gross billings and that our estimates remain sensitive to variances and changes within our payor groups. The contractual allowance calculation is made on the basis of historical allowance rates for the various specific payor groups on a monthly basis with a greater weight being given to the most recent trends; this process is adjusted based on recent changes in underlying contract provisions and shifts in the testing being performed. Bad Debt represents our estimate of net revenues that will ultimately be uncollectable and is based upon our analysis of historical payment rates by specific payor groups on a monthly basis with primary weight being given to the most recent trends; this approach allows bad debt to more accurately adjust to short-term changes in the business environment. These two calculations are routinely analyzed by BRLI on the basis of actual allowances issued by payors and the actual payments made to determine what adjustments, if any, are needed. The chart below shows the adjustments made to gross service revenues to arrive at net service revenues.
24
| | October, 31 | �� |
| | 2012 | | 2011 | | 2010 | |
| | | | | | | |
Gross Revenues | | $ | 3,052,431 | | $ | 2,482,349 | | $ | 1,902,573 | |
| | | | | | | |
Contractual Adjustments and Discounts: | | | | | | | |
Medicare/Medicaid Portion | | 320,697 | | 293,874 | | 281,002 | |
All Other Third Party and Direct Payors* | | 2,070,073 | | 1,629,833 | | 1,163,547 | |
Total Contractual Adjustments and Discounts | | 2,390,770 | | 1,923,707 | | 1,444,549 | |
| | | | | | | |
Net Service Revenues | | $ | 661,661 | | $ | 558,642 | | $ | 458,024 | |
| | | | | | | |
Percent of Contractual Adjustments and Discounts To Gross Revenues | | 78.3 | % | 77.5 | % | 75.9 | % |
* All Other Third Party and Direct Payors consists of almost eight hundred distinct payors, including commercial health insurers and administrators as well as professionally billed accounts such as physicians, hospitals, clinics and other direct billed accounts.
When new business is received by BRLI, net service revenues are calculated by reducing gross service revenues by the estimated contractual allowance. The bad debt expense is determined by calculating the appropriate collection rate for net current service revenues and is a component of general and administrative expenses. BRLI recognized the amounts in subsequent periods for actual allowances/discounts to gross service revenue; bad debt was adjusted over the same periods of time to maintain an accurate balance between net service revenues and actual revenues. Management has reviewed the allowances/discounts recognized in subsequent periods and believes the amounts to be immaterial. A number of proposals for legislation or regulation continue to be under discussion which could have the effect of substantially reducing Medicare reimbursements for clinical laboratories or introducing cost sharing to beneficiaries. Depending upon the nature of regulatory action, if any, which is taken and the content of legislation, if any, which is adopted, the Company could experience a significant decrease in revenues from Medicare and Medicaid, which could have a material adverse effect on the Company. The Company is unable to predict, however, the extent to which such actions will be taken.
Accounting for Contractual Credits and Doubtful Accounts
It is typically the responsibility of the patient to pay for laboratory service bills. Most individuals in the United States have an agreement with a third party payor such as Medicare, Medicaid or commercial insurance to pay all or a portion of their healthcare expenses; this represents the major portion of payment for all services provided to BRLI. In certain cases, the individual has no insurance or does not provide insurance information; in the remainder of the cases, BRLI is provided the third party billing information, usually by the referring physician, and seeks payment from the third party under the terms and conditions of the third party payor for health service providers like BRLI. Each of these third party payors may differ not only with regard to rates, but also with regard to terms and conditions of payment and coverage of specific tests. BRLI routinely reviews the reimbursement policies and subsequent payments and collection rates from these different types of payors. Contractual credits are recorded as reductions to gross service revenues and are collectively referred to as the contractual allowance. BRLI has not been required to record an adjustment in a subsequent period related to revenue recorded in a prior period which was material in nature. Aging of accounts receivable is monitored by billing personnel and follow-up activities including collection efforts are conducted as necessary. Bad debt expense is recorded within selling, general and administrative expenses. BRLI writes off receivables against the allowance for doubtful accounts when they are deemed uncollectible. For client billing, accounts are written off when all reasonable collection efforts prove to be unsuccessful. Patient accounts, where the patient is directly responsible for all or a remainder portion of the account after partial payment or denial by a third party payor, are written off after the normal dunning cycle has occurred, although these may be subsequently transferred to a third party collection agency after being written off. Third party payor accounts are written off when they exceed the payor’s timely filing limits. Accounts Receivable on the balance sheet is net of the following amounts for contractual credits and doubtful accounts:
| | October 31 | |
| | 2012 | | 2011 | |
| | | | | |
Contractual Credits/Discounts | | $ | 267,921 | | $ | 235,922 | |
Doubtful Accounts | | 51,274 | | 45,220 | |
| | | | | |
Total Allowance | | $ | 319,195 | | $ | 281,142 | |
Accounting for Employee Benefit Plans
See Note 21 to our consolidated financial statements for a discussion on Employee Benefit Plans.
New Authoritative Pronouncements
See Note 22 to our consolidated financial statement that discusses new authoritative pronouncements.
Item 7A. - Quantitative and Qualitative Disclosures about Market Risk
We do not invest in or trade instruments which are sensitive to market risk. We also do not have any material foreign operations or foreign sales so we have no exposure to foreign currency exchange rate risk.
25
We do have exposure to both rising and falling interest rates. At October 31, 2012, advances of approximately $-0- under our Loan Agreement with PNC Bank were subject to interest charges at the bank’s then prime rate of 3.25 %.
We estimate that our monthly cash interest expense on the PNC bank Loan Agreement at October 31, 2012 was $-0-as the loan was paid off. A one percentage point increase or decrease in short-term rates would not increase or decrease our monthly interest expense as the loan was paid off. However we expect to utilize the credit line in the future and we thus expect exposure to short term interest rates changes that will depend on the utilization rate at the time.
See Note 5 and Note 6 to the Consolidated Financial Statements contained herein for information on our loans.
Item 8.- Financial Statements and Supplementary Data
Financial Statements are annexed hereto.
Item 9. - Changes in and Disagreements with Accountants on Accounting and Financial Disclosure
None
Item 9A. - Controls and Procedures
(a) Evaluation of Disclosure Controls and Procedures
An evaluation was performed under the supervision and with the participation of our management, including our principal executive officer and our principal financial officer as to the effectiveness of our disclosure controls and procedures (as defined in Rule 13a-15(e) under the Exchange Act) as of the end of the period covered by this report. Any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving the desired control objectives. Based on that evaluation, the principal executive officer and the principal financial officer of the Company have concluded that, as of the end of the period covered by this report, our disclosure controls and procedures are effective at a reasonable assurance level.
(b) Management’s Annual Report on Internal Control over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting to provide reasonable assurance regarding the reliability of our financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. Internal control over financial reporting includes those policies and procedures that:
(i) pertain to the maintenance of records that in reasonable detail accurately and fairly reflect the transactions and dispositions of our assets;
(ii) provide reasonable assurance that the transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that our receipts and expenditures are being made only in accordance with the authorization of management and/or our Board of Directors; and
(iii) provide reasonable assurance regarding the prevention or timely detection of any unauthorized acquisition, use or disposition of our assets that could have a material effect on our financial statements.
Due to its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate due to changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Under the supervision and with the participation of our management, including our principal executive officer and principal financial officer, we conducted an evaluation of the effectiveness of our internal control over financial reporting using the criteria set forth by the Committee of Sponsoring Organizations of the Treadway Commission (COSO) in Internal Control-Integrated Framework. Based on its evaluation, our management concluded that our internal control over financial reporting was effective as of the end of the period covered by this Annual Report on Form 10-K.
MSPC, Certified Public Accountants and Advisors, A Professional Corporation, an independent registered public accounting firm, has audited the Consolidated Financial Statements included in this Annual Report on Form l0-K and, as part of their audit, has issued its attestation report, included herein, on the effectiveness of our internal control over financial reporting. See “Report of Independent Registered Public Accounting Firm” on included in this filling.
(c) Changes in Internal Control over Financial Reporting
There has been no change in our internal control over financial reporting that occurred during the fourth quarter of fiscal 2012 that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
Item 9B. - Other Information
None.
26
PART III
Item 10. - Directors, Executive Officers and Corporate Governance
Executive Officers and Directors
The following table sets forth certain information with respect to each of our directors and executive officers.
Name | | Age | | Position | |
Marc D. Grodman, M.D | | 61 | | Chairman of the Board, President, Chief Executive Officer and Director | |
Howard Dubinett | | 61 | | Executive Vice President, Chief Operating Officer and Director | |
Sam Singer | | 69 | | Senior Vice President, Chief Financial Officer, Chief Accounting Officer and Director | |
Joseph Benincasa(a)(c)(e) | | 63 | | Director | |
Harry Elias(a)(c)(e) | | 82 | | Director | |
Gary Lederman, Esq. (b)(c)(e) | | 78 | | Director | |
John Roglieri, M.D. (a)(d)(e) | | 73 | | Director | |
(a) Member of the Audit Committee
(b) Chairman of the Audit Committee
(c) Member of the Compensation Committee
(d) Chairman of the Compensation Committee
(e) Member of Nominating Committee
Marc D. Grodman, M.D. founded the Company in December 1981 and has been our Chairman of the Board, President, Chief Executive Officer and a director since our formation. Dr. Grodman is an Assistant Professor of Clinical Medicine at Columbia University’s College of Physicians and Surgeons and Assistant Attending Physician at Presbyterian Hospital, New York City. Since January 2005, Dr. Grodman has been a member of the board of directors, served as Chairman and currently serves as Vice Chairman of the American Clinical Laboratory Association, an industry organization comprised of the largest and most significant commercial clinical laboratories in the United States. From 1980 to 1983, Dr. Grodman attended the Kennedy School of Government at Harvard University and was a Primary Care Clinical Fellow at Massachusetts General Hospital. From 1982 to 1984, he was a medical consultant to the Metal Trades Department of the AFL-CIO. Dr. Grodman received a B.A. degree from the University of Pennsylvania in 1973 and an M.D. degree from Columbia University’s College of Physicians and Surgeons in 1977. Except for his part-time duties as Assistant Professor of Clinical Medicine and Assistant Attending Physician at Columbia University and Presbyterian Hospital, Dr. Grodman devotes all of his working time to our business. We believe that Dr. Grodman is qualified to serve on our board of directors because of his extensive medical expertise, his experience on the faculty at Columbia University College of Physicians and Surgeons, his leadership role in our industry and his knowledge of trends in the healthcare industry.
Howard Dubinett has been our Executive Vice-President and Chief Operating Officer of the Company since our formation in 1981. He became a director in April 1986. Mr. Dubinett attended Rutgers University. We believe that Mr. Dubinett is qualified to serve on our board of directors because of his extensive knowledge of and experience in our business and his knowledge of healthcare regulation.
Sam Singer has been our Chief Financial Officer since October 1987, a director since November 1989, and a Senior Vice President since 2007. Mr. Singer was the Controller for Sycomm Systems Corporation, a data processing and management consulting company, from 1981 to 1987, prior to joining us. Mr. Singer also serves on the boards of several not-for-profit institutions. He received a B.A. degree from Strayer University and an M.B.A. from Rutgers University. We believe that Mr. Singer is qualified to serve on our board of directors because of his extensive experience in financial matters, including financial reporting, and his experience with our business gained through his tenure as our Chief Financial Officer.
Joseph Benincasa joined our board of directors in June 2005. Mr. Benincasa currently serves as the executive director of The Actors’ Fund of America, a position he has held since 1989. The Actors’ Fund is the leading national, non-profit human services organization providing comprehensive social and health care services, employment, training and housing support to the entertainment profession. For six years, from 2000 to 2006, Mr. Benincasa served as a director of St. Peter’s University Medical Center, a major hospital in northern New Jersey. He also sits on the board of directors of Broadway Cares/Equity Fights AIDS; the National Theatre Workshop of the Handicapped; Career Transition for Dancers; the Times Square Alliance; the New York Society of Association Executives and the Somerset Patriots, a minor league baseball team. Mr. Benincasa holds a B.A. degree from St. Joseph’s University, an M. Ed. Degree from Rutgers University and also attended the Fordham University Graduate School of Business. We believe that Mr. Benincasa is qualified to serve on our board of directors because of his familiarity with healthcare issues gained through his board service at St. Peter’s University Medical Center and his extensive experience with administrative matters.
Harry Elias became a member of the board of directors in March 2004. Mr. Elias commenced his employment in sales and marketing with JVC Company of America (“JVC”), a distributor of audio and video products, in 1967, subsequently being appointed as JVC’s Senior Vice President of Sales and Marketing in 1983 and as Executive Vice President of Sales and Marketing in 1990. In 1995, Mr. Elias was named as JVC’s Chief Operating Officer, a position he occupied until April 2003 when he resigned his positions upon his appointment as JVC’s “Honorable Chairman.” In January 2005, after retiring from JVC, Mr. Elias was appointed Chairman of the Board of and commenced to serve as a consultant to AKAI USA, the sole distributor in the United States of electronic products produced by AKAI, a Chinese manufacturer. Mr. Elias retired from AKAI in 2007 and currently is self-employed as a business consultant. We believe that Mr. Elias is qualified to serve on our board of directors because of the experience and skills he gained in running a large business operation.
Gary Lederman, Esq. became a member of our board of directors in May 1997. He received his B.A. degree from Brooklyn College in 1954 and his J.D. degree from NYU Law School in 1957. He was manager of Locals 370, 491 and 662 of the U.F.C.W. International Union from 1961 to 1985.. During the 1970s, Mr. Lederman also served as a member of the New York Attorney General’s Consumer Fraud Advisory Committee. He is retired from the unions and has been a lecturer at Queensboro Community College in the field of insurance. He served on an institutional review board for RTL, a pharmaceutical drug testing laboratory until his retirement in February 2007. We believe that Mr. Lederman is qualified to serve on our board of directors as a result of his legal expertise, his union manager experience and responsibilities and his experience with RTL, including his involvement with health and welfare funds and his familiarity with consumer regulation and the activities of pharmaceutical companies.
John Roglieri, M.D. became a member of our board of directors in September 1995. He is an Assistant Professor of Clinical Medicine at Columbia University’s College of Physicians and Surgeons and an Assistant Attending Physician at Presbyterian Hospital, New York City. Dr. Roglieri
27
received a B.S. degree in Chemical Engineering and a B.A. degree in Applied Sciences from Lehigh University in 1960, an M.D. degree from Harvard Medical School in 1966, and a Masters degree from Columbia University’s School of Business in 1978. From 1969 until 1971, he was a Senior Assistant Surgeon in the U.S. Public Health Service in Washington, D.C. From 1971 until 1973 he was a Clinical and Research Fellow at Massachusetts General Hospital. From 1973 until 1975, he was director of the Robert Wood Johnson Clinical Scholars program at Columbia University. In 1975 he was appointed Vice-President, Ambulatory Services at Presbyterian Hospital, a position which he held until 1980. Since 1980, he has maintained a private practice of internal medicine at Columbia-Presbyterian Medical Center. From 1988 until 1992, he was also director of the Employee Health Service at Presbyterian Hospital. From 1992 through 1999, Dr. Roglieri was the corporate medical director of NYLCare, a managed care subsidiary of New York Life Insurance Company. Dr. Roglieri was chief medical officer of Physician WebLink, a national physician practice management company, from 1999 to 2000. Since 2001, he has been a medical director for New York Life in Manhattan. He is a member of advisory boards to several pharmaceutical companies, a member of the Editorial Advisory Board of the journals Managed Care and Seminars in Medical Practice. We believe that Dr. Roglieri is qualified to serve on our board of directors due to his extensive medical background, his role as director of the Employee Health service at Presbyterian Hospital, his role as corporate medical director of a managed care organization and the skill and expertise gained through his many other activities.
There are no family relationships between or among any directors or executive officers of Bio-Reference Laboratories.
Board Composition
Director Independence
Our board of directors has determined that each of Messrs. Benincasa, Elias and Lederman and Dr. Roglieri are independent within the applicable rules of the SEC and the NASDAQ Stock Market, and that each of them is also an independent director under Rule 10A-3 of the Exchange Act for the purpose of audit committee membership. In addition, our board has determined that Mr. Lederman is an audit committee financial expert within the meaning of the applicable rules of the SEC and the NASDAQ Stock Market.
Staggered Board
Our Certificate of Incorporation provides for a staggered board of directors. Accordingly, our board is divided into three classes of directors and the members of only one class are elected each year to serve a three-year term. Dr. Grodman and Mr. Dubinett are the Class I directors whose terms expire in fiscal 2013. Mr. Singer and Mr. Elias are the Class II directors whose terms expire in fiscal 2014. Mr. Benincasa, Mr. Lederman and Dr. Roglieri are the Class III directors whose terms expire in fiscal 2015.
Board Leadership Structure and Board’s Role in Risk Oversight
We have always employed a traditional board leadership model, with our Chief Executive Officer also serving as Chairman of our Board of Directors. We believe this traditional leadership structure benefits our company. A combined Chairman/CEO role helps provide strong, unified leadership for our management team and Board of Directors. Our clients, stockholders and other business partners have always viewed our Chairman/CEO as a visionary leader in our industry, and we believe that having a single leader for the company is good for our business. Accordingly, we believe a combined Chairman/CEO position is the best governance model for our company and our stockholders.
Management is responsible for the day-to-day management of risks we face, while our board of directors, as a whole and through its committees, has responsibility for the oversight of risk management. In its risk management role, our board of directors has the responsibility to satisfy itself that the risk management processes designed and implemented by management are adequate and functioning as designed.
The board of directors’ role in overseeing the management of risk we face is conducted primarily through its committees, as discussed in the description of each committee below and as specified in each committee’s respective charter. The board of directors (or the appropriate board committee in the case of risks that are under the purview of a particular committee) discusses with management potential risk exposures, their potential impact on our company and the steps we take to manage them. When a board committee is responsible for evaluating and overseeing the management of a particular risk or risks, the committee will report such matters to the full board. This enables the board of directors and its committees to coordinate the risk oversight role, particularly with respect to risk interrelationships.
Board Meetings and Committees
Our board of directors met four times during our fiscal year ended October 31, 2012. Our board of directors has established the following committees—an audit committee, a compensation committee and a nominating committee. The audit committee met four times during fiscal 2012. The compensation committee met once during fiscal 2012. The nominating committee did not meet during fiscal 2012. During fiscal 2012, each director attended at least 75% of the meetings of the board of directors and committees on which such director served. Each of the committees of our board of directors acts in accordance with a written charter adopted by our board of directors.
Audit Committee
Our audit committee is comprised of Gary Lederman (Chairman), Joseph Benincasa, Harry Elias and John Roglieri. The audit committee meets at least once a year with the outside auditors with respect to, and shall advise the board of directors in, matters relating to the corporations reporting practices, its application of accounting principals and its internal controls. The outside auditors are accountable to the board of directors and the audit committee and the board of directors and the audit committee have the authority and responsibility to select, evaluate, and where appropriate, replace the outside auditors or to nominate the outside auditors to be proposed for shareholder approval in any proxy statement. The audit committee shall be directly responsible for the appointment, compensation, retention and oversight of the work of any registered public accounting firm engaged for the purpose of preparing or issuing an audit report or performing other audit, review or attest services for us. The audit committee shall be directly responsible for the resolution of disagreements between our management and the outside auditors regarding financial reporting.
Compensation Committee
Our compensation committee is comprised of John Roglieri (Chairman), Joseph Benincasa, Harry Elias and Gary Lederman. The compensation committee oversees the compensation policies and their specific application to our executive officers; prepares an annual report on executive compensation for inclusion in our Annual Report and/or proxy statement, The compensation committee negotiates and approves the
28
compensation of our chief executive officer and our other executive officers; selects a peer group of companies against which to compare our compensation of our chief executive officer; monitor compensation trends and solicit independent advice when deemed appropriate; and approve, reject or modify incentive bonus compensation plans for our senior management, as recommended by management.
From time to time our compensation committee may determine to engage an independent compensation consultant to assist it in reviewing the compensation levels for our executive officers. Starting in fiscal 2010 and continuing into fiscal 2012 the compensation committee engaged Compensation Resources, Inc. as its independent compensation consultant in connection with the negotiation of the new employment agreement with our chief executive officer.
Nominating Committee
Our nominating committee is comprised of Harry Elias, Joseph Benincasa, Gary Lederman and John Roglieri (Chairman). The nominating committee establishes criteria for the selection of directors; identifies individuals qualified to be directors; evaluates director candidates proposed by stockholders; recommends individuals to fill vacancies on the board; and recommends nominees for director at each annual stockholder meeting. The nominating committee considers nominees recommended by stockholders in accordance with the procedures set forth in our by-laws and applicable law. The nominating committee generally identifies potential candidates for director by seeking referrals from management, members of the board of directors and other business contacts. Candidates are evaluated based upon factors such as independence, knowledge, judgment, integrity, character, leadership, skills, education, experience, financial literacy, standing in the community and ability to foster a diversity of backgrounds and views and to complement the board’s existing strengths. There are no differences in the manner in which the nominating committee evaluates nominees for director based on whether the nominee is recommended by a stockholder. The nominating committee seeks to create a board of directors that is strong in its collective knowledge and has a diversity of skills and experience and diversity of backgrounds. The nominating committee assesses the effectiveness of its diversity policies by annually reviewing the nominees for director to our board of directors to determine if such nominees satisfy our then-current needs.
Code of Ethics
Our Code of Ethics is applicable to our senior management, as well as our key financial and accounting personnel. It has been designed to deter wrongdoing and to promote:
honest and ethical conduct including the ethical handling of actual or apparent conflicts of interest;
fair, accurate, timely and understandable disclosure in our public communications and reports filed with the SEC;
compliance with applicable governmental laws, rules and regulations;
prompt internal reporting of violations of the Code to an appropriate person or persons identified in the Code; and
accountability to ensure adherence to the Code.
The Code requires each covered person to deal ethically and honestly with the company and to avoid business, financial or other direct or indirect interests or relationships that conflict with those of the company or divide the covered person’s loyalty to the company. Each covered person is required to sign an attestation of compliance with the Code at the end of each fiscal year.
Compliance with Section 16(a) of the Exchange Act
Based solely on a review of Forms 3 and 4 and any amendments thereto furnished to us pursuant to Rule 16a-3(e) under the Exchange Act, or representations that no Forms 5 were required, we believe that with respect to fiscal 2012, our officers, directors and beneficial owners of more than 10% of our equity timely complied with all applicable Section 16(a) filing requirements, except as follows:
1. Dr. Grodman owns a total of 2,752,200 shares of our common stock. His Section 16 filings report ownership of a total of 2,752,800 shares, a discrepancy of 600 shares.
2. Mr. Elias made late Form 4 filings with respect to his purchase and subsequent sale of 2,000 shares. Upon demand made by us, Mr. Elias promptly disgorged to us the applicable short-swing profits.
29
Item 11. – Executive Compensation
The table below summarizes the total compensation paid or accrued by us with respect to the fiscal years ended October 31, 2010, 2011 and 2012 to our named executive officers (“NEOs”). Our NEOs for fiscal 2012 are Marc D. Goodman, our President and Chief Executive Officer; Howard Dubinett, our Executive Vice President and Chief Operating Officer; and Sam Singer, our Senior Vice President and Chief Financial Officer. This table does not include any amount for our group life, health, hospitalization or medical reimbursement plans, if any, as such benefits do not discriminate in scope, terms or operation, in favor of any or our officers, senior management members or directors, and are generally available to all salaried employees.
SUMMARY COMPENSATION TABLE
Name and
Principal
Position | | Fiscal
Year | | Salary($) | | Bonus
($)(1) | | Stock
Awards($) | | Option
Awards($) | | Non-Equity
Incentive Plan
Compensation
($)(2) | | Change in
Pension Value
and
Nonqualified
Deferred
Compensation
Earnings ($) | | All Other
Compensation
($)(3) | | Total($) | |
Marc D. Grodman | | 2012 | | 1,092,933 | | 70,000 | | 0 | | 0 | | 131,152 | | 0 | | 245,359 | | 1,539,444 | |
M.D., President and Chief | | 2011 | | 1,059,044 | | 1,321,241 | | 0 | | 0 | | 63,543 | | 0 | | 229,638 | | 2,673,466 | |
Executive Officer | | 2010 | | 1,013,439 | | 0 | | 0 | | 0 | | 60,806 | | 0 | | 113,491 | | 1,187,736 | |
| | | | | | | | | | | | | | | | | | | |
Howard Dubinett, | | 2012 | | 431,911 | | 100,000 | | 0 | | 0 | | 51,829 | | 0 | | 42,474 | | 626,214 | |
Executive Vice President and Chief | | 2011 | | 418,518 | | 0 | | 0 | | 0 | | 25,111 | | 0 | | 45,044 | | 488,673 | |
Operating Officer | | 2010 | | 400,496 | | 0 | | 0 | | 0 | | 24,030 | | 0 | | 42,014 | | 466,540 | |
| | | | | | | | | | | | | | | | | | | |
Sam Singer, Senior Vice | | 2012 | | 431,911 | | 300,000 | | 0 | | 0 | | 51,829 | | 0 | | 48,998 | | 832,738 | |
President and Chief | | 2011 | | 418,518 | | 110,000 | | 0 | | 0 | | 25,111 | | 0 | | 45,087 | | 598,716 | |
Financial Officer | | 2010 | | 400,496 | | 0 | | 0 | | 0 | | 24,030 | | 0 | | 40,240 | | 464,766 | |
(1) The amounts shown in this column for fiscal 2012 represent (i) with respect to Dr. Grodman, a cash bonus of $70,000 paid in connection with his payment of the premium costs for an insurance policy owned by the Company insuring the life of Dr. Grodman pursuant to an Endorsement Split-Dollar Insurance Agreement among the Company, Dr. Grodman and an Insurance Trust established by Dr. Goodman (“Premium Payments”); and (ii) with respect to Mr. Singer and Mr. Dubinett, a one-time cash bonus for their entering into new employment contracts during the year. The amounts shown in this column for fiscal 2011 represent (i) with respect to Dr. Grodman, cash bonuses of $1,202,241 and $119,000 paid in connection with his payment of Premium Payments; and (ii) with respect to Mr. Singer, a one-time cash bonus for his activity in the collection of $6.7 million sales tax refund from the State of New Jersey.
(2) The amounts shown in this column represent amounts earned under the Senior Management Incentive Bonus Plan adopted by the Compensation Committee for the applicable fiscal year.
(3) The amounts in the “All Other Compensation” column for fiscal 2012 are detailed below.
Name | | Personal Use of
Company Leased
Automobile ($)(a) | | Personal Use of
Company Airplane
($) (a) | | Life Insurance
Premium ($)(b) | | 401(k) Plan
Contribution ($) | | Total ($) | |
Marc D. Grodman | | 23,984 | | 20,375 | | 200,000 | | 1,000 | | 245,359 | |
Howard Dubinett | | 16,474 | | 0 | | 25,000 | | 1,000 | | 42,474 | |
Sam Singer | | 20,918 | | 2,080 | | 25,000 | | 1,000 | | 48,998 | |
(a) Represents our aggregate incremental costs for personal use of a Company leased automobile or the Company’s aircraft, as applicable.
(b) See “Split Dollar Life Insurance” below.
30
GRANTS OF PLAN-BASED AWARDS
This table provides information regarding awards granted to our NEOs under the 2012 Senior Management Incentive Bonus Plan.
| | Estimated Future Payouts Under Non-Equity Incentive Plan
Awards (1) | |
Name | | Threshold ($) | | Maximum ($) | |
Marc D. Grodman M.D. | | 43,717 | | 273,233 | |
| | | | | |
Howard Dubinett | | 17,276 | | 107,978 | |
| | | | | |
Sam Singer | | 17,276 | | 107,978 | |
(1) The amounts represent the range of annual cash incentive awards the NEO was potentially entitled to receive based on the achievement of the performance goals for fiscal 2012 under the 2012 Senior Management Incentive Bonus Plan. These cash incentive awards were granted with no specified target level, as defined under SEC Regulation S-K, rule 402(d).
Employment Agreements with NEOs
Dr. Grodman
On December 31, 2010, the Company executed an employment agreement with Dr. Grodman (the “Grodman Contract”), employing him as President and Chief Executive Officer through October 31, 2017. The Grodman Contract is automatically renewable for one additional two year period subject to the right of either party to elect not to renew at least four months prior thereto. The Grodman Contract provides Dr. Grodman with a minimum annual base compensation of $1,059,044, subject to annual percentage increases based on the Consumer Price Index as well as to increases at the discretion of the Compensation Committee. Dr. Grodman’s minimum annual base compensation for fiscal 2011 as determined by the Compensation Committee was $1,059,044 and for fiscal 2012 is $1,092,933. Under the Grodman Contract we agreed to lease and insure an automobile for his benefit and agreed to provide him with access for personal use our airplane, which use will be taxable to him. The Grodman Contract also provides Dr. Grodman with participation rights in any fringe benefit and bonus plans available to the Company’s employees to the extent determined by the Compensation Committee. The Grodman Contract provides that in the event of Dr. Grodman’s total disability we may continue to employ him and compensate him at his then current base compensation for the month the disability occurs and a period of 36 months thereafter followed by an unpaid 3 month period, following which his employment will terminate unless we grant an additional leave of absence. If Dr. Grodman incurs a partial disability then his base compensation will be equitably adjusted based on the time he is able to devote to the Company. In the event of Dr. Grodman’s termination due to his death, the Company will pay his estate a death benefit equal to 24 times his monthly base compensation in effect at the date of his death, paid over 24 months. Under the Grodman Contract we may terminate Dr. Grodman’s employment for “Cause” and Dr. Grodman has the right to terminate his employment for “Good Reason”. If he terminates for Good Reason he will be entitled to continuation of his base compensation and employee benefits through the end of the period he otherwise would have been employed under the Grodman Contract.
“Cause” is defined in the Grodman Contact to mean: any act or acts of dishonesty by Dr. Grodman constituting criminal acts resulting or intending to result directly or indirectly in his gain or personal enrichment at our expense; his commission of a crime involving fraud, embezzlement or theft; or his material breach of the Grodman Contract. “Good Reason” is defined in the Grodman Contract to mean: a material diminution of Dr. Grodman’s base compensation; a material diminution in his authority, duties or responsibilities; a material diminution of the authority, duties or responsibilities of any supervisor he reports to; a material diminution in the budget over which he retains authority; a material change in the geographic location at which he provides services; or any other action or inaction that constitutes a material breach by us of the Grodman Contract.
In the event of a Change in Control of the Company, Dr. Grodman can elect to terminate his employment by providing written notice within 30 days following the Change in Control, with a termination date effective at the earlier of 45 days after the Change in Control or the next to last day of the calendar year in which the Change in Control occurs. In that event, he will be entitled to be paid a lump sum severance payment equal to 2.99 times the average of the annual compensation paid to him by the Company for the five calendar years preceding the earlier of the calendar year in which the Change of Control occurred or the calendar year of the date of termination, reduced by the amount of any other payment or the value of any other benefit received or to be received by him in connection with the termination of his employment or contingent on a Change in Control that are not deductible by us pursuant to Section 280G of the Internal Revenue Code of 1986, as amended (the “Tax Code”). “Change in Control” is defined in the Grodman Contact to mean a “change in effective control” or a “change in the ownership of a substantial portion of a corporation’s assets” as such terms are defined under Section 409A of the Tax Code, and means either the acquisition within 12 months by a person or group of ownership of 30% or more of the total voting power of our stock; the replacement of a majority of the member’s of our Board of Directors during any 12 month period by directors not endorsed prior to their appointment or election by a majority of the Board of Directors; or the acquisition by a person or group within 12 months of our assets with a total gross fair market value equal to more than 40% of the total gross fair market value of our assets prior to such acquisition.
Dr. Grodman is also subject to certain non-competition restrictions preventing him from competing with the Company after termination of his employment. Such restrictions will run for one year from the date of his termination, other than following a termination by him for Good Reason in which case they will continue until the greater of one year from the date of termination or ½ of the period remaining from the date of termination through October 31, 2017.
Pursuant to the Grodman Contract, the Company agreed to transfer to an Insurance Trust (the “1999 Trust”) established by Dr. Grodman, an insurance policy (“Policy A”) owned by the Company insuring the life of Dr. Grodman pursuant to an Endorsement Split-Dollar Insurance Agreement (“Split-Dollar Agreement No. 1”) among the Company, Dr. Grodman and the 1999 Trust, by paying a $1,202,411 bonus (the “Initial Bonus”) to Dr. Grodman, which is equal to the amount of the premiums paid by the Company on Policy A through the date of the Grodman Contract. Split-Dollar Agreement No. 1 required the Company to pay the annual premiums on Policy A and provided that in the event of Dr. Grodman’s death while serving as a full time Company employee, the Company would receive that amount out of the policy death proceeds equal to its “interest in the policy” (i.e. the greater of the premiums it had paid on the policy or the policy cash value at the date of death) and the balance of the death proceeds would be paid to
31
Dr. Grodman’s designated beneficiaries. Pursuant to the Grodman Contract, Split-Dollar Agreement No. 1 was terminated and in a “book entry” transaction, the Initial Bonus was “paid” to Dr. Grodman who in turn “transferred” the Initial Bonus amount to the 1999 Trust which in turn “repaid” the Initial Bonus amount back to the Company. The Company then, in accordance with Split-Dollar Agreement No. 1, transferred ownership of Policy A to the 1999 Trust. To facilitate these transactions, the parties agreed that the actual monetary funds did not need to change hands but agreed to treat the transactions appropriately for tax and accounting purposes. The Company also agreed to pay bonuses to Dr. Grodman of $119,000 in 2011, $70,000 in 2012 and $70,000 in 2013 unless his employment was terminated for “Cause” prior to a payment. These three bonuses were equal in amount to the remaining premiums payable on Policy A. The Company will expense the Initial Bonus ratably over the term of the New Contract. If Dr. Grodman’s employment is terminated for “Cause”, he is obligated to pay back the unexpended portion of the Initial Bonus back to the Company.
The Company also agreed to obtain a second insurance policy, a second-to-die policy (“Policy B”) insuring the lives of Dr. Grodman and his wife. Policy B will be owned by the Company pursuant to a second Endorsement Split-Dollar Insurance Agreement (“Split-Dollar Agreement No. 2”) among the Company, Dr. Grodman and an Insurance Trust established by Dr. Grodman. Policy B provides for seven years of annual premiums of approximately $200,000 each, to be paid by the Company unless Dr. Grodman’s employment is terminated for “Cause.” At Dr. Grodman’s death, if his wife survives him, or in the event his employment is terminated for “Cause”, Dr. Grodman’s estate or Dr. Grodman, as the case may be, will cause the premiums paid by the Company under Policy B up to said date, to be paid back to the Company and the Company will transfer ownership of Policy B to Dr. Grodman’s estate, or to Dr. Grodman, as the case may be. If Dr. Grodman survives his wife, and assuming his employment has not been terminated for “Cause,” at his death, the Company will be paid the greater of the premiums it paid on Policy B or the Policy B cash value out of the death proceeds and Dr. Grodman’s estate will be paid the balance of the death proceeds, provided, however, that if Dr. Grodman survives his wife and assuming his employment has not been terminated for “Cause,” at his wife’s death, Dr Grodman or his designee shall have the option, exercisable within 90 days of her death, to purchase Policy B from the Company for the greater of the premiums paid or the cash value at the date of her death.
Mr. Singer
On June 14, 2012, effective February 1, 2012, the Company executed a new employment agreement with Mr. Singer (the “Singer Contract”), employing him as Senior Vice President, Chief Financial Officer and Chief Accounting Officer through January 31, 2015. The Singer Contract replaced Mr. Singer’s employment agreement that expired January 31, 2012. Mr. Singer’s minimum annual base compensation under the Singer Contract is $431,911 subject to increases based on increases in the Consumer Price Index as well as to increases at the discretion of the Compensation Committee. The Singer Contract provides for the leasing of an automobile for his use and participation in fringe benefit, bonus, pension, profit sharing, and similar plans maintained for the Company’s employees. In consideration for his entering into the Singer Contract, the company paid Mr. Singer a sign-on bonus in the amount of $300,000 subject to a pro rata claw-back provision in the event Mr. Singer is terminated for “cause” or if he resigns prior to the earlier of a “change of control” or January 31, 2015. In the event of Mr. Singer’s total disability we may continue to employ him and compensate him at his then current base compensation for the month the disability occurs and a period of 12 months thereafter followed by an unpaid 3 month period, following which his employment will terminate unless we grant an additional leave of absence. If Mr. Singer incurs a partial disability then his base compensation will be equitably adjusted based on the time he is able to devote to the Company. In the event of Mr. Singer’s termination due to his death, we will continue to pay his beneficiary his base salary for 12 months. Under the Singer Contract we may terminate Mr. Singer’s employment for “Cause” and Mr. Singer has the right to terminate for “Good Reason”. If he terminates for Good Reason he will be entitled, subject to his execution of a release, to continuation of his base compensation and employee benefits through the end of the employment period he otherwise would have been employed under his employment agreement. In the event of termination due to a Change in Control of the Company, Mr. Singer will be entitled to the same severance payment described above for Dr. Grodman. Mr. Singer’s agreement does not contain non-competition restrictions.
“Cause” is defined in Mr. Singer’s employment agreement to mean: an act or acts of dishonesty by Mr. Singer constituting criminal acts resulting or intended to result directly or indirectly in his gain or personal enrichment at our expense; his commission of a crime involving fraud, embezzlement or theft against us; or his engaging in competition with us. Good Reason and Change in Control under Mr. Singer’s employment agreement has the same meanings as provided in the Grodman Contract.
Mr. Dubinett
On June 14, 2012, effective February 1, 2012 the Company executed an employment agreement with Mr. Dubinett’s (the “Dubinett Contract”), employing him as Executive Vice President and Chief Operating Officer through January 31, 2015. The Dubinett Contract replaced Mr. Dubinett’s employment agreement with us that expired on October 31, 2011. The Dubinett Contract is substantially identical with the Singer Contract except that Mr. Dubinett’s sign-on bonus was $100,000.
32
Potential Payments Upon Termination or Change in Control as of October 31, 2012.
The following table sets out the estimated payments that would have been paid to each of our NEOs upon termination of employment due to Death, for Good Reason or following a Change in Control in accordance with their employment agreements as described above as in effect, and in each case assuming such termination had occurred, as of October 31, 2012. We have calculated these estimated payments to meet SEC disclosure requirements. The estimated payments are not necessarily indicative of the actual amounts any of our NEOs would receive in such circumstances. The table excludes compensation amounts accrued through October 31, 2012 that would be paid in the normal course of continued employment, such as accrued but unpaid base compensation, and vested account balances under our retirement plans that are generally available to all of our salaried employees.
| | Base Compensation
Continuation/ Lump
Sum ($) (a) | | Benefits Continuation ($)
(b) | | Total ($) | |
Marc D. Grodman M.D. | | | | | | | |
Good Reason | | 5,464,665 | | 25,610 | | 5,490,275 | |
Death | | 2,185,866 | | 0 | | 2,185,866 | |
Change in Control | | 3,660,825 | | 0 | | 3,660,825 | |
Howard Dubinett | | | | | | | |
Good Reason | | 971,800 | | 10,764 | | 982,564 | |
Death | | 431,911 | | 0 | | 431,911 | |
Change in Control | | 1,129,584 | | 0 | | 1,129,584 | |
Sam Singer | | | | | | | |
Good Reason | | 971.800 | | 10,764 | | 982,564 | |
Death | | 431,911 | | 0 | | 431,911 | |
Change in Control | | 1,129,584 | | 0 | | 1,129,584 | |
(a) For a Good Reason termination this payment reflects a continuation of base compensation through the end of period the NEO otherwise would have been employed under his employment agreement. For death this payment reflects a continuation of base compensation for 24 months in the case of Dr. Grodman and 12 months in the case of Messrs. Dubinett and Singer. For Change in Control this payment reflects an amount equal to 2.99 times the NEOs five-year average compensation, without reduction.
(b) For a Good Reason termination this payment reflects our estimated costs for a continuation of the NEOs benefits under our medical plan through the end of period the NEO otherwise would have been employed under his employment agreement.
Split-Dollar Life Insurance
We have established split-dollar life insurance programs for each of our NEOs under which we are entitled to receive the net cash surrender value of the policies. We have entered into Endorsement Split-Dollar Life Insurance Agreements with each of the NEOs pursuant to which we have agreed to continue to pay the annual premiums on the policies during the period of the NEO’s full-time employment by the Company ($200,000 under Dr. Grodman’s policy and $25,000 each under Messrs. Dubinett’s and Singer’s policies). In the case of Dr. Grodman, the insurance policy is a second-to-die policy on the lives of Dr. Grodman and his wife. In the event of an NEO’s death while serving as a full-time employee of the Company, we will be entitled to receive that amount of the death proceeds equal to our interest in the policy (the aggregate amount of premiums paid by the Company with respect to the policy less the amount of any loans, if any, from the Insurer to the Company against the cash value or policy proceeds, and less the aggregate amount of any premiums paid by the NEO to the Company in reimbursement of premiums paid by the Company) and the balance of the death proceeds will be paid to the NEO’s designated beneficiaries. The premiums paid by the Company on such policies are approximately $250,000 at October 31, 2012. As of such date the aggregate net cash surrender value of the three policies was approximately $866,000 and is recorded on the books of the Company at such value.
Stock Options
See Note 11 of Notes to the Consolidated Financial Statements for information on the company’s stock option plans.
Option Grants to Our NEOs in Last Fiscal Year
No options to purchase shares of our Common Stock were granted to any of our NEOs in fiscal 2012.
Option Exercises and Stock Vested
At October 31, 2012, there were no outstanding options held by our NEOs or any of our directors. During fiscal 2012 no options were exercised by any member of the Board of Directors.
Director Compensation
During fiscal 2012, each director who was not a Company employee was compensated for his services as a director with a quarterly fee of $16,250. In addition, Gary Lederman as chairman of the Audit Committee and John Roglieri M.D. as chairman of the Compensation Committee were each compensated for serving as a Committee Chairman with an additional quarterly fee of $3,750. No director’s fees were paid to our employee directors.
33
The following table sets forth the compensation paid to our directors in fiscal 2012.
Fiscal 2012
Director Name: | | Fees Earned or paid in
Cash ($) | | Chairman Fees ($) | | Other | | Total ($) | |
Joseph Benincasa | | 65,000 | | — | | — | | 65,000 | |
Harry Elias | | 65,000 | | — | | — | | 65,000 | |
Gary Lederman (a) | | 65,000 | | 15,000 | (a) | — | | 80,000 | |
John Roglieri M.D (b) | | 65,000 | | 15,000 | (b) | — | | 80,000 | |
(a) Chairman of the Audit Committee
(b) Chairman of the Compensation Committee
Compensation Discussion and Analysis
Executive Compensation Philosophy
The objective of our compensation program for our NEOs is to reward them for their leadership and efficiency in their areas of responsibility and for their overall contribution to the Company’s performance. Our NEOs for fiscal 2012 are Dr. Grodman, our President and Chief Executive officer, Mr. Dubinett, our Executive Vice President Chief Operating officer who is responsible for healthcare regulatory compliance and insurance matters, and Mr. Singer, our Senior Vice President and Chief Financial Officer who is responsible for all financial matters.
We seek to maintain a uniform approach in how we compensate our NEOs. Accordingly, as Dr. Grodman already owns a substantial equity interest in the Company and we believe that further equity compensation would not provide him with an effective incentive, we do not currently provide equity compensation to any of our NEOs. Our compensation program for our NEOs therefore focuses primarily on the following cash based incentives:
(i) Annual base compensation consisting of a set annual cash amount that is subject to annual increase based upon a review of the NEO’s and the Company’s performance and increases in the Consumer Price Index; and
(ii) Participation in the annual Senior Management Incentive Bonus Plan (“Annual Bonus Plan”), which provides cash incentives based on the level of achievement of specific performance objectives. We annually establish targets under the Annual Bonus Plan that are designed to assist in the Company’s profitability by encouraging a “team effort” that rewards participants based on the level of achievement of Company financial targets set by the Compensation Committee with no reward if minimum targets are not achieved. Annual Bonus Plan targets were achieved with respect to fiscal 2010, fiscal 2011 and 2012 so that bonuses were earned and paid to our NEOs under the Annual Bonus Plan for fiscal 2010, the Annual Bonus Plan for fiscal 2011 (the “2011 Bonus Plan”) and the Annual Bonus Plan for fiscal 2012 (the “2012 Bonus Plan”). See “Senior Management Incentive Bonus Plan” herein.
Process for Determining Executive Compensation
Our Compensation Committee reviews and approves the annual base compensation and other compensation of our NEOs. Our Compensation Committee also establishes and reviews the achievement of performance goals and other matters relating to the Annual Bonus Plans.
Mr. Dubinett and Mr. Singer each negotiated the terms of their new contracts including their base compensation with Dr. Grodman who then recommended the terms to the Compensation Committee which approved our entering into the contracts.
In connection with its review of NEO compensation in fiscal 2012, including the new contracts for Messrs. Singer and Dubinett, the Compensation Committee considered an executive compensation study furnished by Compensation Resources, Inc., an independent executive compensation consulting firm (“CRI”) engaged by the Compensation Committee. After taking into account the compensation paid to similar executive officers of a peer group of eleven publicly owned clinical testing laboratories (including the two major national laboratories, Quest Diagnostics, Inc. and Laboratory Corp. of America Holdings), CRI concluded that Dr. Grodman’s total direct compensation was then above the total direct compensation provided to the chief executive officers in the peer group, and that the total direct compensation provided to Messrs. Singer and Dubinett were below the total direct compensation provided to similar executive officers in the peer group. Notwithstanding the report, the Compensation Committee believes that Dr. Grodman’s compensation level is reasonable as the current levels were determined based on a CRI report for fiscal 2011 which showed that Dr. Grodman’s total direct compensation was 20% below the peer group.
For 2012, CRI selected the following eleven peer group publicly owned clinical testing laboratories to be used as a benchmark, most of which generally have revenue in a range of ½ to 2 times that of the Company, but was expanded to include companies with revenues of up to $8 billion:
Alliance Healthcare Services, Inc.
Bioclinica Inc.
Enzo Biochem Inc.
eResearch Technology
Laboratory CP of Amer Hldgs
Medtox Scientific Inc.
Neogenomics Inc.
Psychemedics Corp.
Quest Diagnostics Inc.
Radnet Inc.
Response Genetics Inc.
34
Two companies that were part of the 2011 peer group, Genoptix Inc. and Orchid Cellmark Inc., were excluded for fiscal 2012 as they no longer met the peer group criteria and were replaced by Alliance Healthcare Services, Inc., Enzo Biochem Inc., eResearch Technology, and Radnet Inc.
New Contracts for Messrs. Singer and Dubinett
The Compensation Committee believes that each of Messrs. Singer and Dubinett skills and knowledge of our business and industry are critical to our long term planning and success. Therefore, to ensure their long-term retention with the Company, in fiscal 2012 we entered into new contracts with Messrs. Singer and Dubinett that run through January 31, 2015. These contracts replaced our prior method of entering into short-term contract extension with them. Based on the CRI report and other factors considered by the Compensation Committee, we believe that the new contracts are reasonable and better align their compensation with those of similar executive officers within our peer group. See “Employment Agreements with NEOs” above for a summary of the terms of the new contracts.
Base Compensation
In accordance with the Grodman Contract, the Compensation Committee determined that Dr. Grodman’s base compensation be increased to $1,092,933 for fiscal 2012, which reflects a 3% increase considered the Company’s increase based on increases in the Consumer Price Index.
Since fiscal 2008, the base compensation and the increase in base compensation in each year for Mr. Dubinett and for Mr. Singer have been identical. This is because the Compensation Committee continues to believe that Mr. Dubinett and Mr. Singer perform their duties equally well and to distinguish between them in compensation could cause the Company to lose the services of one of them. The increases in their base compensation in each of the past three fiscal years have been as follows, which reflect annual increases for each fiscal year based on increases in the Consumer Price Index.
Increases in Base Compensation for Each of
Mr. Dubinett and Mr. Singer Over the Prior Three Fiscal Years
Period | | Amount ($) | | Percentage Increase | |
Fiscal 2010 | | 19,075 | | 5 | % |
Fiscal 2011 | | 18,022 | | 4 | % |
Fiscal 2012 | | 13,393 | | 3 | % |
Benefits
Our policy is to provide health benefits as well as access to our 401(k) Plan to which we contribute a maximum of $1,000 per employee each year, to all of our employees including our NEOs.
All senior officers of the Company, including our NEOs, are entitled to an automobile leased by the Company and access to the Company’s airplane for personal use to the extent the airplane is not in use for business purposes. The costs for insurance and maintenance of such automobiles are paid by the Company. All amounts reflecting the personal use of such perquisites are reported as income to them subject to tax in accordance with the Tax Code. The amounts reflecting the Company’s incremental costs for the NEO’s personal use of the Company leased automobile and the Company’s airplane are reflected in Footnote (3) to the “Summary Compensation Table” below.
Change in Control Benefits
The employment agreements with our NEOs provide for substantial severance payments to them in the event of a change in control of the Company. This provision provides an additional level of financial security for our NEOs as they may be asked to evaluate a transaction purportedly expected to maximize shareholder value while resulting in the elimination of their jobs. The severance payment provision (2.99 times the annual average of the preceding five years of compensation) is designed to minimize the distraction caused by concerns over personal financial security in the context of a proposed change in control.
Annual Bonus Plans for fiscal years 2011 and 2012.
The Compensation Committee adopts an Annual Bonus Plans for each year which it believes incentivizes senior management to push to achieve operating results that the Compensation Committee believes will inure to the benefit of stockholders as well as management. Each Annual Bonus Plan provides goals which the Compensation Committee believes could only be achieved through extraordinary team efforts by senior management and that are designed to incentivize senior management to operate the Company in the most efficient manner possible. In developing the Annual Bonus Plan for each year, the Compensation Committee takes into consideration the economy in general and the goals of the Company that it wished to reward, namely to improve Company margins within attainable goals for management.
The Compensation Committee has at all times sought (and continues to seek) to provide a mechanism to reward outstanding efforts that enhance shareholder value. The following is a description of the Annual Bonus Plan for fiscal 2011 (the “2011 Bonus Plan”) and fiscal 2012 (the “2012 Bonus Plan”). The Compensation Committee has adopted an Annual Bonus Plan for fiscal 2013 that is substantially similar to the 2012 Bonus Plan other than will respect to the actual levels of the performance metrics to be achieved. Any bonuses required to be paid under the provision of any Annual Bonus Plan is required to be paid to each participant on the pro-rata formula established upon the adoption of the plan and not at the discretion of the Compensation Committee.
2012 Bonus Plan
The 2012 Bonus Plan was based on two separate financial formula calculations. The first formula provided for bonuses (up to a maximum of 10% of the participant’s annual gross wages for 2012, less any bonus, auto or airplane usage expense charge-back or other unearned revenue (“2012 Wages”)) based on the level of the Company’s achievement of total operating income (TOI) as a percentage of our net revenues for fiscal 2012 as follows:
35
If TOI is greater than or equal to: | | and less than: | | Bonus equal to the following
percentage of the participant’s
2012 wages: | |
11.00 | % | 11.50 | % | 4 | % |
11.50 | % | 12.00 | % | 6 | % |
12.00 | % | 12.50 | % | 8 | % |
12.50 | % | N/A | | 10 | % |
The second formula provided for bonuses (up to a maximum of 15% of the participant’s 2012 Wages ) based on the percentage increase on a year over year basis in the Company’s operating income before interest and taxes (“OIBIT”) from fiscal 2011 to fiscal 2012, determined by subtracting the Company’s fiscal 2011 OIBIT from the Company’s fiscal 2012 OIBIT and dividing the difference by the Company’s OIBIT for fiscal 2011 to determine the percentage of change (“2012 PC”), as follows:
If 2012 PC is greater than: | | and less than: | | Bonus equal to the following
percentage of the participant’s
2012 Wages: | |
25.00 | % | 30.00 | % | 6 | % |
30.00 | % | 35.00 | % | 9 | % |
35.00 | % | 40.00 | % | 12 | % |
40.00 | % | N/A | | 15 | % |
Actual results under the 2012 Bonus Plan were as follows:
| | | | Bonus equal to the following percentage of the
participant’s 2012 Wages: | |
TOI as a percentage of our net revenues for fiscal 2012 | | 11.51 | % | 6 | % |
2010 PC | | 27.36 | % | 6 | % |
Total Bonus Percentage: | | — | | 12 | % |
2011 Bonus Plan
The 2011 Bonus Plan was based on two separate financial formula calculations. The first formula provided for bonuses (up to a maximum of 10% of the participant’s annual gross wages for 2011, less any bonus, auto or airplane usage expense charge-back or other unearned revenue (“2011 Wages”)) based on the level of the Company’s achievement of TOI as a percentage of our net revenues for fiscal 2011 as follows:
If TOI is greater than or equal
to: | | and less than: | | Bonus equal to the following
percentage of the participant’s
2011 Wages: | |
11.00 | % | 11.50 | % | 4 | % |
11.50 | % | 12.00 | % | 6 | % |
12.00 | % | 12.50 | % | 8 | % |
12.50 | % | N/A | | 10 | % |
The second formula provided for bonuses (up to a maximum of 15% of the participant’s 2011 Wages) based on the percentage increase on a year over year basis in the Company’s OIBIT from fiscal 2010 to fiscal 2011, determined by subtracting the Company’s fiscal 2010 OIBIT from the Company’s fiscal 2011 OIBIT and dividing the difference by the Company’s OIBIT for fiscal 2010 to determine the percentage of change (“2011 PC”), as follows:
If 2011 PC is greater than or
equal to: | | and less than: | | Bonus equal to the following
percentage of the participant’s
2011 Wages: | |
20 | % | 25 | % | 6 | % |
25 | % | 30 | % | 9 | % |
30 | % | 35 | % | 12 | % |
35 | % | N/A | | 15 | % |
Actual results under the 2011 Bonus Plan were as follows:
| | | | Bonus equal to the following percentage of the
participant’s 2011 Wages: | |
TOI as a percentage of our net revenues for fiscal 2011 | | 10.70 | % | 0 | % |
2011 PC | | 23.56 | % | 6 | % |
Total Bonus Percentage: | | — | | 6 | % |
See Item 11 — the “Summary Compensation Table”, column (g) “Non-Equity Incentive Plan Compensation” as to the bonuses paid under the Senior Management Incentive Compensation Plan with respect to fiscal 2012, 2011 and 2010.
36
Tax Compliance Policy
Section 162(m) of the Code generally disallows a tax deduction to public corporations for compensation in excess of $1,000,000 paid for any fiscal year to a corporation’s chief executive officer and to the three other most highly compensated executive officers in office as of the end of the fiscal year, other than the chief financial officer. The statute exempts qualifying performance-based compensation from the deduction limit if certain requirements are met. However, shareholder interests may at times be best served by not restricting the Compensation Committee’s discretion and flexibility in developing compensation programs, even though the programs may result in non-deductible compensation expenses. Accordingly, the Compensation Committee may from time to time approve elements of compensation for certain officers that are not fully deductible.
Compensation Committee Interlocks and Insider Participation
During fiscal 2012, the members of the Company’s Compensation Committee were:
John Roglieri M.D. — Chairman
Joseph Benincasa
Harry Elias
Gary Lederman
No member of the Compensation Committee was an officer or employee of the Company in fiscal 2012 or was formerly an officer of the Company.
Compensation Committee Report
The members of the Company’s Compensation Committee hereby state:
We have reviewed and discussed the Compensation Discussion and Analysis contained in this Annual Report on Form 10-K for the year ended October 31, 2012 with the Company’s Management, and
Based on such review and discussions, we have recommended to the Company’s Board of Directors that the Compensation Discussion and Analysis be included in the Company’s Annual Report on Form 10-K for the year ended October 31, 2012.
| | COMPENSATION COMMITTEE |
| | |
| By: | John Roglieri M.D., Chairman |
| | Joseph Benincasa |
| | Harry Elias |
| | Gary Lederman |
37
Item 12. - Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters
The following table sets forth information as of January 4, 2013 with respect to the ownership of Common Stock by (i) each person known to us to be the beneficial owner of more than 5% of our outstanding Common Stock, (ii) each of our directors, (iii) each of our executive officers, and (iv) all directors and executive officers as a group.
Name and Address of Beneficial
Owner* | | Shares of Common Stock
Beneficially Owned(1) | | Percentage
Ownership | |
| | | | | |
Marc D. Grodman(2) | | 2,752,800 | | 10 | % |
Howard Dubinett(3) | | 365,138 | | 1 | % |
Sam Singer(4) | | 41,132 | | ** | |
Joseph Benincasa | | 0 | | 0 | % |
Harry Elias | | 0 | | 0 | % |
Gary Lederman(5) | | 30,400 | | ** | |
John Roglieri(6) | | 5,000 | | ** | |
Executive Officers and Directors as a group (seven persons) (2)(3)(4)(5)(6) | | 3,207,670 | | 11 | % |
| | | | | |
Black Rock, Inc(7) 40 East 52nd Street New York, NY 10022 | | 1,918,462 | | 7 | % |
Prudential Financial, Inc.(8) 751 Broad Street Newark, NJ 07102-3777 | | 2,900,514 | | 10 | % |
Jennison Associates LLC(9) 466 Lexington Avenue New York, NY 10017 | | 2,804,461 | | 10 | % |
Palisade Capital Management, L.L.C. (10) One Bridge Plaza, Suite 695 Fort Lee, NJ 07024 | | 1,590,000 | | 5.69 | % |
Riverbridge Partners LLC(11) 801 Nicollet Mall, Suite 600 Minneapolis, MN 55402 | | 1,927,486 | | 6.89 | % |
* The address of all of the Company’s directors and executive officers is c/o the Company, 481 Edward H. Ross Drive, Elmwood Park, New Jersey 07407.
** Less than one (1%) percent.
(1) Except as otherwise noted, each holder named in the table has sole voting and investment power with respect to all shares of Common Stock shown as beneficially owned.
(2) Includes 2,308,466 shares owned directly. Also includes 147,934 shares owned directly by Dr. Grodman’s wife, Pam Grodman, and 200,000 shares held in trust for the benefit of Pam Grodman, and 96,400 shares owned by their children. Dr. Grodman disclaims beneficial ownership of these 444,334 shares.
(3) Includes 365,138 shares owned directly.
(4) Includes 26,132 shares owned directly, and 15,000 shares owned by children who share Mr. Singer’s household. Mr. Singer disclaims beneficial ownership of these 15,000 shares.
(5) Includes 30,400 shares owned directly.
(6) Includes 5,000 shares owned directly.
(7) Black Rock, Inc. (“Black Rock”) is the beneficial owner of these 1,918,462 shares. In its Schedule 13G filing dated January 20, 2012 filed with the Securities and Exchange Commission, Black Rock stated that to the best of its knowledge, these 1,918,462 shares were acquired in the ordinary course of business; were not acquired for the purpose of and do not have the effect of changing or influencing the control of the Company; and were not acquired in connection with or as a participant in any transaction having such purpose or effect.
(8) Prudential Financial, Inc. (“Prudential”) is the beneficial owner of these 2,900,514 shares. In its Schedule 13G filing dated February 10, 2012 (as of December 31, 2011) filed with the Securities and Exchange Commission, Prudential stated that to the best of its knowledge, these 2,900,514 shares were acquired in the ordinary course of business; were not acquired for the purpose of and do not have the effect of changing or influencing the control of the Company; and were not acquired in connection with or as a participant in any transaction having such purpose or effect. Prudential is a parent holding company and the indirect parent of, among others, Jennison Associates LLC.
(9) Jennison Associates LLC (“Jennison”) is the beneficial owner of these 2,804,461 shares. In its Schedule 13G filing dated February 10, 2012 (as of December 31, 2011) filed with the Securities and Exchange Commission, Jennison stated that to the best of its knowledge, these 2,804,461 shares were acquired in the ordinary course of business; were not acquired for the purpose of and do not have the effect of changing or influencing the control of the Company; and were not acquired in connection with or as a participant in any transaction having such purpose or effect.
(10) Palisade Capital Management, L.L.C. (“Palisade”) is the beneficial owner of these 1,590,000 shares. In its Schedule 13G filing dated February 8, 2012 (as of December 31, 2011) filed with the Securities and Exchange Commission, Palisade stated that to the best of its
38
knowledge, these 1,590,000 shares were acquired in the ordinary course of business; were not acquired for the purpose of and do not have the effect of changing or influencing the control of the Company; and were not acquired in connection with or as a participant in any transaction having such purpose or effect.
(11) Riverbridge Partners LLC (“Riverbridge”) is the beneficial owner of these 1,927,486 shares. In its Schedule 13G filing dated February 6, 2012 (as of December 31, 2011) filed with the Securities and Exchange Commission, Riverbridge stated that to the best of its knowledge, these 1,927,486 shares were acquired in the ordinary course of business; were not acquired for the purpose of and do not have the effect of changing or influencing the control of the Company; and were not acquired in connection with or as a participant in any transaction having such purpose or effect.
Equity Compensation Plan Information
The following table provides information as of October 31, 2012 regarding shares of Common Stock that may be issued pursuant to the Company’s equity compensation plans:
| | (a)
Number of Shares Issuable
upon Exercise of Outstanding
Options | | (b)
Weighted-Average Exercise
Price per Share of Outstanding
Options | | (c)
Number of Shares Remaining
Available for Future Issuances Under
Equity Compensation Plans
(Excluding Shares Reflected
in Column (a)) | |
| | | | | | | |
Equity Compensation Plans Approved by Stockholders | | 311,000 | (1) | $ | 9.18 | | 841,520 | (2) |
| | | | | | | | |
(1) Reflects shares issuable upon exercise of outstanding ISOs granted pursuant to the Company’s 2000 and 2003 Employee Stock Option Plans.
(2) Reflects shares reserved for issuance upon the grant of ISOs which may be granted pursuant to the 2003 Employee Incentive Stock Option Plans.
Item 13. — Certain Relationships and Related Transactions
No material transactions occurred between the Company and related parties during fiscal 2012. See item 11 herein and footnote 7 to the consolidated financial statements.
It is the Company’s policy that transactions involving related persons (excluding executive officer compensation which is determined by the Compensation Committee) are to be presented to and assessed by the independent members of the board of directors. Related persons include the Company’s directors and executive officers, immediate family members of the directors and executive officers, and certain large security holders and their family members. If the determination is made that a related person has or may have a material direct or indirect interest in any Company transaction and that the amount involved equals or exceeds $120,000, the Company’s independent directors will review, approve and ratify the transaction, if appropriate, and the transaction will be disclosed if required under SEC rules. If the related party at issue is a director of the Company or a family member of a director, then that director will not participate in the relevant discussion and review.
Information considered in evaluating such transactions include the nature of the related person’s interest in the transaction, the material terms of the transaction, the importance of the transaction to the Company and the related person, whether the transaction would impair the judgment of a director or an executive officer to act in the best interests of the Company, and any other matters that management or the independent directors deem appropriate. Corporate policy requires all directors and employees, including all executives, to disclose their interests (including indirect interests through family members) with individuals or entities doing business with the Company, to management and/or the Board of Directors, and to remove themselves from all decisions related to that organization. No such transactions with related parties occurred in fiscal year 2010 through 2012.
Item 14. - Principal Accountant Fees and Services
The firm of MSPC, Certified Public Accountants and Advisors, A Professional Corporation (“MSPC”) audited our accounts and the accounts of our subsidiaries for the fiscal years ended October 31, 2012 and 2011. MSPC and its predecessor firm have been our auditors since 1988. The table set forth below lists the fees billed to the company by MSPC for audit services rendered in connection with the audits of our consolidated financial statements for the years ended October 31, 2012 and 2011, and fees billed for other services rendered by MSPC during these periods.
| | 2012 | | 2011 | |
| | (in thousands) ($) | |
(1) Audit Fees | | 376 | | 273 | |
(2) Audit-Related Fees | | 40 | | 43 | |
(3) Tax Fees | | 15 | | 15 | |
(4) All Other Fees | | 0 | | 0 | |
Total | | 430 | | 331 | |
(1) Audit Fees
MSPC billed us approximately $376,000 for professional services rendered in connection with the audit of our annual financial statements for the fiscal year ended October 31, 2012 and the review of the financial statements included in our quarterly reports on Form 10-Q for such fiscal year compared to approximately $273,000 in billings for such services for the fiscal year ended October 31, 2011. In addition, MSPC billed us approximately $29,000 in fiscal 2012 for its audit of our 401(k) Plan for calendar year 2011 as compared to approximately $15,000 of such fees in fiscal 2011 with respect to calendar year 2010.
39
(2) Audit-Related Fees
MSPC billed us approximately $40,000 during fiscal 2012 and approximately $43,000 during fiscal 2011 for Sarbanes-Oxley (“SOX”) related audit fees.
(3) Tax Fees
MSPC billed us approximately $15,000 for tax services for fiscal 2012 and approximately $15,000 for tax services for fiscal 2011.
(4) All Other Fees
No fees were billed to us by MSPC with respect to fiscal 2012 or fiscal 2011 other than for services described in Item 14 (1), (2) and (3) herein.
(5) Pre-Approval Policies and Procedures
The engagement of MSPC to render the above audit and tax services was approved by our audit committee prior to the engagement.
40
PART IV
Item 15. — Exhibits and Financial Statement Schedules
(a) 1. Financial Statements
The following financial statements of the Company are included in Part II, Item 8, “Financial Statements and Supplementary Data:”
Report of Independent Registered Public Accounting Firm
Consolidated Balance Sheets - October 31, 2012 and 2011
Consolidated Statements of Operations for the Years ended October 31, 2012, 2011 and 2010
Consolidated Statements of Shareholders’ Equity for the Years ended October 31, 2012, 2011, and 2010
Consolidated Statements of Cash Flows for the Years ended October 31, 2012, 2011 and 2010
Notes to Consolidated Financial Statements
2. Financial Statements Schedule
The following is included in Item 8, “Financial Statements and Supplementary Data:”
Schedule II — Valuation and Qualifying Accounts for the Years ended October 31, 2012, 2011 and 2010
(b) Exhibits
Exhibit No. | | Item |
| | |
3.1* | | Amended and Restated Certificate of Incorporation dated November 15, 1989 (Incorporated by reference to exhibit filed with the Company’s annual report on form 10-K for the year ended October 31, 2011. (SEC File No. 0-15266). |
| | |
3.1.1* | | Amendment to Certificate of Incorporation dated August 23, 1993 (Incorporated by reference to exhibit filed with the Company’s annual report on form 10-K for the year ended October 31, 2011. (SEC File No. 0-15266). |
| | |
3.1.2* | | Amendment to Certificate of Incorporation dated August 23, 1993 (Incorporated by reference to exhibit filed with the Company’s annual report on form 10-K for the year ended October 31, 2011. (SEC File No. 0-15266). |
| | |
3.1.3* | | Amendment to Certificate of Incorporation dated March 27, 1998 (Incorporated by reference to exhibit filed with the Company’s annual report on form 10-K for the year ended October 31, 2011. (SEC File No. 0-15266). |
| | |
3.1.4* | | Amendment to Certificate of Incorporation dated March 31, 1998 (Incorporated by reference to exhibit filed with the Company’s annual report on form 10-K for the year ended October 31, 2011. (SEC File No. 0-15266). |
| | |
3.1.5* | | Amendment to Certificate of Incorporation dated September 26, 2003 (Incorporated by reference to exhibit filed with the Company’s annual report on form 10-K for the year ended October 31, 2011. (SEC File No. 0-15266). |
| | |
3.2.2* | | By-laws, as amended. (Incorporated by reference to exhibit filed with the Company’s annual report on form 10-K for the year ended October 31, 2011. (SEC File No. 0-15266). |
| | |
4.1* | | Form of Common Stock Certificate, $.01 par value (Incorporated by reference to exhibit filed with the Company’s annual report on form 10-K for the year ended October 31, 2004 (SEC File No. 0-15266)). |
| | |
10.1* | | Lease Agreement for Elmwood Park, New Jersey Premises, expiring in February, 2004 (Incorporated by reference to exhibit filed with the Company’s annual report on Form 10-K for the year ended October 31, 1999 (SEC File No. 0-15266)). |
| | |
10.1.1* | | Fifth Amendment dated as of July 16, 2004 to Lease for Elmwood Park, New Jersey Premises (Incorporated by reference to exhibit filed with the Company’s annual report on Form 10-K for the year ended October 31, 2004 (SEC File No. 0-15266)). |
| | |
10.1.2* | | Sixth Amendment dated as of October 27, 2004 to Lease for Elmwood Park, New Jersey Premises (Incorporated by reference into exhibit filed with the Company’s annual report on Form 10-K for the year ended October 31, 2004 (SEC File No. 0-15266)). |
| | |
10.2* | | Employment Agreement between the Company and Marc Grodman expiring October 31, 2017. (Incorporated by reference to exhibit filed with the Company’s current report on Form 8-K for December 31, 2010 (SEC File No. 0-15266)). |
| | |
10.3* | | Employment Agreement between the Company and Sam Singer as in effect at October 31, 2001 (Incorporated by reference to exhibit filed with the Company’s annual report on Form 10-K for the year ended October 31, 1999 (SEC File No. 0-15266)). |
| | |
10.3.1* | | Extension to Employment Agreement between the Company and Sam Singer effective November 1, 2002 (Incorporated by reference to exhibit filed with the Company’s annual report on Form 10-K for the year ended October 31, 2002 (SEC File No. 0-15266)). |
| | |
10.3.2* | | Extension to Employment Agreement between the Company and Sam Singer effective November 1, 2004 (Incorporated by reference to exhibit filed with the Company’s annual report on Form 10-K for the year ended October 31, 2004 (SEC File No. 0-15266)). |
| | |
10.3.3* | | Amendment No. 3 to Employment Agreement between the Company and Sam Singer dated December 18, 2007. (Incorporated by reference to exhibit filed with the Company’s annual report on Form 10-K for the year ended October 31, 2007 (SEC File No. 0-15266)). |
| | |
10.3.4* | | Amendment No. 4 to Employment Agreement between the Company and Sam Singer dated March 4, 2008. (Incorporated by reference to exhibit filed with the Company’s annual report on form 10-K for the year ended October 31, 2011. (SEC File No. 0-15266). |
| | |
10.3.5* | | Amendment No. 5 to Employment Agreement between the Company and Sam Singer dated September 18, 2008. (Incorporated by reference to exhibit filed with the Company’s annual report on form 10-K for the year ended October 31, 2011. (SEC File No. 0-15266). |
41
10.3.6* | | Amendment No. 6 to Employment Agreement between the Company and Sam Singer dated October, 2009. (Incorporated by reference to exhibit filed with the Company’s annual report on form 10-K for the year ended October 31, 2011. (SEC File No. 0-15266). |
| | |
10.3.7* | | Amendment No. 7 to Employment Agreement between the Company and Sam Singer dated November 1, 2010. (Incorporated by reference to exhibit filed with the Company’s annual report on form 10-K for the year ended October 31, 2011. (SEC File No. 0-15266). |
| | |
10.4* | | The Company’s 2000 Employee Incentive Stock Option Plan. (Incorporated by reference to exhibit filed with the Company’s annual report on Form 10-K for the year ended October 31, 2000 (SEC File No. 0-15266)). |
| | |
10.4.1* | | The Company’s 2003 Employee Incentive Stock Option Plan. (Incorporated by reference to exhibit filed with the Company’s Registration Statement on Form S-8 (File No. 333-111578)). |
| | |
10.5* | | The Company’s 2010 Senior Management Incentive Bonus Plan (Incorporated by reference to exhibit filed with the Company’s annual report on Form 10-K for the year ended October 31, 2010 (SEC File No. 0-15266)). |
| | |
10.5.1* | | The Company’s 2011 Senior Management Incentive Bonus Plan. (Incorporated by reference to exhibit filed with the Company’s annual report on form 10-K for the year ended October 31, 2011. (SEC File No. 0-15266). |
| | |
10.5.2* | | The Company’s 2012 Senior Management Incentive Bonus Plan. (Incorporated by reference to exhibit filed with the Company’s annual report on form 10-K for the year ended October 31, 2011. (SEC File No. 0-15266). |
| | |
10.5.3 | | The Company’s 2013 Senior Management Incentive Bonus Plan. |
| | |
10.6* | | Amended and Restated Loan and Security Agreement as of September 30, 2004 between the Company and PNC Bank, National Association. (Incorporated by reference to exhibit filed with the Company’s annual report on Form 10-K for the year ended October 31, 2004 (SEC File No. 0-15266)). |
| | |
10.6.1* | | Fourth Amendment as of October 31, 2006 to Loan and Security Agreement as of September 30, 2004 between the Company and PNC Bank, National Association (Incorporated by reference to exhibit filed with the Company’s annual report on Form 10-K for the year ended October 31, 2006 (SEC File No. 0-15266)). |
| | |
10.6.2* | | Fifth Amendment as of October 31, 2007 to Loan and Security Agreement as of September 30, 2004 between the Company and PNC Bank, National Association (Incorporated by reference to exhibit filed with the Company’s annual report on Form 10-K for the year ended October 31, 2007 (SEC File No. 0-15266)). |
| | |
10.6.3* | | Sixth Amendment as of May 12, 2008 to Loan and Security Agreement as of September 30, 2004 between the Company and PNC Bank, National Association (Incorporated by reference to exhibit filed with the Company’s current report on Form 8-K (for December 31, 2010) (SEC File No. 0-15266)). |
| | |
10.6.4* | | Seventh Amendment as of October 22, 2010 to Loan and Security Agreement between the Company and PNC Bank, National Association. (Incorporated by reference to exhibit filed with the Company’s annual report on form 10-K for the year ended October 31, 2011. (SEC File No. 0-15266). |
| | |
10.6.5* | | Eighth Amendment as of November 2, 2011 to Loan and Security Agreement as of October 31, 2010 between the Company and PNC Bank, National Association. (Incorporated by reference to exhibit filed with the Company’s annual report on form 10-K for the year ended October 31, 2011. (SEC File No. 0-15266). |
| | |
21 | | Subsidiaries of the Company |
| | |
23.1 | | Consent of Independent Registered Public Accounting Firm |
| | |
31.1 | | Certification of Chief Executive Officer |
| | |
31.2 | | Certification of Chief Financial Officer |
| | |
32.1 | | Certification pursuant to 18 U.S.C. Section 1350 of Chief Executive Officer |
| | |
32.2 | | Certification pursuant to 18 U.S.C. Section 1350 of Chief Financial Officer |
| | |
101 | | Interactive Data File |
The exhibits designated above with an asterisk (*) have previously been filed with the Commission and, pursuant to 17 C.F.R. Secs. 201.24 and 240.12b-32, are incorporated by reference to the documents as indicated.
42
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
BIO-REFERENCE LABORATORIES, INC. | |
| |
| |
By | /S/ Marc D. Grodman | |
Marc D. Grodman | |
Chairman of the Board, President, | |
Chief Executive Officer and Director | |
Dated: January 11, 2013 | |
| | |
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
/S/ Marc D. Grodman | |
Marc D. Grodman | |
Chairman of the Board, President, | |
Chief Executive Officer and Director | |
January 11, 2013 | |
| |
/S/ Howard Dubinett | |
Howard Dubinett | |
Executive Vice President, | |
Chief Operating Officer and Director | |
January 11, 2013 | |
| |
/S/ Sam Singer | |
Sam Singer | |
Sr. Vice President, Chief Financial Officer, | |
Chief Accounting Officer and Director | |
January 11, 2013 | |
| |
/S/ Joseph Benincasa | |
Joseph Benincasa | |
Director | |
January 11, 2013 | |
| |
/S/ Harry Elias | |
Harry Elias | |
Director | |
January 11, 2013 | |
| |
/S/ Gary Lederman | |
Gary Lederman | |
Director | |
January 11, 2013 | |
| |
/S/ John Roglieri | |
John Roglieri | |
Director | |
January 11, 2013 | |
43
Index to Financial Statements and Financial Statement Schedule
44
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Board of Directors and Shareholders
Bio-Reference Laboratories, Inc.
Elmwood Park, New Jersey
We have audited the accompanying consolidated balance sheets of Bio-Reference Laboratories, Inc. and its subsidiaries (the “Company”) as of October 31, 2012 and 2011, and the related consolidated statements of operations, shareholders’ equity, and cash flows for each of the fiscal years in the three-year period ended October 31, 2012. We also have audited the Company’s internal control over financial reporting as of October 31, 2012, based on criteria established in Internal Control - Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (“COSO”). The Company’s management is responsible for these consolidated financial statements, for maintaining effective internal control over financial reporting, and for its assessment of the effectiveness of internal control over financial reporting, included in the accompanying Management’s Report on Internal Control over Financial Reporting. Our responsibility is to express an opinion on these consolidated financial statements and an opinion on the Company’s internal control over financial reporting based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audits to obtain reasonable assurance about whether the financial statements are free of material misstatement and whether effective internal control over financial reporting was maintained in all material respects. Our audits of the consolidated financial statements included examining, on a test basis, evidence supporting the amounts and disclosures in the consolidated financial statements, assessing the accounting principles used and significant estimates made by management, and evaluating the overall consolidated financial statement presentation. Our audit of internal control over financial reporting included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, and testing and evaluating the design and operating effectiveness of internal control based on the assessed risk. Our audits also included performing such other procedures as we considered necessary in the circumstances. We believe that our audits provide a reasonable basis for our opinions.
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (a) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (b) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (c) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the consolidated financial position of Bio-Reference Laboratories, Inc. and its subsidiaries as of October 31, 2012 and 2011, and the consolidated results of their operations and their cash flows for each of the fiscal years in the three-year period ended October 31, 2012, in conformity with accounting principles generally accepted in the United States of America. Also in our opinion, Bio-Reference Laboratories Inc. and its subsidiaries maintained, in all material respects, effective internal control over financial reporting as of October 31, 2012, based on criteria established in Internal Control - Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (“COSO”).
MSPC
Certified Public Accountants and Advisors,
A Professional Corporation
Cranford, New Jersey
January 11, 2013
45
BIO-REFERENCE LABORATORIES, INC. AND SUBSIDIARIES
CONSOLIDATED BALANCE SHEETS
[Dollars In Thousands, Except Share Data]
| | October 31, | | October 31, | |
| | 2012 | | 2011 | |
| | | | | |
CURRENT ASSETS: | | | | | |
Cash and Cash Equivalents | | $ | 25,143 | | $ | 22,013 | |
Accounts Receivable - Net | | 153,247 | | 148,060 | |
Inventory | | 14,902 | | 9,691 | |
Other Current Assets | | 5,373 | | 4,457 | |
Deferred Tax Assets | | 24,912 | | 22,559 | |
TOTAL CURRENT ASSETS | | 223,577 | | 206,780 | |
| | | | | |
PROPERTY AND EQUIPMENT - AT COST | | 102,701 | | 81,717 | |
LESS: Accumulated Depreciation | | (52,261 | ) | (38,150 | ) |
PROPERTY AND EQUIPMENT - NET | | 50,440 | | 43,567 | |
| | | | | |
OTHER ASSETS: | | | | | |
Investment in Unconsolidated Affiliate | | 4,977 | | — | |
Deposits | | 956 | | 882 | |
Goodwill - Net | | 23,408 | | 23,408 | |
Intangible Assets - Net | | 6,323 | | 6,904 | |
Other Assets | | 866 | | 725 | |
Deferred Tax Assets | | 2,278 | | 993 | |
TOTAL OTHER ASSETS | | 38,808 | | 32,912 | |
| | | | | |
TOTAL ASSETS | | $ | 312,825 | | $ | 283,259 | |
The Accompanying Notes are an Integral Part of These Consolidated Financial Statements.
46
BIO-REFERENCE LABORATORIES, INC. AND SUBSIDIARIES
CONSOLIDATED BALANCE SHEETS
[Dollars In Thousands, Except Share Data]
| | October 31, | | October 31, | |
| | 2012 | | 2011 | |
| | | | | |
CURRENT LIABILITIES: | | | | | |
Accounts Payable | | $ | 41,288 | | $ | 38,612 | |
Accrued Salaries and Commissions Payable | | 16,490 | | 11,770 | |
Accrued Taxes and Expenses | | 9,753 | | 8,853 | |
Other Short Term Acquisition Payable | | — | | 375 | |
Revolving Note Payable - Bank | | — | | 18,632 | |
Current Maturities of Long-Term Debt | | 464 | | 1,270 | |
Capital Lease Obligations - Short-Term Portion | | 3,957 | | 3,002 | |
TOTAL CURRENT LIABILITIES | | 71,952 | | 82,514 | |
| | | | | |
LONG-TERM LIABILITIES: | | | | | |
Capital Lease Obligations - Long-Term Portion | | 9,463 | | 6,351 | |
Long Term Debt - Net of Current Portion | | 4,163 | | 4,627 | |
TOTAL LONG-TERM LIABILITIES | | 13,626 | | 10,978 | |
| | | | | |
SHAREHOLDERS’ EQUITY: | | | | | |
Preferred Stock $.10 Par Value; | | | | | |
Authorized 1,666,667 shares, including 3,000 shares of Series A Junior Preferred Stock | | | | | |
None Issued | | — | | — | |
Common Stock, $.01 Par Value; | | | | | |
Authorized 35,000,000 shares: | | | | | |
Issued and Outstanding 27,707,382 and 27,949,900 at October 31, 2012 and at October 31, 2011, respectively | | 277 | | 280 | |
| | | | | |
Additional Paid-In Capital | | 40,907 | | 45,580 | |
| | | | | |
Retained Earnings | | 186,063 | | 143,907 | |
| | | | | |
TOTAL SHAREHOLDERS’ EQUITY | | 227,247 | | 189,767 | |
TOTAL LIABILITIES AND SHAREHOLDERS’ EQUITY | | $ | 312,825 | | $ | 283,259 | |
The Accompanying Notes are an Integral Part of These Consolidated Financial Statements.
47
BIO-REFERENCE LABORATORIES, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF OPERATIONS
[Dollars In Thousands, Except Share Data]
| | Years Ended | |
| | October 31, | |
| | 2012 | | 2011 | | 2010 | |
| | | | | | | |
NET REVENUES: | | $ | 661,661 | | $ | 558,642 | | $ | 458,024 | |
| | | | | | | |
COST OF SERVICES: | | | | | | | |
Depreciation and Amortization | | 13,101 | | 11,036 | | 8,653 | |
Employee Related Expenses | | 146,292 | | 126,354 | | 104,519 | |
Reagents and Lab Supplies | | 121,446 | | 100,569 | | 77,798 | |
Other Cost of Services | | 56,805 | | 49,894 | | 41,282 | |
| | | | | | | |
TOTAL COST OF SERVICES | | 337,644 | | 287,853 | | 232,252 | |
| | | | | | | |
GROSS PROFIT ON REVENUES | | 324,017 | | 270,789 | | 225,772 | |
| | | | | | | |
General and Administrative Expenses: | | | | | | | |
| | | | | | | |
Depreciation and Amortization | | 3,562 | | 3,969 | | 3,168 | |
Other General and Administrative Expenses | | 154,928 | | 131,967 | | 111,983 | |
Bad Debt Expense | | 89,396 | | 75,079 | | 62,243 | |
| | | | | | | |
TOTAL GENERAL AND ADMIN. EXPENSES | | 247,886 | | 211,015 | | 177,394 | |
| | | | | | | |
OPERATING INCOME | | 76,131 | | 59,774 | | 48,378 | |
| | | | | | | |
OTHER (INCOME) EXPENSES: | | | | | | | |
| | | | | | | |
Interest Expense | | 1,455 | | 1,747 | | 1,566 | |
Other (Income) Expense | | 323 | | (6,656 | ) | | |
Interest Income | | (163 | ) | (163 | ) | (151 | ) |
| | | | | | | |
TOTAL OTHER EXPENSES - NET | | 1,615 | | (5,072 | ) | 1,415 | |
| | | | | | | |
INCOME BEFORE INCOME TAXES | | 74,516 | | 64,846 | | 46,963 | |
| | | �� | | | | |
Provision for Income Taxes | | 32,360 | | 28,487 | | 20,582 | |
| | | | | | | |
NET INCOME | | 42,156 | | 36,359 | | $ | 26,381 | |
| | | | | | | |
NET INCOME PER SHARE - BASIC: | | $ | 1.52 | | $ | 1.30 | | $ | 0.95 | |
WEIGHTED AVERAGE NUMBER OF SHARES - BASIC: | | 27,742,257 | | 27,971,100 | | 27,786,083 | |
| | | | | | | |
NET INCOME PER SHARE - DILUTED: | | $ | 1.51 | | $ | 1.29 | | $ | 0.94 | |
WEIGHTED AVERAGE NUMBER OF SHARES - DILUTED: | | 27,920,920 | | 28,207,358 | | 28,038,304 | |
The Accompanying Notes are an Integral Part of These Consolidated Financial Statements.
48
BIO-REFERENCE LABORATORIES, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF SHAREHOLDERS’ EQUITY
[Dollars In Thousands Except Number of Shares]
| | Series A | | | | | | | | | | | | | |
| | Senior Preferred
Stock | | Common Stock | | Additional
Paid-in | | Retained | | Deferred | | Total Shareholders’ | |
| | Shares | | Amount | | Shares | | Amount | | Capital | | Earnings | | Compensation | | Equity | |
| | | | | | | | | | | | | | | | | |
Balance on October 31, 2009 | | | | | | 27,694,876 | | $ | 276 | | $ | 43,080 | | $ | 81,167 | | — | | $ | 124,523 | |
| | | | | | | | | | | | | | | | | |
Exercise of Options - Employees | | | | | | 117,800 | | 2 | | 795 | | | | | | 797 | |
Stock Based Compensation | | | | | | 11,432 | | — | | 290 | | | | | | 290 | |
Stock Issued for Acquisition | | | | | | 23,096 | | — | | 397 | | | | | | 397 | |
Common Stock Repurchased and Canceled | | | | | | — | | | | — | | | | | | — | |
Net Income | | | | | | | | | | | | 26,381 | | | | 26,381 | |
| | | | | | | | | | | | | | | | | |
Balance on October 31, 2010 | | | | | | 27,847,204 | | $ | 278 | | $ | 44,562 | | $ | 107,548 | | — | | $ | 152,388 | |
| | | | | | | | | | | | | | | | | |
Exercise of Options - Employees | | | | | | 79,600 | | 1 | | 497 | | | | | | 498 | |
Stock Based Compensation | | | | | | | | | | 40 | | | | | | 40 | |
Stock Issued for Acquisition | | | | | | 23,096 | | — | | 482 | | | | | | 482 | |
Net Income | | | | | | | | | | | | 36,359 | | | | 36,359 | |
| | | | | | | | | | | | | | | | | |
Balance on October 31, 2011 | | | | | | 27,949,900 | | $ | 279 | | $ | 45,581 | | $ | 143,907 | | — | | $ | 189,767 | |
| | | | | | | | | | | | | | | | | |
Exercise of Options - Employees | | | | | | 31,500 | | 1 | | 226 | | | | | | 227 | |
Stock Based Compensation | | | | | | 11,432 | | — | | 290 | | | | | | 290 | |
Net Income | | | | | | | | | | | | 42,156 | | | | 42,156 | |
Common Stock Repurchased and Canceled | | | | | | (285,450 | ) | (3 | ) | (5,190 | ) | | | | | (5,193 | ) |
| | | | | | | | | | | | | | | | | |
Balance on October 31, 2012 | | | | | | 27,707,382 | | $ | 277 | | $ | 40,907 | | $ | 186,063 | | | | $ | 227,247 | |
The Accompanying Notes are an Integral Part of These Consolidated Financial Statements.
49
BIO-REFERENCE LABORATORIES, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF CASH FLOWS
[Dollars In Thousands]
| | Years Ended October 31, | |
| | 2012 | | 2011 | | 2010 | |
OPERATING ACTIVITIES: | | | | | | | |
Net Income | | $ | 42,156 | | $ | 36,359 | | $ | 26,381 | |
Adjustments to Reconcile Net Income to Cash Provided by Operating Activities: | | | | | | | |
Depreciation and Amortization | | 16,663 | | 15,005 | | 11,821 | |
Deferred Income Taxes (Benefit) | | (3,638 | ) | (5,911 | ) | (4,005 | ) |
Stock - Based Compensation Expense | | 290 | | 40 | | 290 | |
Loss on Disposal of Property and Equipment | | 537 | | 1,680 | | 368 | |
Undistributed Equity Method Loss | | 323 | | — | | — | |
Change in Assets and Liabilities: | | | | | | | |
(Increase) Decrease in: | | | | | | | |
Accounts Receivable | | (11,240 | ) | (29,254 | ) | (32,984 | ) |
Provision for Doubtful Accounts | | 6,053 | | 10,316 | | 8,857 | |
Inventory | | (5,211 | ) | (3,498 | ) | (2,045 | ) |
Other Current Assets | | (916 | ) | (1,637 | ) | (941 | ) |
Other Assets | | (141 | ) | 798 | | (150 | ) |
Deposits | | (74 | ) | 507 | | (759 | ) |
Increase in: | | | | | | | |
Accounts Payable and Accrued Liabilities | | 8,296 | | 6,541 | | 6,572 | |
| | | | | | | |
NET CASH - OPERATING ACTIVITIES | | 53,098 | | 30,946 | | 13,405 | |
| | | | | | | |
INVESTING ACTIVITIES: | | | | | | | |
Business Acquisitions Related Costs | | (5,675 | ) | (1,425 | ) | (1,917 | ) |
Acquisition of Equipment and Leasehold Improvements | | (15,715 | ) | (14,117 | ) | (16,494 | ) |
| | | | | | | |
NET CASH - INVESTING ACTIVITIES | | (21,390 | ) | (15,542 | ) | (18,411 | ) |
| | | | | | | |
FINANCING ACTIVITIES: | | | | | | | |
Payments of Long-Term Debt | | (1,270 | ) | (1,178 | ) | (1,191 | ) |
Payments of Capital Lease Obligations | | (3,710 | ) | (2,968 | ) | (2,778 | ) |
Increase (Decrease) in Revolving Line of Credit | | (18,632 | ) | (7,522 | ) | 8,962 | |
Proceeds from Exercise of Options | | 227 | | 498 | | 797 | |
Common Stock Repurchased | | (5,193 | ) | | | | |
| | | | | | | |
NET CASH - FINANCING ACTIVITIES | | (28,578 | ) | (11,170 | ) | 5,790 | |
| | | | | | | |
NET INCREASE IN CASH AND CASH EQUIVALENTS | | 3,130 | | 4,234 | | 784 | |
| | | | | | | |
CASH AND CASH EQUIVALENTS AT BEGINNING OF PERIODS | | $ | 22,013 | | $ | 17,779 | | $ | 16,995 | |
| | | | | | | |
CASH AND CASH EQUIVALENTS AT END OF PERIODS | | $ | 25,143 | | $ | 22,013 | | $ | 17,779 | |
| | | | | | | |
SUPPLEMENTAL DISCLOSURES OF CASH FLOW INFORMATION: | | | | | | | |
Cash paid during the period for: | | | | | | | |
Interest | | $ | 1,547 | | $ | 1,754 | | $ | 1,517 | |
Income Taxes | | $ | 36,697 | | $ | 32,773 | | $ | 26,539 | |
The Accompanying Notes are an Integral Part of These Consolidated Financial Statements
50
BIO-REFERENCE LABORATORIES, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF CASH FLOWS
[Dollars In Thousands Except Share Data]
Supplemental Schedule of Non-Cash Investing and Financing Activities:
During fiscal 2012, 2011 and 2010, the Company wrote-off approximately $2,508, $5,944 and $6,352 of property which was fully depreciated.
During fiscal 2011, the Company disposed of certain equipment with an initial cost of $4,558. During the same period the Company financed the purchase of new equipment through a term note of $5,408.
During fiscal 2012, 2011, and 2010, the Company incurred capital lease obligations totaling approximately $7,777, $5,444, and $3,403 in connection with the acquisition of property and equipment.
During fiscal 2012, 2011 and 2010 the company recorded approximately $290, $40 and $290 of stock based compensation expense related to granting of stock options and Company’s stock to employees.
[See Notes 9, 11 and 18 for additional non-cash transactions]
The Accompanying Notes are an Integral Part of These Consolidated Financial Statements
51
BIO-REFERENCE LABORATORIES, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
[Dollars In Thousands Except Share Data or Unless Otherwise Indicated]
[1] Organization and Business
Bio-Reference Laboratories, Inc. [“Bio-Reference” or the “Company”] was incorporated on December 24, 1981. Bio-Reference is principally engaged in providing laboratory testing services, primarily to customers in the greater New York metropolitan area as well as to customers in a number of other states. Bio-Reference offers a comprehensive list of chemical diagnostic tests including blood and urine analysis, blood chemistry, hematology services, serology, radio-immuno analysis, toxicology (including drug screening), pap smears, tissue pathology (biopsies) and other tissue analysis. We perform cancer cytogenetic testing at our leased facilities in at our main processing facility in Elmwood Park, Smithtown, NY, Clarksburg, MD and Milford, MA and genetic testing at our GeneDx leased facility in Gaithersburg, MD, as well as at our Elmwood Park facility. We perform cytology testing in Frederick, MD, Milford, MA, Columbus, OH, Houston, TX and at our Elmwood Park facility. Bio-Reference markets its laboratory testing services directly to physicians, geneticists, hospitals, clinics, correctional and other health facilities.
The Company’s laboratory testing business currently represents its one reportable business segment. The laboratory testing business accounts for over 98% of consolidated assets, net revenues and net income in each of the three years ended October 31, 2012. All other operating segments include the Company’s non-clinical laboratory testing businesses and consist of our clinical knowledge management service through our PSIMedica business unit and a web-based connectivity portal solution for laboratories and physicians through its CareEvolve subsidiary.
[2] Summary of Significant Accounting Policies
Principles of Consolidation - The consolidated financial statements include the accounts of the Company and its wholly-owned subsidiaries. All significant intercompany accounts and transactions have been eliminated.
Cash and Cash Equivalents - Cash equivalents are comprised of certain highly liquid investments with a maturity of three months or less when purchased. The Company had $24,665 and $22,013 in cash and cash equivalents at October 31, 2012 and 2011, respectively.
Inventory - Inventory is stated at the lower of cost [determined on a first-in, first-out basis] or market. Inventory consists primarily of purchased laboratory supplies, which is used in our various testing laboratories.
Property and Equipment - Property and equipment are carried at cost. Depreciation is computed by the straight-line method over the estimated useful lives of the respective assets, which range from 2 to 15 years. Leasehold improvements are amortized over the life of the lease, which is approximately five years.
The statements of operations reflect depreciation expense related to property and equipment of $16,082, $13,684 and $10,520 for the years ended October 31, 2012, 2011 and 2010, respectively.
On sale or retirement, the asset cost and related accumulated depreciation or amortization are removed from the accounts, and any related gain or loss is reflected in general and administrative expenses. Repairs and maintenance are charged to expense when incurred.
Goodwill - Effective November 1, 2011, the Company adopted revised Financial Accounting Standards Board (“FASB”) rules promulgated under Accounting Standards Update (“ASU”) No. 2011-08 issued on September 15, 2011, the, Intangibles—Goodwill and Other (Topic 350) Testing Goodwill for Impairment. Under these simplified goodwill impairment testing rules the Company assessed qualitative factors to determine whether events and circumstances lead to the conclusion that it is necessary to perform the two-step goodwill impairment test have occurred and determined that no such events had occurred. Under ASU No. 2011-08, entities are not required to calculate the fair value of a reporting unit unless they conclude that it is more likely than not that the unit’s carrying value is greater than its fair value based on an assessment of events and circumstances. The “more likely than not” threshold is when there is a likelihood of more than 50% that a reporting unit’s carrying value is greater than its fair value. No impairment loss was recognized in the years ended October 31, 2012, 2011 and 2010.
The balance sheet reflects prior Goodwill accumulated amortization of $2,401 as of October 31, 2012 and 2011, respectively.
Other Intangible Assets - Intangible assets are amortized using the straight-line method. The estimated useful life of costs capitalized is evaluated for each specific project when completed, at which time such costs begin to be amortized. The statements of operations reflect amortization expense related to intangible assets of $581, $1,322, and $1,301 for the years ended October 31, 2012, 2011 and 2010, respectively. The balance sheet reflects accumulated amortization of $7,852, and $7,271 as of October 31, 2012, and 2011, respectively. During the 2012 and 2011 fiscal years, the Company did not write off any intangible assets.
Fair Value Measurements.
On November 1, 2008, the Company adopted “Fair Value Measurements” for its financial assets discussed under topic number 820 “Fair Value Measurements and Disclosures” of FASB codification. This topic provides a single definition of fair value, establishes a framework for measuring fair value in U.S. generally accepted accounting principles (“GAAP”), and expands disclosures about fair value measurements. This topic creates a three-level hierarchy for the inputs used in the valuation techniques to derive fair values where Level 1 is having the highest priority and Level 3 having the lowest priority.
52
| | 10/31/2012 | | Quoted Prices in
Active Markets for
Identical
Assets/Liabilities | | Significant Other
Observable Inputs | | Significant
Unobservable
Inputs | |
| | | | Level 1 | | Level 2 | | Level 3 | |
Assets: | | | | | | | | | |
Cash surrender value of officers’ life insurance policies (a component of Other Assets) | | $ | 866 | | — | | $ | 866 | | — | |
| | | | | | | | | | | |
Accounting for Revenue
Service revenues are principally generated from laboratory testing services including chemical diagnostic tests such as blood analysis, urine analysis and genetic testing among others. Net service revenues are recognized at the time the testing services are performed and are reported at their estimated net realizable amounts.
Net service revenues are determined utilizing gross service revenues net of contractual allowances. Even though it is the responsibility of the patient to pay for laboratory service bills, most individuals in the United States have an agreement with a third party payor such as Medicare, Medicaid or a commercial insurance provider to pay all or a portion of their healthcare expenses; the majority of services provided by BRLI are to patients covered under a third party payor contract. In certain cases, the individual has no insurance or does not provide insurance information and in other cases tests are performed under contract to a professional organization (such as physicians, hospitals, and clinics) which reimburse BRLI directly; in the remainder of the cases, BRLI is provided the third party billing information and seeks payment from the third party under the terms and conditions of the third party payor for health service providers like BRLI. Each of these third party payors may differ not only with regard to rates, but also with regard to terms and conditions of payment and providing coverage (reimbursement) for specific tests. Estimated revenues are established based on a series of highly complex procedures and judgments that require industry specific healthcare experience and an understanding of payor methods and trends. We review our calculations on a monthly basis in order to make certain that we are properly allowing for the uncollectable portion of our gross billings and that our estimates remain sensitive to variances and changes within our payor groups. The contractual allowance calculation is made on the basis of historical allowance rates for the various specific payor groups on a monthly basis with a greater weight being given to the most recent trends; this process is adjusted based on recent changes in underlying contract provisions and shifts in the testing being performed. Bad Debt represents our estimate of net revenues that will ultimately be uncollectable and is based upon our analysis of historical payment rates by specific payor groups on a monthly basis with primary weight being given to the most recent trends; this approach allows bad debt to more accurately adjust to short-term changes in the business environment. These two calculations are routinely analyzed by BRLI on the basis of actual allowances issued by payors and the actual payments made to determine what adjustments, if any, are needed. The chart below shows the adjustments made to gross service revenues to arrive at net service revenues.
| | October, 31 | |
| | 2012 | | 2011 | | 2010 | |
| | | | | | | |
Gross Revenues | | $ | 3,052,431 | | $ | 2,482,349 | | $ | 1,902,573 | |
| | | | | | | |
Contractual Adjustments and Discounts: | | | | | | | |
Medicare/Medicaid Portion | | 320,697 | | 293,874 | | 281,002 | |
All Other Third Party and Direct Payors* | | 2,070,073 | | 1,629,833 | | 1,163,547 | |
Total Contractual Adjustments and Discounts | | 2,390,770 | | 1,923,707 | | 1,444,549 | |
| | | | | | | |
Net Service Revenues | | $ | 661,661 | | $ | 558,642 | | $ | 458,024 | |
| | | | | | | |
Percent of Contractual Adjustments and Discounts To Gross Revenues | | 78.3 | % | 77.5 | % | 75.9 | % |
* All Other Third Party and Direct Payors consists of almost eight hundred distinct payors, including commercial health insurers and administrators as well as professionally billed accounts such as physicians, hospitals, clinics and other direct billed accounts.
When new business is received by BRLI, net service revenues are calculated by reducing gross service revenues by the estimated contractual allowance. The bad debt expense is determined by calculating the appropriate collection rate for net current service revenues and is a component of general and administrative expenses. BRLI recognized the amounts in subsequent periods for actual allowances/discounts to gross service revenue; bad debt was adjusted over the same periods of time to maintain an accurate balance between net service revenues and actual revenues. Management has reviewed the allowances/discounts recognized in subsequent periods and believes the amounts to be immaterial. A number of proposals for legislation or regulation continue to be under discussion which could have the effect of substantially reducing Medicare reimbursements for clinical laboratories or introducing cost sharing to beneficiaries. Depending upon the nature of regulatory action, if any, which is taken and the content of legislation, if any, which is adopted, the Company could experience a significant decrease in revenues from Medicare and Medicaid, which could have a material adverse effect on the Company. The Company is unable to predict, however, the extent to which such actions will be taken.
53
Accounting for Contractual Credits and Doubtful Accounts
It is typically the responsibility of the patient to pay for laboratory service bills. Most individuals in the United States have an agreement with a third party payor such as Medicare, Medicaid or commercial insurance to pay all or a portion of their healthcare expenses; this represents the major portion of payment for all services provided to BRLI. In certain cases, the individual has no insurance or does not provide insurance information; in the remainder of the cases, BRLI is provided the third party billing information, usually by the referring physician, and seeks payment from the third party under the terms and conditions of the third party payor for health service providers like BRLI. Each of these third party payors may differ not only with regard to rates, but also with regard to terms and conditions of payment and coverage of specific tests. BRLI routinely reviews the reimbursement policies and subsequent payments and collection rates from these different types of payors. Contractual credits are recorded as reductions to gross service revenues and are collectively referred to as the contractual allowance. BRLI has not been required to record an adjustment in a subsequent period related to revenue recorded in a prior period which was material in nature. Aging of accounts receivable is monitored by billing personnel and follow-up activities including collection efforts are conducted as necessary. Bad debt expense is recorded within selling, general and administrative expenses. BRLI writes off receivables against the allowance for doubtful accounts when they are deemed uncollectible. For client billing, accounts are written off when all reasonable collection efforts prove to be unsuccessful. Patient accounts, where the patient is directly responsible for all or a remainder portion of the account after partial payment or denial by a third party payor, are written off after the normal dunning cycle has occurred, although these may be subsequently transferred to a third party collection agency after being written off. Third party payor accounts are written off when they exceed the payor’s timely filing limits. Accounts Receivable on the balance sheet is net of the following amounts for contractual credits and doubtful accounts:
| | October 31 | |
| | 2012 | | 2011 | |
| | | | | |
Contractual Credits/Discounts | | $ | 267,921 | | $ | 235,922 | |
Doubtful Accounts | | 51,274 | | 45,220 | |
| | | | | |
Total Allowance | | $ | 319,195 | | $ | 281,142 | |
Current Income Taxes — The Company recognizes interest and penalties on settlement of tax liabilities in its income from operations. For the fiscal years 2010 through 2012, no material amounts for interest and penalties have been recorded.
Deferred Income Taxes - Deferred income tax assets and liabilities are computed annually for differences between the financial statement and tax bases of assets and liabilities that will result in taxable or deductible amounts in the future based on enacted tax laws and rates applicable to the periods in which the differences are expected to affect taxable income.
The Company adopted GAAP guidance with respect to uncertain tax positions when it became effective. Under these rules the Company may recognize the tax benefit from an uncertain tax position only if it meets the more-likely-than-not criteria (over 50% likelihood) of being realized on an examination by taxing authorities. For the years ended October 31, 2012 through October 31, 2010 the Company had no material uncertain tax positions to report.
Earnings Per Share - Basic earnings per share [“EPS”] reflects the amount of income attributable to each share of common stock based on average common shares outstanding during the period. Diluted EPS reflects Basic EPS while giving effect to all potential dilutive common shares that were outstanding during the period, such as common shares that could result from the exercise or conversion of securities into common stock. The computation of Diluted EPS is calculated by using the treasury stock method, which assumes that any proceeds obtained from the exercise of such dilutive securities would be used to purchase common stock at the average market price of the common stock during the period. This reduces the gross number of dilutive shares by the number of shares purchasable from the proceeds of the securities assumed to be exercised. Securities whose conversion would have an anti-dilutive effect on EPS are not assumed converted. Securities that could potentially dilute earnings in the future are disclosed in Note 10.
Use of Estimates - The preparation of financial statements in conformity with generally accepted accounting principles requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the reporting period. Actual results could differ from those estimates.
Recoverability and Impairment of Intangible Assets and Other Long-Lived Assets — The Company evaluates the possible impairment of its long-lived assets under the provisions of FASB codification 350-30-35 and 360-10-35. The Company reviews the recoverability of its long-lived assets on an annual basis. Evaluation of possible impairment is based on the Company’s ability to recover the asset from the expected future pretax cash flows (undiscounted and without interest charges) of the related operations. If the expected undiscounted pretax cash flows are less than the carrying amount of such asset, an impairment loss is recognized for the difference between the estimated fair value and carrying amount of the asset. No impairment loss was recognized in the fiscal years ended October 31, 2012, 2011 and 2010.
Advertising Costs -Advertising costs are expensed when incurred. Advertising costs amounted to approximately $2,366, $2,026 and $2,065 for the years ended October 31, 2012, 2011 and 2010, respectively.
Reclassifications - Certain prior year amounts may have been reclassified to conform to the current year presentation.
Other Income — During the year the Company recorded a loss of $323 on its investment in IncellDx. The loss represents the Company’s share of IncellDX undistributed net loss under the equity method of accounting.
Subsequent Events — The management considered subsequent events through the date the financial statements are issued as defined in FASB Codification 855-10-50.
54
[3] Property and Equipment - Property and equipment - at cost is summarized as follows:
| | October 31 | |
| | 2012 | | 2011 | |
| | | | | |
Medical Equipment | | $ | 50,338 | | $ | 38,479 | |
Leasehold Improvements | | 19,768 | | 14,388 | |
Furniture, Fixtures and Office & Computer Equipment | | 16,503 | | 13,586 | |
Automobiles and Aircraft | | 16,092 | | 15,264 | |
| | | | | |
Sub Totals | | 102,701 | | 81,717 | |
Less Accumulated Depreciation | | 52,261 | | 38,150 | |
| | | | | |
Totals — Net of Accumulated Depreciation | | $ | 50,440 | | $ | 43,567 | |
[4] Intangible Assets
Intangible assets are summarized as follows:
October 31, 2011
| | Weighted-Average | | | | Accumulated | | Net of
Accumulated | |
Intangible Asset | | Amortization Period | | Cost | | Amortization | | Amortization | |
| | | | | | | | | |
Customer Lists | | 20 | | $ | 4,573 | | $ | 2,328 | | $ | 2,245 | |
Covenants Not-to-Compete | | 5 | | 4,305 | | 4,237 | | 68 | |
Patents and Licenses | | 17 | | 5,297 | | 706 | | 4,591 | |
| | | | | | | | | |
Totals | | | | $ | 14,175 | | $ | 7,285 | | $ | 6,904 | |
October 31, 2012
| | Weighted-Average | | | | Accumulated | | Net of
Accumulated | |
Intangible Asset | | Amortization Period | | Cost | | Amortization | | Amortization | |
| | | | | | | | | |
Customer Lists | | 20 | | $ | 4,573 | | $ | 2,537 | | $ | 2,036 | |
Covenants Not-to-Compete | | 5 | | 4,305 | | 4,257 | | 48 | |
Patents and Licenses | | 17 | | 5,297 | | 1,058 | | 4,239 | |
| | | | | | | | | |
Totals | | | | $ | 14,175 | | $ | 7,852 | | $ | 6,323 | |
The estimated amortization expense related to intangible assets for each of the five succeeding fiscal years and thereafter as of October 31, 2012 is as follows:
October 31, | | | |
2013 | | $ | 558 | |
2014 | | 551 | |
2015 | | 526 | |
2016 | | 509 | |
2017 | | 503 | |
Thereafter | | 3,676 | |
| | | |
Total | | $ | 6,323 | |
| | | | | |
[5] Revolving Note Payable - Bank
In October 2011, the Company entered into an amended revolving note payable loan agreement with PNC Bank, N.A. The maximum amount of the credit line available to the Company pursuant to the loan agreement is the lesser of (i) $45,000 or (ii) 50% of the Company’s qualified accounts receivable [as defined in the agreement]. The amendment to the Loan and Security Agreement provides for an interest rate on advances to be subject, at the election of the Company, to either the bank’s base rate or the Eurodollar rate of interest plus, in certain instances, an additional interest percentage. The additional interest percentage charge on bank’s base rate borrowings and on Eurodollar rate borrowings ranges from 1% to 4% and is determined based upon certain financial ratios achieved by the Company. At October 31, 2012, the Company had elected to have all of the total advances outstanding to be subject to the bank’s base rate of interest of 3.50%. The credit line is collateralized by substantially all of the Company’s assets. The line of credit is available through October 2016 and may be extended for annual periods by mutual consent, thereafter. The terms of this agreement contain, among other provisions, requirements for maintaining defined levels of capital expenditures, fixed charge coverage, and the prohibition of the payment by the Company of cash dividends. As of October 31, 2012, the Company paid off the credit line.
55
[6] Long-Term Debt - Bank
Effective as of October 31, 2007, we executed a fifth amendment to the Loan Agreement formalizing the repayment terms of the $5 million term loan from PNC Bank used by our wholly-owned GeneDX (formerly, BRLI No. 2 Acquisition Corp.) subsidiary to fund the $5 million acquisition cash payment in connection with its purchase of the operating assets of GeneDx, Inc. The term loan is evidenced by a secured promissory note payable over a six year term in equal monthly principal payments of approximately $69, plus interest at an annual rate of 6.85%. The note was paid off on October 31, 2012.
In December 2010, The Company issued a seven year term note for $5,408 at the rate of interest of 6.12% per annum for the financing of new equipment. The note is payable in eighty-four equal monthly installments commencing on January 29, 2011 of $61 including principal and interest followed by a balloon payment of the principal and interest outstanding on the loan repayment date of December 29, 2017. The balance on this note as of October 31, 2012 is approximately $4,627.
Principal repayment for each of the five succeeding fiscal years and thereafter as of October 31, 2012 is as follows:
Year Ended | | | |
October 31, | | | |
2013 | | $ | 464 | |
2014 | | 486 | |
2015 | | 518 | |
2016 | | 551 | |
2017 | | 585 | |
Thereafter | | 2,023 | |
Totals | | $ | 4,627 | |
[7] Related Party Transactions [Not in Thousands]
There were no material related party transactions during fiscal 2012.
[8] Income Taxes
The reconciliation of income tax from continuing operations computed at the U.S. federal statutory tax rate to the Company’s effective income tax rate is as follows:
| | October 31 | |
| | 2012 | | 2011 | | 2010 | |
| | | | | | | |
U.S. Federal Statutory Rate | | 35 | % | 35 | % | 35 | % |
State and Local Taxes, Net of U.S. Federal Tax Benefit | | 8.87 | % | 9.87 | % | 9.77 | % |
Permanent differences and Other | | (0.44 | )% | (0.94 | )% | (0.94 | )% |
| | | | | | | |
Actual Rate | | 43.43 | % | 43.93 | % | 43.83 | % |
The provision for income taxes shown in the consolidated statements of operations consists of the following:
| | October 31 | |
| | 2012 | | 2011 | | 2010 | |
| | | | | | | |
Current: | | | | | | | |
Federal | | $ | 25,794 | | $ | 24,573 | | $ | 17,201 | |
State & Local | | 10,203 | | 9,825 | | 7,069 | |
| | | | | | | |
Deferred: | | | | | | | |
Federal | | (2,183 | ) | (4,223 | ) | (2,618 | ) |
State and Local | | (1,454 | ) | (1,688 | ) | (1,070 | ) |
| | | | | | | |
Total Provision for Income Taxes | | $ | 32,360 | | $ | 28,487 | | $ | 20,582 | |
At October 31, 2012 and 2011, the Company had a net deferred tax asset of approximately $27,190 and $23,552, respectively. The deferred taxes primarily relate to timing differences associated with the deductibility of depreciation and amortization, bad debts and certain accrued expenses and deferred costs. For fiscal years ended in 2012 and in 2011, the Company had no material net operating loss carry-forwards available to reduce current year taxable income.
| | October 31, | |
| | 2012 | | 2011 | |
| | | | | |
Deferred Tax Asset: | | | | | |
Bad Debt Allowance | | $ | 22,560 | | $ | 19,897 | |
Depreciation and amortization | | 1,963 | | 1,723 | |
Accrued Expenses | | 2,667 | | 1,932 | |
| | | | | |
Deferred Tax Asset - Net | | 27,190 | | 23,552 | |
| | | | | |
Current Deferred Tax Asset - Net | | 24,912 | | 21,710 | |
Long Term Deferred Tax Asset - Net | | 2,278 | | 1,842 | |
| | | | | |
Deferred Tax Asset — Net | | $ | 27,190 | | $ | 23,552 | |
56
During fiscal year ended October 31, 2012 the Company recorded a net deferred tax benefit of $3,638. This reflects a net benefit of approximately $2,664 in allowance for bad debts, a benefit of approximately $240 from depreciation and amortization timing differences, and a benefit of approximately $734 in certain accrued expenses. Although realization is not assured and dependent upon things such as generating sufficient taxable income in future periods, management, through sufficient positive evidence, believes it is more likely than not that all of the deferred tax asset will be realized. The amount of the deferred tax asset considered realizable, however, could be reduced in the near term if estimates of future taxable income or changes in the accrued expenses during the future periods are reduced.
At October 31, 2012, fiscal 2009 through 2012 are subject to examination by US federal and state tax authorities. Through the issuance of these financial statements the outcome of all of these examinations has not been determined.
[9] Capital Transactions
[A] Preferred Stock and Common Stock - The Company is authorized to issue an aggregate of 1,666,667 shares of preferred stock, $.10 par value. None was outstanding as of October 31, 2012 and October 31, 2011.
Holders of the Company’s Common Stock are entitled to one vote per share on matters submitted for shareholder vote. Holders are also entitled to receive dividends ratably, if declared. In the event of dissolution or liquidation, holders are entitled to share ratably in all assets remaining after payment of liabilities.
On July 14, 2008, the Board of Directors authorized a repurchase of up to 1,000,000 shares of the Company’s common stock over the period ending October 31, 2010. As of October 31, 2010 the Company repurchased 39,400 shares at a cost of $452. The shares were canceled upon repurchase.
On November 11, 2011, the Company announced that its board of directors has approved a Stock Repurchase Program authorizing the repurchase of up to 1,000,000 shares of its Common Stock in the over-the-counter market at prevailing market prices over the period ending October 31, 2012. As of October 31, 2012 the Company repurchased 274,018 shares at a cost of $5,193. On December 6, 2012, the Company announced that its board of directors has approved a new Stock Repurchase Program authorizing the buyback of up to 714,550 shares of its Common Stock in the over-the-counter market at prevailing market prices through October 31, 2013.
[B] Equity Transactions for Services — For the fiscal years ended in 2012, 2011 and 2010, the Company issued 11,432, 11,432 and 16,432 shares of the Company’s common stock for employment or consulting services [See Note 11 for common stock options issued for employee and consulting services].
[10] Earnings Per Share
The computation of basic and diluted net earnings per common share is as follows [in thousands, except per share data rounded]:
| | For Years Ended October 31, | |
| | 2012 | | 2011 | | 2010 | |
| | | | | | | |
Income Available to Common Stockholders | | $ | 42,156 | | $ | 36,359 | | $ | 26,381 | |
Weighted Average Common Shares Outstanding | | 27,742 | | 27,971 | | 27,786 | |
| | | | | | | |
Effect of Dilutive Securities: | | | | | | | |
Warrants/Options | | 179 | | 236 | | 252 | |
| | | | | | | |
Weighted Average Diluted Common Shares Outstanding | | 27,921 | | 28,207 | | 28,038 | |
| | | | | | | |
Net Income Per Share - Basic | | $ | 1.52 | | $ | 1.30 | | $ | 0.95 | |
Net Income Per Share - Diluted | | $ | 1.51 | | $ | 1.29 | | $ | 0.94 | |
[11] Stock Options and Warrants
Employee Incentive Stock Options - In June 2003, the Board of Directors adopted, and in July 2003, the stockholders approved, the 2003 Employee Incentive Stock Option Plan [the “2003 Plan”]. The 2003 Plan authorizes the grant of stock options, which may be designated as incentive stock options, to purchase up to a maximum aggregate 1,600,000 shares of Company common stock. The 2003 Plan provides that the exercise price of an option granted there under shall not be less than the fair market value of the Common Stock on the date the option is granted. However, in the event an option is granted under the 2003 Plan to a holder of 10% or more of the Company’s outstanding Common Stock, the exercise price must be at least 110% of such fair market value. Under the 2003 Plan, options must be granted before the June 2, 2013 Termination Date. No option may have a term longer than ten years (limited to five years in the case of an option granted to a 10% or greater stockholder of the Company). The aggregate fair market value of the Company’s Common Stock with respect to which options are exercisable for the first time by a grantee under all of the Company’s Stock Option Plans during any calendar year cannot exceed $100. Options granted under the 2003 Plan are non-transferable and must be exercised by an optionee, if at all, while employed by the Company or a subsidiary or within three months after termination of such optionee’s employment due to retirement, or within one year of such termination if due to disability or death. The Board (or a Stock Option Committee, if designated), may, in its sole discretion, cause the Company to lend money to or guaranty any obligation of an employee for the purpose of enabling such employee to exercise an option granted under the 2003 Plan provided that such loan or obligation cannot exceed fifty percent (50%) of the exercise price of such option. In fiscal year ended October 31, 2012, 2011 and 2010, -0-, -0- and -0- options were granted under the Plan, respectively. A total of 23,500, 40,000 and 59,000 incentive stock options issued under the 2003 Plan were exercised in fiscal years ended in October 31, 2012, 2011 and 2010, respectively. A total of 13,000, -0- and 12,000 options were cancelled in fiscal years ended October 31, 2012, 2011 and 2010.
In August 2000, the Company adopted, and on December 15, 2000, the stockholders approved, the 2000 Employee Incentive Stock Option Plan [“2000 Plan”]. The 2000 Plan provided for the granting of stock options, which may have been designated as incentive stock options, to purchase an aggregate of 1,600,000 shares of the Company’s common stock (after giving effect to our 2-1 stock split) at a price not less than 100% of the fair market value per share of the common stock at the date of grant. However, in the event an option was granted under the 2000 Plan to a holder of 10% or more of the Company’s outstanding common stock, the exercise price must have been at least 110% of fair market value at the date of grant. Employees of the Company or its subsidiary, as determined, were eligible for the 2000 Plan. The term of the options could not exceed ten years from the date of grant. In fiscal years ended October 31, 2012, 2011 and 2010, no options were granted under the Plan. A total of 8,000, 39,600 and 58,800 incentive stock options issued under the 2000 Plan were exercised
57
in fiscal years ended in October 31, 2012, 2011 and 2010, respectively. A total of -0-, -0-, and -0- options were cancelled in fiscal years ended October 31, 2012, 2011 and 2010, respectively. Options issued under the 2000 Plan must have been granted before the August 2010 termination date.
The following is a summary of Employee Incentive Stock Option Plan transactions:
| | 2003 Plan | |
| | Shares Under Options [In Thousands] | | Weighted Average Exercise Price Per Share | |
Outstanding at October 31, 2009* | | 406 | | $ | 9.52 | |
Granted | | — | | — | |
Expired | | (12 | ) | 8.62 | |
Exercised | | (59 | ) | 8.88 | |
Outstanding at October 31, 2010* | | 335 | | 9.66 | |
Granted | | — | | — | |
Expired | | — | | — | |
Exercised | | (40 | ) | 8.67 | |
Outstanding at October 31, 2011* | | 295 | | 9.80 | |
| | | | | |
Granted | | — | | — | |
Expired | | (13 | ) | 9.13 | |
Exercised | | (23 | ) | 8.52 | |
Outstanding at October 31, 2012* | | 259 | | $ | 9.95 | |
*Eligible for exercise at October 31, 2009 were 376 at a weighted average exercise price per share of $7.80
*Eligible for exercise at October 31, 2010 were 310 at a weighted average exercise price per share of $9.66
*Eligible for exercise at October 31, 2011 were 275 at a weighted average exercise price per share of $9.80
*Eligible for exercise at October 31, 2012 were 244 at a weighted average exercise price per share of $9.95
| | 2000 Plan | |
| | Shares Under
Options
[In Thousands] | | Weighted
Average
Exercise Price
Per Share | |
| | | | | |
Outstanding and Eligible for Exercise at October 31, 2009 | | 158 | | $ | 4.64 | |
Granted | | — | | — | |
Expired | | — | | — | |
Exercised | | (58 | ) | 4.63 | |
Outstanding and Eligible for Exercise at October 31, 2010 | | 100 | | 4.64 | |
Granted | | — | | — | |
Expired | | — | | — | |
Exercised | | (40 | ) | 3.82 | |
Outstanding and Eligible for Exercise at October 31, 2011 | | 60 | | 5.19 | |
| | | | | |
Granted | | — | | — | |
Expired | | — | | — | |
Exercised | | (8 | ) | 3.39 | |
Outstanding and Eligible for Exercise at October 31, 2012 | | 52 | | $ | 5.47 | |
| | Weighted Average | | Exercisable | |
Exercise Price Range | | Shares
Outstanding | | Remaining
Life | | Exercise
Price | | Shares
Outstanding | | Exercise
Price | |
$2.76 | to | $2.76 | Per Share | | 20 | | 0.17 | | $ | 2.76 | | 20 | | 2.76 | |
$3.60 | to | $3.60 | Per Share | | 4 | | 0.17 | | $ | 3.60 | | 4 | | 3.60 | |
$6.57 | to | $6.57 | Per Share | | 6 | | 2.69 | | $ | 6.57 | | 6 | | 6.57 | |
$7.25 | to | $7.25 | Per Share | | 4 | | 2.58 | | $ | 7.25 | | 4 | | 7.25 | |
$7.41 | to | $7.67 | Per Share | | 86 | | 2.70 | | $ | 7.53 | | 86 | | 7.53 | |
$9.12 | to | $9.13 | Per Share | | 151 | | 2.00 | | $ | 9.13 | | 151 | | 9.13 | |
$17.50 | to | $17.50 | Per Share | | 40 | | 5.08 | | $ | 17.50 | | 25 | | 17.50 | |
| | 311 | | | | | | 296 | | | |
Compensation cost recognized for the years ended October 31, 2012, October 31, 2011 and October 31, 2010 was $40 for each one of the years, with a related tax benefit of $-0- with respect to these options.
[12] Employment Contracts and Consulting Agreements
The Company has multiple employment contracts with its key executives with expiration dates ranging from October 31, 2015 through October 31, 2017. At October 31, 2012, the approximate aggregate minimum commitment under these employment contracts and agreements, excluding commissions or consumer price index increases, is as follows:
58
October 31 | | Employees and Consultants | |
2013 | | $ | 4,982 | |
2014 | | 4,302 | |
2015 | | 3,654 | |
2016 | | 2,780 | |
2017 | | 1,243 | |
Thereafter | | — | |
| | | |
Total | | $ | 16,961 | |
Some of these agreements provide bonuses and commissions based on a percentage of collected revenues ranging from 1% to 10% on accounts referred by or serviced by the employee or consultant.
In addition to the above, the Company has entered into forty nine at — will employment and consulting agreements which together with prior at — will agreements provide for annual aggregate minimum commitments of approximately $27,497 which have no termination dates.
[13] Capitalized Lease Obligations
The Company leases various assets under capital leases expiring in fiscal 2017 as follows:
| | October 31 | |
| | 2012 | | 2011 | |
Medical Equipment | | $ | 12,078 | | $ | 7,732 | |
Furniture, Fixtures and Office Equipment | | — | | — | |
Automobiles | | 8,711 | | 9,512 | |
| | | | | |
Totals | | 20,789 | | 17,244 | |
Less: Accumulated Depreciation | | 6,776 | | 4,950 | |
| | | | | |
Net | | $ | 14,013 | | $ | 12,294 | |
Depreciation expense on assets under capital leases was approximately $3,792, $1,418, and $2,364 for the years ended October 31, 2012, 2011 and 2010, respectively.
Aggregate future minimum rentals under capital leases are:
October 31, | | | |
2013 | | $ | 1,200 | |
2014 | | 1,199 | |
2015 | | 1,199 | |
2016 | | 1,199 | |
2017 | | 598 | |
Thereafter | | — | |
| | | |
Total | | 5,395 | |
| | | |
Less Interest: | | 440 | |
| | | |
Present Value of Minimum Lease Payments | | $ | 4,955 | |
[14] Commitments and Contingencies
The Company leases various office and laboratory facilities and equipment under operating leases expiring from 2013 to 2019. Several of these leases contain renewal options for one to five year periods.
Total expense for property and equipment rental for the years ended October 31, 2012, 2011 and 2010 was $8,787, $8,010 and $7,285, respectively. There were no contingent rental amounts due through October 31, 2012.
Aggregate future minimum rental payments on non cancelable operating leases [exclusive of several month to month leases] are as follows:
October 31, | | Property | | Equipment | |
| | | | | |
2013 | | $ | 6,809 | | $ | 318 | |
2014 | | 3,493 | | 187 | |
2015 | | 1,535 | | 73 | |
2016 | | 1,049 | | | |
2017 | | 429 | | | |
Thereafter | | 1,357 | | | |
| | | | | |
Totals | | $ | 14,672 | | $ | 578 | |
| | | | | | | | |
59
The Company has entered into several purchase agreements for reagent supplies through October, 2017. Minimum purchase commitments as of October 31, 2012 are as follows:
October 31, | | | |
| | | |
2013 | | $ | 23,758 | |
2014 | | 22,365 | |
2015 | | 19,943 | |
2016 | | 17,441 | |
2017 | | 7,566 | |
Thereafter | | — | |
| | | |
Totals | | $ | 91,073 | |
Reagent supplies expensed under purchase agreements amount to $13,338 $8,379, and $7,290 for the years ended October 31, 2012, 2011 and 2010, respectively.
[15] Litigation
In the normal course of business, the Company is exposed to a number of asserted and unasserted potential claims. In the opinion of management, the resolution of these matters will not have a material adverse effect on the Company’s financial position or results of operations.
[16] Insurance
The Company maintains professional liability insurance of $3,000 in the aggregate, with a per occurrence limit of $1,000. In addition, the Company maintains excess commercial insurance of $5,000 per occurrence and $5,000 in aggregate over the primary limits. In addition, the Company also maintains excess umbrella coverage of $15,000. The Company believes, but cannot assure, that its insurance coverage is adequate for its current business needs. A determination of Company liability for uninsured or underinsured acts or omissions could have a material adverse affect on the Company’s operations.
[17] Significant Risks and Uncertainties
[A] Concentrations of Credit Risk - Cash - At October 31, 2012 and 2011, the Company had approximately $23,260 and $21,000 , respectively, in cash and certificate of deposit balances at financial institutions which were in excess of the federally insured limits.
[B] Concentration of Credit Risk - Accounts Receivable - Credit risk with respect to accounts receivable is generally diversified due to the large number of patients comprising the client base. The Company does have significant receivable balances with government payors and various insurance carriers. Generally, the Company does not require collateral or other security to support customer receivables. However, the Company continually monitors and evaluates its client acceptance and collection procedures to minimize potential credit risks associated with its accounts receivable and establishes an allowance for uncollectible accounts and as a consequence, believes that its accounts receivable credit risk exposure beyond such allowance is not material to the financial statements.
A number of proposals for legislation continue to be under discussion which could substantially reduce Medicare and Medicaid (CMS) reimbursements to clinical laboratories. Depending upon the nature of regulatory action, and the content of legislation, the Company could experience a significant decrease in revenues from Medicare and Medicaid (CMS), which could have a material adverse effect on the Company. The Company is unable to predict, however, the extent to which such actions will be taken.
[18] Acquisitions
On March 2, 2010, the Company completed the purchase of substantially all of the tangible and intangible assets, excluding cash, receivables and certain other assets, of Lenetix Medical Screening Laboratory, Inc. (“Lenetix”) from Lenetix and its sole stockholder. These assets were utilized in Lenetix’s operation of a clinical testing laboratory located in Mineola, New York. The laboratory performs both clinical laboratory diagnostic testing and genetic testing. The purchase price of $5,490 included a down payment of $4,740 and a hold-back of $750 to insure the accuracy of the Sellers’ representations and to protect the Company from any claims based on the operations of the Laboratory prior to the closing. This acquisition resulted in an addition to Goodwill in the amount of $490.
On August 5, 2011, the Company acquired all of the authorized, issued and outstanding shares of The Genetics Center, Inc. (“GCI”), a New York corporation engaged in the clinical laboratory business with principal place of business in Smithtown, New York for $800 in cash. The entire acquisition was recorded as an addition to Goodwill.
On April 27, 2012, the Company entered into an agreement pursuant to which the Company purchased preferred shares of IncellDx, Inc. (“IncellDx”), a Delaware corporation. Information about IncellDx and the agreement may be found in the Current Report on Form 8-K the Company filed on May 1, 2012.
The investment in IncellDx is being recorded under the equity method of accounting. As of October 31, 2012 the Company invested a total $5,300 and recorded a loss on the Company’s share of undistributed loss of IncellDX of $323. The Company also has $700 allocated for an additional investment in IncellDx. These funds have not been used as of October 31, 2012.
On December 21, 2012, a date subsequent to our yearend, the Company entered into an agreement pursuant to which the Company agreed to purchase all of the authorized, issued and outstanding shares of Meridian Clinical Laboratory, Corp. (“Meridian”), a Florida corporation. Information about Meridian and the agreement may be found in the Form 8-K the Company filed on December 27, 2012.
On December 31, 2012, a date subsequent to our year end, we entered into an agreement pursuant to which we agreed to purchase all of the authorized, issued and outstanding shares of Florida Clinical Laboratory, Inc. (“FCL”), a Florida corporation. Information about FCL and the agreement may be found in the Form 8-K we filed on January 4, 2013.
[19] Fair Value of Financial Instruments
For certain financial instruments, including cash and cash equivalents, trade receivables, trade payables, and short-term debt, it was estimated that the carrying amount approximated fair value for the majority of these items because of their short maturities. The fair value of the Company’s long-term debt is estimated based on the quoted market prices for similar issues or by discounting expected cash flows at the rates currently offered to the Company for debt of the same remaining maturities.
60
Due to the non-interest bearing nature and unspecified payment terms, it was not practicable to estimate the fair value of amounts due from related parties [See also Note 7].
[20] Health Insurance Plan
The Company has a limited self-funded health insurance plan for its employees under which the Company pays the initial $150 of covered medical expenses per person each year. The Company has a contract with an insurance carrier for any excess up to a maximum of $2,000 per person and $20,504 in the aggregate. Health insurance premium expense for the years ended October 31, 2012, 2011 and 2010 amounted to approximately $5,792, $4,426 and $4,324, respectively. Uninsured employee medical expenses incurred by the Company amounted to approximately $25,994, $19,408 and $14,347 for the years ended October 31, 2012, 2011 and 2010, respectively. During fiscal years ended October 31, 2012, 2011 and 2010, employee contributions of $4,124, $3,593 and $2,720 offset the above health plan costs.
[21] Employee Benefit Plan
The Company sponsors a 401(k) Profit-Sharing Plan [the “Plan”]. Employees become eligible for participation after attaining the age of eighteen and completing one year of service. Participants may elect to contribute up to ten percent of their compensation, as defined in the Plan, to a maximum allowed by the Internal Revenue Service. The Company may choose to make a matching contribution to the plan for each participant who has elected to make tax-deferred contributions for the plan year, at a percentage determined each year by the Company. The Company elected to make a matching contribution which amounted to $1,106 for 2012, $993 for 2011, and $801 for 2010. These amounts were charged to the Statement of Operations. The Employer contribution will be fully vested after the third year of service.
[22] New Authoritative Accounting Pronouncements
Accounting Standards Update (ASU) 2012-02: Intangibles—Goodwill and Other (Topic 350)—Testing Indefinite-Lived Intangible Assets for Impairment. The Financial Accounting Standards Board (“FASB”) issued an Accounting Standards Update (“ASU”) 2012-02, Intangibles—Goodwill and Other (Topic 350)—Testing Indefinite-Lived Intangible Assets for Impairment, to establish an optional two-step analysis for impairment testing of indefinite-lived intangibles other than goodwill. The standards update will be effective for financial statements for periods beginning after September 15, 2012, with early adoption permitted.
In particular, the two-step analysis establishes an optional qualitative assessment to precede the quantitative assessment, if necessary. In the qualitative assessment, the entity must evaluate the totality of qualitative factors, including any recent fair value measurements, that impact whether an indefinite-lived intangible asset other than goodwill has a carrying amount that more likely than not exceeds its fair value. The entity must proceed to conducting a quantitative analysis, according to which the entity would record an impairment charge for the amount of the asset’s fair value exceeding the carrying amount, if (1) the entity determines that such impairment is more likely than not to exist, or (2) the entity foregoes the qualitative assessment entirely. The company adopted this update with no impact on its consolidated financial statements.
61
[23] Selected Quarterly Financial Data [Unaudited]
| | Three Month Ended | | Audited
Fiscal
Year | |
| | 1/31/12 | | 4/30/12 | | 7/31/12 | | 10/31/12 | | 2012 | |
| | | | | | | | | | | |
Net Revenues | | $ | 149,919 | | $ | 163,388 | | $ | 172,302 | | $ | 176,052 | | $ | 661,661 | |
Gross Profit | | $ | 71,243 | | $ | 79,479 | | $ | 86,049 | | $ | 87,246 | | $ | 324,017 | |
Net Income | | $ | 7,365 | | $ | 9,306 | | $ | 12,596 | | $ | 12,889 | | $ | 42,156 | |
Net Income Per Common Share: | | | | | | | | | | | |
| | | | | | | | | | | |
Basic | | $ | 0.26 | | $ | 0.34 | | $ | 0.45 | | $ | 0.47 | | $ | 1.52 | |
Diluted | | $ | 0.26 | | $ | 0.33 | | $ | 0.45 | | $ | 0.46 | | $ | 1.51 | |
| | | | | | | | | | | |
Weighted Average Common Shares Outstanding — Basic [in thousands] | | 27,888 | | 27,685 | | 27,695 | | 27,705 | | 27,742 | |
| | | | | | | | | | | |
Weighted Average Common Shares Outstanding - Diluted [in thousands] | | 28,041 | | 27,878 | | 27,888 | | 27,906 | | 27,921 | |
| | Three Month Ended | | Audited
Fiscal
Year | |
| | 1/31/11 | | 4/30/11 | | 7/31/11 | | 10/31/11 | | 2011 | |
| | | | | | | | | | | |
Net Revenues | | $ | 121,658 | | $ | 137,658 | | $ | 148,029 | | $ | 151,297 | | $ | 558,642 | |
Gross Profit | | $ | 56,804 | | $ | 65,639 | | $ | 73,432 | | $ | 74,914 | | $ | 270,789 | |
Net Income | | $ | 7,985 | | $ | 7,817 | | $ | 10,081 | | $ | 10,476 | | $ | 36,359 | |
Net Income Per Common Share: | | | | | | | | | | | |
| | | | | | | | | | | |
Basic | | $ | 0.29 | | $ | 0.28 | | $ | 0.36 | | $ | 0.37 | | $ | 1.30 | |
Diluted | | $ | 0.28 | | $ | 0.28 | | $ | 0.36 | | $ | 0.37 | | $ | 1.29 | |
| | | | | | | | | | | |
Weighted Average Common Shares Outstanding — Basic [in thousands] | | 27,884 | | 27,920 | | 27,941 | | 27,949 | | 27,971 | |
| | | | | | | | | | | |
Weighted Average Common Shares Outstanding - Diluted [in thousands] | | 28,122 | | 28,142 | | 28,147 | | 28,138 | | 28,207 | |
| | Three Month Ended | | Audited
Fiscal
Year | |
| | 1/31/10 | | 4/30/10 | | 7/31/10 | | 10/31/10 | | 2010 | |
| | | | | | | | | | | |
Net Revenues | | $ | 99,262 | | $ | 110,447 | | $ | 121,719 | | $ | 126,596 | | $ | 458,024 | |
Gross Profit | | $ | 47,508 | | $ | 53,668 | | $ | 61,630 | | $ | 62,966 | | $ | 225,772 | |
Net Income | | $ | 4,005 | | $ | 5,787 | | $ | 8,013 | | $ | 8,577 | | $ | 26,381 | |
Net Income Per Common Share: | | | | | | | | | | | |
| | | | | | | | | | | |
Basic | | $ | 0.14 | | $ | 0.21 | | $ | 0.29 | | $ | 0.31 | | $ | 0.95 | |
Diluted | | $ | 0.14 | | $ | 0.21 | | $ | 0.29 | | $ | 0.31 | | $ | 0.94 | |
| | | | | | | | | | | |
Weighted Average Common Shares Outstanding — Basic [in thousands] | | 27,723 | | 27,772 | | 27,815 | | 27,835 | | 27,786 | |
| | | | | | | | | | | |
Weighted Average Common Shares Outstanding - Diluted [in thousands] | | 28,022 | | 28,077 | | 28,098 | | 28,087 | | 28,038 | |
62
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Board of Directors and Shareholders of
Bio-Reference Laboratories, Inc.
Elmwood Park, New Jersey
Our report on our audit of the basic consolidated financial statements of Bio-Reference Laboratories, Inc. and its subsidiaries appears earlier in this document. That audit was conducted for the purpose of forming an opinion on the consolidated basic financial statements taken as a whole. The supplemental schedule II is presented for purposes of complying with the Securities and Exchange Commission’s Rules and Regulations under the Securities Exchange Act of 1934 and is not otherwise a required part of the basic consolidated financial statements. Such information has been subjected to the auditing procedures applied in the audit of the basic consolidated financial statements, and in our opinion, is fairly stated in all material respects in relation to the basic consolidated financial statements taken as a whole.
| MSPC |
| Certified Public Accountants and Advisors, |
| A Professional Corporation |
|
|
Cranford, New Jersey |
January 11, 2013 |
63
BIO-REFERENCE LABORATORIES, INC. AND SUBSIDIARIES
SCHEDULE II - VALUATION AND QUALIFYING ACCOUNTS FOR THE YEARS ENDED OCTOBER 31, 2012, 2011 AND 2010
[In Thousands]
| | (b) ($) | | | | (d) ($) | | | |
(a)
Description | | Balance at the
Beginning of a
Period | | (c) ($)
Charged to Cost
and Expenses | | Deductions Charged
to Valuation
Allowance Accounts | | (e) ($)
Balance at the End
of a Period | |
Year Ended October 31, 2012 | | | | | | | | | |
Allowance for Doubtful Accounts | | 45,220 | | 89,396 | | (83,342 | ) | 51,274 | |
Contractual Credits/Discounts | | 235,922 | | 2,390,770 | | (2,358,771 | ) | 267,921 | |
| | | | | | | | | |
Total Allowance | | 281,142 | | 2,480,166 | | (2,442,113 | ) | 319,195 | |
| | | | | | | | | |
Year Ended October 31, 2011 | | | | | | | | | |
Allowance for Doubtful Accounts | | 34,904 | | 75,079 | | (64,763 | ) | 45,220 | |
Contractual Credits/Discounts | | 186,372 | | 1,926,164 | | (1,876,614 | ) | 235,922 | |
| | | | | | | | | |
Total Allowance | | 221,276 | | 2,001,243 | | (1,941,377 | ) | 281,142 | |
| | | | | | | | | |
Year Ended October 31, 2010 | | | | | | | | | |
Allowance for Doubtful Accounts | | 26,047 | | 62,243 | | (53,386 | ) | 34,904 | |
Contractual Credits/Discounts | | 130,974 | | 1,444,549 | | (1,389,151 | ) | 186,372 | |
| | | | | | | | | |
Total Allowance | | 157,021 | | 1,506,792 | | (1,442,537 | ) | 221,276 | |
. . . . . . . . . .
64