UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
__________________________________
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 OR 15(d) of the Securities Exchange Act of 1934
Date of Report (date of earliest event reported): November 27, 2007
REHABCARE GROUP, INC.
(Exact name of Company as specified in its charter)
| Delaware | 0-19294 | 51-0265872 | |
| (State or other jurisdiction | (Commission | (I.R.S. Employer | |
| of incorporation) | File Number) | Identification No.) |
| | | | | | | | | | | |
| 7733 Forsyth Boulevard | |
| Suite 2300 | |
| St. Louis, Missouri | 63105 | |
(Address of principal executive offices) | (Zip Code) |
| | | | | | | | |
(314) 863-7422
(Company's telephone number, including area code)
Not applicable
(Former name or former address if changed since last report)
Check the appropriate box below if the Form 8-K filing is intended to simultaneously satisfy the filing obligation of the Company under any of the following provisions:
o Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425)
o Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12)
o Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b))
o Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c))
Item 7.01 | Regulation FD Disclosure |
Beginning on November 27, 2007, RehabCare executives will make presentations at investor conferences to analysts and in other forums using the slides as included in this Form 8-K as Exhibit 99. Presentations will be made using these slides, or modifications thereof, in connection with other presentations in the foreseeable future.
Information contained in this presentation is an overview and intended to be considered in the context of RehabCare's SEC filings and all other publicly disclosed information. We undertake no duty or obligation to update or revise this information. However, we may update the presentation periodically in a Form 8-K filing.
Forward-looking statements have been provided pursuant to the safe harbor provisions of the Private Securities Litigation Reform Act of 1995. Forward-looking statements involve known and unknown risks and uncertainties that may cause our actual results in future periods to differ materially from forecasted results. These risks and uncertainties may include but are not limited to, our ability to consummate acquisitions and other partnering relationships at reasonable valuations; our ability to integrate acquisitions and partnering relationships within the expected timeframes and to achieve the revenue, cost savings and earnings levels from such acquisitions and relationships at or above the levels projected; our ability to comply with the terms of our borrowing agreements; changes in governmental reimbursement rates and other regulations or policies affecting reimbursement for the services provided by us to clients and/or patients; the operational, administrative and financial effect of our compliance with other governmental regulations and applicable licensing and certification requirements; our ability to attract new client relationships or to retain and grow existing client relationships through expansion of our service offerings and the development of alternative product offerings; the future financial results of any unconsolidated affiliates; our ability to attract and the additional costs of attracting and retaining administrative, operational and professional employees; shortages of qualified therapists and other healthcare personnel; significant increases in health, workers compensation and professional and general liability costs; litigation risks of our past and future business, including our ability to predict the ultimate costs and liabilities or the disruption of our operations; competitive and regulatory effects on pricing and margins; our ability to effectively respond to fluctuations in our census levels and number of patient visits; the adequacy and effectiveness of our information systems; natural disasters and other unexpected events which could severely damage or interrupt our systems and operations; changes in federal and state income tax laws and regulations, the effectiveness of our tax planning strategies and the sustainability of our tax positions; and general and economic conditions, including efforts by governmental reimbursement programs, insurers, healthcare providers and others to contain healthcare costs.
Item 9.01 | Financial Statements and Exhibits. |
| (d) | Exhibits - See exhibit index |
SIGNATURE
Pursuant to the requirements of the Securities Exchange Act of 1934, the company has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
Dated: November 27, 2007
By: /s/ Jay W. Shreiner
Name: Jay W. Shreiner
Title: Senior Vice President and
Chief Financial Officer
EXHIBIT INDEX
99 | Investor Relations Presentation in use beginning November 27, 2007. |
Exhibit 99

Investor Presentation, Third Quarter 2007
0
About Us
RehabCare is a leading national provider of
physical rehabilitation services in conjunction with
nearly 1,250 hospitals and skilled nursing facilities
in 43 states and the District of Columbia. We also
own and/or operate 10 freestanding rehabilitation
and long-term acute care hospitals.
1
Service Lines
$720 million consolidated
revenues(1)
Contract Therapy Division
$405 million revenue - 57% of revenue (1)
1,085 skilled nursing facility programs
39 states
7.5 million annual patient visits
Hospital Rehabilitation Services Division
$169 million revenue - 23% of revenue (1)
154 hospital-based programs
31 states & DC
47,000 inpatient and skilled nursing unit discharges/year
1.0 million annual outpatient visits
$101 million revenue - 14% of revenue (1)
Freestanding Hospitals Division
6 rehabilitation hospitals, 3 LTACHs
1 rehabilitation hospital minority owned (2)
5 states (3)
462 beds (3)
6,100 annualized patient discharges (3)
Other Healthcare Services Division
$45 million revenue - 6% of revenue (1)
Phase 2 Consulting – consulting and care management for hospitals and health systems
Polaris Group – consulting for long-term care facilities
VTA Management Services – therapy and nurse staffing for New York
(1)
For twelve months ended 9/30/07
(2)
Not included in consolidated
revenues
(3)
These statistics include the
minority-owned rehab hospital
2
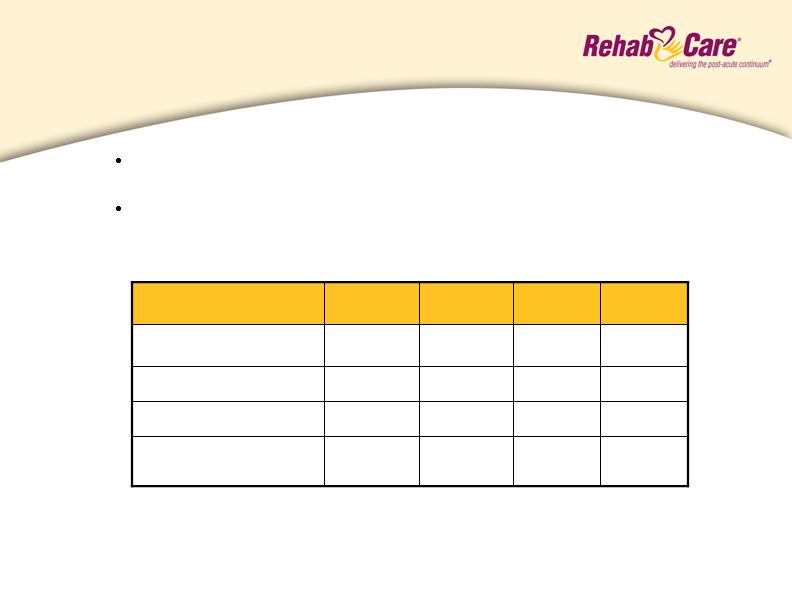
Financial Summary
$0.22
3.9
8.2
$172.9
3Q 07
$0.12(1)
2.1(1)
4.7(1)
$182.2
4Q 06
$0.12
$0.09(2)
Diluted Earnings Per
Share
2.0
1.7(2)
Net Earnings
5.5
4.2(2)
Operating Earnings
$184.0
$181.1
Operating Revenues
1Q 07
2Q 07
(dollars in millions except per
share)
(1) Includes a pretax software development impairment charge of $2.4 million, or $0.09 per diluted
share after tax
(2) Includes a pretax intangible asset impairment charge of $4.9 million ($2.9 million after tax), or $0.17
per diluted share after tax
Q3/07 operating earnings of $8.2 million and EPS of $0.22 per
diluted share, are at the highest level in the last 8 quarters
Lower operating revenues reflect elimination of programs that
don’t meet profit and credit objectives
3
Consolidated Balance Sheet
(Dollars in thousands)
Cash and Cash Equivalents
Total Assets
Total Debt
Stockholders’ Equity
Percent of Debt to Total Capital
12/31/06
9/30/07
$ 9,430
428,296
120,559
$210,779
36%
$ 14,203
425,331
100,600
$235,142
30%
Cash flow from operations totaled $30.9 million for nine
months ended September 30, 2007; $20 million debt
repaid during this period
4

Contract Therapy
Market Overview
The Contract Therapy division manages skilled nursing facility rehab programs that are
designed to provide therapy intervention to both short-stay patients and long-term residents
with a wide range of conditions, including neurological, orthopedic and other conditions
common to the geriatric patient.
Market Size
10,000 Medicare certified skilled nursing facilities
Competitive Landscape
Owned
Self-Operation
Aegis (333)
Kindred - Peoplefirst (332)
Genesis (220)
Sundance (103)
Skilled Healthcare (74)
Managed
RehabCare (1,085)
Aegis (667)
Genesis (480)
Select Medical (400)
Sundance (309)
Kindred - Peoplefirst (286)
EnduraCare (270)
Skilled Healthcare (122)
Source: Information available from public filings or from company websites
5
Contract Therapy
Performance
Q4 06
Q1 07
Q2 07
Q3 07
Dollars in millions
1,085
3.2%
$3.2
$98.3
1,197
(1.2)%
$(1.3)
$103.4
1,146
1,110
Number of Locations End
of Period
(2.2)%
1.1%
Operating Earnings
Margin
$(2.2)
$1.1
Operating Earnings (loss)
$102.8
$100.3
Operating Revenues
Outlook (assumes no unfavorable regulatory changes)
Quarterly sequential improvement in operating earnings
4.5 - 5.5% operating earnings margins during 2008
Return to net additions in locations in 2008
Operating earnings have improved sequentially
each quarter since Q1/07 with a cumulative
improvement of $5.4 million over that time period
Lower operating revenues reflect elimination of programs
that don’t meet profit and credit objectives
6
Contract Therapy
Legislative/Regulatory Environment
Part B Therapy Caps
Places annual limit on physical and speech therapy services as well as
occupational therapy services provided in non-hospital settings; exceptions
process scheduled to expire December 31, 2007
Legislative Update: House Medicare language extends exceptions process
through 2009 and requires HHS to conduct a study on a refined payment plan;
legislation currently under consideration by the Senate Finance Committee
Physician Fee Schedule (PFS)
Scheduled 9.9% reduction beginning January 2008; impacts Medicare
reimbursement for Part B services. PFS serves as the charge master for Part
B therapy
Legislative Update: House Medicare language allows 0.5% increase in
reimbursement versus a 9.9% scheduled reduction; legislation currently under
consideration by the Senate Finance Committee
For conditions most frequently treated and reimbursed under Medicare Part B, we developed a
care mapping process that ties treatment plans to cost of care. This mapping process, scheduled
for completion in December, will enable clinicians to match treatment and cost to therapy cap dollars
assisting patients to better manage their limited annual benefits.
7
Hospital Rehabilitation Services
Market Overview
Acute care hospital-based inpatient rehabilitation facilities in RehabCare’s Hospital
Rehabilitation Services (HRS) division are for patients who require early, intensive therapies (at
least 3 hours/day 5 days/week) for recovery from stroke, brain injury, neurological disorders,
amputation and other disabling injuries and illnesses. Outpatient therapy programs provide
proactive, exercise-oriented therapy with hands-on treatment for individuals of all ages.
Market Size
5,000 acute care hospitals (approximately 1,000 hospital-based IRFs)
Competitive Landscape (Acute care hospital-based IRFs)
Self-Operation
RehabCare (108)
Horizon Health (Specialty Rehab Mgmt) (23)
HealthSouth (11)
Milestone(1)
TherEx (formerly National Rehab Partners)(1)
(1) Private company or a subsidiary of a public company; number of locations is not available
Source: Information available from public filings or from company websites
8
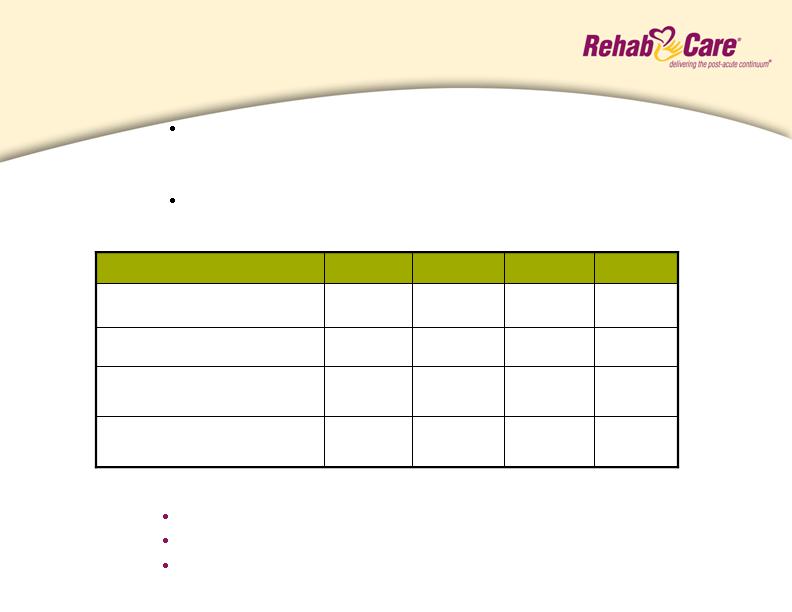
Hospital Rehab Services
Performance
Q4 06
Q1 07
Q2 07
Q3 07
Dollars in millions
10,173
154
15.7%
$6.3
$40.3
11,337
11,093
10,786
IRF Discharges
172
16.7%
$7.3
$43.8
164
161
Number of Locations End
of Period
12.0%
12.9%
Operating Earnings
Margin
$5.2
$5.4
Operating Earnings
$43.3
$41.8
Operating Revenues
Outlook
Continued modest declines in IRFs in Q4 and relatively flat same
store discharges until implementation of 75% Rule is clarified
legislatively
Continued strong operating earnings performance through
focus on controlling costs
Lower operating revenues reflect impact of the 75% Rule and
reduction in units that don’t meet profit and credit objectives
9
Hospital Rehab Services
Legislative/Regulatory Environment
Medicare Fiscal Intermediaries (FI) and Recovery Audit Contractor
Reviews (RAC)
Medical necessity reviews are growing in frequency; RHB has 90.5% overturn rate of
HRS denied claims
The Tax Relief and Healthcare Act of 2006 requires the RAC program be in place
nationwide by 2010. A demonstration project was established in 2006 for California,
Florida and New York. CMS intends to expand the program in 2008, but recently
established October 1, 2007 as earliest reach-back review date.
According to the September 2007 Moran report, IRF same store discharges for four quarters
ending Q2/07 versus four quarters ending Q2/04 declined 24.8%. On the same basis,
RehabCare discharges declined 9.7%.
For the nine months ended 3Q/07, non-Medicare discharges increased 13.1% over the same
period last year
IRF 75% Rule
Requires inpatient rehabilitation programs to maintain a minimum of 75% of their
Medicare admissions from 13 diagnostic categories. Transitioned from 60% to 65%
on July 1, 2007 with final phase-in to 75% scheduled for July 1, 2008. The comorbidity
provision (4% of RHB discharges) scheduled to expire on July 1, 2008. Division
operating at average 65% compliance.
Legislative Update: House Medicare language permanently freezes
threshold at 60% and extends the use of comorbidities; legislation
currently under consideration by the Senate Finance Committee
10
Inpatient rehabilitation facilities (IRFs) are equipped to treat patients with a wide range of
debilitating injuries and illnesses, offering inpatient and outpatient services in a home-like
environment. Long-term acute care hospitals (LTACHs) are specialty care hospitals
designed for extended stay patients with complex and chronic conditions.
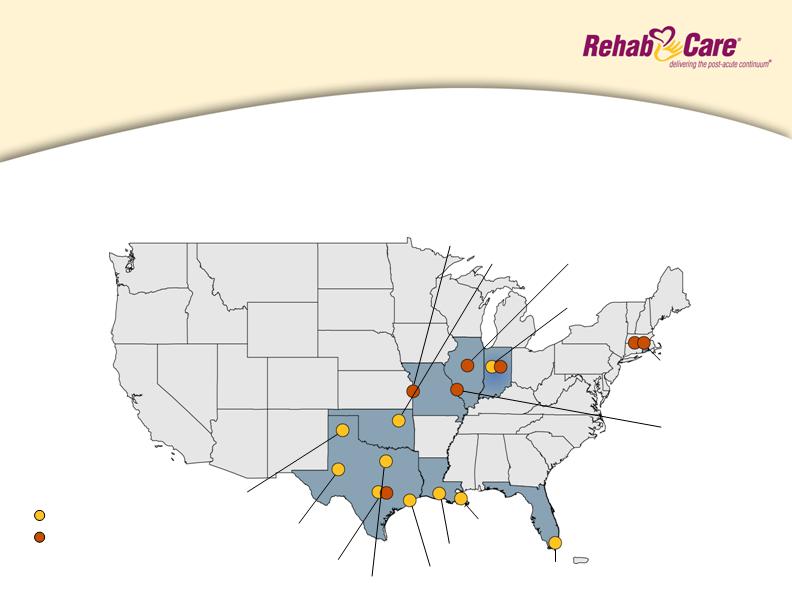
Freestanding Hospitals
Description and Locations
Tulsa, OK
Miami, FL
Arlington, TX
Houston, TX
New Orleans, LA
Amarillo, TX
Midland, TX
Austin, TX
Kokomo, IN
Lafayette, LA
Providence, RI
Peoria, IL
St. Louis, MO
N. Kansas City, MO
10 current locations
7 future locations
11
Freestanding Hospitals
Market Overview
Competitive Landscape
HealthSouth (94)
RehabCare (7)
Ernest Health (5)
Select Medical (4)
Vibra Healthcare (4)
Centerre (2)
Market Size:
240+ IRFs
Competitive Landscape
Select Medical (87)
Kindred (83)
Regency Hospital (23)
Triumph Healthcare (22)
LifeCare (20)
Vibra Healthcare (9)
HealthSouth (6)
Ernest Health (6)
RehabCare (3)
Market Size:
460+ LTACHs
Freestanding IRFs
LTACHs
Source: Information available from public filings or from company websites
12
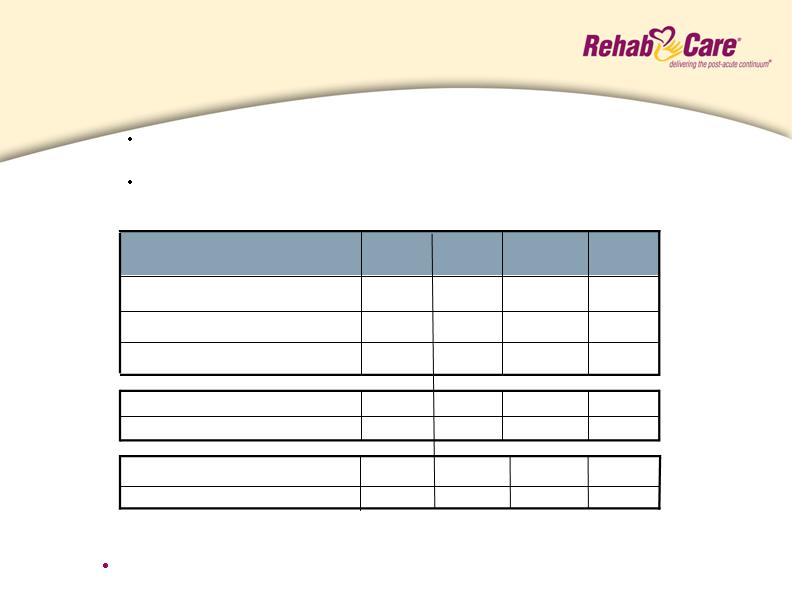
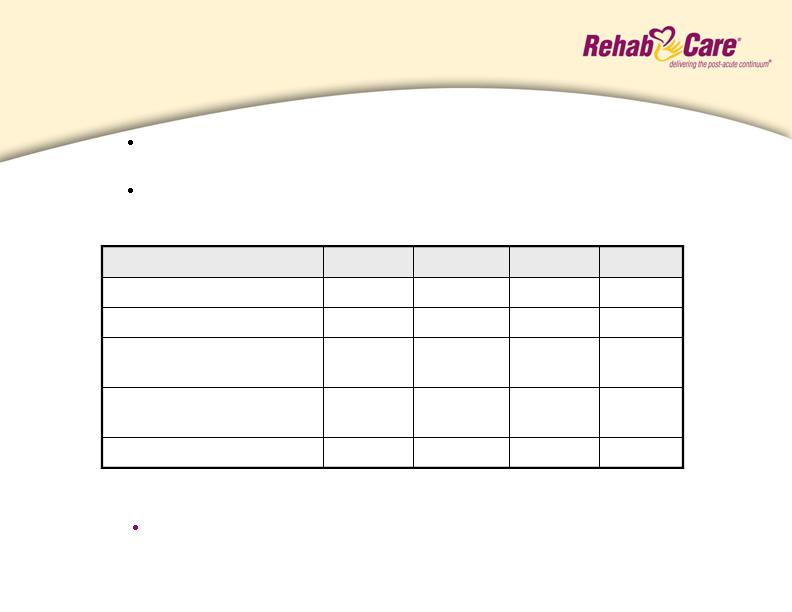
Freestanding Hospitals
Performance
Q4 06
Q1 07
Q2 07
Q3 07
Dollars in millions
386
3
1,060
6(2)
(6.7)%
$(1.6)
$24.4
398
403
380
LTACH Patient Discharges
3
3
3
Number of LTACHs End of Period
857
972
1,006
IRF Patient Discharges
5
0.1%
$0.0
$23.7
5
5
Number of IRFs End of Period
7.3%
(11.6)%
Operating Earnings Margin (loss)
$1.9
$(3.1)(1)
Operating Earnings (loss)
$26.0
$27.0
Operating Revenues
(1)
Includes a pretax impairment charge on Louisiana Specialty Hospital intangible asset of $4.9 million
(2)
Includes Central Texas Rehabilitation Hospital, which is in its Medicare demonstration period
Outlook
17-19% EBITDA margins before corporate overhead in 2008 for hospitals in
operation more than one year
Q3/07 operating revenues and operating loss impacted by $1.4 million
additional contractual reserve adjustment
Q3/07 operating results also impacted by $700,000 start-up costs
at Central Texas Rehabilitation Hospital
13
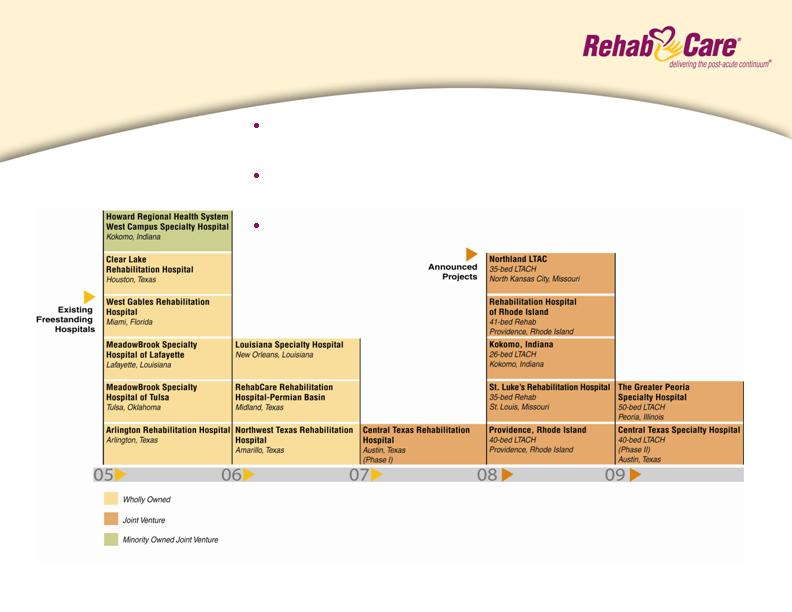
Freestanding Hospitals
Development Timeline
Division established in 2005 with the acquisition of
MeadowBrook Healthcare
10 existing hospitals, 5 in development, 1 awaiting State
Attorney General approval, 1 pending CON approval
Anticipated 4-6 new projects/year
14
Freestanding Hospitals
Legislative/Regulatory Environment
LTACH 25% Rule
3-year phase-in of rule that limits hospital-in-hospital LTACHs from receiving
no more than 25% of their admissions from a single provider; impacts
Louisiana Specialty Hospital. Mitigation strategy is currently under
development.
Legislative Update: House Medicare language prevents 25% Rule from impacting
grandfathered LTACHs, such as Louisiana Specialty, and creates specific patient
and facility admission criteria, four-year moratorium on new facilities; legislation
currently under consideration by the Senate Finance Committee
IRF 75% Rule
Freestanding Hospitals are subject to the same 75% Rule provisions as
previously discussed. Division operating at average 64% compliance.
15
Continuous Improvement
Initiatives
Intermediate
Long-Term
Open 4-6 joint ventures
annually
Standardize care
management processes
across FSH and ARUs
Implement IT roadmap for
improved clinical,
revenue cycle, and data
warehouse systems
Standardize and integrate
back office processes and
information systems
Implement centralized
support infrastructure
for FSH division
Build out continuum of
care delivery model
around key market
relationships
Implement electronic
medical record system
Continue to address
therapist supply issue
through innovation
programs like Allied
Health Research Institute
and partnerships with
the Universities of
Kansas and Missouri
2008 Initiatives
CT operating earnings
margins to 4.5% - 5.5%
HRS product development
to better match long-term
client needs
FSH EBITDA margin to
17-19% target for mature
hospitals
“Move The Mountain”
recruiting program
Roll out Patient Plus
compensation program in
CT division
16
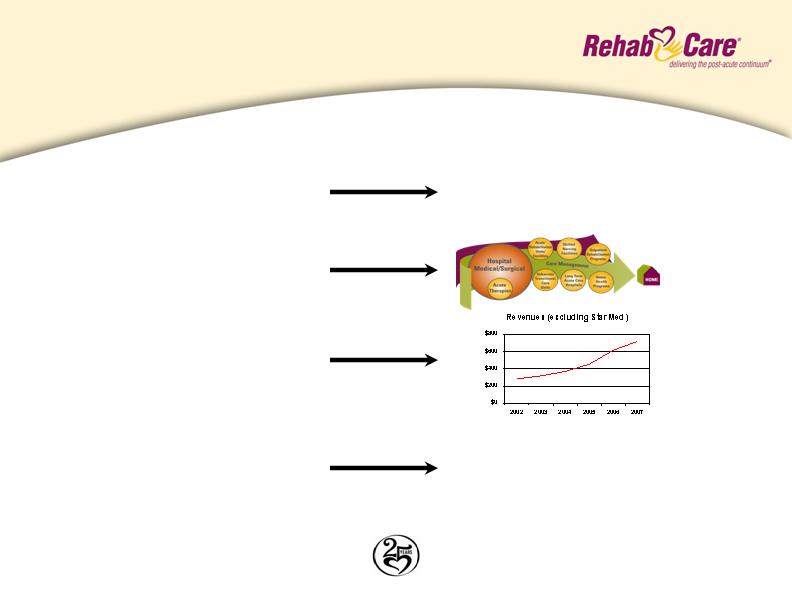
Investment Considerations
Why RehabCare?
Increasing market demand
Unique continuum of care model
Demonstrated ability to grow revenue
organically and through acquisitions
Proven ability to adapt to market
and regulatory changes
Expenditures for post-acute services:
Increase of 239% since 1998
Projected increase of 150% by 2016
Represents 12% of Medicare spending
75% rule, Part B therapy caps, LTACH
25% rule, physician fee schedule
(Annualized)
Celebrating 25 years as one of the longest tenured post-acute providers
of service in the industry
17

Safe Harbor
Forward-looking statements have been provided pursuant to the safe harbor provisions of the Private Securities Litigation Reform Act of 1995. Forward-looking statements involve known and unknown risks and uncertainties that may cause our actual results in future periods to differ materially from forecasted results. These risks and uncertainties may include but are not limited to, our ability to consummate acquisitions and other partnering relationships at reasonable valuations; our ability to integrate acquisitions and partnering relationships within the expected timeframes and to achieve the revenue, cost savings and earnings levels from such acquisitions and relationships at or above the levels projected; our ability to comply with the terms of our borrowing agreements; changes in governmental reimbursement rates and other regulations or policies affecting reimbursement for the services provided by us to clients and/or patients; the operational, administrative and financial effect of our compliance with other governmental regulations and applicable licensing and certification requirements; our ability to attract new client relationships or to retain and grow existing client relationships through expansion of our service offerings and the development of alternative product offerings; the future financial results of any unconsolidated affiliates; our ability to attract and the additional costs of attracting and retaining administrative, operational and professional employees; shortages of qualified therapists and other healthcare personnel; significant increases in health, workers compensation and professional and general liability costs; litigation risks of our past and future business, including our ability to predict the ultimate costs and liabilities or the disruption of our operations; competitive and regulatory effects on pricing and margins; our ability to effectively respond to fluctuations in our census levels and number of patient visits; the adequacy and effectiveness of our information systems; natural disasters and other unexpected events which could severely damage or interrupt our systems and operations; changes in federal and state income tax laws and regulations, the effectiveness of our tax planning strategies and the sustainability of our tax positions; and general and economic conditions, including efforts by governmental reimbursement programs, insurers, healthcare providers and others to contain healthcare costs.
18