UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM 10-K
|
| |
| R | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
| | For the Fiscal Year Ended December 31, 2012 |
| | OR |
| £ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
| | For the Transition Period From to |
Commission File Number 001-32209
WellCare Health Plans, Inc.
(Exact Name of Registrant as Specified in Its Charter)
|
| |
| Delaware | 47-0937650 |
| (State or Other Jurisdiction | (I.R.S. Employer |
| of Incorporation or Organization) | Identification No.) |
| | |
| 8725 Henderson Road, Renaissance One | |
| Tampa, Florida | 33634 |
| (Address of Principal Executive Offices) | (Zip Code) |
(813) 290-6200
Registrant's telephone number, including area code
Securities registered pursuant to Section 12(b) of the Exchange Act:
|
| |
| Common Stock, par value $0.01 per share | New York Stock Exchange |
| (Title of Class) | (Name of Each Exchange on which Registered) |
Securities registered pursuant to Section 12(g) of the Exchange Act:
NONE
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes R No £
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 of Section 15(d) of the Act. Yes £ No R
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes R No £
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Website, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§ 232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes R No £
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K (§ 229.405) is not contained herein, and will not be contained, to the best of registrant's knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. R
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of "large accelerated filer," "accelerated filer" and "smaller reporting company" in Rule 12b-2 of the Exchange Act. (Check one):
|
| | | |
Large accelerated filer R | Accelerated filer £ | Non-accelerated filer £ | Smaller reporting company £ |
| | | (Do not check if a smaller reporting company) | |
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes £ No R
The aggregate market value of Common Stock held by non-affiliates of the registrant (assuming solely for the purposes of this calculation that all directors and executive officers of the registrant are "affiliates") as of June 30, 2012 was approximately $2,270,561,000 (based on the closing sale price of the registrant's Common Stock on that date as reported on the New York Stock Exchange).
As of February 11, 2013, there were outstanding 43,215,622 shares of the registrant's Common Stock, par value $0.01 per share.
Documents Incorporated by Reference: Portions of the registrant's definitive Proxy Statement for the 2013 Annual Meeting of Stockholders are incorporated by reference into Part III of this Form 10-K.
TABLE OF CONTENTS
|
| |
| | Page |
| PART I | |
| Item 1: Business | |
| Item 1A: Risk Factors | |
| Item 1B: Unresolved Staff Comments | |
| Item 2: Properties | |
| Item 3: Legal Proceedings | |
| Item 4: Mine Safety Disclosures | |
| | |
| PART II | |
| Item 5: Market for Registrant's Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities | |
| Item 6: Selected Financial Data | |
| Item 7: Management's Discussion and Analysis of Financial Condition and Results of Operations | |
| Item 7A: Qualitative and Quantitative Disclosures About Market Risk | |
| Item 8: Financial Statements and Supplementary Data | |
| Item 9: Changes In and Disagreements With Accountants on Accounting and Financial Disclosure | |
| Item 9A: Controls and Procedures | |
| Item 9B: Other Information | |
| | |
| PART III | |
| Item 10: Directors, Executive Officers and Corporate Governance | |
| Item 11: Executive Compensation | |
| Item 12: Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters | |
| Item 13: Certain Relationships and Related Transactions, and Director Independence | |
| Item 14: Principal Accounting Fees and Services | |
| | |
| PART IV | |
| Item 15: Exhibits, Financial Statement Schedules | |
References to the "Company," "WellCare," "we," "our," and "us" in this Annual Report on Form 10-K for the fiscal year ended December 31, 2012 (the "2012 Form 10-K") refer to WellCare Health Plans, Inc., together, in each case, with our subsidiaries and any predecessor entities unless the context suggests otherwise.
FORWARD-LOOKING STATEMENTS
Statements contained in this 2012 Form 10-K which are not historical fact may be forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995 and Section 21E of the Exchange Act, and we intend such statements to be covered by the safe harbor provisions for forward-looking statements contained therein. Such statements, which may address, among other things, market acceptance of our products and services, product development, our ability to finance growth opportunities, our ability to respond to changes in laws and government regulations, implementation of our sales and marketing strategies, projected capital expenditures, liquidity and the availability of additional funding sources may be found in the sections of this 2012 Form 10-K entitled "Business," "Risk Factors," "Management's Discussion and Analysis of Financial Condition and Results of Operations" and elsewhere in this report generally. In some cases, you can identify forward-looking statements by terminology such as "may," "will," "should," "expects," "plans," "anticipates," "believes," "estimates," "targets," "predicts," "potential," "continues" or the negative of such terms or other comparable terminology. You are cautioned that forward-looking statements involve risks and uncertainties, including economic, regulatory, competitive and other factors that may affect our business. These forward-looking statements are inherently susceptible to uncertainty and changes in circumstances, as they are based on management's current expectations and beliefs about future events and circumstances. We undertake no obligation beyond that required by law to update publicly any forward-looking statements for any reason, even if new information becomes available or other events occur in the future.
Our actual results may differ materially from those indicated by forward-looking statements as a result of various important factors including the expiration, cancellation or suspension of our state and federal contracts. In addition, our results of operations and estimates of future earnings depend, in large part, on accurately predicting and effectively managing health benefits and other operating expenses. A variety of factors, including competition, changes in health care practices, changes in federal or state laws and regulations or their interpretations, inflation, provider contract changes, changes or suspensions or terminations of our contracts with government agencies, new technologies, government-imposed surcharges, taxes or assessments, reductions in provider payments by governmental payors, major epidemics, disasters and numerous other factors affecting the delivery and cost of health care, such as major health care providers' inability to maintain their operations, may affect our ability to control our medical costs and other operating expenses. Governmental action or inaction could result in premium revenues not increasing to offset any increase in medical costs or other operating expenses. Once set, premiums are generally fixed for one-year periods and, accordingly, unanticipated costs during such periods generally cannot be recovered through higher premiums. Furthermore, if we are unable to estimate accurately incurred but not reported medical costs in the current period, our future profitability may be affected. Due to these factors and risks, we cannot provide any assurance regarding our future premium levels or our ability to control our future medical costs.
From time to time, at the federal and state government levels, legislative and regulatory proposals have been made related to, or potentially affecting, the health care industry, including but not limited to limitations on managed care organizations, including benefit mandates, and reform of the Medicaid and Medicare programs. Any such legislative or regulatory action, including benefit mandates or reform of the Medicaid and Medicare programs, could have the effect of reducing the premiums paid to us by governmental programs, increasing our medical and administrative costs or requiring us to materially alter the manner in which we operate. We are unable to predict the specific content of any future legislation, action or regulation that may be enacted or when any such future legislation or regulation will be adopted. Therefore, we cannot predict accurately the effect or ramifications of such future legislation, action or regulation on our business.
PART I
Item 1. Business.
OVERVIEW
We are a leading provider of managed care services to government-sponsored health care programs, focusing on Medicaid and Medicare. Headquartered in Tampa, Florida, we offer a variety of health plans for families, children, and the aged, blind and disabled, as well as prescription drug plans. As of December 31, 2012, we served approximately 2.7 million members nationwide. We believe that our broad range of experience and exclusive government focus allows us to effectively serve our members, partner with our providers and government clients, and efficiently manage our ongoing operations.
As of December 31, 2012, we operated Medicaid health plans in Florida, Georgia, Hawaii, Illinois, Kentucky, New York and Ohio. We also operated our Medicare Advantage ("MA") coordinated care plans ("CCPs") in California, Connecticut, Florida, Georgia, Hawaii, Illinois, Louisiana, Missouri, New Jersey, New York, Ohio and Texas, as well as a stand-alone Medicare prescription drug plan ("PDP") in 49 states and the District of Columbia. Effective as of January 1, 2013, we began serving Medicare members in Arizona as a result of our acquisition of certain assets of Desert Canyon Community Care from Humana, Inc. Effective as of February 1, 2013, we began serving Medicaid members in South Carolina as a result of our acquisition of UnitedHealth Group, Incorporated's South Carolina subsidiary. See further discussion below under "Acquisitions".
All of our Medicare plans are offered under the WellCare name, for which we hold a federal trademark registration, with the exception of our Hawaii CCP, California CCP, and Arizona CCP, which we respectively offer under the name 'Ohana, Easy Choice and Desert Canyon Community Care. For our Medicaid plans, we offer a number of brand names depending on the state, consisting of the Staywell and HealthEase brands in Florida, the 'Ohana brand in Hawaii, the Harmony brand name in Illinois and the WellCare brand name in Georgia, Kentucky, New York and Ohio.
A "managed care" plan can be defined as an integrated system that manages health care services for an enrolled population rather than simply providing or paying for them. Services within managed care plans are usually delivered by providers who are under contract to, or employed by, the plan. Managed care plans use a variety of approaches to "manage" care, including care management, capitation, risk-sharing or incentive-based arrangements with providers, the use of primary care physicians to act as primary care gatekeepers and the use of preferred provider networks.
We were formed in May 2002 when we acquired our Florida, New York and Connecticut health plans. From inception to July 2004, we operated through a holding company that was a Delaware limited liability company. In July 2004, immediately prior to the closing of our initial public offering, the limited liability company was merged into a Delaware corporation and we changed our name to WellCare Health Plans, Inc.
In the following table, we have summarized membership for our business segments in each state that exceeds 5% of our total membership, as well as all other states in the aggregate, as of December 31, 2012.
|
| | | | | | | | | | | | | | |
| | | | Medicare Membership | | Total Membership | | Percent of Total Membership |
| State | Medicaid | | MA | | PDP | | |
| Georgia | 570,000 |
| | 19,000 |
| | 31,000 |
| | 620,000 |
| | 23.3 | % |
| Florida | 454,000 |
| | 68,000 |
| | 34,000 |
| | 556,000 |
| | 20.8 | % |
| California | — |
| | 39,000 |
| | 260,000 |
| | 299,000 |
| | 11.2 | % |
| Kentucky | 207,000 |
| | — |
| | 15,000 |
| | 222,000 |
| | 8.3 | % |
| Illinois | 141,000 |
| | 12,000 |
| | 23,000 |
| | 176,000 |
| | 6.6 | % |
| New York | 84,000 |
| | 31,000 |
| | 41,000 |
| | 156,000 |
| | 5.8 | % |
| All other states (1) | 131,000 |
| | 44,000 |
| | 465,000 |
| | 640,000 |
| | 24.0 | % |
| Total | 1,587,000 |
| | 213,000 |
| | 869,000 |
| | 2,669,000 |
| | 100.0 | % |
| |
| (1) | Represents the aggregate of all states that individually have less than 5% of total membership. |
Acquisitions
In January 2013, we entered into an agreement to acquire Missouri Care, Inc., a subsidiary of Aetna, Inc. ("Missouri Care"). As of December 2012, Missouri Care served more than 100,000 Missouri HealthNet Medicaid program members in 54 counties across the state. Missouri Care has an extensive provider network that includes more than 50 hospitals and 9,500 physicians. The transaction is subject to regulatory approvals and certain other closing conditions. We anticipate that the transaction will close in the first half of 2013.
In January 2013, we acquired UnitedHealthcare's Medicaid business in South Carolina from UnitedHealth Group Incorporated. As of January 2013, UnitedHealthcare's Medicaid business in South Carolina served members in 39 of the state's 46 counties, including the Columbia and Greenville metropolitan areas, through the South Carolina Healthy Connections Choices program. It has a network that includes more than 30 hospitals, 1,800 primary care physicians, and 2,000 specialists.
In December 2012, we acquired certain assets of Arcadian Health Plan, Inc.'s Desert Canyon Community Care ("Desert Canyon") MA plans from Humana, Inc. Approximately 4,000 Desert Canyon plan members in Mohave and Yavapai Counties became members of our Arizona MA health plan on January 1, 2013.
In November 2012, we acquired all outstanding interests in America's 1st Choice California Holdings, LLC, the sole shareholder of Easy Choice Health Plan, Inc. ("Easy Choice"). As of December 2012, Easy Choice served approximately 39,000 MA plan members in the Los Angeles, Orange, Riverside, and San Bernardino Counties in Southern California. This includes approximately 12,000 MA dual special needs plan ("D-SNP") members, making Easy Choice one of the largest D-SNPs in Los Angeles County. Easy Choice increased its 2013 service area to 11 California counties, including the San Diego area and five counties in northern California. More than 60% of California's 5 million Medicare eligibles reside in these counties. In addition, in 2013, Easy Choice began offering MA chronic condition special needs plans in five of the 11 counties in its service area. The Easy Choice acquisition provides us with a presence in a new and attractive market, and gives us a platform for meaningful growth in the western United States across our complementary lines of business. Additionally, Easy Choice's D-SNP membership dovetails with our strategy to focus on this population.
OUR VISION AND STRATEGY
We operate exclusively within the Medicare, Medicaid and Medicaid-related programs, serving the full spectrum of eligibility groups, with a focus on lower-income beneficiaries. We are committed to operating our business in a manner that serves our key constituents – members, providers, government customers, and associates – while delivering competitive returns for our investors.
Vision
Our vision is to be the leader in government-sponsored health care programs in partnership with the members, providers, governments and communities we serve.
Mission
Our primary mission is to:
| |
| • | Enhance our members' health and quality of life; |
| |
| • | Partner with providers and governments to provide cost-effective health care solutions, while improving health care quality and access; and |
| |
| • | Create a rewarding and enriching environment for our associates. |
We have defined three long-term strategic priorities:
| |
| • | Improving health care quality and access; |
| |
| • | Achieving a competitive cost structure for administrative and medical expenses; and |
| |
| • | Delivering prudent, profitable growth. |
Improving health care quality and access
We work closely with providers and government clients to further enhance health care delivery and improve the quality of, and access to, health care services for our members. We are focused on preventive health, wellness and care management programs that help governments provide quality care within their fiscal constraints and present us with long-term opportunities for prudent and profitable growth.
Achieving a competitive cost structure for administrative and medical expenses
Our cost management initiatives are concentrated on aligning our expense structure with our current revenue base through process improvement and other initiatives, focusing on ensuring a competitive cost structure in terms of both administrative and medical expenses. We continually assess opportunities to improve the efficiency and effectiveness of our administrative processes. In addition, as part of our medical expense initiatives, we have implemented provider contracting, case and disease management and pharmacy initiatives.
Delivering prudent and profitable growth
Our strategy for growth primarily entails entering new markets to pursue attractive opportunities for our product lines and may include an assessment of potential acquisitions that would complement our strategy, existing geographic markets, and product mix. After establishing a presence, we leverage that infrastructure to further establish our presence in the marketplace to pursue geographic expansion, product expansion or both.
For a list of key developments and accomplishments relating to progress on our strategic business priorities that occurred or impacted our financial condition and results of operations during 2012, and in the 2013 period prior to issuance of this 2012 Annual Report on Form 10-K, please see Item 7 – Management's Discussion and Analysis of Financial Condition and Results of Operations, Key Developments and Accomplishments.
MEDICARE AND MEDICAID HEALTH CARE PROGRAMS
The Congressional Budget Office ("CBO") estimated that in June 2012, approximately 55 million people were covered by the joint state and federally funded Medicaid program and approximately 50 million people were covered by the federally funded Medicare program. Of these, approximately 8 million people were dual-eligibles. In addition in 2010, approximately 8 million people were covered by the joint state and federally funded Children's Health Insurance Program ("CHIP") program.
Medicare
Medicare is a federal health insurance program that provides eligible persons age 65 and over, and some disabled persons under the age of 65, certain hospital, medical and prescription drug benefits. Medicare is federally administered by the Centers for Medicare and Medicaid Services ("CMS"). The Medicare program consists of four parts, labeled Parts A-D.
| |
| • | Part A—Hospitalization benefits are provided under Part A. These benefits are financed largely through Social Security taxes. Beneficiaries are not required to pay any premium for Part A benefits. However, they are still required to pay out-of-pocket deductibles and coinsurance. |
| |
| • | Part B—Benefits for medically necessary services and supplies including outpatient care, doctor's services, physical or occupational therapists and home health care are provided under Part B. Beneficiaries enrolled in Part B are required to pay monthly premiums and are subject to an annual deductible. |
The Part A and B programs are referred to as Original Medicare. Since the 1970s, Medicare beneficiaries have had the option to receive their Medicare benefits through private health plans, mainly health maintenance organizations ("HMOs"), as an alternative to Original Medicare. The Balanced Budget Act of 1997 named Medicare's managed care program "Medicare+Choice" and in 2003 it was renamed as MA under the Medicare Modernization Act ("MMA"). In geographic areas where a managed care organization has contracted with CMS pursuant to the MA program, Medicare beneficiaries may choose to receive benefits from a MA organization under Medicare Part C.
| |
| • | Part C—Under the MA program, private plans provide benefits to enrollees that are at least comparable to those offered under Original Medicare and can include prescription drug coverage. Part C benefits are provided through HMOs, preferred provider organizations ("PPOs") and private fee-for-service ("PFFS") plans. MA plans may charge beneficiaries monthly premiums and other copayments for Medicare-covered services or for certain extra benefits. |
| |
| • | Part D—Under Part D, which was established in 2003 by the Medicare Modernization Act ("MMA"), prescription drug benefits are offered by MA plans. Effective January 1, 2006, stand-alone PDP plans could also be offered to individuals eligible for benefits under Part A and/or enrolled in Part B. Plans can include varying degrees of out-of-pocket costs for premiums, deductibles and coinsurance. |
Depending on medical coverage type, a beneficiary has various options for accessing drug coverage. Beneficiaries enrolled in Original Medicare can either join a stand-alone PDP or forgo Part D drug coverage. Beneficiaries enrolled in MA CCPs can join a plan with Part D coverage, select a stand-alone PDP or forgo Part D coverage. Dually-eligible beneficiaries, and certain beneficiaries who qualify for the low-income subsidy ("LIS") but do not enroll themselves in a PDP, are automatically assigned to a plan by CMS. These assignments are made amongst those PDPs which submitted bids below the applicable regional benchmarks for standard plans.
In 2012, projected Medicare spending was $556 billion, with more than 20% for Medicare Advantage. According to a January 2013 report by the Department of Health and Human Services ("HHS"), the number of Medicare beneficiaries is projected to grow at approximately 3% annually as a result of the aging of the U.S. population. Consequently, Medicare spending, including premiums to Medicare Advantage plans, is expected to grow significantly as baby boomers retire. In fact, according to the CBO, total Medicare spending is projected to double to approximately $1.1 trillion in 2022 due to growth in Medicare beneficiaries and sustained increases in health care costs.
In 2012, the majority of the 50 million people on Medicare were in the traditional Medicare program, with 27% enrolled in a MA plan. Since 2004, the number of beneficiaries enrolled in private plans has more than doubled from 5.3 million to 13.1 million in 2012. MA enrollment rates vary by state, ranging from 46% in Minnesota to less than 1% in Alaska, and vary within states by county.
Medicaid
Medicaid was established to provide medical assistance to low-income and disabled persons. It is state operated and implemented, although it is funded and regulated by both the state and federal governments. Within broad federal guidelines, each state may define its own package of covered medical services, resulting in considerable variation in the types of services covered and the amount of care provided across states. Our Medicaid segment includes plans for beneficiaries of Temporary Assistance for Needy Families ("TANF"), Supplemental Security Income ("SSI"), Aged Blind and Disabled ("ABD") and other state-based programs that are not part of the Medicaid program, such as CHIP, Family Health Plus ("FHP") and Managed Long-Term Care ("MLTC") programs. TANF generally provides assistance to low-income families with children; ABD and SSI generally provide assistance to low-income aged, blind or disabled individuals. CHIP and FHP programs provide assistance to qualifying families who are not eligible for Medicaid because their income exceeds the applicable income thresholds. The MLTC program is designed to help people with chronic illnesses or who have disabilities and need health and long-term care services, such as home care or adult day care, to enable them to stay in their homes and communities as long as possible.
CMS estimates total Medicaid spending in 2012 at approximately $459 billion, increasing to $491 billion in 2013. Approximately 57% of Medicaid funding comes from the federal government, with the remainder coming from state governments. Due to the Medicaid expansion provisions under the Patient Protection and Affordable Care Act and the Health Care and Education Reconciliation Act of 2010 (collectively, the "2010 Acts") passed in March 2010 (as discussed below), it is projected that Medicaid expenditures will increase an additional $1 trillion through 2022, with the federal government paying approximately 93% of these costs. Medicaid continues to be one of the fastest-growing and largest components of states' budgets. According to a report by the National Association of State Budget Officers in December 2012, Medicaid spending represented approximately 24% on average of a state's budget, and state spending for Medicaid grew an estimated 16% in 2012, as the portion of federal government funds declined.
Macroeconomic conditions in recent years have, and are expected to continue to, put pressure on state budgets as the Medicaid eligible population increases, creating more need and competing for funding with other state priorities. As Medicaid consumes more and more of the states' limited dollars, states must either increase their tax revenues or reduce their total costs. Since states are limited in their ability to increase their tax revenues, states often look to reduce costs by reducing funds allotted for Medicaid or finding ways to control rising Medicaid costs, which may include reducing premium rates or imposing further restrictions on beneficiary eligibility. We believe that the most effective way to control rising Medicaid costs is through managed care.
States have traditionally provided Medicaid benefits using a fee-for-service system. However, states are now more frequently implementing a managed care delivery system for Medicaid benefits. In a managed care delivery system, people get most or all of their Medicaid services from an organization under contract with the state. According to the Kaiser Family Foundation, in 2012 all states except Alaska, New Hampshire and Wyoming have implemented comprehensive managed care programs. However, New Hampshire is currently in the process of implementing a statewide managed care program. Approximately two-thirds of all Medicaid beneficiaries are in some form of a managed care arrangement, either on a voluntary or mandatory basis. With the passage of health care reform legislation (as discussed below), states will expand coverage under the Medicaid program to an estimated 7 million people in 2014, which will increase to 12 million in 2022, according to the Congressional Budget Office. Expansion of Medicaid is likely to increase the number of people enrolled in and the amount of spending for managed care. Accordingly, the opportunity for growth in managed care may be significant.
Dual-eligibles
Those qualifying for both Medicare and Medicaid are defined as "dual-eligibles". For dual-eligibles, if a service is covered by Medicare and Medicaid, Medicare is the primary payer. Medicaid pays for services above and beyond what Medicare covers, which is often referred to as wrap-around coverage. Medicaid may also cover some beneficiary cost-sharing associated with particular Medicare services. For Medicaid benefits that are not covered by Medicare, such as certain long-term care services, Medicaid covers the cost of these benefits unless there is another liable third-party payer. Medicaid is generally the payer of last resort. The Medicare and Medicaid services that dual-eligibles receive do not blend seamlessly with one another. The programs often have different eligibility requirements or scope of coverage for the same (or similar) services. Fragmentation can result in providers lacking information about the full range of services someone receives (which could compromise health care decision-making); beneficiary confusion; cost inefficiencies in Medicare and Medicaid; and poorer quality of care and health care outcomes for the beneficiary.
There are approximately 8.3 million dual-eligibles according to CMS, and Federal and state governments spend approximately $300 billion annually on the dual-eligible population and according to CMS, they make up 17% of Medicaid enrollees but incur 39% of its expenses. Presently, only 12%-15% of dual-eligibles are covered by private health plans. It is imperative to enhance care options for dual-eligibles as the numbers are expected to shoot up with an aging population and increased life expectancy among Americans with disabilities. As such, dual-eligibles have become an immediate target for spending reductions and quality improvements in care. The 2010 Acts created a federal Medicare-Medicaid Coordination Office to serve dual-eligibles. This Medicare-Medicaid Coordination Office has initiated a series of state demonstration projects intended to provide better coordination and integration of care between Medicare and Medicaid on a capitated or fee for service basis, which is required to produce cost savings ("Duals Alignment Demonstration Program").
As of January 2013, three states have executed Memorandums of Agreement with CMS to participate in the program, a key step in demonstration implementation, and eighteen states are still negotiating with CMS on their demonstration parameters. CMS has issued guidance that no programs will begin before April 1, 2013 and the target enrollment will be limited to 1 to 2 million beneficiaries. Exact implementation times vary by state. CMS has issued guidance indicating that dual-eligible beneficiaries participating in the states' Duals Alignment Demonstration Programs cannot be forced to remain in a duals alignment plan and will be allowed to switch between plans on a monthly basis. However, enrollment in a MA plan is limited to the federally designated annual enrollment period or in the event of a special election period unless the individual seeks to enroll in a plan that has obtained a score of 5 on Medicare's quality performance system ("Star Ratings"). None of our health plans have yet achieved 5 stars. For this reason, dual-eligible beneficiaries subject to a dual alignment demonstration programs will only be able to elect to remain in or join a WellCare plan during the annual enrollment period or special election periods.
The guidance promulgated by CMS requires a cost savings to both Medicare and Medicaid. To the extent that the assumed savings are deemed unrealistic, these programs could limit the number of states in which we choose to provide services. If the rates are deemed sufficient to support the provision of high quality care, we may choose to bid for participation in these programs.
In addition, certain states' programs have not permitted us to participate, since those states require plans to be licensed as a Medicaid provider or restrict participation to fee for service programs. For those states that have a Duals-Eligible Demonstration Program in which we do not participate, the membership in our MA and PDP plans in those states would be reduced. Per CMS guidance, Part D auto assignments to another PDP will be limited to January 1, 2014, and January 1, 2015, for 2013 and 2014 demonstration states, respectively.
General Economic and Political Environment Impacting our Business
The U.S. health care economy currently comprises approximately 18% of the U.S. gross domestic product, according to CMS. We expect overall spending on health care in the U.S. to continue to rise due to inflation, medical technology and pharmaceutical advancement, regulatory requirements, demographic trends in the U.S. population and national interest in health and well-being. The rate of market growth may be affected by a variety of factors, including macro-economic conditions and enacted health care reforms, which could also impact our results of operations.
The general economic environment remains challenging, with continued high unemployment throughout 2012 and sluggish job growth. During an economic downturn individuals lose jobs and their incomes decline, more individuals qualify and enroll in Medicaid which increases program spending. At the same time, increases in unemployment have a negative impact on state tax revenues, which could make it more difficult for states to pay their share of Medicaid spending increases. As a result, budgetary challenges at the federal and state level may continue. We expect that the state and federal governments will continue to look for budgetary cost control savings through reductions in health care costs. We may also experience delays in premium payments from our state customers. The "maintenance of effort" requirements under the 2010 Acts generally prohibit states from restricting Medicaid eligibility or tightening enrollment procedures. These provisions are due to phase out for adults in Medicaid in 2014 and for children in 2019. However, the 2012 Supreme Court decision regarding the 2010 Acts has created some uncertainty regarding whether the maintenance of effort provisions can be enforced. In the event that they cannot, states could seek to restrict eligibility or tighten enrollment procedures.
The political environment is uncertain. Although the President signed into law the Budget Control Act of 2011 on August 2, 2011, the Congressional Super Committee failed to reach an agreement on a budget. On January 2, 2013, President Obama signed the American Taxpayer Relief Act of 2012 delaying the imposition of sequestration until March 2013. As a result, in the absence of Congressional intervention, approximately $1.2 trillion in domestic and defense spending reductions would begin in March 2013. The Budget Control Act of 2011 stipulates that payments to Medicare providers may be reduced by no more than 2% and exempts Medicaid from the automatic spending cuts. At this time, we cannot predict the impact of this pending legislation.
Because the rate of growth of Medicare expenses is outpacing the growth rate of the economy, and the trust funds are not adequately funded, Congress has proposed several plans to cut or restructure Medicare including raising the Medicare eligibility age, moving Medicare to a defined contribution model and various cuts to provider reimbursement. Medicaid is similarly situated, consuming ever greater portions of the federal budget. As a result, several programs have been offered to modify the Medicaid program including moving from a match program to a block grant, moving to a per-capita system, and limiting the use of provider taxes to fund the state's portion of the Medicaid program. We do not know whether these proposals will pass, or the impact the ultimate reform will have on our business.
In addition, Congress has annually appropriated funds to avoid the imposition of the Sustainable Growth Rate formula, enacted by the Balanced Budget Act of 1997, on physician payments under Medicare. The cut to physician payments that would result from the imposition of the Sustainable Growth Rate formula would be approximately 25% at the start of 2014. The cuts could have a significant impact on health care provider willingness to participate in Medicare programs. Congress has not yet appropriated funds for these payments for 2014 and may fail to do so, or may delay doing so which could cause delays in receipt of payments from CMS for our MA plans.
Health Care Reform
In March 2010, the 2010 Acts became law and significantly reformed various aspects of the U.S. health insurance industry. Financing for these reforms will come in part from substantial additional fees and taxes on us and other health insurers, health plans and individuals beginning in 2014, as well as reductions in certain levels of payments to us and other health plans under Medicare. While regulations and interpretive guidance on some provisions of the 2010 Acts have been issued to date by the HHS, the Department of Labor, the Treasury Department, and the National Association of Insurance Commissioners ("NAIC"), there are many significant provisions of the legislation that will require additional guidance and clarification in the form of regulations and interpretations in order to fully understand the impact of this legislation on our overall business, which we expect to occur over the next several years.
The 2010 Acts include a number of changes to the way MA plans are operating, or will operate, such as:
| |
| • | Reduced Enrollment Period. Medicare beneficiaries generally have a limited annual enrollment period during which they can choose to participate in a MA plan rather than receive benefits under the traditional fee-for-service Medicare program. After the annual enrollment period, most Medicare beneficiaries are not permitted to change their Medicare benefits until the following annual enrollment period. Beginning with the 2012 plan year, the 2010 Acts changed the annual enrollment period, which now begins in mid-October and ends in early December. Previously, open enrollment was from November 15 to December 31. Also beginning on January 1, 2011, the 2010 Acts began mandating that persons enrolled in MA may disenroll only during the first 45 days of the year and only may enroll in traditional Medicare fee-for-service rather than another MA plan. Prior law allowed a member to disenroll during the first 90 days of the year and enroll in another MA plan. |
| |
| • | Reduced Medicare Premium Rates. In 2012, MA plans received a range of 95% of Medicare fee-for-service costs in high-cost areas to 115% of Medicare fee-for-service costs in low-cost areas, with changes being phased-in over two to six years, depending on the level of payment reduction in a county. |
| |
| • | CMS Star Ratings. Certain provisions in the 2010 Acts tie MA premiums to the achievement of certain quality performance measures ("Star Ratings"). Beginning in 2012, MA plans with an overall Star Rating of three or more stars (out of five) became eligible for a quality bonus in their basic premium rates. Initially, quality bonuses were limited to the few plans that achieved four or more stars as an overall rating, but CMS has expanded the quality bonus to three star plans for a three-year period through 2014. Members of Congress have challenged whether CMS had the authority to expand the quality bonus. We cannot predict the ultimate resolution of this matter or the impact on our plans' quality bonus eligibility. Plans that receive quality bonuses may have a competitive advantage in the Medicare market, as they may be able to offer more attractive benefit packages to members and/or achieve higher profit margins. Also, beginning with open enrollment for the 2014 plan year, Part C or Part D Medicare plans with Star Ratings of less than three stars for three consecutive years will be excluded from mention in the CMS "Medicare and You" handbook, denoted as "low performing" plans on the CMS website, and excluded from on-line enrollment through the Medicare Plan Finder website. These actions may adversely impact these plans' ability to maintain or increase membership. In addition, in April 2012, CMS announced that Part C and Part D Medicare plans with an overall Star Rating of less than three stars for three consecutive years may be terminated at CMS' discretion beginning on January 1, 2015. |
| |
| • | Minimum MLRs. Beginning in 2014, the 2010 Acts require the establishment of a minimum medical loss ratio ("minimum MLR") for MA plans, requiring them to spend not less than 85% of premiums on medical benefits. While HHS has issued rules clarifying the definitions and minimum MLR requirements for certain commercial health plans, it has not issued rules or guidance specific to MA plans. The rules that have been issued impose financial and other penalties for failing to achieve the minimum MLR, including requirements to refund to CMS shortfalls in amounts spent on medical benefits and termination of a plan's MA contract for prolonged failure to achieve the minimum MLR. MLR is determined by adding a plan's total reimbursement for clinical services plus its total spending on quality improvement activities and dividing the total by earned premiums (after subtracting specific identified taxes and other fees). However, there can be no assurance that CMS will interpret the minimum MLR requirement in the same manner for MA plans. CMS is considering imposing the minimum MLR on Part D plans as well. |
With respect to PDPs, beginning in 2010 through 2020, the "coverage gap" (i.e., the dollar threshold at which an individual has to pay full price for his or her medications) will be gradually closed, with beneficiaries retaining a 25% co-pay. While this change ultimately results in increased insurance coverage, such improved benefits could result in changes in member behavior with respect to drug utilization. Such actions could also impact the cost structure of our PDPs.
The health reforms in the 2010 Acts present both challenges and opportunities for Medicaid plans. The reforms expand the eligibility for Medicaid programs. However, state budgets continue to be strained due to economic conditions and uncertain levels of federal financing for current populations. As a result, the effects of any potential future expansions are uncertain, making it difficult to determine whether the net impact of the 2010 Acts will be positive or negative for Medicaid plans.
Additionally, the 2010 Acts will impose certain new taxes and fees, including limitations on the amount of compensation that is tax deductible and annual premium-based assessments on the insurance industry, worth approximately $8 billion beginning in 2014, with increasing annual amounts thereafter. The assessments will impact margins and will not be deductible for income tax purposes. If plans are unable to adjust their business model to address this new tax, it may have a material adverse effect on our results of operations, financial position, and cash flows.
On June 28, 2012, the U.S. Supreme Court upheld the constitutionality of the provisions in the 2010 Acts requiring all Americans meeting certain income qualifications to purchase health insurance meeting certain standards or to pay a financial penalty ("the individual mandate"). The Supreme Court made the expansion of the states' Medicaid programs to individuals with incomes up to 133% of the federal poverty line optional; however, the effect of the modification to the Medicaid expansion requirements remains to be seen. We expect some, but not all, of the states we operate in will participate in the Medicaid expansion. States also have the option to create state-based exchanges. As of January 7, 2013, 24 states and the District of Columbia have submitted applications or letters of intent to run part or all of their health insurance marketplaces. Seventeen states and the District of Columbia have received conditional approval to operate state-based exchanges; two states have received conditional approval to run partnership exchanges with the federal government. February 15, 2013 is the deadline for states to notify the federal government of their intent to run a partnership exchange.
As discussed above, implementing regulations and related interpretive guidance continue to be issued on several significant provisions of the 2010 Acts. Given the breadth of possible changes and the uncertainties of interpretation, implementation and timing of these changes, which we expect to occur over the next several years, the 2010 Acts could change the way we do business, potentially impacting our pricing, benefit design, product mix, geographic mix, and distribution channels. The response of other companies to the 2010 Acts and adjustments to their offerings, if any, could have a meaningful impact on the health care markets. Further, various health insurance reform proposals are also emerging at the state level. It is reasonably possible that regulations related to the 2010 Acts, as well as future legislative changes, in the aggregate may have a material adverse effect on our results of operations, financial position, and cash flows by restricting revenue, enrollment and premium growth in certain products and market segments; restricting our ability to expand into new markets; increasing our medical and administrative costs; lowering our Medicare payment rates and/or increasing our expenses associated with the non-deductible federal premium-based assessment and other assessments.
OUR PRODUCT SEGMENTS
Our operations are conducted in three business segments: Medicaid, MA and PDP, which correspond with the Medicaid and Medicare products that we offer. Membership by segment, and as a percentage of consolidated totals, is as follows.
|
| | | | | | | | | | | | | | | | | |
| | For the Years Ended December 31, |
| | 2012 | | 2011 | | 2010 |
| Segment | Membership | | Percentage of Total | | Membership | | Percentage of Total | | Membership | | Percentage of Total |
| Medicaid | 1,587,000 |
| | 59.5 | % | | 1,451,000 |
| | 56.6 | % | | 1,340,000 |
| | 60.3 | % |
| MA | 213,000 |
| | 8.0 | % | | 135,000 |
| | 5.3 | % | | 116,000 |
| | 5.2 | % |
| PDP | 869,000 |
| | 32.5 | % | | 976,000 |
| | 38.1 | % | | 768,000 |
| | 34.5 | % |
| Total | 2,669,000 |
| | 100.0 | % | | 2,562,000 |
| | 100.0 | % | | 2,224,000 |
| | 100.0 | % |
Premium revenue by segment, and as a percentage of consolidated totals, is as follows.
|
| | | | | | | | | | | | | | | | | | | | |
| | For the Years Ended December 31, |
| | 2012 | | 2011 | | 2010 |
| Segment | Premium Revenue (In Millions) | | Percentage of Total | | Premium Revenue (In Millions) | | Percentage of Total | | Premium Revenue (In Millions) | | Percentage of Total |
| Medicaid | $ | 4,471.2 |
| | 60.4 | % | | $ | 3,581.5 |
| | 58.7 | % | | $ | 3,308.8 |
| | 60.9 | % |
| MA | 1,936.4 |
| | 26.2 | % | | 1,479.8 |
| | 24.3 | % | | 1,336.1 |
| | 24.6 | % |
| PDP | 992.6 |
| | 13.4 | % | | 1,036.8 |
| | 17.0 | % | | 785.3 |
| | 14.5 | % |
| Total | $ | 7,400.2 |
| | 100.0 | % | | $ | 6,098.1 |
| | 100.0 | % | | $ | 5,430.2 |
| | 100.0 | % |
Medicaid
Our Medicaid segment includes plans for beneficiaries of TANF, SSI, ABD and other state-based programs that are not part of the Medicaid program, such as CHIP, FHP, and MLTC programs. For purposes of our Medicaid segment, we define our customer as the state and related governmental agencies that have common control over the contracts under which we operate in that particular state. In our Medicaid segment, we are operating in five of the ten largest membership states. We are the largest Medicaid health plan by revenue in Florida, Georgia, Hawaii and Kentucky. As of January 2013, our Florida Medicaid program is the only Medicaid plan serving every county in the state.
The Medicaid programs and services we offer to our members vary by state and county and are designed to effectively serve our constituencies in the communities in which we operate. Although our Medicaid contracts determine to a large extent the type and scope of health care services that we arrange for our members, in certain markets we customize our benefits in ways that we believe make our products more attractive. Our Medicaid plans provide our members with access to a broad spectrum of medical benefits from primary care and preventive programs to full hospitalization and long-term care.
In general, members are required to use our network to receive care, except in cases of emergencies, transition of care or when network providers are unavailable to meet their medical needs. In addition, members generally must receive a referral from their primary care providers ("PCPs") in order to receive health care from a specialist, such as an orthopedic surgeon or neurologist. Members do not pay any premiums, deductibles or co-payments for most of our Medicaid plans.
Medicaid Membership
The following table summarizes our Medicaid segment membership by the programs we offer.
|
| | | | | | | | |
| | As of December 31, |
| | 2012 | | 2011 | | 2010 |
| Medicaid | | | | | |
| TANF | 1,212,000 |
| | 1,159,000 |
| | 1,085,000 |
|
| CHIP | 207,000 |
| | 162,000 |
| | 168,000 |
|
| SSI and ABD and other | 146,000 |
| | 115,000 |
| | 77,000 |
|
| FHP | 22,000 |
| | 15,000 |
| | 10,000 |
|
| Total | 1,587,000 |
| | 1,451,000 |
| | 1,340,000 |
|
We received over 10% of our consolidated premium revenue in 2012, 2011 and 2010, individually, from the states of Florida and Georgia and, in 2012, Kentucky, and the membership for those states is summarized in the following table.
|
| | | | | | | | |
| | As of December 31, |
| | 2012 | | 2011 | | 2010 |
| Medicaid | | | | | |
| Georgia | 570,000 |
| | 562,000 |
| | 566,000 |
|
| Florida | 454,000 |
| | 404,000 |
| | 415,000 |
|
| Kentucky | 207,000 |
| | 129,000 |
| | — |
|
| All other states* | 356,000 |
| | 356,000 |
| | 359,000 |
|
| Total | 1,587,000 |
| | 1,451,000 |
| | 1,340,000 |
|
|
| |
| * | "All other states" consists of Hawaii, Illinois, New York, and Ohio and, in 2011 and 2010, Missouri. |
We were not awarded a Medicaid contract in Ohio for the 2013 fiscal year; however, the state of Ohio has contracted with us to provide services to Ohio Medicaid beneficiaries through the transition period. We currently estimate that the transfer of our Ohio Medicaid members to other plans should be substantially complete in the first quarter of 2013, but it may extend through June 30, 2013.
Medicaid Segment Revenues
Our Medicaid segment generates revenues primarily from premiums received from the states in which we operate health plans. We receive a fixed premium per member per month ("PMPM") pursuant to our state contracts. Our Medicaid contracts with state governments are generally multi-year contracts subject to annual renewal provisions. We generally receive premium payments during the month in which we provide services, although we have experienced delays in receiving monthly payments from certain states. For example, Georgia has delayed making supplemental payments for obstetric deliveries and newborns to us. In some instances, our base premiums are subject to risk score adjustments based on our members' acuity. Generally, the risk score is determined by the state by analyzing encounter submissions of processed claims data to determine the acuity of our membership relative to the entire state's Medicaid membership. In Georgia, Illinois, Kentucky, New York and Ohio, we are eligible to receive supplemental payments for obstetric deliveries and newborns. In Missouri, we earned supplemental payments for obstetric deliveries and newborns through the expiration of our contract on June 30, 2012. Each contract is specific as to how and when these supplemental payments are earned and paid. Upon delivery of a newborn, the state agency is notified according to the contract terms. Revenues are recorded based on membership and eligibility data provided by the states, which may be adjusted by the states for any subsequent updates to this data.
The following table sets forth information relating to premium revenues, net of premium taxes, from the states of Florida, Georgia and Kentucky, as well as all other states on an aggregate basis.
|
| | | | | | | | | | | | | | | | | | | | |
| | For the Years Ended December 31, |
| | 2012 | | 2011 | | 2010 |
| State | Revenue (In Millions) | | Percentage of Total Segment Revenue | | Revenue (In Millions) | | Percentage of Total Segment Revenue | | Revenue (In Millions) | | Percentage of Total Segment Revenue |
| Georgia | $ | 1,460.8 |
| | 33.3 | % | | $ | 1,449.3 |
| | 41.3 | % | | $ | 1,374.7 |
| | 41.5 | % |
| Florida | 970.9 |
| | 22.1 | % | | 881.1 |
| | 25.1 | % | | 889.7 |
| | 26.9 | % |
| Kentucky | 723.7 |
| | 16.5 | % | | 86.2 |
| | 2.5 | % | | — |
| | — | % |
| All other states* | 1,233.6 |
| | 28.1 | % | | 1,088.9 |
| | 31.1 | % | | 1,044.4 |
| | 31.6 | % |
| Total | $ | 4,389.0 |
| | 100.0 | % | | $ | 3,505.5 |
| | 100.0 | % | | $ | 3,308.8 |
| | 100.0 | % |
|
| |
| * | "All other states" consists of Hawaii, Illinois, Missouri, New York and Ohio. Effective as of June 30, 2012, our Missouri contract expired and was not renewed. |
Our Florida Medicaid and Healthy Kids contracts and Illinois Medicaid contract require us to expend a minimum percentage of premiums on eligible medical services and to the extent that we expend less than the minimum percentage of the premiums on eligible medical service, we are required to refund all or a portion of the difference between the minimum and our actual allowable medical expense. We estimate the amounts due to the state as a return of premium each period based on the terms of our contract with the applicable state agency.
Our current state contracts are set to expire or renew between June 2013 and August 2015. The following table sets forth the terms and expiration dates of our material Medicaid contracts with the states of Florida and Georgia, the two states that each accounted for greater than 10% of our consolidated premium revenues during 2012, 2011, and 2010, and with Kentucky, a third state that accounted for greater than 10% of our consolidated premium revenues during 2012.
|
| | | | | | |
| State | | Line of Business | | Term of Contract | | Expiration Date of Current Term |
| Florida | | Medicaid (Staywell) | | 3-year term(1) | | August 31, 2015 |
| Florida | | Medicaid (HealthEase) | | 3-year term(1) | | August 31, 2015 |
| Georgia | | Medicaid and CHIP | | 1-year term with 1 one- year renewal (2) | | June 30, 2013 |
| Kentucky | | Medicaid | | 3-year term with 4 one- year renewals (3) | | July 5, 2014 |
___________
(1) The Florida Agency for Health Care Administration ("AHCA") recently began a competitive procurement program to award contracts for Medicaid managed care across the state. These contracts may be terminated early, possibly at the end of 2013, with the new contracts expected to begin in the first quarter of 2014.
| |
| (2) | Our Georgia contract commenced in July 2005 and currently has one additional one-year option term, exercisable by the Georgia Department of Community Health ("Georgia DCH"), which potentially extends the total term until June 30, 2014. In addition, in 2012 Georgia DCH advised us that it intends to further amend our contract to add an additional two one-year option terms which would potentially extend the total term until June 30, 2016. |
| |
| (3) | Our original Kentucky contract, not including Region 3, commenced in July 2011 and we began offering services to members on November 1, 2011. The contract has an initial three-year term and provides for four additional one-year option terms, exercisable upon mutual agreement of the parties, which potentially extends the total term until July 2018. |
In October 2012, we were awarded a contract by the Commonwealth of Kentucky to coordinate physical, behavioral and dental care for a total of approximately 170,000 Medicaid eligible beneficiaries in Medicaid Managed Care Region 3, which consists of 16 counties. We began serving Medicaid beneficiaries in Region 3 effective January 1, 2013. As of January 1, 2013, our membership for this region was estimated to be more than 20,000.
Medicare Advantage (MA)
We contract with CMS under the Medicare program to provide a comprehensive array of Part C and Part D benefits to Medicare eligible persons. These benefits are provided through our MA plans, which are comprised of CCPs. CCPs are administered through HMOs and generally require members to seek health care services and select a PCP from a network of health care providers. In addition, we offer Medicare Part D coverage, which provides prescription drug benefits, as a component of our MA plans.
As of January 1, 2013, we offer MA plans in a total of 204 counties across 14 states, with over 15 million eligible beneficiaries in these service areas. For 2013, we expanded our Medicare Advantage service area by 53 counties in Florida, Georgia, Illinois, Kentucky, New York, and Texas. We offer duals special needs plans ("D-SNPs") in nearly all the counties that we serve, and approximately 33% of our MA members are "dually eligible" for Medicare and Medicaid and are enrolled in one of our D-SNPs. We cover a wide spectrum of medical services through our MA plans. For many of our plans, we provide additional benefits not covered by Original Medicare, such as vision, dental and hearing services. Through these enhanced benefits, out-of-pocket expenses incurred by our members are generally reduced, which allows our members to better manage their health care costs.
Some of our MA plans require members to pay a co-payment, which varies depending on the services and level of benefits provided. Typically, members of our MA CCPs are required to use our network of providers, except in specific cases such as emergencies, transition of care or when specialty providers are unavailable in our network to meet their medical needs. MA CCP members may see out-of-network specialists if they receive referrals from their PCPs and may pay incremental cost-sharing. We also offer D-SNPs for those who are dually-eligible for Medicare and Medicaid in most of our MA markets. We believe that our D-SNPs are attractive to these beneficiaries due to the enhanced benefit offerings and clinical support programs.
In October 2012, our Medicare plans in Connecticut, Florida, Hawaii, Illinois, and Ohio achieved a three Star summary rating, while our plans in Georgia, Louisiana, Missouri, New Jersey, New York and Texas received a 2.5 Star summary rating.
MA Membership
As of December 31, 2012, 2011 and 2010, we had approximately 213,000, 135,000 and 116,000 MA members, respectively. Membership at December 31, 2012 includes 39,000 California members resulting from the Easy Choice acquisition, which closed in November 2012. Membership as of January 1, 2013 was approximately 250,000, a 71% increase compared to the 146,000 members at January 31, 2012, and a 17% increase from the 213,000 as of December 31, 2012. Excluding the Desert Canyon and Easy Choice acquisitions, our January 2013 enrollment was approximately 194,000 members, an increase of 11% from 174,000 members as of December 2012. In January 2013 our Easy Choice plan achieved enrollment of approximately 52,000, and through the closing of the Desert Canyon acquisition, we added approximately 4,000 members to our January 2013 membership, as well as our 14th Medicare state, Arizona. At this time, we expect MA segment membership to continue to grow during the remaining months of 2013, as we leverage our success in serving dually-eligible members as well as the broader growth in the Medicare population.
MA Segment Revenues
The amount of premiums we receive for each MA member is established by contract, although the rates vary according to a combination of factors, including upper payment limits established by CMS, the member's geographic location, age, gender, medical history or condition, or the services rendered to the member. MA premiums are due monthly and are recognized as revenue during the period in which we are obligated to provide services to members. We record adjustments to revenues based on member retroactivity. These adjustments reflect changes in the number and eligibility status of enrollees subsequent to when revenue was billed. We estimate the amount of outstanding retroactivity adjustments each period and adjust premium revenue accordingly. The estimates of retroactivity adjustments are based on historical trends, premiums billed, the volume of member and contract renewal activity and other information. Changes in member retroactivity adjustment estimates had a minimal impact on premiums recorded during the periods presented.
MA premium revenue for the year ended December 31, 2012, 2011 and 2010 was approximately $1,936.4 million, $1,479.8 million and $1,336.1 million, respectively. We currently offer MA plans under separate contracts with CMS for each of the states in which we offer such plans. Our MA contracts with CMS all have one year terms that expire at the end of each calendar year and are renewable by the parties; our current MA contracts expire on December 31, 2013.
Medicare Risk-Adjusted Premiums
CMS employs a risk-adjustment model to determine the premium amount it pays for each Medicare member. The risk-adjustment model apportions premiums paid to all plans according to the health status of each beneficiary enrolled and pays more for MA members with predictably higher costs. We collect claims and encounter data from inpatient and ambulatory treatment settings and submit the data to CMS, within prescribed deadlines, which are used to calculate the risk-adjusted premiums we receive. CMS establishes the premium payments to MA plans generally at the beginning of the plan year, and then adjusts premium levels on two separate occasions on a retroactive basis. The first retroactive adjustment for a given plan year generally occurs during the third quarter of that year. This initial settlement represents the update of risk scores for the current plan year based on the severity of claims incurred in the prior plan year. CMS then issues a final retroactive risk-adjusted premium settlement for that plan year in the following year.
We develop our estimates for risk-adjusted premiums utilizing historical experience, or other data, and predictive models as sufficient member risk score data becomes available over the course of each CMS plan year. Our estimates are periodically updated as additional diagnosis code information is reported to CMS and adjusted to actual amounts when the ultimate adjustment settlements are either received from CMS or we receive notification from CMS of such settlement amounts.
The data provided to CMS to determine the risk score is subject to audit by CMS even after the annual settlements occur. These audits may result in the refund of premiums to CMS previously received by us. While our experience to date has not resulted in a material refund, future refunds could be significant, which would reduce our premium revenue in the year that CMS determines repayment is required.
Prescription Drug Plans (PDPs)
We have contracted with CMS to serve as a plan sponsor offering stand-alone Medicare Part D PDP plans to Medicare-eligible beneficiaries through our PDP segment. The Medicare Part D program offers national in-network prescription drug coverage with more than 60,000 pharmacies, subject to limitations in certain circumstances.
We offer PDP plans in 49 states and the District of Columbia and are focused on value-conscious beneficiaries. For 2013, we launched a new PDP product that we believe is well positioned as a low-cost enhanced plan targeted to value-focused beneficiaries that actively choose their plan. We estimate that we added over 110,000 members to this plan through the 2013 annual election period. As of January 1, 2013, approximately 75% of our membership is comprised of beneficiaries that actively chose us for their current plan.
Our PDP contract with CMS is renewable for successive one-year terms unless CMS notifies us of its decision not to renew by May 1 of the current contract year, or we notify CMS of our decision not to renew by the first Monday in June of the contract year.
PDP Membership
As of December 31, 2012, 2011 and 2010, we served approximately 869,000, 976,000 and 768,000 PDP members, respectively. Membership as of December 31, 2012 decreased by 107,000 compared to December 31, 2011 as a result of our 2012 PDP bids, which resulted in the reassignment to other plans, effective January 1, 2012, of members who were auto-assigned to us in 2011 or prior years. Based on the outcome of our 2013 PDP bids, our plans are below the benchmarks in 14 of the 34 Centers for Medicare & Medicaid Services ("CMS") regions and within the de minimis range of the benchmark in five other CMS regions. Comparatively, in 2012, our plans were below the benchmark in five regions and within the de minimis range in 17 other regions. In 2013, we are being auto-assigned newly-eligible members into our plans for the 14 regions that are below the benchmark. We are retaining our auto-assigned members in the 5 regions in which we bid within the de minimis range; however, we are not being auto-assigned new members in those regions during 2013. Members previously auto assigned to our PDP plans in regions for which our 2013 bids were not within the de minimus range were reassigned to other plans as of January 1, 2013. Membership as of January 1, 2013 was approximately 750,000, a decrease of 119,000, or approximately 14% from 869,000 as of December 31, 2012, due to the reassignment to other plans of members who were previously auto-assigned to us, primarily in California, offset in part by additional auto-assignments to us in other regions and an increase in the members who actively chose our PDP plans. We expect membership for the remainder of 2013 to be relatively stable, as we focus on marketing our PDP products to those who actively choose us to offset normal attrition.
PDP Segment Revenues
Annually, we provide written bids to CMS for our PDPs, which reflect the estimated costs of providing prescription drug benefits over the plan year. Substantially all of the premium for this insurance is paid by the federal government, and the balance is due from the enrolled beneficiaries. The premium and subsidy components under Part D are described below.
Member Premium—We receive a monthly premium from members based on the plan year bid we submitted to CMS. The member premium, which is fixed for the entire plan year, is recognized over the contract period and reported as premium revenue.
CMS Direct Premium Subsidy—Represents monthly premiums from CMS based on the plan year bid submitted by plan sponsors to CMS. The monthly payment is a risk-adjusted amount per member and is based upon the member's health status as determined by CMS. Refer to the "Medicare Risk-Adjusted Premiums" section under the "Medicare Advantage (MA)" segment discussion above for a more detailed description of risk-adjusted premiums.
Low-Income Premium Subsidy—For qualifying LIS members, CMS pays for some or all of the LIS member's monthly premium. The CMS payment is dependent upon the member's income level, which is determined by the Social Security Administration.
Low-Income Cost Sharing Subsidy (LICS)—For qualifying LIS members, CMS reimburses plans for all or a portion of the LIS member's deductible, coinsurance and co-payment amounts above the out-of-pocket threshold. LICS subsidies are paid by CMS prospectively as a fixed amount PMPM, and are determined based upon the plan year bid submitted by plan sponsors to CMS. Following the plan year, CMS performs an annual reconciliation of the LICS received by the plan sponsor to the actual amount paid by the plan sponsor.
Catastrophic Reinsurance Subsidy—CMS reimburses plans for 80% of the drug costs after a member reaches his or her out-of-pocket catastrophic threshold through a catastrophic reinsurance subsidy. Catastrophic reinsurance subsidies are paid by CMS prospectively as a fixed amount PMPM, and are determined based upon the plan year bid submitted by plan sponsors to CMS. Following the plan year, CMS performs an annual reconciliation of the catastrophic reinsurance subsidy received by the plan sponsor to the actual amount paid by the plan sponsor.
Coverage Gap Discount Subsidy—Since 2011, CMS has provided monthly prospective payments for pharmaceutical manufacturer discounts made available to members. The prospective discount payments are determined based upon the plan year bid submitted by plan sponsors to CMS and current plan enrollment. Following the plan year, CMS performs an annual reconciliation of the prospective discount payments received by the plan sponsor to the amount of actual manufacturer discounts made available to each plan sponsor's enrollees under the program.
Low-income cost sharing, catastrophic reinsurance subsidies and coverage gap discount subsidies represent funding from CMS for which we assume no risk. The receipt of these subsidies and the payments of the actual prescription drug costs related to the low-income cost sharing, catastrophic reinsurance and coverage gap discounts are not recognized as premium revenues or benefits expense, but are reported on a net basis as funds receivable/held for the benefit of members in the consolidated balance sheets. These receipts and payments are reported as a financing activity in our consolidated statements of cash flows. After the close of the annual plan year, CMS reconciles actual experience to prospective payments paid to our plans and any differences are settled between CMS and our plans. Historically, we have not experienced material adjustments related to the CMS annual reconciliation of prior plan year low-income cost sharing and catastrophic reinsurance subsidies. We do not have a history of adjustments for the coverage gap discount subsidy as the 2011 plan year, which was the year CMS implemented the coverage gap discount subsidy, has not yet been settled by CMS.
CMS Risk Corridor—Premiums from CMS are subject to risk sharing through the Medicare Part D risk corridor provisions. The CMS risk corridor calculation compares the target amount of prescription drug costs (limited to costs under the standard coverage as defined by CMS) less rebates in the plan year bid to actual experience. Variances of more than 5% above the target amount will result in CMS making additional payments to plan sponsors and variances of more than 5% below the target amount will require plan sponsors to refund to CMS a portion of the premiums received. Historically, we have not experienced material adjustments related to the CMS settlement of the prior plan year risk corridor estimate.
PDP premium revenue for the year ended December 31, 2012, 2011 and 2010 was approximately $992.6 million, $1,036.8 million and $785.3 million, respectively. We offer our PDPs under a single contract with CMS, which has a term of one year expiring on December 31, 2013 and is renewable by the parties.
OUR OPERATIONS
Provider Networks and Provider Reimbursement Methods
We contract with a wide variety of health care providers to provide our members with access to medically-necessary services. Our contracted providers deliver a variety of services to our members including: primary and specialty physician care; laboratory and imaging services; inpatient, outpatient, home health and skilled facility care; medication and injectable drug therapy; ancillary services; durable medical equipment and related services; mental health and chemical dependency counseling and treatment; transportation; and dental, hearing and vision care.
The following are the types of providers in our Medicaid and MA CCP contracted networks:
| |
| • | Professionals such as PCPs, provider groups, specialty care physicians, psychologists and licensed social workers; |
| |
| • | Facilities such as hospitals with inpatient, outpatient and emergency services, skilled nursing facilities, outpatient surgical facilities and diagnostic imaging centers; |
| |
| • | Ancillary providers such as laboratory providers, radiology, home health, physical therapy, speech therapy, occupational therapy, ambulance providers and transportation providers; and |
| |
| • | Pharmacies, including retail pharmacies, mail order pharmacies and specialty pharmacies. |
These providers are contracted through a variety of mechanisms, including agreements with individual providers, groups of providers, independent provider associations, integrated delivery systems and local and national provider chains such as hospitals, surgical centers and ancillary providers. We also contract with other companies who provide access to contracted providers, such as pharmacy, dental, hearing, vision, transportation and mental health benefit managers.
Facility, pharmacy, dental, vision and behavioral health contracts cover medically-necessary services and, under some of our plans, enhanced benefits. These contracts typically have terms of one to four years with some of the agreements automatically renewing at the end of the contract period, unless otherwise specified in writing by either party. During the contract period, these agreements typically can be terminated without cause upon written notice by either party, but the notification period may range from 90 to 180 days and early termination may subject the terminating party to financial penalties.
The contract terms require providers to participate in our quality improvement and utilization review programs, which we may modify from time to time. Providers must also adhere to applicable state and federal regulations.
We periodically review the fees paid to providers and make adjustments as necessary. Generally, our contracts with providers do not allow for automatic annual increases in reimbursement levels. Among the factors generally considered in adjustments are changes to state Medicaid or Medicare fee schedules, competitive environment, current market conditions, anticipated utilization patterns and projected medical expenses. Some provider contracts are directly tied to state Medicaid or Medicare fee schedules, in which case reimbursement levels will be adjusted up or down, generally on a prospective basis, based on adjustments made by the state or CMS to the appropriate fee schedule.
Physicians and Provider Groups
PCPs play an important role in coordinating and managing the care of our Medicaid and MA CCP members. This coordination includes delivering preventive services as well as referring members to other providers for medically-necessary services. PCPs are typically trained in internal medicine, pediatrics, family practice, general practice or, in some markets, obstetrics and gynecology. In rare instances, a physician trained in sub-specialty care will perform primary care services for a member with a chronic condition.
To help ensure quality of care, we credential and re-credential all professional providers with whom we contract, including physicians, psychologists, licensed social workers, certified nurse midwives, advanced registered nurse practitioners and physician assistants who provide care under the supervision of a physician directly or through delegated arrangements. This credentialing and re-credentialing is performed in accordance with standards required by CMS and consistent with the standards of the National Committee for Quality Assurance ("NCQA").
We reimburse some of our PCPs on a fixed-fee PMPM basis. This type of reimbursement methodology is commonly referred to as capitation. The reimbursement covers care provided directly by the PCP as well as coordination of care from other providers as described above. In certain markets, services such as vaccinations and laboratory or screening services delivered by the PCP may warrant reimbursement in addition to the capitation payment. Further, in some markets, PCPs may also be eligible for incentive payments for achieving certain measurable levels of compliance with our clinical guidelines covering prevention and health maintenance. These incentive payments may be paid as a periodic bonus or when the PCP submits documentation of a member's receipt of services. In limited instances, specialty care provider groups in certain regions are paid a capitation rate to provide specialty care services to members in those regions.
In all instances, we require providers to submit data reporting all direct encounters with members. This data helps us to monitor the amount and level of medical treatment provided to our members to help improve the quality of care provided and comply with regulatory reporting requirements. Our regulators use the encounter data that we submit, as well as data submitted by other health plans, to set reimbursement rates, assign membership, assess the quality of care being provided to members and evaluate contractual and regulatory compliance.
PCPs in our MA CCP products and, in limited instances, in our Medicaid products, are eligible for a specialized risk arrangement to further align the interests of the PCPs with ours. PCPs participating in specialized risk arrangements cover 76% and 25% of our MA and Medicaid membership, respectively, as of December 31, 2012. Under these arrangements, we establish a risk fund for each provider based on a percentage of premium received. We periodically evaluate and monitor this fund on an individual or group basis to determine whether these providers are eligible for additional payments or, in the alternative, whether they should reimburse us. Payments due to us are normally carried forward and offset against future payments.
Specialty care providers and, in some cases, PCPs, are typically reimbursed a specified fee for the service performed, which is known as fee-for-service. The specified fee is set as a percentage of the amount Medicaid or Medicare would pay under the applicable fee-for-service program. For the year ended December 31, 2012 and 2011, approximately 10% and 12%, respectively, of our payments to physicians serving our Medicaid members were on a capitated basis and approximately 90% and 88%, respectively, were on a fee-for-service basis. During the years ended December 31, 2012 and 2011, approximately 13% and 15%, respectively, of our payments to physicians serving our Medicare members in MA CCPs were on a capitated basis and approximately 87% and 85%, respectively, were on a fee-for-service basis.
In addition, our recent amendments to our Medicaid contracts with AHCA required us to comply with federal law related to increased reimbursements to Medicaid providers. We do not currently expect to increase the reimbursement amounts until we receive an adjustment to the premium rates we receive, but if we are required to do so in the future, our medical benefits expense and medical benefits ratio would increase.
Facilities
Our health plans arrange for hospital care primarily through contracts with selected hospitals in their service areas for coverage of medically-necessary care. These hospital contracts generally have multi-year terms or annual terms with automatic renewals and provide for payments on a variety of bases, including capitation, per diem rates, case rates and discounted fee-for-service schedules. These contracts typically can be canceled by either party, without cause, usually upon 90 days written notice. In some cases a longer notice period may be required, such as where a longer period is required by regulation or the applicable government contract.
Inpatient services are sometimes reimbursed as a fixed global payment for an admission based on the associated diagnosis related group, or DRG, as defined by CMS. In many instances, certain services, such as implantable devices or particularly expensive admissions, are reimbursed as a percentage of hospital charges either in addition to, or in lieu of, the DRG payment. Certain facilities in our networks are reimbursed on a negotiated rate paid for each day of the member's admission, known as a per diem. This payment varies based upon the intensity of services provided to the member during admission, such as intensive care, which is reimbursed at a higher rate than general medical services.
Facility outpatient services are reimbursed either as a percentage of charges or based on a fixed-fee schedule for the services rendered, in accordance with ambulatory payment groups or ambulatory payment categories, both as defined by CMS. Outpatient services for diagnostic imaging are reimbursed on a fixed-fee schedule as a percentage of the applicable Medicare or Medicaid fee-for-service schedule or a capitation payment.
In Florida, AHCA plans to amend the DRG schedule that it uses to set rates for certain providers whose contracts are tied to Medicaid effective July 1, 2013, which may increase or decrease our payments to these providers.
Ancillary Providers
Our typical ancillary agreements provide for coverage of medically-necessary care and, in general, have terms of one year. These contracts automatically renew for successive one-year periods unless otherwise specified in writing by either party. These contracts typically can be canceled by either party, without cause, usually upon 90 days written notice. In some cases a longer notice period may be required, such as where a longer period is required by regulation or the applicable government contract.
Ancillary providers, who provide services such as laboratory services, home health, physical, speech and occupational therapy, and ambulance and transportation services, are reimbursed on a capitation or fee-for-service basis.
Pharmacies
Pharmacy services are reimbursed based on a fixed fee for dispensing medication and a separate payment for the ingredients. Ingredients produced by multiple manufacturers are reimbursed based on a maximum allowable cost for the ingredient. Ingredients produced by a single manufacturer are reimbursed as a percentage of the average wholesale price. In certain instances, we contract directly with the sole-source manufacturer of an ingredient to receive a rebate, which may vary based upon volumes dispensed during the year.
Out-of-Network Providers
When our members receive services for which we are responsible from a provider outside our network, such as in the case of emergency room services from non-contracted hospitals, we generally attempt to negotiate a rate with that provider. In most cases, when a member is treated by a non-contracted provider, we are obligated to pay only the amount that the provider would have received from traditional Medicaid or Medicare.
Member Recruitment
Our member recruitment and marketing efforts for both Medicaid and Medicare members are heavily regulated by state agencies and CMS. For many products, we rely on the auto-assignment of members into our plans, including our PDP plan. The auto-assignment of a beneficiary into a health or prescription drug plan generally occurs when that beneficiary does not choose a plan. The agency with responsibility for the program determines the approach by which a beneficiary becomes a member of a plan serving the program. Some programs assign members to a plan automatically based on predetermined criteria. These criteria frequently include a plan's rates, the outcome of a bidding process, quality scores or similar factors. For example, CMS auto-assigns PDP members based on whether a plan's bids during the annual renewal process are above or below the CMS benchmark. In most states, our Medicaid health plans benefit from auto-assignment of individuals who do not choose a plan but for whom participation in managed care programs is mandatory. Each state differs in its approach to auto-assignment, but one or more of the following criteria is typical in auto-assignment algorithms: a Medicaid beneficiary's previous enrollment with a health plan or experience with a particular provider contracted with a health plan, enrolling family members in the same plan, a plan's quality or performance status, a plan's network and enrollment size, awarding all auto-assignments to a plan with the lowest bid in a county or region, and equal assignment of individuals who do not choose a plan in a specified county or region.
Our Medicaid marketing efforts are regulated by the states in which we operate, each of which imposes different requirements for, or restrictions on, Medicaid sales and marketing. These requirements and restrictions can be revised from time to time. Several states, including our three largest Medicaid states, Florida, Georgia and Kentucky, do not permit direct sales by Medicaid health plans. We rely on member selection and auto-assignment of Medicaid members into our plans in those states.
Our Medicare marketing and sales activities are regulated by CMS and the states in which we operate. CMS has oversight over all, and in some cases has imposed advance approval requirements with respect to, marketing materials used by MA plans, and our sales activities are limited to activities such as conveying information regarding benefits, describing the operations of managed care plans and providing information about eligibility requirements. The activities of our independently-licensed insurance agents are also regulated by CMS.
We also employ our own sales force and contract with independent, licensed insurance agents to market our MA and PDP products. We have continued to expand our use of independent agents whose cost is largely variable in nature and whose engagement is more conducive to the shortened Medicare selling season and the elimination of the open enrollment period. We also use direct mail, mass media and the Internet to market our products.
Enrollment in our PDPs is impacted by the auto-assignment of members, which is subject to a bid process whereby we submit to CMS our estimated costs to provide services in the next fiscal year. For example, based on the outcome of our 2013 PDP bids, our plans are below the benchmarks in 14 of the 34 CMS regions and within the de minimis range of the benchmark in five other CMS regions. In 2013, we are being auto-assigned newly-eligible members into our plans for the 14 regions that are below the benchmark. Members previously auto assigned to our PDP plans in regions for which our 2013 bids were not within the de minimis range are being reassigned to other plans in 2013. Comparatively, in 2012, our prescription drug plans were below the benchmarks in five regions and within the de minimus ranges in 17 other regions. We are retaining our auto-assigned members in the five regions in which we bid within the de minimis range; however, we are not being auto-assigned new members in those regions during 2013. Consequently, our PDP membership has declined to approximately 750,000 as of January 1, 2013. We expect membership for the remainder of 2013 to be relatively stable as we focus on marketing our PDP products to those who actively choose us to offset normal attrition.
Enrollment into our plans is also subject to suspension or termination due to sanctions. For example, during 2009, CMS imposed a sanction against us that prohibited us from the marketing of, and enrolling members into, all lines of our Medicare business from March until the sanction was released in November of 2009. As a result of the sanction, we were also not eligible to receive auto-assignment of low-income subsidy, dually-eligible beneficiaries into our PDPs for January 2010 enrollment.
Quality Improvement
We are focused on improving quality across all of our lines of business, which is critical to the continued growth and success of our business. We continually seek to improve the quality of care delivered by our network providers to our members and our ability to measure the quality of care provided. Our quality improvement program provides the basis for our quality and utilization management functions and outlines ongoing processes designed to improve the delivery of quality health care services to our members, as well as to enhance compliance with regulatory and accreditation standards. Our operating expenditures for quality improvement costs increased by more than 60% in 2012 compared to 2011. For 2013, we expect to sustain our investment consistent with the level of premium revenues, as was the case in 2012.
Our quality improvement activities will continue to focus on:
| |
| • | Preventive health and wellness and care management; |
| |
| • | Case and disease management; |
| |
| • | Health plan accreditation; |
| |
| • | Provider education and incentives for closing care gaps; |
| |
| • | Member education and outreach; |
| |
| • | Information technology initiatives related to the above activities; and |
Preventive health and wellness and care management
We sponsor a number of initiatives aimed at the promotion of healthy lifestyles and the prevention of disease, including preventive screenings, health education programs to inform members about health care issues and healthy behaviors and health assessment & counseling to inform members how to use the resources and services available to them to help reduce preventable diseases.
Case and disease management
Some examples of our intervention programs include: a prenatal case management program to help women with high-risk pregnancies; a program to reduce the number of inappropriate emergency room visits; and disease management programs to decrease the need for emergency room visits and hospitalizations.
Accreditation
Several of our health plans are accredited by nationally-recognized independent organizations that have been established to measure health plans' commitment to effective management and accountability. Our Florida HMOs are currently accredited by URAC and our Georgia, Hawaii and Missouri HMOs are accredited by NCQA. In January 2013, our Florida Medicaid and Medicare health plans were awarded NCQA accreditation. We remain dedicated to our long-term target of attaining accreditation for all of our health plans and currently expect NCQA accreditation in a number of states before the end of 2013.
Provider credentialing
We credential physicians, hospitals and other health care professionals in our participating provider networks using quality criteria which meet or exceed the standards of external accreditation or state regulatory agencies, or both. Typically, most health care professionals are re-credentialed every three years, depending on applicable state laws.
Provider education and incentives for closing care gaps
As part of our quality improvement program, at times we have implemented changes to our reimbursement methods to reward those providers who encourage preventive care, such as well-child check-ups, prenatal care and/or who adopt evidence- based guidelines for members with chronic conditions. Additionally, several of our markets have provider incentives for closing care gaps inherent to the health care system. This initiative has resulted in increased member experiences to drive improvement in the quality of care.
Member education and outreach
Regarding our members, we are focused on improving access to a high-performing network of providers, including PCPs, specialists and ancillary providers, and ensuring that members see the appropriate providers, based on clinical condition. If members experience difficulties in maintaining their appointments with providers, we will proactively outreach to members telephonically or arrange for home visits to assess and close care gaps. We are focused on enhancing our members' experience by improving service and reducing complaint levels through improved grievance and appeals processes and member satisfaction surveys. In June 2011, we successfully launched new customer service tools to support more intensive management of care gaps, which has resulted in over 45,000 member education sessions, many involving real time appointment setting with our providers.
Information technology initiatives
We understand the importance of information technology in improving the level of service that we can provide to our members. Accordingly, we continue to invest in our information technology infrastructure and capabilities including tools that support our focus on improving our ability in providing members with quality health care. We have specialized systems to support our quality improvement activities and to gather information from our systems to identify opportunities to improve care and track the outcomes of the services provided to achieve those improvements, such as evaluating the effects of particular preventive measures.
Oversight and audits
Internally, our quality improvement programs benefit from executive oversight and project management processes. Additionally, each of our health plans has a Quality Improvement Committee comprised of senior members of management, medical directors and other key associates of ours. Each of these committees report directly to the applicable health plan boards of directors, which have ultimate oversight responsibility for the quality of care rendered to our members. The Quality Improvement Committees also have a number of subcommittees that are charged with monitoring certain aspects of care and service, such as health care utilization, pharmacy services and provider credentialing and re-credentialing. Several of these subcommittees include physicians as committee members.
Our board of directors recognizes the importance of delivering quality care and providing access to that care for our members and has established the Health Care Quality and Access Committee of the board. The primary purpose of this committee is to assist the board by reviewing, and providing general oversight of, our health care quality and access strategy, including our policies and procedures governing health care quality and access for our members. This input helps provide overall direction and guidance to our Quality Improvement Committees.
We conduct routine site audits of select providers and medical record audits to ensure the effectiveness of our quality improvement programs.
Technology
The accurate and timely capture, processing and analysis of critical data are cornerstones for providing managed care services. Focusing on data is also essential to operating our business in a cost effective manner. Data processing and data-driven decision making are key components of both administrative efficiency and medical cost management. We use our information system for premium billing, claims processing, utilization management, reporting, medical cost trending, planning and analysis. The system also supports member and provider service functions, including enrollment, member eligibility verification, primary care and specialist physician roster access, claims status inquiries, and referrals and authorizations.
On an ongoing basis, we evaluate the ability of our existing operations to support our current and future business needs and to maintain our compliance requirements. This evaluation may result in enhancing or replacing current systems and/or processes which could result in our incurring substantial costs to improve our operations and services. We recently completed an upgrade of our core operating systems. This new technology will enable further progress on our work to improve service and productivity, and positions us to comply with future regulatory requirements such as the implementation of ICD-10 by October 2014. This upgrade will also support our health care quality and access initiatives.
We have a disaster recovery plan that addresses how we recover business functionality within stated timelines. We have a cold site and business recovery site agreement with a nationally-recognized, third-party vendor to provide for the restoration of our general support systems at a remote processing center. We perform disaster recovery testing at least annually for those business applications that we consider critical.
Reinsurance
We bear underwriting and reserving risks associated with our HMO and insurance subsidiaries. We retain certain of these risks through our wholly-owned, captive insurance subsidiary. We reduce exposure to large catastrophic losses by insuring levels of coverage for losses in excess of what we retain internally with highly-rated, unaffiliated insurance companies. However, we remain liable in the event these insurance companies are unable to pay their portion of the losses, so we continually monitor the financial condition of these companies to ensure that they are maintaining these high ratings.
Outsourcing Arrangements
Our care and service delivery model is designed to optimize our use of our personnel versus third parties based on an evaluation of factors, including cost, compliance, quality and procurement success. As a result, we have contracted with a number of vendors to provide significant operational support including, but not limited to, pharmacy benefit management and behavioral health services for our members as well as certain enrollment, billing, call center, benefit administration, claims processing functions, sales and marketing and certain aspects of utilization management. Our dependence on these vendors makes our operations vulnerable to such third parties' failure to perform adequately under our contracts with them. In addition, where a vendor provides services that we are required to provide under a contract with a government customer, we are responsible for such performance and will be held accountable by our government customers for any failure of performance by our vendors. We evaluate the competency and solvency of our third-party vendors prior to execution of contracts and include service level guarantees in our contracts where appropriate. Additionally, we perform ongoing vendor oversight activities to identify any performance or other issues related to our vendors.
Centralized Management Services
We provide centralized management services to each of our health plans from our Tampa, Florida headquarters and call centers, with the current exceptions of our recently acquired California and South Carolina HMO subsidiaries. We expect to integrate and begin providing services directly to these subsidiaries once we receive regulatory approval to do so, which we expect to occur before the end of 2013. These services include information technology, product development and administration, finance, human resources, accounting, legal, public relations, marketing, insurance, purchasing, risk management, internal audit, actuarial, underwriting, claims processing and customer service and are provided by a non-regulated affiliated administrator. We have managed behavioral health care for the Kentucky Medicaid program since its inception in November 2011 and plan to begin insourcing behavioral health services for most of our health plans in 2013.
Employees
We refer to our employees as associates. As of December 31, 2012, we had approximately 4,460 full-time associates. Our associates are not represented by any collective bargaining agreement, and we have never experienced a work stoppage. We believe we have good relations with our associates.
OUR COMPETITION
Competitive Environment
We operate in a highly competitive environment to manage the cost and quality of services that are delivered to government health care program beneficiaries. We currently compete in this environment by offering Medicare and Medicaid health plans in which we accept all or nearly all of the financial risk for management of beneficiary care under these programs.
We typically must be awarded a contract by the government agency with responsibility for a program in order to offer our services in a particular location. Some government programs choose to limit the number of plans that may offer services to beneficiaries, while other agencies allow an unlimited number of plans to serve a program, subject to each plan meeting certain contract requirements. When the number of plans participating in a program is limited, an agency generally employs a bidding process to select the participating plans.
As a result, the number of companies with which we compete varies significantly depending on the geographic market, business segment and line of business. For example, in Florida, the Medicaid program currently does not specifically restrict the number of participating plans. In contrast, the Georgia Department of Community Health, which operates the Georgia Families and PeachCare programs, awarded contracts to only three plans. We compete with one or two other plans in each of the six regions in Georgia. Likewise, in our Medicare business, the number of competitors varies significantly by geography. In most cases, there are numerous other Medicare plans and other competitors. We believe a number of our competitors in both Medicare and Medicaid have strengths that may match or exceed our own with respect to one or more of the criteria on which we compete with them. Further, some of our competitors may be better positioned than us to withstand rate compression.
Competitive Factors—Program Participation
Regardless of whether the number of health plans serving a program is limited, we believe government agencies determine program participation based on several criteria. These criteria generally include the terms of the bids as well as the breadth and depth of a plan's provider network; quality and utilization management processes; responsiveness to member complaints and grievances; timeliness and accuracy of claims payment; financial resources; historical contractual and regulatory compliance; quality scores, references and accreditation; and other factors.
Competitive Factors—Network Providers
In addition, we compete with other health plans to contract with hospitals, physicians, pharmacies and other providers for inclusion in our networks that serve government program beneficiaries. We believe providers select plans in which they participate based on several criteria. These criteria generally include reimbursement rates; timeliness and accuracy of claims payment; potential to deliver new patient volume and/or retain existing patients; effectiveness of resolution of calls and complaints; and other factors.
Obtaining Members
The agency with responsibility for a particular program determines the approach by which a beneficiary becomes a member of one of the plans serving the program. Generally, government programs either assign members to a plan automatically or they permit participating plans to market to potential members, though some programs employ both approaches. For more information about auto-assignment and how we obtain our members generally, see the Member Recruitment discussion above.
Medicaid Competitors
In the Medicaid managed care market, our principal competitors for state contracts, members and providers include the following types of organizations:
| |
| • | MCOs—Managed care organizations ("MCOs") that, like us, receive state funding to provide Medicaid benefits to members. Many of these competitors operate in a single or small number of geographic locations. There are a few multi-state Medicaid-only organizations that are able to leverage their infrastructure over a larger membership base. Competitors include private and public companies, which can be either for-profit or non-profit organizations, with varying degrees of focus on serving Medicaid populations. |
| |
| • | Medicaid Fee-For-Service—Traditional Medicaid offered directly by the states or a modified version whereby the state administers a primary care case management model. |
| |
| • | PSNs—A Provider Service Network ("PSN") is a network of providers that is established and operated by a health care provider or group of affiliated health care providers. A PSN operates as either a fee-for-service ("FFS") health plan or as a prepaid health plan that, like us, receives a capitated premium to provide Medicaid benefits to members. A PSN that operates as a FFS health plan is not at risk for medical benefit costs. FFS PSNs are at risk for 50% of their administrative cost allocation if their total costs exceed the estimated at-risk capitation amount. |
Medicare Competitors
In the Medicare market, our primary competitors for contracts, members and providers include the following types of competitors:
| |
| • | Original Fee-For-Service Medicare—Original Medicare is available nationally and is a fee-for-service plan managed by the federal government. Beneficiaries enrolled in Original Medicare can go to any doctor, supplier, hospital or other facility that accepts Medicare and is accepting new Medicare patients. |
| |
| • | Medicare Advantage and Prescription Drug Plans—MA and stand-alone Part D plans are offered by national, regional and local MCOs and insurance companies that serve Medicare beneficiaries. In addition, prescription drug plans are being offered by or co-branded with retail drug store chains or other retail store chains, which may be able to offer lower priced plans and achieve benefits from integration with their pharmacy benefit management operations. |
| |
| • | Employer-Sponsored Coverage—Employers and unions may subsidize Medicare benefits for their retirees in their commercial group. The group sponsor solicits proposals from MA plans and may select an HMO, PPO and/or PDP to provide these benefits. |
| |
| • | Medicare Supplements—Original Medicare pays for many, but not all, health care services and supplies. A Medicare supplement policy, commonly called "Medigap", is private health insurance designed to supplement Original Medicare by covering the cost of items such as co-payments, coinsurance and deductibles. Some Medicare supplements cover additional benefits for an additional cost. Medicare supplement plans can be used to cover costs not otherwise covered by Original Medicare, but cannot be used to supplement MA plans. |
REGULATION IMPACTING OUR BUSINESS
Our health care operations are highly regulated by both state and federal government agencies. Regulation of managed care products and health care services is an ever-evolving area of law that varies from jurisdiction to jurisdiction. Regulatory agencies generally have discretion to issue regulations and interpret and enforce laws and rules. Changes in applicable laws, statutes, regulations and rules occur frequently. These changes may include a requirement to provide health care services not contemplated in our current contracted premium rate or to pay providers at a state-mandated fee schedule without a commensurate adjustment to the premium rate. For further information, see the Provider Networks and Reimbursement Methods discussion above. In addition, government agencies may impose taxes, fees or other assessments upon us and other managed care companies at any time.
Our contracts with various state government agencies and CMS to provide managed health care services include provisions regarding provider network adequacy, maintenance of quality measures, accurate submission of encounter and health care cost information, maintaining standards of call center performance and other requirements specific to government and program regulations. We must also have adequate financial resources to protect the state, our providers and our members against the risk of our insolvency. Our failure to comply with these requirements may result in the assessment of penalties, fines and liquidated damages. For further information on data provided to CMS that is subject to audit, refer to the Medicare Risk-Adjusted Premiums discussion above.
Government enforcement authorities have become increasingly active in recent years in their review and scrutiny of various sectors of the health care industry, including health insurers and managed care organizations. We routinely respond to subpoenas and requests for information from these entities and, more generally, we endeavor to cooperate fully with all government agencies that regulate our business.
Product Compliance
Medicaid programs
Medicaid is state operated and implemented, although it is funded by both the state and federal governments. Within broad guidelines established by the federal government, each state:
| |
| • | establishes its own eligibility standards; |
| |
| • | determines the type, amount, duration and scope of services; |
| |
| • | sets the rate of payment for services; and |
| |
| • | administers its own program. |
We have entered into contracts with Medicaid agencies in each state in which we operate Medicaid plans. Some of the states in which we operate award contracts to applicants that can demonstrate that they meet the state's minimum requirements. Other states engage in a competitive bidding process for all or certain programs. In either case, we must demonstrate to the satisfaction of the respective agency that we are able to meet certain operational and financial requirements. For example:
| |
| • | we must measure provider access and availability in terms of the time needed for a member to reach the doctor's office; |
| |
| • | our quality improvement programs must emphasize member education and outreach and include measures designed to promote utilization of preventive services; |
| |
| • | we must have linkages with schools, city or county health departments and other community-based providers of health care in order to demonstrate our ability to coordinate all of the sources from which our members may receive care; |
| |
| • | we must have the capability to meet the needs of disabled members; |
| |
| • | our providers and member service representatives must be able to communicate with members who do not speak English or who are hearing impaired; and |
| |
| • | our member handbook, newsletters and other communications must be written at the prescribed reading level and must be available in languages other than English. |
Once awarded, our Medicaid program contracts generally have terms of one to three years. Most of these contracts provide for renewal upon mutual agreement of the parties, or at the option of the government agency, and both parties have certain early termination rights. In addition to the operating requirements listed above, state contract requirements and regulatory provisions applicable to us generally set forth detailed provisions relating to subcontractors, marketing, safeguarding of member information, fraud and abuse reporting and grievance procedures.
Our Medicaid plans are subject to periodic financial and informational reporting and comprehensive quality assurance evaluations. We regularly submit periodic utilization reports, operations reports and other information to the appropriate Medicaid program regulatory agencies.
Our compliance with the provisions of our contracts is subject to monitoring or examination by state regulators. Certain contracts require us to be subject to quality assurance evaluations by a third-party organization.
Medicare programs
Medicare is a federal health insurance program that provides eligible persons age 65 and over and some disabled persons a variety of hospital, medical insurance and prescription drug benefits. Medicare beneficiaries have the option to enroll in various types of MA plans, such as MA CCP plans, PPO benefit plans or MA PFFS plans, in areas where such plans are offered. Under MA, managed care plans contract with CMS to provide benefits that are comparable to, or that may be more attractive to Medicare beneficiaries than, Original Medicare in exchange for a fixed monthly payment per member that varies based on the county in which a member resides, the demographics of the member and the member's health condition. Currently, we only offer CCP plans under the MA program.
Along with other Part D plans, both PDPs and Medicare Advantage-Prescription Drug Plans ("MA-PDs"), we bid on providing Part D benefits in June of each year. Based on the bids submitted, CMS establishes a national benchmark. CMS pays the Part D plans a percentage of the benchmark on a PMPM basis with the remaining portion of the premium being paid by the Medicare member. Members whose income falls below 150% of the federal poverty level qualify for the federal LIS, through which the federal government helps pay the member's Part D premium and certain other cost sharing expenses.
Each of our MA health plans and our PDP plan contract with CMS are on a calendar-year basis. CMS requires that each plan meet certain regulatory requirements including, as applicable: provisions related to enrollment and disenrollment; restrictions on marketing activities; benefits or formulary requirements; quality assessment; fraud, waste and abuse monitoring; maintaining relationships with health care providers; and responding to appeals and grievances.
Our MA and PDP plans perform ongoing monitoring of our compliance with the CMS requirements, including functions performed by vendors. From time to time, CMS conducts examinations of our compliance with the provisions of our MA and PDP contracts.
Licensing and Solvency Regulation
Our operations are conducted primarily through HMO and insurance subsidiaries. These subsidiaries are licensed by the insurance department in the state in which they operate, except our New York HMO subsidiary, which is licensed as a prepaid health services plan by the New York State Department of Health, and our California HMO, which is licensed by the California Department of Managed Health Care. The subsidiaries are subject to the rules, regulation and oversight of the applicable state agencies in the areas of licensing and solvency. State insurance laws and regulations prescribe accounting practices for determining statutory net income and capital and surplus. Each of our regulated subsidiaries is required to report regularly on its operational and financial performance to the appropriate regulatory agency in the state in which it is licensed. These reports describe each of our regulated subsidiaries' capital structure, ownership, financial condition, certain intercompany transactions and business operations. From time to time, any of our regulated subsidiaries may be selected to undergo periodic audits, examinations or reviews by the applicable state agency of our operational and financial assertions.
Our regulated subsidiaries generally must obtain approval from, or provide notice to, the state in which it is domiciled before entering into certain transactions such as declaring dividends in excess of certain thresholds, entering into other arrangements with related parties, acquisitions or similar transactions involving an HMO or insurance company, or any change in control. For purposes of these laws, in general, control commonly is presumed to exist when a person, group of persons or entity, directly or indirectly, owns, controls or holds the power to vote 10% or more of the voting securities of another entity.
Each of our HMO and insurance subsidiaries must maintain a minimum amount of statutory capital determined by statute or regulation. The minimum statutory capital requirements differ by state and are generally based on a percentage of annualized premium revenue, a percentage of annualized health care costs, a percentage of certain liabilities, a statutory minimum, risk-based capital ("RBC") requirements or other financial ratios. The RBC requirements are based on guidelines established by the NAIC, and have been adopted by most states. As of December 31, 2012, our HMO operations in all states except California, New York, and Florida were subject to RBC requirements. The RBC requirements may be modified as each state legislature deems appropriate for that state. The RBC formula, based on asset risk, underwriting risk, credit risk, business risk and other factors, generates the authorized control level ("ACL"), which represents the amount of capital required to support the regulated entity's business. For states in which the RBC requirements have been adopted, the regulated entity typically must maintain a minimum of the greater of 200% of the required ACL or the minimum statutory net worth requirement calculated pursuant to pre-RBC guidelines. Our subsidiaries operating in Texas and Ohio are required to maintain statutory capital at RBC levels equal to 225% and 300%, respectively, of the applicable ACL. Failure to maintain these requirements would trigger regulatory action by the state. At December 31, 2012, our HMO and insurance subsidiaries were in compliance with these minimum capital requirements. The combined statutory capital and surplus of our HMO and insurance subsidiaries was approximately $926.0 million and $858.0 million at December 31, 2012 and 2011, respectively, compared to the required surplus of approximately $383.0 million and $310.0 million at December 31, 2012 and 2011, respectively.
The statutory framework for our regulated subsidiaries' minimum capital requirements changes over time. For instance, RBC requirements may be adopted by more of the states in which we operate. These subsidiaries are also subject to their state regulators' overall oversight powers. For example, the state of New York adopted regulations that increase the reserve requirement annually until 2018. In addition, regulators could require our subsidiaries to maintain minimum levels of statutory net worth in excess of the amount required under the applicable state laws if the regulators determine that maintaining such additional statutory net worth is in the best interest of our members and other constituencies. Moreover, if we expand our plan offerings in a state or pursue new business opportunities, we may be required to make additional statutory capital contributions.
In addition to the foregoing requirements, our regulated subsidiaries are subject to restrictions on their ability to make dividend payments, loans and other transfers of cash. Dividend restrictions vary by state, but the maximum amount of dividends which can be paid without prior approval from the applicable state is subject to restrictions relating to statutory capital, surplus and net income for the previous year. Some states require prior approval of all dividends, regardless of amount. States may disapprove any dividend that, together with other dividends paid by a subsidiary in the prior 12 months, exceeds the regulatory maximum as computed for the subsidiary based on its statutory surplus and net income. For the years ended December 31, 2012, 2011 and 2010, we received $192.0 million, $92.0 million and $45.7 million respectively, in cash dividends from our regulated subsidiaries.
Also, we may only invest in the types of investments allowed by a particular state in order to qualify as admitted assets in that state and we are required by certain states to deposit or pledge assets that are considered restricted assets. At December 31, 2012 and 2011, our restricted assets consisted of cash and cash equivalents, money market accounts, certificates of deposits, and U.S. government securities.
HIPAA and State Privacy Laws
The Health Insurance Portability and Accountability Act of 1996 ("HIPAA") and the regulations adopted under HIPAA are intended to improve the portability and continuity of health insurance coverage and simplify the administration of health insurance claims and related transactions. All health plans, including ours, are subject to HIPAA. HIPAA generally requires health plans to:
| |
| • | protect the privacy and security of patient health information through the implementation of appropriate administrative, technical and physical safeguards; and |
| |
| • | establish the capability to receive and transmit electronically certain administrative health care transactions, such as claims payments, in a standardized format. |
We are also subject to state laws that provide for greater privacy of individuals' health information; such laws are not preempted by HIPAA.
Fraud and Abuse Laws
Federal and state enforcement authorities have prioritized the investigation and prosecution of health care fraud, waste and abuse. Fraud, waste and abuse prohibitions encompass a wide range of operating activities, including kickbacks or other inducements for referral of members or for the coverage of products (such as prescription drugs) by a plan, billing for unnecessary medical services by a provider, improper marketing and violation of patient privacy rights. Companies involved in public health care programs such as Medicaid and Medicare are required to maintain compliance programs to detect and deter fraud, waste and abuse, and are often the subject of fraud, waste and abuse investigations and audits. The regulations and contractual requirements applicable to participants in these public-sector programs are complex and subject to change. Although we have structured our compliance program with care in an effort to meet all statutory and regulatory requirements, our policies and procedures are continuously under review and subject to updates and our training and education programs are always evolving. We have invested significant resources to enhance our compliance efforts, and we expect to continue to do so.
Federal and state laws and regulations governing submission of information and claims to agencies
We are subject to federal and state laws and regulations that apply to the submission of information and claims to various agencies. For example, the federal False Claims Act provides, in part, that the federal government may bring a lawsuit against any person or entity who it believes has knowingly presented, or caused to be presented, a false or fraudulent request for payment from the federal government, or who has made a false statement or used a false record to get a claim approved. The federal government has taken the position that claims presented in violation of the federal anti-kickback statute may be considered a violation of the federal False Claims Act. Violations of the False Claims Act are punishable by treble damages and penalties of up to a specified dollar amount per false claim. In addition, a special provision under the False Claims Act allows a private person (for example, a "whistleblower" such as a disgruntled former associate, competitor or member) to bring an action under the False Claims Act on behalf of the government alleging that an entity has defrauded the federal government and permits the private person to share in any settlement of, or judgment entered in, the lawsuit.
A number of states, including states in which we operate, have adopted false claims acts that are similar to the federal False Claims Act.
PRINCIPAL EXECUTIVE OFFICES
Our principal executive offices are located at 8725 Henderson Road, Renaissance One, Tampa, Florida 33634, and our telephone number is (813) 290-6200.
AVAILABILITY OF REPORTS AND OTHER INFORMATION
Our corporate website is http://www.wellcare.com. We make available on this website or in print, free of charge, our Annual Report on Form 10-K, Quarterly Reports on Form 10-Q, Current Reports on Form 8-K, Proxy Statement and amendments to those materials filed or furnished pursuant to Section 13(a) or 15(d) of the Securities and Exchange Act of 1934, as amended, as soon as reasonably practicable after we electronically file such materials with, or furnish such materials to, the Securities and Exchange Commission ("SEC").
Also available on our website, or in print to any stockholder upon request, are WellCare's Corporate Governance Guidelines and Code of Conduct and Business Ethics, as well as charters of the following committees of the Board of Directors: the Audit and Finance Committee, Compensation Committee, Health Care Quality and Access Committee, Nominating and Corporate Governance Committee and Regulatory Compliance Committee. In addition, we intend to disclose any amendments to, or waivers of, our Code of Conduct and Business Ethics on our website. To obtain printed materials contact Investor Relations at WellCare Health Plans, Inc., 8725 Henderson Road, Tampa, Florida 33634. In addition, the SEC's website is http://www.sec.gov. The SEC makes available on its website, free of charge, reports, proxy and information statements, and other information regarding issuers, such as us, that file electronically with the SEC. Information provided on our website or on the SEC's website is not part of this Annual Report on Form 10-K.
Item 1A. Risk Factors
You should carefully consider the following factors, together with all of the other information included in this report, in evaluating our company and our business. If any of the following risks actually occur, our business, financial condition and results of operations could be materially and adversely affected, and the value of our stock could decline. The risks and uncertainties described below are those that we currently believe may materially affect our company. Additional risks and uncertainties not presently known to us or that we currently deem immaterial also may impair our business operations. As such, you should not consider this list to be a complete statement of all potential risks or uncertainties.
Risks Related to Our Business
Failure to maintain satisfactory quality scores could negatively impact our premium rates, subject us to penalties, limit or reduce our membership, impede our ability to compete for new business in existing or new markets or result in the termination of our contracts.
Quality scores are used by certain agencies to establish premium rates or, in the case of CMS, to pay bonuses to better-performing MA plans that enable those plans to offer improved member health benefits to attract more members. In certain states, plans that do not meet the quality measures can be required to refund premiums previously received, or pay penalties, or the plan may be subject to enrollment limitations, including suspension of auto assignment of members, or termination of the contract. If the state determines that we have failed to meet the contractual requirements, these contracts may be subject to termination, or other remedies, at the discretion of the state. We are unable to predict what actions the state may take, if any, when assessing our contractual performance.
In addition, lower quality scores compared to our competitors may result in us losing potential new business in new markets, obtaining regulatory approval for acquisitions and expansions or dissuading potential members from choosing our plan in markets in which we already compete. As a result, lower quality scores compared to our competitors could have a material adverse effect on our rate of growth.
Medicaid premiums are fixed by contract and do not permit us to increase our premiums during the contract term, therefore, if we are unable to estimate and manage medical benefits expense effectively, our profitability likely will be reduced or we could cease to be profitable.
Our profitability depends, to a significant degree, on our ability to predict and effectively manage our costs related to the provision of health care services. Relatively small changes in the ratio of our expenses related to health care services to the premiums we receive, or medical benefits ratio, can create significant changes in our financial results. Factors that may cause medical benefits expense to exceed our estimates include:
| |
| • | the addition of new members, whether by acquisition, new enrollment, program startup or expansion, whose risk profiles are uncertain or unknown and for whom initiatives to manage their care take longer than expected; |
| |
| • | an increase in the cost of health care services and supplies, including pharmaceuticals, whether as a result of inflation or otherwise; |
| |
| • | higher-than-expected utilization of health care services; |
| |
| • | periodic renegotiation of hospital, physician and other provider contracts; |
| |
| • | the occurrence of catastrophes, major epidemics, terrorism or bio-terrorism; |
| |
| • | changes in the demographics of our members and medical trends affecting them; and |
| |
| • | new mandated benefits, increased mandated provider reimbursement rates or other changes in health care laws, regulations and/or practices. |
If our medical benefits expense increases and we are unable to manage these medical costs effectively in the future, our profits could be reduced or we may not remain profitable.
Most of our revenues are generated by premiums consisting of fixed monthly payments per member and supplemental payments for other services such as maternity deliveries, determined by the types of members in our plans. These payments are fixed by contract and we are obligated during the contract period, which is generally one to four years, to provide or arrange for the provision of health care services as established by states and the federal government. The payments are generally set based on an estimation of the medical costs using actuarial methods based on historical data. Actual experience, however, could differ from the assumptions used in the premium-setting process, which could result in premiums being insufficient to cover our medical benefits expense. If our medical benefits expense exceeds our estimates or our regulators' actuarial pricing assumptions, and we are unable to adjust the premiums we receive under our current contracts, it could have a material adverse effect on our results of operations.
In particular, our Medicaid plan in Kentucky has operated at an MBR of greater than 100% for each period since we began our operations there in November 2011. While we have begun to improve care coordination to manage costs, and we have received revenue enhancements from Kentucky, we cannot be assured that these efforts will be successful or sufficient. In addition, one of the other managed care plans in Kentucky announced its intention to terminate its contract with the commonwealth effective July 2013, and some of those members may be transferred to our plan; however, the plan may decide to remain in Kentucky or we may not be allocated any of these members even if the other plan does exit Kentucky. The addition of these members may adversely impact our MBR in Kentucky.
In addition, there are sometimes wide variations in the established rates per member in both our Medicaid and Medicare lines of business. For instance, the rates we receive for an SSI member are generally significantly higher than for a non-SSI member who is otherwise similarly situated. As the composition of our membership base changes as the result of programmatic, competitive, regulatory, benefit design, economic or other changes, there is a corresponding change to our premium revenue, costs and margins, which may have a material adverse effect on our cash flow and results of operations.
Our membership is concentrated in certain geographic areas in the U.S., and unfavorable changes in health care or other benefit costs or reimbursement rates or increased competition in those geographic areas could therefore have a disproportionately adverse effect on our operating results.
Some provider contracts are directly tied to state Medicaid fee schedules, which the state or CMS may adjust without granting a corresponding increase in premiums to us. For example, in Florida the state is considering implementing changes to the Medicaid fee schedules, which may increase our reimbursement rates to providers. We have experienced such adjustments in the states in which we operate. Unless such adjustments are mitigated by an increase in premiums, or if this were to occur in any more of the states in which we operate, our profitability will be negatively impacted.
Also, in some rural areas, it is difficult to maintain a provider network sufficient to meet regulatory requirements. In situations where we have a deficiency in our provider network, regulators require us to allow members to obtain care from out-of-network providers at no additional cost, which could have a material adverse effect on our ability to manage expenses. In some states, with respect to certain services, the amount that the health plan must pay to out-of-network providers for services provided to our members is defined by law or regulation, but in certain instances it is either not defined or it is established by a standard that is not clearly translatable into dollar terms. Out-of-network providers may believe they are underpaid for their services and may either litigate or arbitrate their dispute with the health plan. The uncertainty of the amount to pay and the possibility of subsequent adjustments of the payment could adversely affect our financial position, results of operations or cash flows.
Although we maintain reinsurance to protect us against certain severe or catastrophic medical claims, we cannot assure you that such reinsurance coverage currently is or will be adequate or available to us in the future or that the cost of such reinsurance will not limit our ability to obtain it.
Difficulties in successfully executing acquisitions, expansions and other significant transactions may have a material adverse effect on our results of operations, financial position and cash flows.
As part of our prudent, profitable growth strategy, we identify potential acquisition targets, bid and negotiate acquisition terms, work with regulators to receive regulatory approval for the acquisition and once the transaction is closed, we must integrate the acquisition into our operations. In 2012, we completed two acquisitions, Easy Choice in California and Desert Canyon in Arizona, and in January 2013, we completed our acquisition of UnitedHealth Group Incorporated's South Carolina Medicaid plan. Our acquisition of Aetna, Inc.'s Missouri Medicaid plan is pending closing.
Once an attractive acquisition target is identified, we may not be successful in bidding against competitors. Other potential acquirers may have greater financial resources or different profitability criteria than we have. Depending on the transaction size, we may not be able to obtain appropriate financing, especially in light of the volatility in the capital markets over the past several years.
Even if we are successful in bidding against competitors, we may not be able to obtain the regulatory approval from federal and state agencies required to complete the acquisition. We may not be able to comply with the regulatory requirements necessary for approval of the acquisition or state regulators may give preference to competing offers made by locally-owned entities, competitors with higher quality scores or not-for-profit entities.
In addition, when making award determinations and regulatory approvals of acquisitions and expansions, regulators frequently consider the plan's historical regulatory compliance, litigation and reputation and we are required to disclose material investigations and litigation, including in some cases investigations and litigation that occurred in the past. As a result of the previous federal and state investigations, stockholder and derivative litigation, restatement during 2009 of our previously issued financial statements and related matters, and the criminal trial of certain of our former executives and employees that is scheduled to begin in the first quarter of 2013, we have been, and may continue to be, the subject of negative publicity. As a result, continuing negative publicity and other negative perceptions regarding these matters may adversely affect our ability to grow.
Once acquired, we may have difficulties integrating the businesses within our existing operations, due to:
| |
| • | associates who must become familiar with our operations and corporate culture; |
| |
| • | acquired provider networks which operate on different terms than our existing networks and whose contracts may need to be renegotiated; |
| |
| • | existing members who decide to switch to another health care plan; |
| |
| • | disparate administrative and information technology systems; and |
| |
| • | difficulties implementing our operations strategy to operate the acquired businesses profitably. |
Furthermore, we may incur significant transaction expenses in connection with a potential acquisition or expansion opportunity which may not be successful. These expenses could impact our selling, general and administrative expense ratio. If we are unable to effectively execute our acquisition strategy or integrate acquired businesses, our future growth may suffer and our profitability may decrease.
Our rate of expansion into other geographic areas may also be inhibited by:
| |
| • | the time and costs associated with obtaining the necessary license to operate in the new area or the expansion of our licensed service area, if necessary; |
| |
| • | lower quality scores compared to our competitors; |
| |
| • | participation in fewer lines of business compared to our competitors; |
| |
| • | our inability to develop a network of physicians, hospitals and other health care providers that meets our requirements and those of government regulators; |
| |
| • | CMS or state contract provisions regarding quality measures, such as CMS star ratings; |
| |
| • | competition, which increases the cost of recruiting members; |
| |
| • | the cost of providing health care services in those areas; |
| |
| • | demographics and population density; and |
| |
| • | applicable state regulations that, among other things, require the maintenance of minimum levels of capital and surplus. |
In any program start-up, acquisition, expansion, or re-bid, the implementation of the contract as designed may be affected by factors beyond our control. These include political considerations, network development, contract appeals, incumbency, participation in other lines of business, membership assignment (allocation of members who do not self-select), errors in the bidding process, difficulties experienced by other private vendors involved in the implementation, such as enrollment brokers, and noncompliance with contractual requirements with which we do not yet have experience and similar risks. Our business, particularly plans for expansion or increased membership levels, could be negatively impacted by these delays or changes.
Growth could also place a significant strain on our management and on other resources and we are likely to incur additional costs if we enter states or counties where we do not currently operate. Our ability to manage our growth may depend on our ability to retain and strengthen our management team; attract, train and retain skilled associates; and implement and improve operational, financial and management information systems on a timely basis. If we are unable to manage our growth effectively, our financial condition and results of operations could be materially and adversely affected. In addition, due to the initial substantial costs related to acquisitions and expansions, such growth could materially adversely affect our short-term profitability and liquidity.
Future changes in health care law present challenges for our business that could have a material adverse effect on our results of operations and cash flows.
Future changes in existing health care laws or regulations, or their interpretations, or the enactment of new laws or the issuance of new regulations could materially reduce our revenue and/or profitability by, among other things:
| |
| • | imposing additional license, registration and/or capital requirements; |
| |
| • | increasing our administrative and other costs; |
| |
| • | requiring us to change our operating structure; |
| |
| • | increasing mandated benefits; |
| |
| • | further limiting our ability to engage in intra-company transactions with our affiliates and subsidiaries; |
| |
| • | restricting our revenue and enrollment growth; |
| |
| • | requiring us to restructure our relationships with providers; or |
| |
| • | requiring us to implement additional or different programs and systems. |
Requirements relating to increased plan information disclosure, expedited appeals and grievance procedures, third party review of certain medical decisions, health plan liability, access to specialists, "clean claim" payment timing (claims for which no additional information is needed), mandated increases in provider reimbursement rates, physician collective bargaining rights and confidentiality of medical records either have been enacted or are under consideration. Changes in state law, regulations and rules also may materially adversely affect our profitability.
We believe The Patient Protection and Affordable Care Act and The Health Care and Education Reconciliation Act of 2010 (collectively, the "2010 Acts") will bring about significant changes to the American health care system. These measures are intended to expand the number of United States residents covered by health insurance and make other coverage, delivery, and payment changes to the current health care system. The costs of implementing the 2010 Acts will be financed, in part, from substantial additional fees and taxes on us and other health insurers, health plans and individuals, as well as reductions in certain levels of payments to us and other health plans under Medicare.
The 2010 Acts will also impose certain new taxes and fees, including limitations on the amount of compensation that is tax deductible and annual assessments on all health insurers, worth approximately $8 billion beginning in 2014, which will increase in subsequent years. The imposition of this assessment will impact our operating margins. In addition, in states in which we compete with not-for profit Medicaid health plans, we may need to reduce margins in order to assure price competitiveness. As a result, this new tax may have a material adverse effect on our results of operations, financial position and cash flows.
On June 28, 2012, the U.S. Supreme Court upheld the constitutionality of the individual mandate contained in the 2010 Acts and modified the Medicaid expansion provisions to make the expansion optional for states. Some states have decided not to participate in the Medicaid expansion, and more states may choose not to participate in the future. Congress may also withhold the funding necessary to fully implement the 2010 Acts or may attempt to replace the legislation with amended provisions or repeal it altogether. Given the breadth of possible changes and the uncertainties of interpretation, implementation, and timing of these changes, which we expect to occur over the next several years, the 2010 Acts could change the way we do business, potentially impacting our pricing, benefit design, product mix, geographic mix, and distribution channels.
Regulations related to the 2010 Acts, as well as future legislative changes, in the aggregate may have a material adverse effect on our results of operations, financial position, and cash flows by restricting revenue, enrollment and premium growth in certain products and market segments; restricting our ability to expand into new markets; increasing our medical and administrative costs; lowering our Medicare payment rates and/or increasing our expenses associated with the non-deductible federal premium tax and other assessments. In addition, the response of other companies to the 2010 Acts and adjustments to their offerings, if any, could have a meaningful impact in the health care markets.
The 2010 Acts include a number of changes that could impact the way MA plans will operate, such as:
| |
| • | Reduced Medicare Premium Rates. In 2012, MA plans received a range of 95% of Medicare fee-for-service costs in high-cost areas to 115% of Medicare fee-for-service costs in low-cost areas, with changes being phased-in over two to six years, depending on the level of payment reduction in a county. |
| |
| • | CMS Star Ratings. Certain provisions in the 2010 Acts tie MA premiums to the achievement of Star Ratings. Beginning in 2012, MA plans with an overall Star Rating of three or more stars (out of five) are eligible for a quality bonus in their basic premium rates. Initially, quality bonuses were limited to the few plans that achieved a four or higher overall Star Rating, but CMS expanded the quality bonus to plans with a three overall Star Rating for a three year period through 2014. Members of Congress have challenged whether CMS had the authority to expand the quality bonus. We cannot predict the ultimate resolution of this matter or the impact on our plans' quality bonus eligibility. Plans that receive quality bonuses may have a competitive advantage in the Medicare market, as they may be able to offer more attractive benefit packages to members and/or achieve higher profit margins. Also, beginning with open enrollment for the 2014 plan year, Part C or Part D Medicare plans with Star Ratings of less than three stars for three consecutive years will be excluded from mention in the CMS "Medicare and You" handbook, denoted as "low performing" plans on the CMS website, and excluded from on-line enrollment through the Medicare Plan Finder website. These actions may adversely impact these plans' ability to maintain or increase membership. In addition, in April 2012, CMS announced that Part C and Part D Medicare plans with an overall Star Rating of less than three stars for three consecutive years may be terminated at CMS' discretion beginning on January 1, 2015. Some of our plans have less than three stars. While we are continuing efforts to improve our Star Ratings and other quality measures for 2013 and beyond, there is no guarantee that we will be able to maintain or improve our Star Ratings in future years. |
| |
| • | Minimum MLRs. Beginning in 2014, the 2010 Acts require MA plans to spend not less than 85% of premiums on medical benefits. While the Department of Health and Human Services ("HHS") has issued rules clarifying the definitions and minimum medical loss ratio ("MLR") requirements for certain commercial health plans, it has not issued rules or guidance specific to Medicare plans. The rules that have been issued impose financial and other penalties for failing to achieve the minimum MLR ratio, including requirements to refund to CMS shortfalls in amounts spent on medical benefits and termination of a plan's MA contract for prolonged failure to achieve the minimum MLR ratio. CMS is considering imposing the minimum MLR on Part D plans as well. |
From 2010 through 2020, the "coverage gap" (i.e., the dollar threshold at which an individual has to pay full price for his or her medications) under Part D will be gradually closed, with beneficiaries retaining a 25% co-pay. While this change ultimately results in increased insurance coverage, such improved benefits could result in changes in member behavior with respect to drug utilization. Such actions could also impact the cost structure of our Part D programs.
The health reforms in the 2010 Acts present both challenges and opportunities for our Medicaid business. The reforms allow states to expand eligibility for Medicaid programs. However, state budgets continue to be strained due to economic conditions and uncertain levels of federal financing for current populations. As a result, the effects of any potential future expansions are uncertain, making it difficult to determine whether the net impact of the 2010 Acts will be positive or negative for our Medicaid business.
We encounter significant competition for program participation, members, network providers, key personnel and sales personnel and our failure to compete successfully may limit our ability to increase or maintain membership in the markets we serve, or have a material adverse effect on our growth prospects and results of operations.
We operate in a highly competitive industry. Some of our competitors are more established in the insurance and health care industries, with larger market share, greater financial resources and better quality scores than we have in some markets. We operate in, or may attempt to acquire business in, programs or markets in which premiums are determined on the basis of a competitive bidding process. In these programs or markets, funding levels established by bidders with significantly different cost structures, target profitability margins or aggressive bidding strategies could negatively impact our ability to maintain or acquire profitable business which could have a material adverse effect on our results of operations.
Regulatory reform or other initiatives may bring additional competitors into our markets. Regulators may prefer companies that operate in multiple lines of business when we bid on new business or renewals of existing business, in which we may not operate.
We compete for members principally on the basis of size and quality of provider network, benefits provided and quality of service. We may not be able to develop innovative products and services which are attractive to members. We cannot be sure that we will continue to remain competitive, nor can we be sure that we will be able to successfully acquire members for our products and services at current levels of profitability.
In addition, we compete with other health plans to contract with hospitals, physicians, pharmacies and other providers for inclusion in our networks that serve government program beneficiaries. We believe providers select plans in which they participate based on several criteria including reimbursement rates, timeliness and accuracy of claims payment, potential to deliver new patient volume and/or retain existing patients, effectiveness of resolution of calls and complaints and other factors. We cannot be sure that we will be able to successfully attract or retain providers to maintain a competitive network in the geographic areas we serve.
We may not be able to attract or retain qualified management, clinical and commercial personnel in the future due to the intense competition for qualified personnel in the managed care and health care industry and other businesses. If we are not able to attract and retain necessary personnel to accomplish our business objectives, we may experience constraints that will significantly impede the achievement of our objectives, our ability to raise additional capital and our ability to implement our business strategy. In particular, if we lose any members of our senior management team, we may not be able to find suitable replacements, and our business may be harmed as a result.
Our MA plans are sold primarily through our sales personnel, who frequently work with independent brokers, consultants and agents who assist in the production and servicing of business. The independent brokers, consultants and agents generally are not dedicated to us exclusively and may frequently also recommend and/or market health care benefits products of our competitors, and we must compete intensely for their services and allegiance. Our sales could be adversely affected if we are unable to attract or retain sales personnel and third-party brokers, consultants and agents or if we do not adequately provide support, training and education to this sales network regarding our product portfolio, which is complex, or if our sales strategy is not appropriately aligned across distribution channels.
To the extent that competition intensifies in any market that we serve, our ability to retain or increase members and providers, maintain or increase our revenue growth, and control medical cost trends, and/or our pricing flexibility, may be adversely affected. Failure to compete successfully in the markets we serve may have a material adverse effect on our growth prospects and results of operations. For a discussion of the competitive environment in which we operate, see Part I, Item 1 – Business – Competition.
Risk-adjustment payment systems make our revenue and results of operations more difficult to predict and could result in material retroactive adjustments that have a material adverse effect on our results of operations.
Most of our government customers employ risk-adjustment models to determine the premium amount they pay for each member. This model pays more for members with predictably higher costs according to the health status of each beneficiary enrolled. Premium payments are generally established at fixed intervals according to the contract terms, and then adjusted on a retroactive basis. We reassess the estimates of the risk adjustment settlements each reporting period and any resulting adjustments are made to premium revenue.
As a result of the variability of certain factors that determine estimates for risk-adjusted premiums, including plan risk scores, the actual amount of retroactive payment could be materially more or less than our estimates. Consequently, our estimate of our plans' risk scores for any period, and any resulting change in our accrual of premium revenues related thereto, could have a material adverse effect on our results of operations, financial position and cash flows. The data provided to our government customers to determine the risk score are subject to audit by them even after the annual settlements occur. These audits may result in the refund of premiums to the government customer previously received by us, which could be significant and would reduce our premium revenue in the year that repayment is required.
Government customers have performed and continue to perform audits of selected plans to validate the provider coding practices under the risk adjustment model used to calculate the premium paid for each member. It is likely that a payment adjustment will occur as a result of these audits, and that any such adjustment could have a material adverse effect on our results of operations, financial position, and cash flows.
Our Medicaid operations are concentrated in a limited number of states. Loss of a material contract, reduced premium rates, or delayed payment of earned premiums may adversely impact our business.
Our concentration of operations in a limited number of states could cause our revenue, profitability or cash flow to change suddenly and unexpectedly as a result of significant premium rate reductions or payment delays, a loss of a material contract, legislative actions, changes in Medicaid eligibility methodologies, catastrophic claims, an epidemic or pandemic, or an unexpected increase in utilization, general economic conditions and similar factors in those states. Our inability to continue to operate in any of these states, or a significant change in the nature of our existing operations, could adversely affect our business, financial condition, or results of operations.
We provide managed care programs and selected services to individuals receiving benefits under federal assistance programs, including Medicare Advantage, Medicaid, CHIP and ABD. We provide those health care services under contracts with regulatory entities in the areas in which we operate. For the year ended December 31, 2012, three of our Medicaid customers each accounted for greater than 10% of our consolidated premium revenue, net of premium taxes. These customers (Florida, Georgia and Kentucky) accounted for contracts that have terms of between one and three years with varying expiration dates.
Our Florida Medicaid contracts expire in August 2015, however we currently anticipate that these will be terminated early, possibly as early as the end of 2013. The Florida agency that operates the state's Medicaid program recently began a competitive procurement process to award contracts for Medicaid managed care across the state. The agency expects to award contracts under the competitive procurement in 2013. We currently intend to submit a proposal under this process but we cannot assure you our proposal will be successful.
Our contracts with other states are generally intended to run for one to three years and in some cases may be extended for one or two additional years if the state or its agent elects to do so. Our current state contracts are set to expire or renew between June 2013 and December 2015. When our state contracts expire, they may be opened for bidding by competing health care providers. There is no guarantee that our contracts will be renewed or extended. Further, our contracts with the states are subject to cancellation by the state after a short notice period in the event of unavailability of state funds. Our contracts could also be terminated if we fail to perform in accordance with the standards set by state regulatory agencies. If any of our contracts are terminated, not renewed, renewed on less favorable terms, or not renewed on a timely basis, or if an increased number of competitors were awarded contracts in these states, our business will suffer, and our financial position, results of operations or cash flows may be materially affected.
State governments generally are experiencing tight budgetary conditions within their Medicaid programs due to difficult macroeconomic conditions and increases in the Medicaid eligible population. We anticipate this will require government agencies with which we contract to find funding alternatives, which may result in reductions in funding. If any state in which we operate were to decrease premiums paid to us, or pay us less than the amount necessary to keep pace with our cost trends, it could have a material adverse effect on our revenues and results of operations. Economic conditions affecting state governments and agencies could also result in delays in receiving premium payments. If there is a significant delay in our receipt of premiums to pay health benefit costs, it could have a material adverse effect on our results of operations, cash flows and liquidity.
A significant percentage of our Medicaid plan enrollment results from mandatory enrollment in Medicaid managed care plans. States may mandate that certain types of Medicaid beneficiaries enroll in Medicaid managed care through CMS-approved plan amendments or, for certain groups, through federal waivers or demonstrations. Waivers and programs under demonstrations are generally approved for two- to five-year periods, and can be renewed on an ongoing basis if the state applies and the waiver request is approved or renewed by CMS. We have no control over this renewal process. If a state in which we operate does not mandate managed care enrollment in its state plan or does not renew an existing managed care waiver, our membership would likely decrease, which could have a material adverse effect on our results of operations.
We derive a significant portion of our Medicare revenue from our PDP operations, for which we submit annual bids for participation. The results of our bids could materially impact our revenue and profits.
A significant portion of our PDP membership is obtained from the auto-assignment of beneficiaries in CMS-designated regions where our PDP premium bids are below benchmarks of other plans' bids. In general, our premium bids are based on assumptions regarding PDP membership, utilization, drug costs, drug rebates and other factors for each region. If our future Part D premium bids are not below the CMS benchmarks, we risk losing PDP members who were previously assigned to us and we may not have additional PDP members auto-assigned to us, which would materially reduce our revenue and profits.
Based on the outcome of our 2013 PDP bids, our plans are below the benchmarks in 14 of the 34 CMS regions and within the de minimis range of the benchmark in five other CMS regions. In 2013, newly-eligible members are being auto-assigned into our plans for the 14 regions that are below the benchmark. We will retain our auto-assigned members in the five regions in which we bid within the de minimis range; however, we will not be auto-assigned new members in those regions during 2013. As of January 1, 2013, the beneficiaries who had previously been auto-assigned to our plans in the 15 regions in which our bids were neither below the benchmark nor within the de minimis range were reassigned to other plans.
We are subject to extensive government regulation and risk of litigation, and any violation by us of the terms of our contracts, applicable laws or regulations could have a material adverse effect on our results of operations.
Our business is extensively regulated by the federal government and the states in which we operate. The laws and regulations governing our operations are generally intended to benefit and protect health plan members and providers rather than stockholders. The government agencies administering these laws and regulations have broad latitude to enforce them. These laws and regulations, along with the terms of our government contracts, regulate how we do business, what services we offer, and how we interact with our members, providers and the public. Any violation by us of applicable laws or regulations could reduce our revenues and profitability, thereby having a material adverse effect on our results of operations.
We face a significant risk of class action lawsuits and other litigation and regulatory investigations and actions in the ordinary course of operating our businesses. The following are examples of types of potential litigation and regulatory investigations we face:
| |
| • | claims by government agencies relating to compliance with laws and regulations; |
| |
| • | claims relating to sales practices; |
| |
| • | claims relating to the methodologies for calculating premiums; |
| |
| • | claims relating to the denial or delay of health care benefit payments; |
| |
| • | claims relating to claims payments and procedures; |
| |
| • | claims relating to provider marketing; |
| |
| • | medical malpractice or negligence actions based on our medical necessity decisions or brought against us on the theory that we are liable for our providers' alleged malpractice or negligence; |
| |
| • | allegations of anti-competitive and unfair business activities; |
| |
| • | provider disputes over compensation and termination of provider contracts; |
| |
| • | allegations of discrimination; |
| |
| • | allegations of breaches of duties; |
| |
| • | claims relating to inadequate or incorrect disclosure or accounting in our public filings; |
| |
| • | allegations of agent misconduct; |
| |
| • | claims related to deceptive trade practices; and |
| |
| • | claims relating to audits and contract performance. |
As we contract with various governmental agencies to provide managed health care services, we are subject to various reviews, audits and investigations to verify our compliance with the contracts and applicable laws and regulations. Any adverse review, audit, investigation or adverse result from litigation could result in:
| |
| • | forfeiture or recoupment of amounts we have been paid pursuant to our government contracts; |
| |
| • | imposition of significant civil or criminal penalties, fines or other sanctions on us and/or our key associates; |
| |
| • | reduction or limitation of our membership; |
| |
| • | loss of our right to participate in government-sponsored programs, including Medicaid and Medicare; |
| |
| • | damage to our reputation in various markets; |
| |
| • | increased difficulty in marketing our products and services; |
| |
| • | inability to obtain approval for future service or geographic expansion; and |
| |
| • | suspension or loss of one or more of our licenses to act as an insurer, HMO or third party administrator or to otherwise provide a service. |
In particular, because we receive payments from federal and state governmental agencies, we are subject to various laws commonly referred to as "fraud and abuse" laws, including the federal False Claims Act, which permit agencies and enforcement authorities to institute suit against us for violations and, in some cases, to seek treble damages, penalties and assessments. Many states, including states where we currently operate, have enacted parallel legislation. Liability under such federal and state statutes and regulations may arise if we know, or it is found that we should have known, that information we provide to form the basis for a claim for government payment is false or fraudulent.
Some courts have permitted False Claims Act suits to proceed if the claimant was out of compliance with program requirements. Liability for such matters could have a material adverse effect on our financial position, results of operations and cash flows. Qui tam actions under federal and state law can be brought by any individual on behalf of the government. Qui tam actions have increased significantly in recent years, causing greater numbers of health care companies to defend false claim actions, pay fines or be excluded from Medicare, Medicaid or other state or federal health care programs as a result of investigations arising out of such actions.
For example, in October 2008, the Civil Division of the United States Department of Justice (the "Civil Division") informed us that as part of its civil inquiry, it was investigating four qui tam complaints filed by relators against us under the whistleblower provisions of the False Claims Act. We also learned from a docket search that a former employee filed a qui tam action in state court for Leon County, Florida against several defendants, including us and one of our subsidiaries. With respect to these actions, in April 2012, we announced that we reached a settlement with the Civil Division, the Civil Division of the United States Attorney's Office for the Middle District of Florida, and the Civil Division of the United States Attorney's Office for the District of Connecticut. However, other qui tam actions may have been filed against us of which we are presently unaware, or other qui tam actions may be filed against us in the future.
Under Delaware law, our charter and bylaws and certain indemnification agreements to which we are a party, we have an obligation to indemnify, or we have otherwise agreed to indemnify, certain of our current and former directors, officers and associates with respect to current and future investigations and litigation. In connection with some of these pending matters, including the upcoming criminal trial of certain of our former executives and associates, we are required to, or we have otherwise agreed to, advance, and have advanced, significant legal fees and related expenses and expect to continue to do so while these matters are pending. We have exhausted our insurance for these matters, and expenses incurred by us for these matters will not be further reimbursed.
We currently maintain insurance in the amount of $125.0 million which provides coverage for our independent directors and officers hired after January 24, 2008 for certain potential matters to the extent they occur after October 2007. We cannot provide any assurances that pending claims, or claims yet to arise, will not exceed the limits of our insurance policies, that such claims are covered by the terms of our insurance policies or that our insurance carrier will be able to cover our claims.
We are currently undergoing standard periodic audits by several state agencies and CMS to verify compliance with our contracts and applicable laws and regulations. For additional risks associated with these audits, see Risk adjustment payment systems make our revenue and results of operations more difficult to predict and could result in material retroactive adjustments that have a material adverse effect on our results of operations above.
In addition, there have been a number of investigations regarding the marketing practices of brokers and agents selling health care and other insurance products and the payments they receive. These have resulted in enforcement actions against companies in our industry and brokers and agents marketing and selling those companies' products. For example, CMS and state departments of insurance have increased their scrutiny of the marketing practices of brokers and agents who market Medicare products. These investigations and enforcement actions could result in penalties and the imposition of corrective action plans and/or changes to industry practices, which could adversely affect our ability to market our products.
We rely on a number of third parties, and failure of any one of the third parties to perform in accordance with our contracts could have a material adverse effect on our business and results of operations.
Our care and service delivery model is designed to optimize our use of our personnel versus third parties based on an evaluation of factors, including cost, compliance, quality and procurement success. As a result, we have contracted with a number of third parties to provide significant operational support including, but not limited to, pharmacy benefit management and behavioral health services for our members as well as certain enrollment, billing, call center, benefit administration, claims processing functions, sales and marketing and certain aspects of utilization management. We have limited ability to control the performance of these third parties. If a third party provides services that we are required to provide under a contract with a government client, we are responsible for such performance and will be held accountable by the government client for any failure of performance by our vendors. Significant failure by a third party to perform in accordance with the terms of our contracts could subject us to fines or other sanctions or otherwise have a material adverse effect on our business and results of operations. In addition, upon termination of a third party contract, we may encounter difficulties in replacing the third party on favorable terms, or in assuming those responsibilities ourselves, which may have a material adverse effect on our business, quality scores and results of operations. Further, we rely on state-operated systems and sub-contractors to qualify and assign eligible members into our health plan. Ineffectiveness of these state operations and sub-contractors can have a material adverse effect on our enrollment.
We rely on the accuracy of eligibility lists provided by our government clients to collect premiums, and any inaccuracies in those lists may cause states to recoup premium payments from us, which could materially reduce our revenues and results of operations.
Premium payments that we receive are based upon eligibility lists produced by our government clients. A state will require us to reimburse it for premiums that we received from the state based on an eligibility list that it later discovers contains individuals who were not eligible for any government-sponsored program, have been enrolled twice in the same program or are eligible for a different premium category or a different program. Our review of remittance files may not identify all member eligibility errors and could result in repayment of premiums in years subsequent to the year in which the revenue was recorded.
In addition to recoupment of premiums previously paid, we also face the risk that a state could fail to pay us for members for whom we are entitled to payment. Our results of operations would be reduced as a result of the state's failure to pay us for related payments we made to providers and were unable to recoup. We have established a reserve in anticipation of recoupment by the states of previously paid premiums that we believe to be erroneous, but ultimately our reserve may not be sufficient to cover the amount, if any, of recoupments. If the amount of any recoupment exceeds our reserves, our revenues could be materially reduced and it could have a material adverse effect on our results of operations.
Our encounter data may be inaccurate or incomplete, which could have a material adverse effect on our results of operations, cash flows and ability to bid for, and continue to participate in, certain programs.
To the extent that our encounter data is inaccurate or incomplete, we have expended and may continue to expend additional effort and incur significant additional costs to collect or correct this data and have been and could be exposed to operating sanctions and financial fines and penalties for noncompliance. The accurate and timely reporting of encounter data is increasingly important to the success of our programs because more states are using encounter data to determine compliance with performance standards and, in part, to set premium rates. In some instances, our government clients have established retroactive requirements for the encounter data we must submit. There also may be periods of time in which we are unable to meet existing requirements. In either case, it may be prohibitively expensive or impossible for us to collect or reconstruct this historical data.
We have experienced challenges in obtaining complete and accurate encounter data, due to difficulties with providers and third-party vendors submitting claims in a timely fashion in the proper format, and with state agencies in coordinating such submissions. As states increase their reliance on encounter data these difficulties could affect the premium rates we receive and how membership is assigned to us, which could have a material adverse effect on our results of operations, cash flows and our ability to bid for, and continue to participate in, certain programs.
If we are unable to have access to sufficient capital, whether as a result of difficulties finding acceptable public or private financing, restrictions due to our existing credit agreement, restrictions on dividend payments from our subsidiaries, or higher statutory capital levels, we may be unable to grow or maintain our business, which could have a material adverse effect on our results of operations, cash flows and financial condition.
Our business strategy has been defined by three primary initiatives, one of which includes our ability to enter new markets by pursuing attractive growth opportunities for our existing product lines. We may need to access the debt or equity markets and receive dividends from our subsidiaries to fund these growth activities.
Our ability to enter new markets may be hindered in situations where we need to access the public markets and financing may not be available on terms that are favorable to us. Our ability to obtain favorable financing may be unfavorable in terms such as high rates of interest, restrictive covenants and other restrictions and could impede our ability to profitably operate our business and increase the expected rate of return we require to enter new markets, making such efforts unfeasible.
Our credit agreement has restrictions on our ability to secure additional capital. Our substantial indebtedness and restrictive covenants:
| |
| • | limit our ability to borrow additional funds for working capital, capital expenditures, acquisitions and general corporate or other purposes; and |
| |
| • | expose us to greater interest rate risk since the interest rate on borrowings under our senior credit facilities is variable. |
Our debt service obligations require us to use a portion of our operating cash flow to pay interest and principal on indebtedness instead of for other corporate purposes, including funding future expansion of our business and ongoing capital expenditures, which could impede our growth. If our operating cash flow and capital resources are insufficient to comply with the financial covenants in the credit agreement or to service our debt obligations, we may be forced to sell assets, seek additional equity or debt financing or restructure our debt which could harm our long-term business prospects.
Our credit agreement contains various restrictions and covenants that restrict our financial and operating flexibility, including our ability to grow our business or declare dividends without lender approval. If we fail to pay any of our indebtedness when due, or if we breach any of the other covenants in the instruments governing our indebtedness, one or more events of default may be triggered. If we are unable to obtain a waiver, these events of default could permit our creditors to declare all amounts owed to be immediately due and payable. If we were unable to repay indebtedness owed to our secured creditors, they could proceed against the collateral securing that indebtedness.
In addition, in most states, we are required to seek the prior approval of state regulatory authorities to transfer money or pay dividends from our regulated subsidiaries in excess of specified amounts or, in some states, any amount. Extraordinary dividends require approval by state regulators prior to declaration. If our state regulators do not approve payments of dividends and/or distributions by certain of our regulated subsidiaries to us or our non-regulated subsidiaries, our liquidity, unregulated cash flows, business and financial condition may be materially adversely affected.
Our licensed HMO and insurance subsidiaries are subject to state regulations that, among other things, require the maintenance of minimum levels of statutory capital and maintenance of certain financial ratios, as defined by each state. One or more of these states may raise the statutory capital level from time to time, which could have a material adverse effect on our cash flows and liquidity.
Our subsidiaries also may be required to maintain higher levels of statutory capital due to the adoption of risk-based capital requirements by other states in which we operate. Our subsidiaries are subject to their state regulators' general oversight powers. Regardless of whether a state adopts the risk-based capital requirements, the state's regulators can require our subsidiaries to maintain minimum levels of statutory net worth in excess of amounts required under the applicable state laws if they determine that maintaining such additional statutory net worth is in the best interests of our members and other constituents. For example, if premium rates are inadequate, reduced profits or losses in our regulated subsidiaries may cause regulators to increase the amount of capital required. Any additional capital contribution made to one or more of the affected subsidiaries could have a material adverse effect on our liquidity, cash flows and growth potential. In addition, increases of statutory capital requirements could cause us to withdraw from certain programs or markets where it becomes economically difficult to continue operating profitably.
If we commit a material breach of our Corporate Integrity Agreement, we may be excluded from certain programs, resulting in the revocation or termination of contracts and/or licenses potentially having a material adverse effect on our results of operations.
On April 26, 2011, we entered into a Corporate Integrity Agreement (the "Corporate Integrity Agreement") with the Officer of Inspector General of the Department of Health and Human Services ("OIG-HHS"). The Corporate Integrity Agreement has a term of five years and concludes the previously disclosed matters relating to us under review by OIG-HHS. The Corporate Integrity Agreement requires us to maintain various ethics and compliance programs that were designed to help ensure our ongoing compliance with federal health care program requirements. The terms of the Corporate Integrity Agreement include certain organizational structure requirements, internal monitoring requirements, compliance training, screening processes for new employees, requirements for reporting to OIG-HHS, and the engagement of an independent review organization to review and prepare written reports regarding, among other things, our reporting practices and bid submissions to federal health care programs.
If we fail to comply with the terms of the Corporate Integrity Agreement we may be required to pay certain monetary penalties. Furthermore, if we commit a material breach of the Corporate Integrity Agreement, OIG-HHS may exclude us from participating in federal health care programs. Any such exclusion would result in the revocation or termination of contracts and/or licenses and potentially have a material adverse effect on our results of operations.
We are exposed to fluctuations in the securities and debt markets, which could impact our investment portfolio.
Our investment portfolio represents a significant portion of WellCare's assets and is subject to general credit, liquidity, market and interest rate risks. Market fluctuations in the securities and credit markets could impact the value or liquidity of our investment portfolio and adversely impact interest income. As a result, we may experience a reduction in value or loss of liquidity which may materially impact our results of operations, liquidity and financial condition.
Risks Related to Ownership of Our Stock
We are subject to laws, government regulations and agreements that may delay, deter or prevent a change in control of our Company, which could have a material adverse effect on our ability to enter into transactions favorable to stockholders.
Our operating subsidiaries are subject to state laws that require prior regulatory approval for any change of control of an HMO or insurance company. For purposes of these laws, in most states "control" is presumed to exist when a person, group of persons or entity acquires the power to vote 10% or more of the voting securities of another entity, subject to certain exceptions. These laws may discourage acquisition proposals and may delay, deter or prevent a change of control of our Company, including through transactions, and in particular through unsolicited transactions, which could have a material adverse effect on our ability to enter into transactions that some or all of our stockholders find favorable.
In addition, certain of our settlements require us to make additional payments upon the occurrence of certain change of control events. These include a $35.0 million payment in the event that we are acquired or otherwise experience a change in control within three years of March 23, 2012, the effective date of the final settlement agreement with the Civil Division of the United States Department of Justice (the "Civil Division"), the Civil Division of the United States Attorney's Office for the Middle District of Florida (the "USAO"), and the Civil Division of the United States Attorney's Office for the District of Connecticut to settle their pending inquiries. Additionally, if, within three years following the May 4, 2011 execution of the settlement agreement with the lead plaintiffs in the consolidated securities class action against us, we are acquired or otherwise experience a change in control at a share price of $30.00 or more, we will be required to pay to the class an additional $25.0 million.
(17) Our stock price and trading volume may be volatile and future sales of our common stock could adversely affect the trading price of our common stock.
From time to time, the price and trading volume of our common stock, as well as the stock of other companies in the health care industry, may experience periods of significant volatility. Company-specific issues and developments generally in the health care industry (including the regulatory environment) and the capital markets and the economy in general may cause this volatility. Our stock price and trading volume may fluctuate in response to a number of events and factors, including:
| |
| • | variations in our operating results; |
| |
| • | changes in the market's expectations about our future operating results; |
| |
| • | changes in financial estimates and recommendations by securities analysts concerning our Company or the health care industry generally; |
| |
| • | operating and stock price performance of other companies that investors may deem comparable; |
| |
| • | news reports relating to trends in our markets; |
| |
| • | changes or proposed changes in the laws and regulations affecting our business; |
| |
| • | acquisitions and financings by us or others in our industry; and |
| |
| • | sales of substantial amounts of our common stock by our directors and executive officers or principal stockholders, or the perception that such sales could occur. |
We may issue equity securities in the future, including securities that are convertible into or exchangeable for, or that represent the right to receive, common stock. We have an effective shelf registration statement on Form S-3 filed with the SEC under which we may offer from time to time an indeterminate amount of any combination of debt securities, common and preferred stock and warrants. The registration statement allows us to seek additional financing, subject to the SEC's rules and regulations relating to eligibility to use Form S-3. Additional equity financing will be dilutive to stockholders, and debt financing, if available, may involve restrictive covenants.
Sales of a substantial number of shares of our common stock or other equity securities, including sales of shares in connection with any future acquisitions, could be substantially dilutive to our stockholders. These sales may have a harmful effect on prevailing market prices for our common stock and our ability to raise additional capital in the financial markets at a time and price favorable to us. Holders of shares of our common stock have no preemptive rights that entitle them to purchase a pro rata share of any offering of shares of any class or series and, therefore, such sales or offerings could result in increased dilution to our stockholders. Our certificate of incorporation provides that we have authority to issue 100,000,000 shares of common stock and 20,000,000 shares of preferred stock.
Risks Related to Information Technology
If we are unable to maintain effective and secure management information systems and applications, successfully update or expand processing capability or develop new capabilities to meet our business needs we could experience operational disruptions and other materially adverse consequences to our business and results of operations.
Our business depends on effective and secure information systems, applications and operations. The information gathered, processed and stored by our management information systems assists us in, among other things, marketing and sales and membership tracking, billing, claims processing, medical management, medical care cost and utilization trending, financial and management accounting, reporting, and planning and analysis. These systems also support our customer service functions, provider and member administrative functions and support tracking and extensive analysis of medical expenses and outcome data. These systems remain subject to unexpected interruptions resulting from occurrences such as hardware failures or increased demand. There can be no assurance that such interruptions will not occur in the future, and any such interruptions could have a material adverse effect on our business and results of operations. Moreover, operating and other issues can lead to data problems that affect the performance of important functions, including, but not limited to, claims payment, customer service and financial reporting.
There can also be no assurance that our process of improving existing systems, developing new systems to support our operations and improving service levels will not be delayed or that system issues will not arise in the future. Our information systems and applications require continual maintenance, upgrading and enhancement to meet our operational needs. If we are unable to maintain or expand our systems, we could suffer from, among other things, operational disruptions, such as the inability to pay claims or to make claims payments on a timely basis, loss of members, difficulty in attracting new members, regulatory problems and increases in administrative expenses.
Additionally, events outside our control, including terrorism or acts of nature such as hurricanes, earthquakes, or fires, could significantly impair our information systems, applications and critical business functions. To help ensure continued operations in the event that our primary operations are rendered inoperable, we have a disaster recovery plan to recover critical business functionality within stated timelines. Our plan may not operate effectively during an actual disaster and our operations and critical business functions could be disrupted, which would have a material adverse effect on our results of operations.
Our costs to comply with laws governing the transmission, security and privacy of health information could be significant, and any disruptions or security breaches in our information technology systems could have a material adverse effect on our results of operations.
Our business requires the secure transmission of confidential information over public networks. Advances in computer capabilities, new discoveries in the field of cryptography or other events or developments could result in compromises or breaches of our security systems and client data stored in our information systems. Anyone who circumvents our security measures could misappropriate our confidential information or cause interruptions in services or operations. The Internet is a public network, and data is sent over this network from many sources. In the past, computer viruses or software programs that disable or impair computers have been distributed and have rapidly spread over the Internet. Computer viruses could be introduced into our systems, or those of our providers or regulators, which could disrupt our operations, or make our systems inaccessible to our providers or regulators. We may be required to expend significant capital and other resources to protect against the threat of security breaches or to alleviate problems caused by breaches.
Failure to keep our computer networks, information technology systems, computers and programs and our members' and customers' sensitive information secure from attack, damage or unauthorized access, whether as a result of our action or inaction or that of one of our business associates or other vendors, could adversely affect our reputation, membership and revenues and also expose us to mandatory disclosure to the media, contract termination, litigation (including class action litigation), and other enforcement proceedings, material fines, penalties and/or remediation costs, and compensatory, special, punitive and statutory damages, consent orders, adverse actions against our licenses to do business and/or injunctive relief, any of which could adversely affect our business, cash flows, operating results or financial condition.
Our measures to prevent security breaches may not be successful. As we expand our business, including through acquisitions and organic growth, increase the amount of information we make available to members and consumers on mobile devices and expand our use of social media, our exposure to these data security and related cybersecurity risks, including the risk of undetected attacks, damage or unauthorized access, increases, and the cost of attempting to protect against these risks also increases.
Under the American Recovery and Reinvestment Act of 2009 ("ARRA"), civil penalties for HIPAA violations by covered entities are increased up to an annual maximum of $1.5 million for uncorrected violations based on willful neglect. In addition, imposition of these penalties is now more likely because ARRA strengthens enforcement. For example, commencing February 2010, HHS was required to conduct periodic audits to confirm compliance. Investigations of violations that indicate willful neglect, for which penalties became mandatory in February 2011, are statutorily required. In addition, state attorneys general are authorized to bring civil actions seeking either injunctions or damages in response to violations of HIPAA privacy and security regulations that threaten the privacy of state residents. Initially monies collected will be transferred to a division of HHS for further enforcement and, within three years, a methodology will be adopted for distributing a percentage of those monies to affected individuals to fund enforcement and provide incentive for individuals to report violations.
In addition, ARRA requires us to notify affected individuals, HHS, and in some cases the media when unsecured personal health information is subject to a security breach.
ARRA also contains a number of provisions that provide incentives for states to initiate certain programs related to health care and health care technology, such as electronic health records. While provisions such as these do not apply to us directly, states wishing to apply for grants under ARRA, or otherwise participating in such programs, may impose new health care technology requirements on us through our contracts with state Medicaid agencies. We are unable to predict what such requirements may entail or what their effect on our business may be.
We will continue to assess our compliance obligations as regulations under ARRA are promulgated and more guidance becomes available from HHS and other federal agencies. The new privacy and security requirements, however, may require substantial operational and systems changes, associate education and resources and there is no guarantee that we will be able to implement them adequately or prior to their effective date. Given HIPAA's complexity and the anticipated new regulations, which may be subject to changing and perhaps conflicting interpretation, our ongoing ability to comply with all of the HIPAA requirements is uncertain, which may expose us to the criminal and increased civil penalties provided under ARRA and may require us to incur significant costs in order to seek to comply with its requirements.
Our business could be adversely impacted by adoption of the new ICD-10 standardized coding set for diagnoses.
HHS has released rules pursuant to HIPAA which mandate the use of standard formats in electronic health care transactions. HHS also has published rules requiring the use of standardized code sets and unique identifiers for providers. By October 2014, the federal government will require that health care organizations, including health insurers, upgrade to updated and expanded standardized code sets used for documenting health conditions. These new standardized code sets, known as ICD-10, will require substantial investments from health care organizations, including us. While use of the ICD-10 code sets will require significant administrative changes, we believe that the cost of compliance with these regulations has not had and is not expected to have a material adverse effect on our cash flows, financial position or results of operations. However, these changes may result in errors and otherwise negatively impact our service levels, and we may experience complications related to supporting customers that are not fully compliant with the revised requirements as of the applicable compliance date. Furthermore, if physicians fail to provide appropriate codes for services provided as a result of the new coding set, we may not be reimbursed, or adequately reimbursed, for such services.
Item 1B. Unresolved Staff Comments.
None.
Item 2. Properties.
Our principal administrative, sales and marketing facilities are located at our leased corporate headquarters in Tampa, Florida. Our corporate headquarters is used in all of our lines of business. We also lease office space for the administration of our health plans in California, Connecticut, Florida, Georgia, Hawaii, Illinois, Kentucky, Louisiana, Missouri, New Jersey, New York, Ohio, South Carolina, Tennessee and Texas. These properties are all in good condition and are well maintained. We believe these facilities are suitable and provide the appropriate level of capacity for our current operations. Upon expiration of the terms of the leases, we believe we could renew these leases on acceptable terms, or find suitable space elsewhere.
Item 3. Legal Proceedings.
United States Department of Health and Human Services
In April 2011, we entered into a Corporate Integrity Agreement (the "Corporate Integrity Agreement") with the Office of Inspector General of Health and Human Services ("OIG-HHS"). The Corporate Integrity Agreement has a term of five years. The Corporate Integrity Agreement requires various ethics and compliance programs designed to help ensure our ongoing compliance with federal health care program requirements. The terms of the Corporate Integrity Agreement include certain organizational structure requirements, internal monitoring requirements, compliance training, screening processes for new employees, reporting requirements to OIG-HHS, and the engagement of an independent review organization to review and prepare written reports regarding, among other things, our reporting practices and bid submissions to federal health care programs.
If we fail to comply with the terms of the Corporate Integrity Agreement we may be required to pay certain monetary penalties. Furthermore, if we commit a material breach of the Corporate Integrity Agreement, OIG-HHS may exclude us from participating in federal health care programs. Any such exclusion would result in the revocation or termination of contracts and/or licenses and potentially have a material adverse effect on our results of operations.
Other Lawsuits and Claims
Separate and apart from the legal matter described above, we are also involved in other legal actions in the normal course of our business, including, without limitation, wage and hour claims, tax disputes, vendor disputes and provider disputes regarding payment of claims. Some of these actions seek monetary damages, including claims for liquidated or punitive damages, which are not covered by insurance. We accrue for contingent liabilities related to these matters if a loss is deemed probable and is estimable. The actual outcome of these matters may differ materially from our current estimates and therefore could have a material adverse effect on our results of operations, financial position, and cash flows.
Item 4. Mine Safety Disclosures.
Not Applicable.
PART II
Item 5. Market for Registrant's Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities.
Market for Common Stock
Our common stock is listed on the New York Stock Exchange under the symbol "WCG." The following table sets forth the high and low sales prices of our common stock, as reported on the New York Stock Exchange, for each of the periods listed.
|
| | | | | | | |
| | High | | Low |
| 2012 | | | |
| First Quarter ended March 31, 2012 | $ | 73.10 |
| | $ | 70.61 |
|
| Second Quarter ended June 30, 2012 | $ | 56.00 |
| | $ | 52.71 |
|
| Third Quarter ended September 30, 2012 | $ | 56.94 |
| | $ | 56.37 |
|
| Fourth Quarter ended December 31, 2012 | $ | 48.90 |
| | $ | 47.54 |
|
| 2011 | |
| | |
|
| First Quarter ended March 31, 2011 | $ | 41.99 |
| | $ | 41.40 |
|
| Second Quarter ended June 30, 2011 | $ | 52.78 |
| | $ | 51.41 |
|
| Third Quarter ended September 30, 2011 | $ | 39.62 |
| | $ | 37.90 |
|
| Fourth Quarter ended December 31, 2011 | $ | 53.27 |
| | $ | 52.38 |
|
The last reported sale price of our common stock on the New York Stock Exchange on February 11, 2013 was $52.88. As of February 11, 2013, we had approximately 27 holders of record of our common stock.
Performance Graph
The following graph compares the cumulative total stockholder return on our common stock for the period from December 31, 2007, to December 31, 2012 with the cumulative total return on the stocks included in the Standard & Poor's 500 Stock Index and the custom composite index over the same period. The Custom Composite Index includes the stock of Aetna, Inc., Centene Corporation, Cigna Corp., Coventry Health Care Inc., Health Net Inc., Humana, Inc., Molina Healthcare, Inc., Unitedhealth Group, Inc., Universal American Corp. and WellPoint, Inc. The graph assumes an investment of $100 made in our common stock and the custom composite index on December 31, 2007. The graph also assumes the reinvestment of dividends and is weighted according to the respective company's stock market capitalization at the beginning of each of the periods indicated. We did not pay any dividends on our common stock during the period reflected in the graph. Further, our common stock price performance shown below should not be viewed as being indicative of future performance.
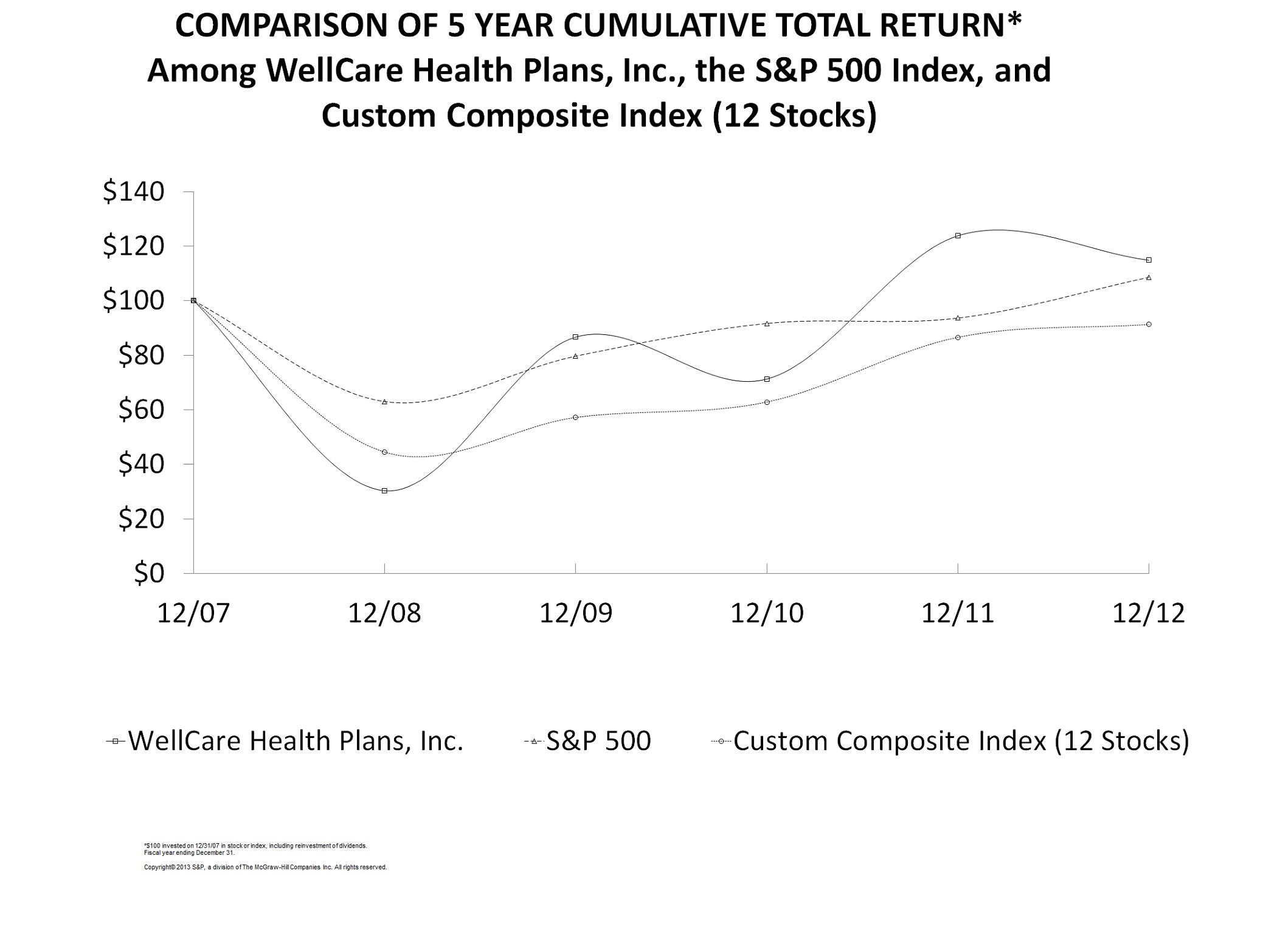
|
| | | | | | | | | | | | | | | | | | | | | | | |
| | 12/31/2007 | | 12/31/2008 | | 12/31/2009 | | 12/31/2010 | | 12/31/2011 | | 12/31/2012 |
| WellCare Health Plans, Inc. | $ | 100 |
| | $ | 30 |
| | $ | 87 |
| | $ | 71 |
| | $ | 124 |
| | $ | 115 |
|
| S&P 500 Index | $ | 100 |
| | $ | 63 |
| | $ | 80 |
| | $ | 92 |
| | $ | 94 |
| | $ | 109 |
|
| Custom Composite Index (12 stocks) | $ | 100 |
| | $ | 45 |
| | $ | 57 |
| | $ | 63 |
| | $ | 87 |
| | $ | 91 |
|
Dividends
We have never paid cash dividends on our common stock. We currently intend to retain any future earnings to fund our business, and we do not anticipate paying any cash dividends in the foreseeable future.
Our ability to pay dividends is partially dependent on, among other things, our receipt of cash dividends from our regulated subsidiaries. The ability of our regulated subsidiaries to pay dividends to us is limited by the state departments of insurance in the states in which we operate or may operate, as well as requirements of the government-sponsored health programs in which we participate. Any future determination to pay dividends will be at the discretion of our board and will depend upon, among other factors, our results of operations, financial condition, capital requirements and contractual restrictions. For more information regarding restrictions on the ability of our regulated subsidiaries to pay dividends to us, please see Item 7 – Management's Discussion and Analysis of Financial Condition and Results of Operations – Regulatory Capital and Restrictions on Dividends.
Unregistered Issuances of Equity Securities
None.
Issuer Purchases of Equity Securities
We do not have a stock repurchase program.
Item 6. Selected Financial Data.
The following table sets forth our summary financial data. This information should be read in conjunction with our consolidated financial statements and the related notes and "Management's Discussion and Analysis of Financial Condition and Results of Operations" included elsewhere in this 2012 Form 10-K. The data for the years ended December 31, 2012, 2011 and 2010, and as of December 31, 2012 and 2011, is derived from consolidated financial statements and related notes included elsewhere in this 2012 Form 10-K. The data for the years ended December 31, 2009 and 2008, and as of December 31, 2010, 2009 and 2008, is derived from audited financial statements not included in this 2012 Form 10-K.
|
| | | | | | | | | | | | | | | | |
| | | For the Years Ended December 31, |
| | | 2012 | 2011 | 2010 | 2009 | 2008 |
| | | (In thousands, except per share data) |
| Revenues: | | | | | | |
| Premium: | | | | | | |
| Medicaid | | $ | 4,389,068 |
| $ | 3,505,448 |
| $ | 3,252,377 |
| $ | 3,165,705 |
| $ | 2,902,120 |
|
| Medicaid premium taxes | | 82,164 |
| 76,163 |
| 56,374 |
| 91,026 |
| 88,929 |
|
| Total Medicaid | | 4,471,232 |
| 3,581,611 |
| 3,308,751 |
| 3,256,731 |
| 2,991,049 |
|
| Medicare Advantage | | 1,936,378 |
| 1,479,750 |
| 1,336,089 |
| 2,775,442 |
| 2,436,226 |
|
| PDP | | 992,607 |
| 1,036,769 |
| 785,350 |
| 835,079 |
| 1,055,795 |
|
| Total premium | | 7,400,217 |
| 6,098,130 |
| 5,430,190 |
| 6,867,252 |
| 6,483,070 |
|
| Investment and other income | | 8,815 |
| 8,738 |
| 10,035 |
| 10,912 |
| 38,837 |
|
| Total revenues | | 7,409,032 |
| 6,106,868 |
| 5,440,225 |
| 6,878,164 |
| 6,521,907 |
|
| Expenses: | | |
| |
| |
| |
| |
|
| Medical benefits (7): | | |
| |
| |
| |
| |
|
| Medicaid | | 3,892,076 |
| 2,890,090 |
| 2,888,467 |
| 2,847,826 |
| 2,569,201 |
|
| Medicare Advantage | | 1,630,565 |
| 1,198,764 |
| 1,067,178 |
| 2,311,591 |
| 2,070,694 |
|
| PDP | | 781,293 |
| 859,113 |
| 638,892 |
| 755,733 |
| 937,693 |
|
| Total medical benefits | | 6,303,934 |
| 4,947,967 |
| 4,594,537 |
| 5,915,150 |
| 5,577,588 |
|
| Selling, general and administrative (1)(7) | | 690,842 |
| 642,107 |
| 837,988 |
| 752,545 |
| 797,557 |
|
| Medicaid premium taxes | | 82,164 |
| 76,163 |
| 56,374 |
| 91,026 |
| 88,929 |
|
| Depreciation and amortization | | 31,531 |
| 26,454 |
| 23,946 |
| 23,336 |
| 21,324 |
|
| Interest (2) | | 4,122 |
| 6,510 |
| 229 |
| 3,087 |
| 11,340 |
|
| Goodwill impairment (3) | | — |
| — |
| — |
| — |
| 78,339 |
|
| Total expenses | | 7,112,593 |
| 5,699,201 |
| 5,513,074 |
| 6,785,144 |
| 6,575,077 |
|
| Income (loss) from operations | | 296,439 |
| 407,667 |
| (72,849 | ) | 93,020 |
| (53,170 | ) |
| Gain on repurchase of subordinated notes (4) | | — |
| 10,807 |
| — |
| — |
| — |
|
| Income (loss) before income taxes | | 296,439 |
| 418,474 |
| (72,849 | ) | 93,020 |
| (53,170 | ) |
| Income tax expense (benefit) | | 111,711 |
| 154,228 |
| (19,449 | ) | 53,149 |
| (16,337 | ) |
| Net income (loss) | | $ | 184,728 |
| $ | 264,246 |
| $ | (53,400 | ) | $ | 39,871 |
| $ | (36,833 | ) |
| Net income (loss) per share: | | |
| |
| |
| |
| |
|
| Basic | | $ | 4.29 |
| $ | 6.17 |
| $ | (1.26 | ) | $ | 0.95 |
| $ | (0.89 | ) |
| Diluted | | $ | 4.22 |
| $ | 6.10 |
| $ | (1.26 | ) | $ | 0.95 |
| $ | (0.89 | ) |
|
| | | | | | | | | | | | | | | | | | | |
| | For the Years Ended December 31, |
| | 2012 | | 2011 | | 2010 | | 2009 | | 2008 |
| Operating Statistics: | | | | | | | | | |
| Medical benefits ratio (7): | | | | | | | | | |
| Medicaid, including premium taxes | 87.0 | % | | 80.7 | % | | 87.3 | % | | 87.4 | % | | 85.9 | % |
| Medicaid (5) | 88.7 | % | | 82.4 | % | | 88.8 | % | | 90.0 | % | | 87.2 | % |
| Medicare Advantage | 84.2 | % | | 81.0 | % | | 79.9 | % | | 83.3 | % | | 82.8 | % |
| PDP | 78.7 | % | | 82.9 | % | | 81.4 | % | | 90.5 | % | | 88.8 | % |
| SG&A expense ratio, including premium taxes | 9.3 | % | | 10.5 | % | | 15.4 | % | | 10.9 | % | | 12.2 | % |
| SG&A expense ratio (6)(7) | 9.4 | % | | 10.6 | % | | 15.6 | % | | 11.1 | % | | 12.4 | % |
| Membership: | | | | | | | | | |
| Consolidated | 2,669,000 |
| | 2,562,000 |
| | 2,224,000 |
| | 2,321,000 |
| | 2,532,000 |
|
| Medicaid | 1,587,000 |
| | 1,451,000 |
| | 1,340,000 |
| | 1,349,000 |
| | 1,300,000 |
|
| Medicare Advantage | 213,000 |
| | 135,000 |
| | 116,000 |
| | 225,000 |
| | 246,000 |
|
| PDP | 869,000 |
| | 976,000 |
| | 768,000 |
| | 747,000 |
| | 986,000 |
|
| | | | | | | | | | |
| | As of December 31, |
| | 2012 | | 2011 | | 2010 | | 2009 | | 2008 |
| | (In thousands) |
| Balance Sheet Data: | |
| | | | | | | | |
| Cash and cash equivalents | $ | 1,100,495 |
| | $ | 1,325,098 |
| | $ | 1,359,548 |
| | $ | 1,158,131 |
| | $ | 1,181,922 |
|
| Total assets | 2,675,516 |
| | 2,488,111 |
| | 2,247,293 |
| | 2,118,447 |
| | 2,203,461 |
|
| Long-term debt (including current maturities) | 135,000 |
| | 146,250 |
| | — |
| | — |
| | 152,741 |
|
| Total liabilities | 1,352,352 |
| | 1,371,265 |
| | 1,415,247 |
| | 1,237,547 |
| | 1,397,632 |
|
| Total stockholders' equity | 1,323,164 |
| | 1,116,846 |
| | 832,046 |
| | 880,900 |
| | 805,829 |
|
| |
| (1) | Selling, general and administrative ("SG&A") expense includes $52.0 million, $47.0 million, $266.0 million, $105.0 million and $103.0 million for the years ended December 31, 2012, 2011, 2010, 2009, and 2008, respectively, of aggregate costs related to the resolution of the previously disclosed governmental and Company investigations, such as settlement accruals and related fair value accretion, legal fees and other similar costs. These amounts are net of $25.8 million, $6.4 million and $0.3 million of D&O insurance recoveries related to the consolidated securities class action during the years ended December 31, 2010, 2009 and 2008, respectively. |
| |
| (2) | Interest expense includes interest related to the $150.0 million term loan which closed on August 1, 2011. |
| |
| (3) | Based on the general economic conditions and outlook during 2008, we performed an analysis of the underlying valuation of Goodwill at December 31, 2008. Upon reviewing the valuation results, we determined that the Goodwill associated with our Medicare reporting unit was fully impaired. The impairment to our Medicare reporting unit was due to, among other things, the anticipated operating environment resulting from regulatory changes and new health care legislation, and the resulting effects on our future membership trends. In 2008, we recorded goodwill impairment expense of $78.3 million. |
| |
| (4) | Gain relates to the December 15, 2011 repurchase of all of the $112,500 tradable unsecured subordinated notes we issued on September 30, 2011 in connection with the stipulation and settlement agreement, which was approved in May 2011, to resolve the putative class-action complaints previously filed against us in 2007. |
| |
| (5) | Medical benefits ratio measures medical benefits expense as a percentage of premium revenue, excluding premium taxes. |
| |
| (6) | SG&A expense ratio measures selling, general and administrative expense as a percentage of total revenue, excluding premium taxes, and does not include depreciation and amortization expense for purposes of determining the ratio. |
| |
| (7) | Medical benefits expense, selling, general and administrative expense and the MBR and SG&A ratios reflect the reclassification of certain quality improvement costs from selling, general and administrative expense to medical benefits expense as discussed within Part II, Item 7 – Management Discussion and Analysis of Financial Condition and Results of Operations – Medical Benefits Expense. |
We have never paid cash dividends on our common stock. We currently intend to retain any future earnings to fund our business, and we do not anticipate paying any cash dividends in the future.
Item 7. Management's Discussion and Analysis of Financial Condition and Results of Operations.
The following discussion and analysis of our financial condition and results of operations should be read in conjunction with Item 6 – Selected Financial Data and our consolidated financial statements and related notes appearing elsewhere in this 2012 Form 10-K. The following discussion contains forward-looking statements that involve risks, uncertainties and assumptions that could cause our actual results to differ materially from management's expectations. Factors that could cause such differences include those set forth under Part I, Item 1 – Business and Part I, Item 1A – Risk Factors, as well as Forward-Looking Statements discussed earlier in this 2012 Form 10-K.
OVERVIEW
Introduction
We are a leading provider of managed care services to government-sponsored health care programs, focusing on Medicaid and Medicare. Headquartered in Tampa, Florida, we offer a variety of health plans for families, children, and the aged, blind and disabled, as well as prescription drug plans. As of December 31, 2012, we served approximately 2.7 million members nationwide. We believe that our broad range of experience and exclusive government focus allows us to effectively serve our members, partner with our providers and government clients, and efficiently manage our ongoing operations.
Summary of Consolidated Financial Results
Summarized below are the key highlights for the year ended December 31, 2012. For additional information, see the remaining sections of this item, which discuss both consolidated and segment results in more detail.
| |
| • | Membership increased 4%, reflecting growth in our Medicaid segment, particularly in Kentucky, which commenced in November 2011 and had a subsequent open enrollment in November 2012, and in Florida, as well as growth in our Medicare MA membership due to service area expansion. |
| |
| • | Premiums increased 21%, mainly reflecting the membership growth in our Medicaid and Medicare Advantage ("MA") markets, as well as rate increases in certain of our Medicaid markets. |
| |
| • | Net Income decreased 30%, primarily due to a decrease in our Medicaid segment results, and higher selling, general and administrative expense ("SG&A") expense - mainly due to our spending on quality and growth initiatives; partially offset by improved results in our MA and PDP segments. 2011 results also benefited from a pre-tax gain of $10.8 million on the repurchase of subordinated notes. The decrease in Medicaid segment results was due mainly to a lower amount of net favorable development of prior period medical benefits payable in 2012 than occurred in 2011, and a relatively higher MBR in the Kentucky Medicaid program due to transition of members into managed care. |
Key Developments and Accomplishments
Our strategic priorities for 2012 included improving health care quality and access for our members, ensuring a competitive cost position and delivering prudent and profitable growth. See Part I, Item 1 – Business for a complete definition of our strategic priorities.
Presented below are key developments and accomplishments relating to progress on our strategic business priorities that occurred or impacted our financial condition and results of operations during 2012 and for 2013, prior to the filing of this 2012 Form 10-K.
| |
| • | In January 2013, we entered into an agreement to acquire Aetna's Medicaid business in Missouri, which as of December 2012, served more than 100,000 MO HealthNet Medicaid program members in 54 counties across the state. |
| |
| • | In January 2013, we acquired UnitedHealthcare Group Incorporated's Medicaid business in South Carolina, which participates in South Carolina's Healthy Connections Choices program across 39 of the state's 46 counties. |
| |
| • | In December 2012, we acquired from Humana, Inc. certain assets of Arcadian Health Plan, Inc.'s Desert Canyon Community Care ("Desert Canyon") MA plans. Approximately 4,000 Desert Canyon plan members in Mohave and Yavapai Counties became members of our Arizona MA health plan on January 1, 2013. |
| |
| • | In November 2012, we acquired Easy Choice Health Plan, Inc. of California ("Easy Choice"). As of January 2013, Easy Choice served approximately 52,000 MA plan members. Easy Choice increased its 2013 service area to 11 California counties, including the San Diego area and five counties in northern California. Easy Choice began offering MA chronic condition special needs plans in five of the 11 counties in its service area in January 2013. |
| |
| • | In October 2012, we added approximately 20,000 new Florida Healthy Kids members as a result of our expansion from serving 18 counties to 65 of Florida's 67 counties. We now offer Florida Healthy Kids services in more counties than any other participating plan. |
| |
| • | As of January 2013, we expanded our service area in the Florida Medicaid program to include all 67 counties across Florida. We also received a premium rate increase of approximately 3.0% to 3.5% retroactive to September 1, 2012. |
| |
| • | In October 2012, we were awarded a contract by the Commonwealth of Kentucky to coordinate physical, behavioral and dental care for a total of approximately 170,000 Medicaid eligible beneficiaries in Medicaid Managed Care Region 3, which consists of 16 counties. We began serving Medicaid beneficiaries in Region 3 effective January 1, 2013. As of January 1, 2013, our membership for this region was estimated to be more than 20,000. |
| |
| • | The Commonwealth of Kentucky recently completed its initiative to ensure that the Medicaid managed care program is structured to deliver quality, cost-effective care to members on a sustainable, long-term basis. As a result, effective January 1, 2013, the Company received an approximate 7.0% premium rate increase for the Kentucky Medicaid program. The Commonwealth also has accelerated to July 1, 2013, our 3.0% rate increase previously scheduled for October 1, 2013. These rate increases apply to all Medicaid geographic regions of the Commonwealth, other than Region 3. |
| |
| • | In October 2012, we were awarded a contract by the Hawaii Department of Human Services to case manage, authorize and facilitate the delivery of behavioral health services to Medicaid-eligible adults who have serious mental illnesses, and who are participants in the state's QUEST Expanded Access (QExA) health program on a statewide basis. We anticipate services beginning in March 2013. |
| |
| • | We continue to expand the geographic footprint of our MA plans and offer D-SNPs for those who are dually-eligible for Medicare and Medicaid in most of the MA markets we serve. This expansion is consistent with our focus on the lower-income demographic of the market and our ability over time to serve both the Medicaid- and Medicare-related coverage of these members. MA membership as of January 1, 2013 was approximately 250,000, an increase from 213,000 as of December 31, 2012. For the 2013 plan year, we now offer plans in a total of 204 counties. |
| |
| • | In October 2012, our MA plans in Florida, Hawaii, Illinois, Connecticut and Ohio each achieved a three Star summary rating while our MA plans in Georgia, Louisiana, Missouri, New York, Texas and New Jersey each received a 2.5 Star summary rating. We are focused on improving quality across all of our lines of business. For example, as a result of our quality improvement measures, we met the performance requirements of our contracts under the New York Medicaid and FHP programs, which were subject to termination if our quality scores did not improve, and we will continue to provide services to members of our New York health plans, and we now have quality health plan status. |
| |
| • | Our 2012 quality accomplishments include the new health plan accreditation of our Hawaii plan. In January 2013, our Florida Medicaid and Medicare health plans were awarded NCQA accreditation. We continue to target accreditation for all of our health plans, and anticipate further progress in 2013. |
| |
| • | With respect to our strategic priority of ensuring a competitive cost structure, 2012 was a year of significant progress. Our administrative expense ratio decreased 120 basis points year-over-year to 9.4% in 2012 compared to 10.6% in 2011. |
Business and Financial Outlook
General Economic, Political Environment and Health Care Reform
A number of states are evaluating new strategies for their Medicaid programs. Given ongoing fiscal challenges, economic conditions, and the success of Medicaid managed care programs over the long run, states continue to recognize the value of collaborating with managed care plans to deliver quality, cost-effective health care solutions. Additionally, we believe that the 2010 Acts will bring about significant changes to the American health care system. For further discussion of the current and political environment that is affecting our business, including health care reform and its potential impact on our business, see Part I, Item 1 – Business, General Economic and Political Environment Impacting our Business. In addition, refer to the risks and uncertainties related to health care reform as discussed in Part I, Item 1A – Risk Factors – Future changes in health care law present challenges for our business that could have a material adverse effect on our results of operations and cash flows.
Medicaid
Our Florida Medicaid contracts expire in August 2015, however we currently anticipate that these will be terminated early, possibly as early as the end of 2013. The Florida agency that operates the state's Medicaid program, AHCA, recently began a competitive procurement process to award contracts for Medicaid managed care across the state. The agency has not yet announced the implementation schedule, but it expects to award contracts under the competitive procurement in 2013. We currently intend to submit a proposal under this process but we cannot assure you our proposal will be successful.
Additionally in Florida, AHCA plans to amend the DRG schedule that it uses to set rates for certain providers whose contracts are tied to Medicaid effective July 1, 2013, which may increase or decrease our payments to these providers.
In addition, our recent amendments to our Medicaid contracts with AHCA required us to comply with federal law related to increased reimbursements to Medicaid providers. We do not currently expect to increase the reimbursement amounts until we receive an adjustment to the premium rates we receive, but if we are required to do so in the future, our medical benefits expense and medical benefits ratio would increase.
In 2012, the Georgia Department of Community Health (the "Georgia DCH") announced further refinements to its Medicaid redesign initiatives. At this time, the Georgia DCH will not conduct a re-procurement of the Georgia Families program, which currently serves Temporary Assistance for Needy Families ("TANF") and Children's Health Insurance Program ("CHIP") members, and will not begin to include aged, blind and disabled ("ABD") beneficiaries as previously planned, given what the Georgia DCH describes as increasing uncertainty at the federal level. Our current Georgia Medicaid contract provides for an additional one-year renewal option exercisable by the Georgia DCH. The Georgia DCH exercised its option to extend the term of our Georgia Medicaid contract until June 30, 2013 and the remaining renewal option potentially extends the contract through June 30, 2014. The Georgia DCH has also indicated its intent to amend our Georgia Medicaid contract to include two additional one-year renewal options, exercisable by the Georgia DCH, that could potentially extend the contract term to June 30, 2016.
The Georgia DCH also plans to move forward with several changes to modernize the Georgia Families program. These may include the promotion of a Primary Care Medical Home initiative, a move to value-based purchasing, and the adoption of a common preferred drug list. Additionally, the state is looking to simplify the administrative process for providers by moving all three care management organizations operating in the state to a common platform for functions such as credentialing, and prior authorization management. We look forward to working with the Georgia DCH to accomplish these initiatives.
Beginning with the fourth quarter 2012, the Commonwealth of Kentucky eliminated its caps on the risk adjustment of premium rates for the Medicaid program. We began serving Medicaid beneficiaries in Region 3 of the Commonwealth of Kentucky on January 1, 2013. As of January 1, 2013, our membership for this region was estimated to be more than 20,000. Region 3 members will have the opportunity to change their health plan through the end of March. In addition, the members assigned to us in January will be served under a 30 day transition of care period.
As a result of our quality improvement measures, we met the performance requirements of our contracts under the New York Medicaid and FHP programs, which were subject to termination if our quality scores did not improve, and we will continue to provide services to members of our New York health plans, and we now have quality health plan status.
With respect to Medicaid rates, we continue to expect the environment to be challenging, given state and federal fiscal conditions. The ultimate premium rate is based on program type, demographic mix and geographic location. We estimate that our rates will decrease approximately 0.3% in Georgia retroactive to July 1, 2012. In Florida, we estimate that our rates will increase approximately 3.0 to 3.5%, retroactive to September 1, 2012. We estimate that our rates will increase by approximately 7.0% in Kentucky retroactive to January 1, 2013. In addition, we expect the approximately 3.0% rate increase we were scheduled to receive on October 1, 2013 will be accelerated to July 1, 2013. These rate increases apply to all regions other than the newly launched Region 3.
Although premiums are generally contractually payable to us before or during the month in which we are obligated to provide services to our members, we have experienced delays in premium payments from certain states. Given the budget shortfalls in many states with which we contract, additional payment delays may occur in the future.
Provider reimbursement levels are subject to change by the states and the Centers for Medicare and Medicaid Services ("CMS"). In addition, some hospital contracts are directly tied to state Medicaid fee schedules, resulting in reimbursement levels that may be adjusted up or down, generally on a prospective basis, based on adjustments made by the state to the fee schedule. We have experienced, and may continue to experience, such adjustments. Unless such adjustments are mitigated by corresponding changes in premiums, our profitability will be negatively impacted.
Medicare Advantage (MA)
As a result of the 2013 annual election period, we have expanded our MA service area to a total of 204 counties. Upon the completion of the acquisitions of Easy Choice and Desert Canyon, we expanded our MA services to California and Arizona and grew our presence in Florida, Georgia, Illinois, New York, and Texas. We also now offer our MA plans to some of the dually eligible members we currently serve through the Kentucky Medicaid program.
Prescription Drug Plans (PDP)
Based on the outcome of our 2013 stand-alone prescription drug plan ("PDP") bids, our plans are below the benchmarks in 14 of the 34 CMS regions and within the de minimis range of the benchmark in five other CMS regions. Comparatively, in 2012, our plans were below the benchmark in five regions and within the de minimis range in 17 other regions. In 2013, we will be auto-assigned newly-eligible members into our plans for the 14 regions that are below the benchmark. We will retain our auto-assigned members in the five regions in which we bid within the de minimis range, however, we will not be auto-assigned new members in those regions during 2013. Members previously auto-assigned to our PDP plans in regions for which our 2013 bids were not within the de minimus range will be reassigned to other plans in 2013. Consequently, membership has declined to approximately 750,000 as of January 2013, a decrease from 869,000 as of December 31, 2012 due to the reassignment to other plans of members who were previously auto-assigned to us, primarily in California, offset in part by additional auto-assignments to us in other regions and an increase in the members who actively chose our PDP plans. We expect membership for the remainder of 2013 to be relatively stable. A decrease in premium rates will further affect our PDP segment's results of operations in 2013.
Dual Eligibles
As of January 2013, three states have executed Memorandums of Agreement with CMS to participate in the Duals Alignment Demonstration Program, a key step in demonstration implementation, and eighteen States are still negotiating with CMS on their demonstration parameters. CMS has issued guidance that no programs will begin before April 1, 2013 and the target enrollment will be limited to 1 to 2 million beneficiaries. Exact implementation times vary by state. CMS has issued guidance indicating that dual-eligible beneficiaries participating in the states' Duals Alignment Demonstration Programs cannot be forced to remain in a duals alignment plan and will be allowed to switch between plans on a monthly basis. However, enrollment in a MA plan is limited to the federally designated annual enrollment period or in the event of a special election period unless the individual seeks to enroll in a plan that has obtained a score of 5 on Medicare's quality performance system ("Star Ratings"). None of our health plans have yet achieved 5 stars. For this reason, dual-eligible beneficiaries subject to a Dual Alignment Demonstration Program will only be able to elect to remain in or join a WellCare plan during the annual enrollment period or special election periods.
The guidance promulgated by CMS requires a cost savings to both Medicare and Medicaid. To the extent that the assumed savings are deemed unrealistic, these programs could limit the number of states in which we choose to provide services. If the rates are deemed sufficient to support the provision of high quality care, we may choose to bid for participation in these programs. In addition, certain states' programs have not permitted us to participate, due to our plan's program design. For those states that have a Duals-Eligible Demonstration Program in which we do not participate, the membership in our MA and PDP plans in those states would be reduced. Per CMS guidance, Part D auto assignments to another PDP will be limited to January 1, 2014, and January 1, 2015, for 2013 and 2014 demonstration states, respectively.
RESULTS OF OPERATIONS
Consolidated Financial Results
The following table sets forth condensed data from our consolidated statements of comprehensive income (loss), as well as other key data used in our results of operations discussion for the year ended December 31, 2012, compared to the years ended December 31, 2011 and 2010. The historical results are not necessarily indicative of results to be expected for any future period. |
| | | | | | | | | | | |
| | For the Years Ended December 31, |
| | 2012 | | 2011 | | 2010 |
| Revenues: | (Dollars in millions, except per share data) |
| Premium | $ | 7,400.2 |
| | $ | 6,098.1 |
| | $ | 5,430.2 |
|
| Investment and other income | 8.8 |
| | 8.7 |
| | 10.0 |
|
| Total revenues | 7,409.0 |
| | 6,106.8 |
| | 5,440.2 |
|
| Expenses: | |
| | |
| | |
|
| Medical benefits | 6,303.9 |
| | 4,948.0 |
| | 4,594.5 |
|
| Selling, general and administrative | 690.8 |
| | 642.1 |
| | 838.0 |
|
| Medicaid premium taxes | 82.2 |
| | 76.2 |
| | 56.4 |
|
| Depreciation and amortization | 31.6 |
| | 26.4 |
| | 23.9 |
|
| Interest | 4.1 |
| | 6.5 |
| | 0.2 |
|
| Total expenses | 7,112.6 |
| | 5,699.2 |
| | 5,513.0 |
|
| Income (loss) from operations | 296.4 |
| | 407.6 |
| | (72.8 | ) |
| Gain on repurchase of subordinated notes | — |
| | 10.8 |
| | — |
|
| Income (loss) before income taxes | 296.4 |
| | 418.4 |
| | (72.8 | ) |
| Income tax (benefit) expense | 111.7 |
| | 154.2 |
| | (19.4 | ) |
| Net income (loss) | $ | 184.7 |
| | $ | 264.2 |
| | $ | (53.4 | ) |
| | | | | | |
| Effective Tax Rate | 37.7 | % | | 36.9 | % | | 26.7 | % |
| | | | | | |
| Membership by Segment | | | | | |
| Medicaid | 1,587,000 |
| | 1,451,000 |
| | 1,340,000 |
|
| MA | 213,000 |
| | 135,000 |
| | 116,000 |
|
| PDP | 869,000 |
| | 976,000 |
| | 768,000 |
|
| Total | 2,669,000 |
| | 2,562,000 |
| | 2,224,000 |
|
Membership
2012 vs. 2011
As of December 31, 2012, we served approximately 2,669,000 members; an increase of approximately 107,000 members from December 31, 2011. We experienced membership growth in both our Medicaid and MA segments when compared to December 31, 2011, which was offset by a decline in PDP membership. Medicaid segment membership increased by 136,000 mainly from membership growth in Florida, membership growth in our Kentucky Medicaid program following its launch in the fourth quarter of 2011 and subsequent open enrollment in November 2012, and membership growth in our Hawaii Medicaid program due to our participation in Hawaii's QUEST program beginning in July 2012. Our Kentucky Medicaid membership increased from 129,000 at December 31, 2011 to 207,000 at December 31, 2012. Members participating in the Kentucky Medicaid program were able to switch plans until January 31, 2012, and membership has also increased due to retroactive member re-assignments. MA segment membership increased by 78,000 compared to December 31, 2011, due to the Easy Choice acquisition, and as a result of the annual election period during 2011, which resulted in an increase of approximately 10,000 members effective January 1, 2012, as well as our continued focus on dually-eligible beneficiaries and expansion into 19 new counties. Excluding the Easy Choice plan, December membership was 174,000, up 29% from December 2011. In our PDP segment, membership decreased by 107,000 compared to December 31, 2011 as a result of our 2012 PDP bids, which resulted in the reassignment to other plans, effective January 1, 2012, of members who were auto-assigned to us in 2011 or prior years.
2011 vs. 2010
As of December 31, 2011, we served approximately 2,562,000 members; an increase of 338,000 members from December 3, 2010. We experienced membership growth in all of our segments. Our Medicaid segment grew with the launch of the Kentucky Medicaid program on November 1, 2011. As of December 31, 2011, we served 129,000 Medicaid members in Kentucky. For our MA segment, we focused on our membership growth activities during the annual election period in the fourth quarter of 2010. Our products have benefit designs that are attractive to both current and prospective members. We invested in strengthening our sales processes and organization and ensuring an effective on-boarding experience for our new members. We added approximately 19,000 MA members from December 31, 2010. In our PDP segment, our plans were below the benchmark in 20 of the 34 CMS regions in 2011, an increase of one region from 2010. Additionally, we were within the de minimis range in eight additional regions. As a result, we added approximately 208,000 PDP members compared to December 31, 2010.
Net income (loss)
2012 vs. 2011
For the year ended December 31, 2012, our net income was $184.7 million compared to $264.2 million for the same period in 2011. Excluding the impact of investigation-related settlements and litigation costs and the 2011 gain on repurchase of subordinated notes, which amounted to a net expense of $30.9 million and $27.2 million, net of tax, for the years ended December 31, 2012 and 2011, respectively, net income decreased by $75.8 million in 2012 compared to 2011. The decrease resulted mainly from a decrease in our Medicaid segment results, higher SG&A expense, partially offset by improved results in our MA and PDP segments. The decrease in our Medicaid segment results were due to the impact of higher net favorable development of prior period medical benefits payable experienced in 2011, the relatively higher MBR in the Kentucky Medicaid program, and a $21.4 million reduction to premium revenue recorded during the third and fourth quarters of 2012 related to a reconciliation of duplicate member records in Georgia dating back to the beginning of the program in 2006. These decreases were partially offset by the impact of higher membership and related premium revenues and the impact of rate increases in certain markets. The improved result in our MA segment was due to increased membership and related premium revenues, while the improvement in the PDP segment resulted mainly from favorable claims experience. The increase in SG&A was driven primarily by higher membership, but the rate of increase was lower than the overall rate of increase in premium revenues.
2011 vs. 2010
For the year ended December 31, 2011, our net income was $264.2 million compared to a net loss of $53.4 million for the same period in 2010. Excluding the impact of investigation-related settlements, litigation costs and gain on repurchase of subordinated notes, all of which amounted to a net expense of $27.2 million and $167.6 million, net of tax, for the years ended December 31, 2011 and 2010, respectively, net income increased by $177.2 million, or 155%, in 2011 compared to 2010. The increase in 2011 resulted mainly from improved results in our Medicaid segment, largely driven by increased premium revenue and the impact of net favorable reserve development of prior period medical benefits payable, rate increases in certain markets, and to a lesser extent, improved results in our PDP segment, mainly driven by an increase in membership. Such increases were partially offset by an increase in SG&A expense and interest incurred on debt.
Premium revenue
2012 vs. 2011
Premium revenue for the year ended December 31, 2012 increased by approximately $1,302.1 million, or 21%, compared to the same period in the prior year. The increase is primarily attributable to membership growth in our Medicaid and MA segments and rate increases in certain of our Medicaid markets, offset by a $21.4 million reduction to premium revenue related to a reconciliation of duplicate member records in the Georgia Medicaid program dating back to the beginning of the program in 2006. Premium revenue includes $82.2 million and $76.2 million of Medicaid premium taxes for the years ended December 31, 2012 and 2011, respectively.
2011 vs. 2010
Premium revenue for the year ended December 31, 2011 increased by approximately $667.9 million, or 12%, compared to the same period in the prior year primarily due to membership growth during 2011 in our PDP and MA segments, rate increases in certain of our Medicaid markets, the launch of our Kentucky Medicaid program in November 2011 and additional premiums recognized in connection with retrospective maternity claims in Georgia. Premium revenue includes $76.2 million and $56.4 million of Medicaid premium taxes for the years ended December 31, 2011 and 2010, respectively.
Investment and other income
2012 vs. 2011
Investment and other income amounted to $8.8 million in 2012, which was consistent with 2011 investment and other income of $8.7 million.
2011 vs. 2010
Investment and other income amounted to $8.7 million in 2011 compared to $10.0 million in 2010. The decrease was due to lower volumes of specialty prescription drugs sold to non-members, partially offset by an increase in investment income resulting from higher average investment balances.
Medical benefits expense
2012 vs. 2011
Total medical benefits expense for the year ended December 31, 2012 increased $1,356.0 million, or 27%, compared to the same period in 2011. The increase is due mainly to increased membership in the Medicaid and MA segments, higher overall utilization in the Medicaid and MA segments in the first half of 2012 and the impact of higher net favorable development of prior period medical benefits payable experienced in 2011 and the relatively higher MBR in the Kentucky Medicaid program, partially offset by a decrease in the PDP segment. For the year ended December 31, 2012, medical benefits expense was impacted by approximately $76.7 million of net favorable development related to prior periods compared to $191.2 million of such development recognized in 2011.
2011 vs. 2010
Total medical benefits expense for the year ended December 31, 2011 increased $353.5 million, or 8%, compared to the same period in 2010. The increase in medical benefits expense is due mainly to the increase in PDP membership, the increase in MBR in the PDP segment that was consistent with our bids, and increased membership and higher MBR in the MA segment. The increases were partially offset by lower expense in the Medicaid segment resulting principally from the impact of net favorable prior period development in medical benefits payable and our medical expense initiatives. For the year ended December 31, 2011, medical benefits expense was impacted by approximately $191.2 million of net favorable development related to prior years. For the year ended December 31, 2010, medical benefits expense was impacted by approximately $56.2 million of net favorable reserve development related to prior years. The increased net favorable development of prior years' medical benefits payable experienced in 2011 compared to 2010 was primarily related to unusually low utilization in our Medicaid segment in 2010 that became clearer over time as claim payments were processed and more complete claims information was obtained.
Effective January 1, 2012, we reclassified to medical benefits expense certain costs related to quality improvement activities that were formerly reported in SG&A expense. The quality improvement costs that we reclassified are consistent with the criteria specified and defined in guidance issued by the Department of Health and Human Services ("HHS") for costs that qualify to be reported as medical benefits under the minimum medical loss ratio provision of the 2010 Acts and include:
| |
| • | Preventive health and wellness and care management; |
| |
| • | Case and disease management; |
| |
| • | Health plan accreditation costs; |
| |
| • | Provider education and incentives for closing care gaps; |
| |
| • | Health risk assessments and member outreach; and |
| |
| • | Information technology costs related to the above activities. |
The reclassification of these quality improvement costs impacted our medical benefits expense and MBR by reportable segment for the years ended December 31, 2011 and 2010 is as follows:
|
| | | | | | | | | | | | | | |
| | For the Year Ended December 31, 2011 |
| | Previously Reported | | Amounts Reclassified | | As Adjusted |
| | (Dollars in millions) |
| Medicaid medical benefits expense | $ | 2,837.6 |
| | | $ | 52.5 |
| | | $ | 2,890.1 |
| |
| Medicaid MBR % | 80.9 | % | | | 1.5 | % | | | 82.4 | % | |
| MA medical benefits expense | 1,180.5 | | | | 18.3 | | | | 1,198.8 | | |
| MA MBR % | 79.8 | % | | | 1.2 | % | | | 81.0 | % | |
| PDP medical benefits expense | 853.9 | | | | 5.2 | | | | 859.1 | | |
| PDP MBR% | 82.4 | % | | | 0.5 | % | | | 82.9 | % | |
| Consolidated medical benefits expense | $ | 4,872.0 |
| | | $ | 76.0 |
| | | $ | 4,948.0 |
| |
| | | | | | | | | |
|
| | | | | | | | | | | | | | |
| | For the Year Ended December 31, 2010 |
| | Previously Reported | | Amounts Reclassified | | As Adjusted |
| | (Dollars in millions) |
| Medicaid medical benefits expense | $ | 2,847.3 |
| | | $ | 41.2 |
| | | $ | 2,888.5 |
| |
| Medicaid MBR % | 87.5 | % | | | 1.3 | % | | | 88.8 | % | |
| MA medical benefits expense | 1,054.1 | | | | 13.1 | | | | 1,067.2 | | |
| MA MBR % | 78.9 | % | | | 1.0 | % | | | 79.9 | % | |
| PDP medical benefits expense | 635.2 | | | | 3.6 | | | | 638.8 | | |
| PDP MBR% | 80.9 | % | | | 0.5 | % | | | 81.4 | % | |
| Consolidated medical benefits expense | $ | 4,536.6 |
| | | $ | 57.9 |
| | | $ | 4,594.5 |
| |
| | | | | | | | | |
Selling, general and administrative expense
SG&A expense includes aggregate costs related to the resolution of the previously disclosed governmental and Company investigations and litigation, such as settlement accruals and related fair value accretion, legal fees and other similar costs; net of $25.8 million of directors and officers liability insurance recoveries during December 31, 2010 related to the putative class action complaints. Please refer to Note 12–Commitments and Contingencies within the Consolidated Financial Statements for additional discussion of investigation-related litigation and other resolution costs. We believe it is appropriate to evaluate SG&A expense exclusive of these investigation-related litigation and other resolution costs because we do not consider them to be indicative of long-term business operations. Additionally, as discussed above, we reclassified costs related to quality improvement activities that were formerly reported in SG&A expenses to medical benefits expense effective January 1, 2012. For the years ended December 31, 2011 and 2010, SG&A expense decreased by $76.0 million and $57.9 million, respectively, due to the reclassification.
A reconciliation of SG&A expense, which reflects the SG&A reclassification previously discussed, is presented below.
|
| | | | | | | | | | | |
| | For the Years Ended December 31, |
| | 2012 | | 2011 | | 2010 |
| | (In millions) |
| SG&A expense | $ | 690.8 |
| | $ | 642.1 |
| | $ | 838.0 |
|
| Adjustments: | |
| | |
| | |
|
| Investigation-related litigation and other resolution costs | (3.8 | ) | | (7.7 | ) | | (258.7 | ) |
| Investigation-related administrative costs, net of D&O insurance policy recovery | (47.7 | ) | | (39.3 | ) | | (7.2 | ) |
| Total investigation-related litigation and other resolution costs | (51.5 | ) | | (47.0 | ) | | (265.9 | ) |
| SG&A expense, excluding investigation-related litigation and other resolution costs | $ | 639.3 |
| | $ | 595.1 |
| | $ | 572.1 |
|
| | | | | | |
| SG&A ratio | 9.4 | % | | 10.6 | % | | 15.6 | % |
| SG&A ratio, excluding investigation-related litigation and other resolution costs | 8.7 | % | | 9.9 | % | | 10.6 | % |
2012 vs. 2011
Excluding investigation-related litigation and other resolution costs, our SG&A expense for the year ended December 31, 2012 increased approximately $44.2 million, or 7%, to $639.3 million. The increase was due to technology investments, including those required by regulatory changes, as well as medical cost initiatives, increased spending related to the launch of our Kentucky Medicaid program, and other growth initiatives. These increases were partially offset by improvements in operating efficiency. Our SG&A expense as a percentage of total revenue, excluding premium taxes ("SG&A ratio"), was 9.4% for the year ended December 31, 2012 compared to 10.6% for the same period in 2011. After excluding the investigation-related litigation and other resolution costs, our SG&A ratio in 2012 was 8.7% compared to 9.9% for the same period in 2011. The improvement in our SG&A ratio, excluding investigation-related litigation and other resolution costs, is related to the growth in premium revenue and improvement in our administrative cost structure driven by business simplification projects, process management in our shared services functions, and continued evaluation of our organizational design. The improvement was partially offset by costs incurred from debt incurred in 2011 to settle investigation-related litigation that was later redeemed in the fourth quarter of 2011, and quality, regulatory and growth initiatives.
Looking ahead to 2013, our growth and other initiatives are driving a need for certain investments. In particular, the integration of our recent acquisitions into our infrastructure will result in incremental expenditures. In addition, we will invest to improve the performance of these businesses and position them for further growth. Finally, as we plan for 2014, we will be making investments to meet the needs of our state and federal customers resulting from implementation of the provisions of the 2010 Acts. As a result of these and other expenditures, we anticipate that our adjusted administrative expense ratio, excluding investigation-related litigation and other resolution costs for 2013 will be consistent with 2012.
2011 vs. 2010
Excluding investigation-related litigation and other resolution costs, our SG&A expense increased approximately $23.0 million, or 4%, in 2011 compared to the same period in 2010. Our SG&A ratio was 10.6% in the 2011 period compared to 15.6% for the same period in the prior year. After excluding the investigation-related litigation and other resolution costs, our SG&A ratio for 2011 was 9.9% compared to 10.6% for the same period in 2010. The improvement in our SG&A ratio, excluding investigation-related litigation and other resolution costs, represents solid progress toward our long-term goal of ensuring our competitive cost position, based on our current business and geographic mix. Business simplification projects, process management in our shared services functions, and continued evaluation of our organizational design continued to drive improvement in our administrative cost structure, partially offset by spending related to the launch of our Kentucky Medicaid program, increased costs associated with our Medicare annual election period strong sales performance, and costs incurred for other growth, regulatory and quality initiatives. An additional factor impacting the comparability of the periods was the impact of relatively low equity-based compensation expense resulting from a larger impact from forfeiture activity in 2010 compared to 2011.
Medicaid premium taxes
2012 vs. 2011
Medicaid premium taxes incurred in the year ended December 31, 2012 were $82.2 million compared to $76.2 million, for the same period in 2011. The increase corresponds to the increase in Medicaid premium revenues.
2011 vs. 2010
Medicaid premium taxes incurred in the years ended December 31, 2011 and 2010 amounted to $76.2 million and $56.4 million, respectively. The increase in Medicaid premium taxes in 2011 was mainly due to the reinstatement of premium taxes by Georgia in July 2010. In October 2009, Georgia stopped assessing taxes on Medicaid premiums remitted to us, which resulted in an equal reduction to premium revenues and Medicaid premium taxes. However, effective July 1, 2010, Georgia began assessing premium taxes again on Medicaid premiums. Therefore, during the first half of 2010, we were not assessed, nor did we remit, any taxes on premiums in Georgia.
Interest expense
2012 vs. 2011
Interest expense for the year ended December 31, 2012 was $4.1 million compared to $6.5 million for the same period in 2011. The decrease in interest expense from 2011 is mainly from debt incurred in 2011 to settle investigation-related litigation that was later redeemed in the fourth quarter of 2011, as discussed below, partially offset by interest on the $150.0 million borrowed under a term loan on August 1, 2011.
2011 vs. 2010
Interest expense for the year ended December 31, 2011 was $6.5 million compared to $0.2 million for the same period in 2010. The increase in interest expense in 2011 is mainly driven by $6.1 million of interest related to the $112.5 million subordinated notes issued in September 2011, and to a lesser extent, interest on the $150.0 million term loan, which closed on August 1, 2011. We issued $112.5 million (aggregate par value) of tradable unsecured subordinated notes on September 30, 2011 in connection with the stipulation and settlement agreement, which was approved in May 2011 to resolve the putative class action complaints previously filed against us in 2007. The subordinated notes had a fixed coupon of 6% and interest was retroactive to May 2011.
Gain on repurchase of subordinated notes
2011 vs. 2010:
On December 15, 2011, we repurchased at 90% of face value all of the $112.5 million of subordinated notes issued in September 2011. The notes had an original a maturity date of December 31, 2016. We recorded a gain on the repurchase of subordinated notes in the amount of $10.8 million. For further information regarding the subordinated notes, refer to Note 11 –Debt within the Consolidated Financial Statements.
Income tax expense (benefit)
2012 vs. 2011
Income tax expense for the year ended December 31, 2012 decreased by $42.5 million compared to the same period in 2011. Our effective income tax rate on pre-tax income was 37.7% for the year ended December 31, 2012 compared to 36.9% for the same period in 2011. The effective tax rate for the year ended December 31, 2012 increased compared to the same period in 2011 due to the settlement of a state tax matter in 2012 which increased the effective rate, partially offset by a decrease in the prevailing state income tax rate which lowered the effective rate.
2011 vs. 2010
Income tax expense for the year ended December 31, 2011 was $154.2 million compared to an income tax benefit of $19.4 million for the same period in 2010. Our effective income tax rate on pre-tax income was 36.9% for the year ended December 31, 2011 compared to 26.7% on a pre-tax loss for the same period in 2010. The comparability of the effective tax rates between 2011 and 2010 was impacted by changes related to estimated non-deductible amounts associated with investigation resolution payments, the favorable resolution of prior years' state tax matters in 2011 and the incurrence of a pre-tax loss in 2010. Additionally, the effective tax rate for the 2010 period was impacted by limitations on the deductibility of certain administrative expenses associated with the resolution of investigation-related matters.
Segment Reporting
Reportable operating segments are defined as components of an enterprise for which discrete financial information is available and evaluated on a regular basis by the Company's decision-makers to determine how resources should be allocated to an individual segment and to assess performance of those segments. Accordingly, we have three reportable segments: Medicaid, MA and PDP.
Segment Performance Measures
We use three measures to assess the performance of our reportable operating segments: premium revenue, medical benefits ratio ("MBR") and gross margin. MBR measures the ratio of medical benefits expense to premiums revenue excluding Medicaid premium taxes. Gross margin is defined as our premium revenue less medical benefits expense. For further information regarding premium revenues and medical benefits expense, please refer below to "Premium Revenue Recognition and Premiums Receivable", and "Medical Benefits Expense and Medical Benefits Payable "under "Critical Accounting Estimates."
Our primary tools for measuring profitability are gross margin and MBR. Changes in gross margin and MBR from period to period depend in large part on our ability to, among other things, effectively price our medical and prescription drug plans, manage medical costs and changes in estimates related to IBNR claims, predict and effectively manage medical benefits expense relative to the primarily fixed premiums we receive, negotiate competitive rates with our health care providers, and attract and retain members. In addition, factors such as changes in health care laws, regulations and practices, changes in Medicaid and Medicare funding, changes in the mix of membership, escalating health care costs, competition, levels of use of health care services, general economic conditions, major epidemics, terrorism or bio-terrorism, new medical technologies and other external factors affect our operations and may have a material impact on our business, financial condition and results of operations.
We use gross margin and MBRs both to monitor our management of medical benefits and medical benefits expense and to make various business decisions, including which health care plans to offer, which geographic areas to enter or exit and which health care providers to select. Although gross margin and MBRs play an important role in our business strategy, we may be willing to enter new geographical markets and/or enter into provider arrangements that might produce a less favorable gross margin and MBR if those arrangements, such as capitation or risk sharing, would likely lower our exposure to variability in medical costs or for other reasons.
Reconciling Segment Results
The following table reconciles our reportable segment results with our income (loss) before income taxes, as reported under GAAP.
|
| | | | | | | | | | | |
| For the Years Ended December 31, |
| | 2012 | | 2011 | | 2010 |
| Gross Margin: | (In millions) |
| Medicaid | $ | 579.2 |
| | $ | 691.5 |
| | $ | 420.3 |
|
| MA | 305.8 |
| | 281.0 |
| | 268.9 |
|
| PDP | 211.3 |
| | 177.7 |
| | 146.5 |
|
| Total gross margin | 1,096.3 |
| | 1,150.2 |
|
| 835.7 |
|
| Investment and other income | 8.8 |
| | 8.7 |
| | 10.0 |
|
| Other expenses | (808.7 | ) | | (751.2 | ) | | (918.5 | ) |
| Income (loss) from operations | $ | 296.4 |
| | $ | 407.6 |
| | $ | (72.8 | ) |
Medicaid
Our Medicaid segment includes plans for beneficiaries of Temporary Assistance for Needy Families ("TANF"), Supplemental Security Income ("SSI"), Aged Blind and Disabled ("ABD") and other state-based programs that are not part of the Medicaid program, such CHIP, Family Health Plus ("FHP") and Managed Long-Term Care ("MLTC") programs. As of December 31, 2012, we operated Medicaid health plans in Florida, Georgia, Hawaii, Illinois, Kentucky, New York and Ohio.
|
| | | | | | | | | | | |
| | For the Years Ended December 31, |
| | 2012 | | 2011 | | 2010 |
| | (In millions) |
| Premium revenue | $ | 4,389.0 |
| | $ | 3,505.4 |
| | $ | 3,252.4 |
|
| Medicaid premium taxes | 82.2 |
| | 76.2 |
| | 56.4 |
|
| Total premiums | 4,471.2 |
| | 3,581.6 |
| | 3,308.8 |
|
| Medical benefits expense | 3,892.0 |
| | 2,890.1 |
| | 2,888.5 |
|
| Gross margin | $ | 579.2 |
| | $ | 691.5 |
| | $ | 420.3 |
|
| | | | | | |
| Medicaid Membership: | |
| | |
| | |
|
| Georgia | 570,000 |
| | 562,000 |
| | 566,000 |
|
| Florida | 454,000 |
| | 404,000 |
| | 415,000 |
|
| Kentucky | 207,000 |
| | 129,000 |
| | — |
|
| Other states | 356,000 |
| | 356,000 |
| | 359,000 |
|
| | 1,587,000 |
| | 1,451,000 |
| | 1,340,000 |
|
| | | | | | |
| Medicaid MBR, including premium taxes | 87.0 | % | | 80.7 | % | | 87.3 | % |
| Medicaid MBR (1) | 88.7 | % | | 82.4 | % | | 88.8 | % |
| |
| (1) | MBR measures the ratio of our medical benefits expense to premiums earned, after excluding Medicaid premium taxes. Because Medicaid premium taxes are included in the premium rates established in certain of our Medicaid contracts and also recognized separately as a component of expense, we exclude these taxes from premium revenue when calculating key ratios as we believe that their impact is not indicative of operating performance. For GAAP reporting purposes, Medicaid premium taxes are included in premium revenue. |
2012 vs. 2011
Excluding Medicaid premium taxes, Medicaid premium revenue for the year ended December 31, 2012 increased 25% when compared to the same period in 2011. The increase was driven mainly by the Kentucky Medicaid program operating for a full year in 2012, compared to two months in 2011, as well as membership growth in that program, both the managed long-term care program and the carve-in of the pharmacy benefit in our New York Medicaid program, membership growth in Florida, and rate increases implemented in most markets in late 2011. The increase in Kentucky Medicaid premiums also reflects the open enrollment in November 2012. Partially offsetting these increases was a $21.4 million reduction of premium revenue recorded during the third and fourth quarters of 2012 related to a reconciliation of duplicate member records in Georgia dating back to the beginning of the program in 2006.
Medicaid medical benefits expense for the year ended December 31, 2012 increased 35% when compared to the same period in 2011. The increase was due mainly to the increase in membership and the relatively higher MBR in the Kentucky Medicaid program and less net favorable development of prior year's medical benefits payable in 2012 than we recognized in 2011, partially offset by the impact of medical cost initiatives that we have implemented. Our Medicaid MBR for the year ended December 31, 2012 increased by 630 basis points when compared to the same period in 2011. The increase was mainly driven by the relatively higher MBR in the Kentucky Medicaid program, the $21.4 million reduction of premium revenue for duplicate member record reconciliation adjustments, and the impact of less net favorable development of prior year's medical benefits payable in 2012 than we recognized in 2011.
The Kentucky Medicaid program MBR for the year ended December 31, 2012 was approximately 105.1% due to the relatively high transitional medical benefit expenses for the program, including the impact of new members from the November 2012 open enrollment which have a higher MBR than previously existing members. We continue to focus on our clinical management capabilities to appropriately address the characteristics of the Kentucky members we serve. In particular, we are executing on emergency room, inpatient, behavioral, and pharmacy cost management activities, all of which are reducing medical costs. We believe the actions we have taken, and are taking, to improve care coordination and manage costs, combined with expected 2013 revenue enhancements and rate increases, will make a meaningful contribution to our 2013 Medicaid gross margin and the long-term stability and soundness of our Kentucky Medicaid program.
2011 vs. 2010
Excluding Medicaid premium taxes, Medicaid premium revenue for the year ended December 31, 2011 increased 8% when compared to the same period in 2010. The increase in premium revenue was mainly due to rate increases in certain markets, the launch of the Kentucky Medicaid program on November 1, 2011 and additional premiums related to certain retrospective maternity claims that were impacted by a change that the Georgia DCH made to its methodology for determining and accepting qualifying maternity claims.
Medicaid medical benefits expense for the year ended December 31, 2011 decreased slightly when compared to the same period in 2010 due mainly to the impact of net favorable reserve development of prior period medical benefits payable and the impact of medical cost initiatives that we have implemented, partially offset by a change in member mix and the launch of the Kentucky Medicaid program in November 2011. The net favorable reserve development resulted primarily from unusually low utilization in 2010. Our Medicaid MBR improved by approximately 640 basis points in 2011 compared to 2010, and the decrease was also driven by the net favorable reserve development of prior period medical benefits payable, the impact of medical cost initiatives, rate increases in certain of our Medicaid markets and additional premiums recognized in connection with retrospective maternity claims in Georgia.
Outlook
We expect Medicaid segment premium revenue to increase in excess of 14% percent, mainly as a result of the Kentucky program expansion and the South Carolina acquisition. We currently anticipate our 2013 premium revenue from the Kentucky Medicaid program will be in excess of $1.0 billion. We currently anticipate that our Medicaid segment MBR will be lower in 2013 as a result of improved performance for the Kentucky program, offset in part by MBR increases in certain other programs and the continuing shift in the mix of our Medicaid segment programs toward higher MBR populations.
Medicare
We contract with CMS under the Medicare program to provide a comprehensive array of Part C and Part D benefits to Medicare eligible persons, provided through our MA plans. Our MA plans are comprised of coordinated care plans ("CCPs"), which are administered through HMOs and generally require members to seek health care services and select a primary care physician from a network of health care providers. In addition, we offer Medicare Part D coverage, which provides prescription drug benefits, as a component of our MA plans. As of December 31, 2012, we operated our MA CCPs in California, Connecticut, Florida, Georgia, Hawaii, Illinois, Louisiana, Missouri, New Jersey, New York, Ohio and Texas.
|
| | | | | | | | | | | |
| | For the Years Ended December 31, |
| | 2012 | | 2011 | | 2010 |
| | (In millions) |
| Premium revenue | $ | 1,936.4 |
| | $ | 1,479.8 |
| | $ | 1,336.1 |
|
| Medical benefits expense | 1,630.6 |
| | 1,198.8 |
| | 1,067.2 |
|
| Gross margin | $ | 305.8 |
| | $ | 281.0 |
| | $ | 268.9 |
|
| | | | | | |
| MA Membership | 213,000 |
| | 135,000 |
| | 116,000 |
|
| | | | | | |
| MA MBR | 84.2 | % | | 81.0 | % | | 79.9 | % |
2012 vs. 2011
MA premium revenue for the year ended December 31, 2012 increased 31% when compared to the same period in 2011 and was mainly attributable to an increase in membership, which increased by approximately 78,000 members between December 31, 2012 and 2011 due to our product design, strengthening of our sales processes and heightened focus on membership growth activities during the annual election period in 2011 and the Easy Choice acquisition. MA segment MBR increased by 320 basis points for the year ended December 31, 2012 compared to the same period in 2011. The changes in the MBR were primarily due to increased quality improvement costs and less net favorable development of prior year's medical benefits payable in 2012 than we recognized in 2011.
2011 vs. 2010
MA premium revenue for the year ended December 31, 2011 increased 11% when compared to the same period in 2010 mainly from an increase in membership. Membership increased by approximately 19,000 members between December 31, 2010 and 2011. The increase in MA premium revenue and membership was attributable to our product design, strengthening of our sales processes and heightened focus on membership growth activities during the annual election periods in 2010 and 2011. MA medical expense increased by 12% in 2011, due to the increase in membership, as well as an increase in the segment MBR. MA segment MBR increased by approximately 110 basis points for the year ended December 31, 2011 compared to the same period in 2010, primarily due to the favorable reserve development we experienced in 2010 from the wind-down of our PFFS plans and increased quality improvement costs. As a result, the segment gross margin increase in 2011 amounted to 4%.
Outlook
For the MA segment, membership as of January 1, 2013 was approximately 250,000, an increase from 213,000 as of December 31, 2012 based on the outcome of the recently completed open enrollment. Excluding Arizona and California, our January 2013 enrollment was approximately 194,000, an increase of 11% from 174,000 as of December 2012. Currently, we expect MA segment membership to continue to grow during the remaining months of 2013, as we leverage our success in serving dually-eligible beneficiaries as well as the broader growth in the Medicare population. Consequently, we expect MA premium revenue to increase by approximately 50% in 2013. Our benefits and cost sharing terms for 2013 have been designed to achieve what we believe is an appropriate financial rate of return with plans that are attractive to both current and prospective members. For the MA segment, we expect the MBR to increase in 2013, driven by the Easy Choice acquisition as well as higher MBRs in many of our other states, consistent with our expectations based on our 2013 bids.
Prescription Drug Plans (PDP)
We have contracted with CMS to serve as a plan sponsor offering stand-alone Medicare Part D PDP plans to Medicare eligible beneficiaries segment through our PDP segment. As of December 31, we offered PDP plans in 49 states and the District of Columbia.
|
| | | | | | | | | | | |
| | For the Years Ended December 31, |
| | 2012 | | 2011 | | 2010 |
| | (In millions) |
| Premium revenue | $ | 992.6 |
| | $ | 1,036.8 |
| | $ | 785.3 |
|
| Medical benefits expense | 781.3 |
| | 859.1 |
| | 638.9 |
|
| Gross margin | $ | 211.3 |
| | $ | 177.7 |
| | $ | 146.4 |
|
| | | | | | |
| PDP Membership | 869,000 |
| | 976,000 |
| | 768,000 |
|
| | | | | | |
| PDP MBR | 78.7 | % | | 82.9 | % | | 81.4 | % |
2012 vs. 2011
PDP premium revenue decreased 4% for the year ended December 31, 2012 when compared to the same period in 2011, primarily due to the decline in membership. Membership decreased by approximately 107,000 members from December 31, 2011 due to the reassignment to other plans, effective January 1, 2012, of members who were auto-assigned to us in 2011 or prior years. PDP MBR for the year ended December 31, 2012 decreased 420 basis points over the same period in 2011 due to the outcome of our 2012 bids and improvements in our pharmacy claims experience, resulting from our focus on member utilization, cost sharing patterns and generic medication utilization.
2011 vs. 2010
PDP premium revenue increased 32% for the year ended December 31, 2011 when compared to the same period in 2010, resulting primarily from increased membership, partially offset by the impact of lower pricing consistent with our bid results. Membership increased by 27% in 2011, largely due to an increase in auto-assigned members resulting from our 2011 bids and the addition of one CMS region. The PDP MBR increased by 150 basis points in 2011 compared to 2010 due to our bid results, member mix and higher utilization. The segment gross margin increased by approximately 21%.
Outlook
PDP membership as of January 1, 2013 was approximately 750,000, a decrease of approximately 14% from 869,000 as of December 31, 2012, based on the outcome of our stand-alone 2013 PDP bids. We expect membership for the remainder of 2013 to be relatively stable as we focus on marketing to those who actively choose our product to offset normal attrition. For the PDP segment, we anticipate the MBR to increase mainly due to the outcome of our 2013 bids and from the addition of our new enhanced product. The decrease in membership and in premium rates is expected to result in a minimum 20% reduction in our PDP segment's premium revenue in 2013 when compared to 2012.
LIQUIDITY AND CAPITAL RESOURCES
Each of our existing and anticipated sources of cash is impacted by operational and financial risks that influence the overall amount of cash generated and the capital available to us. Additionally, we operate as a holding company in a highly regulated industry. The parent and other non-regulated companies ("non-regulated subsidiaries") are dependent upon dividends and management fees from our regulated subsidiaries, most of which are subject to regulatory restrictions. For a further discussion of risks that can affect our liquidity, see Part I – Item 1A – Risk Factors included in this 2012 Form 10-K.
Liquidity
The Company maintains liquidity at two levels: the regulated subsidiary level and the non-regulated subsidiary level.
Regulated subsidiaries
Our regulated subsidiaries' primary liquidity requirements include:
| |
| • | payment of medical claims and other health care services; |
| |
| • | management fees paid to our non-regulated administrator subsidiary under intercompany services agreements and direct administrative costs, which are not covered by the intercompany services agreement, such as selling expenses and legal costs; and |
| |
| • | federal tax payments to the parent company under an intercompany tax sharing agreement. |
Our regulated subsidiaries meet their liquidity needs by:
| |
| • | maintaining appropriate levels of cash, cash equivalents and short-term investments; |
| |
| • | generating cash flows from operating activities, mainly from premium revenue; |
| |
| • | cash flows from investing activities, including investment income and sales of investments; and |
| |
| • | capital contributions received from our non-regulated subsidiaries. |
We refer collectively to the cash, cash equivalents and investment balances maintained by our regulated subsidiaries as "regulated cash and investments," respectively. Our regulated subsidiaries generally receive premiums in advance of payments of claims for medical and other health care services; however, regulated cash and cash equivalents can fluctuate significantly in a particular period depending on the timing of receipts for premiums from our government partners. Our unrestricted regulated cash and investments was $1,224.0 million as of December 31, 2012, a decrease of $74.2 million from December 31, 2011. Included in this change is $192.0 million in dividends and surplus capital paid to, and $119.6 million of contributions received from our non-regulated subsidiaries.
Our regulated subsidiaries are each subject to applicable state regulations that, among other things, require the maintenance of minimum levels of capital and surplus. We continue to maintain significant levels of aggregate excess statutory capital and surplus in our regulated subsidiaries. See further discussion under Regulatory Capital Requirements and Dividend Restrictions below.
Parent and non-regulated subsidiaries
Liquidity requirements at the non-regulated parent level generally consist of:
| |
| • | payment of administrative costs not related to our regulated operations, including, but limited to, business development, branding and certain information technology services; |
| |
| • | capital contributions paid to our regulated subsidiaries; |
Our non-regulated subsidiaries normally meet their liquidity requirements by:
| |
| • | management fees received from our non-regulated administrator subsidiary under intercompany services agreements; |
| |
| • | dividends received from our regulated subsidiaries; |
| |
| • | collecting federal tax payments from the regulated subsidiaries; |
| |
| • | proceeds from issuance of debt and equity securities; and |
| |
| • | cash flows from investing activities, including investment income and sales of investments. |
Our unregulated cash, cash equivalents and investments was $193.5 million as of December 31, 2012, a decrease of $115.0 million from a balance of $308.5 million as of December 31, 2011. The decrease is mainly attributable to $126.6 million in net cash used in relation to our recent acquisitions, payment of certain investigation-related litigation and other resolution costs in connection with our settlement of the Civil Division of the U.S. Department of Justice (the "Civil Division") and $119.6 million in capital contributions made to certain of our regulated subsidiaries that were partially offset by $192.0 million in dividends and surplus capital received from our regulated subsidiaries.
Auction Rate Securities
As of December 31, 2012, $32.0 million of our long-term investments were comprised of municipal note securities with an auction reset feature ("auction rate securities"), which are issued by various state and local municipal entities for the purpose of financing student loans, public projects and other activities and carry investment grade credit ratings. Liquidity for these auction rate securities is typically provided by an auction process which allows holders to sell their notes and resets the applicable interest rate at pre-determined intervals, usually every seven or 35 days. As of the date of this 2012 Form 10-K, auctions have failed for our auction rate securities and there is no assurance that auctions will succeed in the future. An auction failure means that the parties wishing to sell their securities could not be matched with an adequate volume of buyers. In the event that there is a failed auction the indenture governing the security requires the issuer to pay interest at a contractually defined rate that is generally above market rates for other types of similar instruments. The securities for which auctions have failed will continue to accrue interest at the contractual rate and be auctioned every seven or 35 days until the auction succeeds, the issuer calls the securities, or they mature. As a result, our ability to liquidate and fully recover the carrying value of our remaining auction rate securities in the near term may be limited or non-existent. In addition, while all of our auction rate securities currently carry investment grade ratings, if the issuers are unable to successfully close future auctions and their credit ratings deteriorate, we may in the future be required to record an impairment charge on these investments.
Although auctions continue to fail, we believe we will be able to liquidate these securities without significant loss. There are government guarantees or municipal bond insurance in place and we have the ability and the present intent to hold these securities until maturity or market stability is restored. Accordingly, we do not believe our auction rate securities are impaired and as a result, we have not recorded any impairment losses for our auction rate securities. However, it could take until the final maturity of the underlying securities to realize our investments' recorded value. The final maturity of the underlying securities could be as long as 25 years. The weighted-average life of the underlying securities for our auction rate securities portfolio is 20 years.
Cash flow activities
Our cash flows from operations are summarized as follows:
|
| | | | | | | | | | | |
| | For the Years Ended December 31, |
| | 2012 | | 2011 | | 2010 |
| | (In millions) |
| Net cash (used in) provided by operations | $ | (30.7 | ) | | $ | 162.0 |
| | $ | 223.1 |
|
| Net cash used in investing activities | (222.8 | ) | | (111.6 | ) | | (60.5 | ) |
| Net cash provided by (used in) financing activities | 28.9 |
| | (84.9 | ) | | 38.9 |
|
| Total net (decrease) increase in cash and cash equivalents | $ | (224.6 | ) | | $ | (34.5 | ) | | $ | 201.5 |
|
Net cash (used in) provided by operations
For the year ended December 31, 2012, cash from operating activities was negatively impacted by certain delayed Medicaid premiums, primarily associated with our Georgia Medicaid supplemental payments for obstetric deliveries and newborns, and the $39.8 million payment made to the Civil Division of the U.S. Department of Justice ("Civil Division") on March 30, 2012.
Cash provided by operating activities, modified for the impact of the timing of receipts from, and payments to, our government customers, increased in 2011 when compared to 2010 due to improved results from operations, partially offset by $87.5 million of investigation-related litigation and other resolution payments.
Net cash used in investing activities
For the year ended December 31, 2012, cash used in investing activities, excluding acquisitions, primarily reflects our investment in marketable securities and restricted investments of approximately $502.3 million and purchases of property and equipment of $61.3 million, partially offset by $467.3 million of proceeds from maturities of marketable securities and restricted investments. Cash consideration paid for acquisitions, net of cash acquired, was $126.6 million in 2012 related to the Easy Choice and Desert Canyon acquisitions.
In 2011, cash used in investing activities primarily reflects our investment of proceeds provided by our term loan into higher yielding investment alternatives, which had a net impact totaling approximately $108.7 million, and purchases of software and equipment totaling approximately $49.6 million, partially offset by $46.7 million of proceeds from the maturities of restricted investments net of purchases.
Net cash provided by (used in) financing activities
Included in financing activities are funds receivable for the benefit of members, which decreased approximately $36.3 million during the year ended December 31, 2012. These funds represent reinsurance, low-income cost sharing, and coverage gap discount subsidies funded by CMS in connection with the Medicare Part D program, for which we assume no risk.
Included in 2011 financing activities are the repurchase of the subordinated notes in full, which approximated $101.7 million, as well as funds held for the benefit of members, which increased approximately $129.6 million in 2011. These funds represent certain subsidies funded by CMS in connection with the Medicare Part D program for which we assume no risk. This activity is partially offset with the $147.4 million of proceeds from the issuance of the term loan under the Amended Credit Agreement, net of issuance costs.
Financial Impact of Government Investigation and Litigation
Under the terms of settlement agreements entered into on April 26, 2011, and finalized on March 23, 2012, to resolve matters under investigation by the Civil Division and certain other federal and state enforcement agencies (the "Settlement"), WellCare agreed to pay the Civil Division a total of $137.5 million over 36 months plus interest accrued at 3.125%. On March 30, 2012, we made a payment of $39.8 million to the Civil Division, consisting of a $34.4 million principal payment and $5.5 million of accrued interest. The estimated fair value of the discounted remaining liability, to be paid in three annual installments of $34.4 million on March 30 of each year, and related interest, was $105.5 million at December 31, 2012.
The Settlement also provides for a contingent payment of an additional $35.0 million in the event that we are acquired or otherwise experience a change in control within three years of the effective date of the Settlement, provided that the change in control transaction exceeds certain minimum transaction value thresholds as specified in the Settlement.
We currently maintain directors' and officers' liability insurance in the amount of $125.0 million for other matters not addressed above.
Capital Resources
Credit Facility
In August 2011, we entered into a $300.0 million senior secured credit agreement, amended on July 20, 2012 (the "Amended Credit Agreement") that can be used for general corporate purposes. The Amended Credit Agreement provides for a $150.0 million term loan facility as well as a $150.0 million revolving credit facility. In August 2011, we borrowed $150.0 million pursuant to the term loan facility. On February 12, 2013, we borrowed an additional $230.0 million in term loans in connection with the execution of an amended senior secured credit agreement (the "Second Amended Credit Agreement"). The Second Amended Credit Agreement provides for an additional $230.0 million in term loans and a total available credit facility of $515.0 million. As of the date of this 2012 Form 10-K, $365.0 million was outstanding under the Second Amended Credit Agreement. For additional information, see Note 19 – Subsequent Events to the Consolidated Financial Statements.
Each of the term loans and revolving credit facility are set to expire in August 2016. Payments of principal on the term loans are due on a quarterly basis through July 31, 2016. As of December 31, 2012, our remaining term loan balance was $135.0 million, which is included in the current portion of long-term debt and long-term debt line items in our consolidated balance sheet. Our term loan bears interest at 1.75% as of December 31, 2012. For additional information on our long-term debt, see Note 11 – Debt to the Consolidated Financial Statements.
Shelf Registration Statement
In August 2012, we filed a shelf registration statement on Form S-3 with the SEC that became automatically effective covering the registration, issuance and sale of an indeterminate amount of our securities, including common stock, preferred stock, senior or subordinated debt securities, depository shares, securities purchase contracts, units or warrants. We may publicly offer securities in the future at prices and terms to be determined at the time of the offering.
Issuance and Repurchase of Subordinated Notes
On September 30, 2011, we issued tradable unsecured subordinated notes having an aggregate par value of $112.5 million, in connection with the settlement of putative class action complaints filed against us in 2007. On December 15, 2011, we paid $101.7 million to repurchase the subordinated notes at a 10% discount and paid accrued interest of approximately $4.1 million. For further information regarding the subordinated notes, refer to Note 11 – Debt to the Consolidated Financial Statements.
Initiatives to Increase Our Unregulated Cash
We are pursuing alternatives to raise additional unregulated cash. Some of these initiatives include, but are not limited to, consideration of obtaining dividends from certain of our regulated subsidiaries to the extent that we are able to access any available excess capital and/or accessing the debt and equity capital markets. However, we cannot provide any assurances that we will obtain applicable state regulatory approvals for additional dividends to our non-regulated subsidiaries by our regulated subsidiaries or be successful in accessing the capital markets if we determine to do so.
Regulatory Capital and Dividend Restrictions
Each of our HMO and insurance subsidiaries must maintain a minimum amount of statutory capital determined by statute or regulation. The minimum statutory capital requirements differ by state and are generally based on a percentage of annualized premium revenue, a percentage of annualized health care costs, a percentage of certain liabilities, a statutory minimum, risk-based capital ("RBC") requirements or other financial ratios. The RBC requirements are based on guidelines established by the NAIC, and have been adopted by most states. As of December 31, 2012, our operating HMO and insurance company subsidiaries in all states except California, New York and Florida were subject to RBC requirements. The RBC requirements may be modified as each state legislature deems appropriate for that state. The RBC formula, based on asset risk, underwriting risk, credit risk, business risk and other factors, generates the authorized control level ("ACL"), which represents the amount of capital required to support the regulated entity's business. For states in which the RBC requirements have been adopted, the regulated entity typically must maintain a minimum of the greater of 200% of the required ACL or the minimum statutory net worth requirement calculated pursuant to pre-RBC guidelines. Our subsidiaries operating in Texas and Ohio are required to maintain statutory capital at RBC levels equal to 225% and 300%, respectively, of the applicable ACL. Failure to maintain these requirements would trigger regulatory action by the state. At December 31, 2012, our HMO and insurance subsidiaries were in compliance with these minimum capital requirements. The combined statutory capital and surplus of our HMO and insurance subsidiaries was approximately $926.0 million and $858.0 million at December 31, 2012 and 2011, respectively, compared to the required surplus of approximately $383.0 million and $310.0 million at December 31, 2012 and 2011, respectively.
The statutory framework for our regulated subsidiaries' minimum capital requirements changes over time. For instance, RBC requirements may be adopted by more of the states in which we operate. These subsidiaries are also subject to their state regulators' overall oversight powers. For example, the state of New York adopted regulations that increase the reserve requirement annually until 2018. In addition, regulators could require our subsidiaries to maintain minimum levels of statutory net worth in excess of the amount required under the applicable state laws if the regulators determine that maintaining such additional statutory net worth is in the best interest of our members and other constituencies. Moreover, if we expand our plan offerings in a state or pursue new business opportunities, we may be required to make additional statutory capital contributions.
In addition to the foregoing requirements, our regulated subsidiaries are subject to restrictions on their ability to make dividend payments, loans and other transfers of cash. Dividend restrictions vary by state, but the maximum amount of dividends which can be paid without prior approval from the applicable state is subject to restrictions relating to statutory capital, surplus and net income for the previous year. Some states require prior approval of all dividends, regardless of amount. States may disapprove any dividend that, together with other dividends paid by a subsidiary in the prior 12 months, exceeds the regulatory maximum as computed for the subsidiary based on its statutory surplus and net income. For the years ended December 31, 2012, 2011 and 2010, we received $192.0 million, $92.0 million and $45.7 million respectively, in cash dividends from our regulated subsidiaries.
For additional information on regulatory requirements, see Note 16 – Regulatory Capital and Dividend Restrictions to the Consolidated Financial Statements.
Commitments and Contingencies
The following table sets forth information regarding our contractual obligations as of December 31, 2012.
|
| | | | | | | | | | | | | | | | | | | |
| | Payments due to period |
| | Total | | Less Than 1 Year | | 1 - 3 Years | | 3 - 5 Years | | More than 5 Years |
| | (In millions) |
| Operating leases | $ | 70.9 |
| | $ | 19.3 |
| | $ | 37.5 |
| | $ | 9.6 |
| | $ | 4.5 |
|
| Capital leases | 3.3 |
| | 1.6 |
| | 1.7 |
| | — |
| | — |
|
| Purchase obligations (1) | 148.9 |
| | 78.7 |
| | 70.2 |
| | — |
| | — |
|
Amounts accrued related to investigation resolution (2) | 105.5 |
| | 37.3 |
| | 68.2 |
| | — |
| | — |
|
| Long-term debt | 135.0 |
| | 15.0 |
| | 120.0 |
| | — |
| | — |
|
| Total | $ | 463.6 |
| | $ | 151.9 |
| | $ | 297.6 |
| | $ | 9.6 |
| | $ | 4.5 |
|
| |
| (1) | Our purchase obligations include commitments under contracts for equipment leases, software maintenance and the purchase of pharmaceuticals from our pharmacy benefit manager. |
| |
| (2) | Based on the terms of the settlement agreement reached with the Civil Division effective as of March 23, 2012, as discussed in Note 12 – Commitments and Contingencies to the Consolidated Financial Statements. |
We are not an obligor under or guarantor of any indebtedness of any other party; however, we may have to pay referral claims of health care providers under contract with us who are not able to pay costs of medical services provided by other providers.
OFF BALANCE SHEET ARRANGEMENTS
At December 31, 2012, we did not have any off-balance sheet financing arrangements except for operating leases as described in the table above.
CRITICAL ACCOUNTING ESTIMATES
In the ordinary course of business, we make a number of estimates and assumptions relating to the reporting of our results of operations and financial condition in conformity with GAAP. We base our estimates on historical experience and on various other assumptions that we believe to be reasonable under the circumstances. Actual results could differ significantly from those estimates under different assumptions and conditions. We believe that our accounting estimates relating to premium revenue recognition and premiums receivable, medical benefits expense and medical benefits payable, and goodwill and intangible assets, are those that are most important to the portrayal of our financial condition and results and require management's most difficult, subjective and complex judgments, often as a result of the need to make estimates about the effect of matters that are inherently uncertain.
Premium Revenue Recognition and Premiums Receivable
Our Medicare contracts with CMS renew annually. Our contracts with various state Medicaid programs generally are multi-year contracts subject to annual renewal provisions. Our Medicare and Medicaid contracts establish fixed, monthly rates per member ("PMPM"). However, our Medicare contracts also have additional provisions as described in the Medicare section below. The premiums we receive for each member vary according to the specific government program and are generally determined at the beginning of each new contract renewal period or each state's fiscal year; however, premiums may be adjusted by CMS and state agencies throughout the terms of the contracts in certain cases, as described below. Annual rate changes are recorded when they become effective. For a full description of the revenue elements related to our segments, see Part I - Item 1 - Business - OUR PRODUCT SEGMENTS.
We recognize premium revenue in the period in which we are obligated to provide services to our members. We are generally paid by CMS and state agencies in the month in which we provide services. On a monthly basis, we bill members for any premiums for which they are responsible according to their respective plan. Any amounts that have been earned and have not been received are recorded in our consolidated balance sheets as premiums receivable. Any amounts received by us in advance of the period of service are recorded as unearned premiums in the consolidated balance sheets and are not recognized as revenue until the respective services have been provided. We estimate, on an ongoing basis, the amount of member billings that may not be fully collectible based on historical trends. An allowance is established for the estimated amount that may not be collectible. Historically, the allowance for member premiums receivable has not been significant relative to premium revenue. In addition, we routinely monitor the collectability of specific premiums receivable, including Medicaid receivables for obstetric deliveries and newborns (see "Medicaid" below) and net receivables for member retroactivity as described below, and reflect any required adjustments in current operations.
Premium payments are based upon eligibility lists produced by CMS and state agencies. We verify these lists to determine whether we have been paid for the correct premium category and program. From time to time, CMS and state agencies require us to reimburse them for premiums that we received for individuals who were subsequently determined by us, or by CMS or state agencies, to be ineligible for any government-sponsored program or to belong to a plan other than ours. Additionally, the verification of membership may result in additional premiums due to us from CMS and state agencies for individuals who were subsequently determined to belong to our plan for periods in which we received no premium for those members. We estimate the amount of outstanding retroactivity adjustments each period and adjust premium revenue accordingly. As applicable, the estimates of retroactivity adjustments are based on historical trends, premiums billed, the volume of member and contract renewal activity and other information. The amounts receivable or payable identified by us through reconciliation and verification of membership eligibility lists, which relate to current and prior periods, are included in premiums receivable, net and other accrued expenses and liabilities in the accompanying consolidated balance sheets.
Medicaid
In some instances, our Medicaid fixed base PMPM premiums are subject to risk score adjustments based on the health profile of our membership. Generally, the risk score is determined by the state agency's analysis of encounter submissions of processed claims data to determine the acuity of our membership relative to the entire state's Medicaid membership. In some states, supplemental payments are received for certain services such as high cost drugs and early childhood prevention screenings. In contracts with certain states, we are eligible to receive supplemental payments for obstetric deliveries and newborns. Each contract is specific as to how and when these supplemental payments are earned and paid. Upon delivery of a newborn, the state agency is notified according to the contract terms. Revenue is recognized in the period that the delivery occurs and the related services are provided to our member.
We have settled with the Georgia Department of Community Health (the "Georgia DCH") regarding retroactive premium adjustments related to a reconciliation of duplicate member records dating back to the beginning of the program in 2006. As a result, we revised our previous estimate for additional premium revenue receivable related to a previous settlement negotiated with the Georgia DCH in 2011 and we have recorded related reductions of premium revenue totaling approximately $21.4 million during the third and fourth quarters of 2012. The settlement resolved issues with certain premium payments that covered the period from the inception of the program through the settlement, and resulted from a comprehensive review and negotiation involving the three health plans that operate in the program.
Minimum Medical Expense Provisions
Our Florida Medicaid and Healthy Kids contracts and Illinois Medicaid contract require us to expend a minimum percentage of premiums on eligible medical benefits expense. To the extent that we expend less than the minimum percentage of the premiums on eligible medical benefits expense, we are required to refund all or some portion of the difference between the minimum and our actual allowable medical benefits expense. We estimate the amounts due to the state agencies as a return of premium based on the terms of our contracts with the applicable state agency. Such amounts are included in results of operations as reductions of premium.
Medicare Advantage (MA)
The amount of premiums we receive for each MA member is established by contract, although the rates vary according to a combination of factors, including upper payment limits established by CMS, a member's geographic location, age, gender, medical history or condition, or the services rendered to the member. Changes to monthly premiums are also based upon a member's health status as described under "Medicare Risk-Adjusted Premiums" below. We also offer coverage of prescription drug benefits under the Medicare Part D program as a component of most of our MA plans. See further discussion of revenue recognition policies specific to Medicare Part D in "PDP" below.
Medicare Risk-Adjusted Premiums
CMS employs a risk-adjustment model to determine the premium amount it pays for each Medicare member. The risk-adjustment model apportions premiums paid to all plans according to the health status of each beneficiary enrolled and pays more for MA members with predictably higher costs. We collect claims and encounter data from inpatient and ambulatory treatment settings and submit the data to CMS, within prescribed deadlines, which are used to calculate the risk-adjusted premiums we receive. CMS establishes the premium payments to MA plans generally at the beginning of the plan year, and then adjusts premium levels on two separate occasions on a retroactive basis. The first retroactive adjustment for a given plan year generally occurs during the third quarter of that year. This initial settlement represents the update of risk scores for the current plan year based on the severity of claims incurred in the prior plan year. CMS then issues a final retroactive risk-adjusted premium settlement for that plan year in the following year.
We develop our estimates for MA risk-adjusted premiums utilizing historical experience, or other data, and predictive models as sufficient member risk score data becomes available over the course of each CMS plan year. Our estimates are periodically updated as additional diagnosis code information is reported to CMS and are adjusted to actual amounts when the ultimate adjustment settlements are either received from CMS or we receive notification from CMS of such settlement amounts. Historically, we have not experienced significant differences between the amounts that we have recorded and ultimately received; however, it is possible that adjustments to premium revenue could have a material effect on our results of operations, financial position and cash flows in a particular period.
The data provided to CMS to determine members' risk scores is subject to audit by CMS even after the annual settlements occur. An audit may result in the refund of premiums to CMS. While our experience to date has not resulted in a material refund payable to CMS, future refunds could materially reduce premium revenue in the year in which CMS determines a refund is required.
PDP
Substantially all the premium that we receive for Medicare Part D coverage is paid by CMS, and the balance is due from enrolled members. The premium amounts received from CMS are based on the plan year bid submitted to CMS. The monthly payment is a risk-adjusted amount per member and is based upon the member's health status as determined by CMS, as more fully described above under "Medicare Risk Adjusted Premiums". As we do not have access to diagnosis data with respect to our stand-alone PDP members, we cannot anticipate changes in our members' risk scores. Changes in CMS premiums related to risk-score adjustments for our stand-alone PDP membership are recognized when the amounts become determinable and collectability is reasonably assured, which occurs when we are notified by CMS of such adjustments.
Low-income cost sharing, catastrophic reinsurance and coverage gap discount subsidies
Low-income cost sharing, catastrophic reinsurance and coverage gap discount subsidies represent funding from CMS for which we assume no risk. The receipt of these subsidies and the payments of the actual prescription drug costs related to the low-income cost sharing, catastrophic reinsurance and coverage gap discounts are not recognized as premium revenues or benefits expense, but are reported on a net basis as funds receivable/held for the benefit of members in the consolidated balance sheets. These receipts and payments are reported as a financing activity in our consolidated statements of cash flows. Approximately nine months after the close of the annual plan year, except for the coverage gap discount which has a longer settlement timeframe, CMS reconciles actual experience to prospective payments paid to our plans and any differences are settled between CMS and our plans. Historically, we have not experienced material adjustments related to the CMS annual reconciliation of prior plan year low-income cost sharing and catastrophic reinsurance subsidies or coverage gap discount subsidies, due to its recent implementation.
CMS risk corridor
Premiums received from CMS are subject to risk sharing through the Medicare Part D risk corridor provisions. The CMS risk corridor calculation compares our actual experience to the target amount of prescription drug costs, limited to costs under the standard coverage as defined by CMS, less rebates included in our submitted plan year bid. Variances of more than 5% above the target amount result in additional payments by CMS to us. Variances of more than 5% below the target amount require us to refund amounts to CMS. We estimate the risk corridor receivable or payable throughout the year as if the annual contract were to terminate at the end of the reporting period and reflect any adjustments to premium in current operations. This estimate provides no consideration of future pharmacy claims experience, but does require us to consider factors that may not be certain, including membership, risk scores, prescription drug events, and rebates. Approximately nine months after the close of the annual plan year, CMS reconciles actual experience to the target amount and any differences are settled between CMS and our plans. Historically, we have not experienced material adjustments related to the CMS settlement of prior years' risk corridor estimates.
Estimating Medical Benefits Expense and Medical Benefits Payable
The cost of medical benefits is recognized in the period in which services are provided and includes an estimate of the cost of incurred but not reported ("IBNR") medical benefits. Medical benefits payable represents amounts for claims fully adjudicated but not yet paid and estimates for IBNR, and includes direct medical expenses and medically-related administrative costs. Direct medical expenses include amounts paid or payable to hospitals, physicians and providers of ancillary services, such as laboratories and pharmacies. Recorded direct medical expenses are reduced by the amount of pharmacy rebates earned, which are estimated based on historical utilization of specific pharmaceuticals, current utilization and contract terms. Pharmacy rebates earned but not yet received from pharmaceutical manufacturers are included in pharmacy rebates receivable in the accompanying consolidated balance sheets. Direct medical expenses may also include reserves for estimated referral claims related to health care providers under contract with us who are financially troubled or insolvent and who may not be able to honor their obligations for the costs of medical services provided by other providers. In these instances, we may be required to honor these obligations for legal or business reasons. Based on our current assessment of providers under contract with us, such losses have not been and are not expected to be significant. Also, included in direct medical expense are estimates for provider settlements due to clarification of contract terms, out-of-network reimbursement, claims payment differences and amounts due to contracted providers under risk-sharing arrangements. Medically-related administrative costs such as preventive health and wellness, care management, case and disease management, and other quality improvement costs are included in medical benefits expense. Other medically-related administrative costs such as utilization review services, network and provider credentialing and claims handling costs, are recorded in selling, general, and administrative expenses.
The following table provides a detail of the components of medical benefits payable:
|
| | | | | | | | | | | |
| | December 31, 2012 | | % of Total | | December 31, 2011 | | % of Total |
| | (In millions) |
| IBNR | $ | 547.4 |
| | 75% | | $ | 526.7 |
| | 71% |
| Other medical benefits payable | 185.6 |
| | 25% | | 218.1 |
| | 29% |
| Total medical benefits payable | $ | 733.0 |
| | 100% | | $ | 744.8 |
| | 100% |
Medical benefits payable is the most significant estimate included in the consolidated financial statements. We use a consistent methodology to record management's best estimate of medical benefits payable based on the experience and information available to us at the time. This estimate is determined utilizing standard actuarial methodologies based upon historical experience and key assumptions consisting of trend factors and completion factors using an assumption of moderately adverse conditions, which vary by business segment. These standard actuarial methodologies include using, among other factors, contractual requirements, historic utilization trends, the interval between the date services are rendered and the date claims are paid, denied claims activity, disputed claims activity, benefits changes, expected health care cost inflation, seasonality patterns, maturity of lines of business and changes in membership.
The factors and assumptions described above that are used to develop our estimate of medical benefits expense and medical benefits payable inherently are subject to greater variability when there is more limited experience or information available to us. The ultimate claims payment amounts, patterns and trends for new products and geographic areas cannot be precisely predicted at their onset, since we, the providers and the members do not have experience in these products or geographic areas. Standard accepted actuarial methodologies, discussed above, would allow for this inherent variability. This can result in larger differences between the originally estimated medical benefits payable and the actual claims amounts paid.
Conversely, during periods where our products and geographies are more stable and mature, we have more reliable claims payment patterns and trend experience. With more reliable data, we should be able to more closely estimate the ultimate claims payment amounts; therefore, we may experience smaller differences between our original estimate of medical benefits payable and the actual claim amounts paid.
In developing our estimates, we apply different estimation methods depending on the month for which incurred claims are being estimated. For the more recent months, which constitute the majority of the amount of the medical benefits payable, we estimate claims incurred by applying observed trend factors to the fixed fee PMPM costs for prior months, which costs have been estimated using completion factors, in order to estimate the PMPM costs for the most recent months. We validate our estimates of the most recent PMPM costs by comparing the most recent months' utilization levels to the utilization levels in prior months and actuarial techniques that incorporate a historical analysis of claim payments, including trends in cost of care provided and timeliness of submission and processing of claims.
Many aspects of the managed care business are not predictable. These aspects include the incidences of illness or disease (such as congestive heart failure cases, cases of upper respiratory illness, the length and severity of the flu season, diabetes cases, the number of full-term versus premature births and the number of neonatal intensive care babies). Therefore, we must continually monitor our historical experience in determining our trend assumptions to reflect the ever-changing mix, needs and size of our membership. Among the factors considered by management are changes in the level of benefits provided to members, seasonal variations in utilization, identified industry trends and changes in provider reimbursement arrangements, including changes in the percentage of reimbursements made on a capitation as opposed to a fee-for-service basis. These considerations are reflected in the trends in our medical benefits expense. Other external factors such as government-mandated benefits or other regulatory changes, catastrophes and epidemics may impact medical cost trends. Other internal factors such as system conversions and claims processing interruptions may impact our ability to accurately predict estimates of historical completion factors or medical cost trends. Medical cost trends potentially are more volatile than other segments of the economy. Management uses considerable judgment in determining medical benefits expense trends and other actuarial model inputs. We believe that the amount of medical benefits payable as of December 31, 2012 is adequate to cover our ultimate liability for unpaid claims as of that date; however, actual payments may differ from established estimates. If the completion factors we used in estimating our IBNR for the year ended December 31, 2012 were decreased by 1%, our net income would decrease by approximately $73.1 million. If the completion factors were increased by 1%, our net income would increase by approximately $71.5 million.
After determining an estimate of the base reserve, actuarial standards of practice require that a margin for uncertainty be considered in determining the estimate for unpaid claim liabilities. If such a margin is included, the claim liabilities should be adequate under moderately adverse conditions. Therefore, we make an additional estimate in the process of establishing the IBNR, which also uses standard actuarial techniques, to account for moderately adverse conditions that may cause actual claims to be higher than estimated compared to the base reserve. We refer to this additional liability as the provision for moderately adverse conditions. The provision for moderately adverse conditions is a component of our overall determination of the adequacy of our IBNR reserve and is intended to capture the potential adverse development from factors such as our entry into new geographical markets, our provision of services to new populations such as the aged, blind and disabled, the variations in utilization of benefits and increasing medical cost, changes in provider reimbursement arrangements, variations in claims processing speed and patterns, claims payment, the severity of claims, and outbreaks of disease such as the flu. Because of the complexity of our business, the number of states in which we operate, and the need to account for different health care benefit packages among those states, we make an overall assessment of IBNR after considering the base actuarial model reserves and the provision for moderately adverse conditions. We consistently apply our IBNR estimation methodology from period to period. We review our overall estimates of IBNR on a monthly basis. As additional information becomes known to us, we adjust our assumptions accordingly to change our estimate of IBNR. Therefore, if moderately adverse conditions do not occur, evidenced by more complete claims information in the following period, then our prior period estimates will be revised downward, resulting in favorable development. However, when a portion of the development related to the prior year incurred claims is offset by an increase determined to address moderately adverse conditions for the current year incurred claims, we do not consider that development amount as having any impact on net income during the period. If moderately adverse conditions occur and are more than we estimated, then our prior period estimates will be revised upward, resulting in unfavorable development, which would decrease current period net income.
Changes in medical benefits payable estimates are primarily the result of obtaining more complete claims information and medical expense trend data over time. Volatility in members' needs for medical services, provider claims submissions and our payment processes result in identifiable patterns emerging several months after the causes of deviations from assumed trends occur. Since our estimates are based upon PMPM claims experience, changes cannot typically be explained by any single factor, but are the result of a number of interrelated variables, all of which influence the resulting medical cost trend. Differences between actual experience and estimates used to establish the liability, which we refer to as prior period developments, are recorded in the period when such differences become known and have the effect of increasing or decreasing the reported medical benefits expense in such periods.
The following table provides a reconciliation of the beginning and ending balance of medical benefits payable:
|
| | | | | | | | | | | |
| | Years Ended December 31, |
| | 2012 | | 2011 | | 2010 |
| | (In millions) |
| Balances as of beginning of period | $ | 744.8 |
| | $ | 743.0 |
| | $ | 802.5 |
|
| Medical benefits incurred related to: | | | | | |
| Current period | 6,450.5 |
| | 5,200.1 |
| | 4,711.2 |
|
| Prior periods | (146.6 | ) | | (252.1 | ) | | (116.3 | ) |
| Total | 6,303.9 |
| | 4,948.0 |
| | 4,594.9 |
|
| Medical benefits paid related to: | | | | | |
| Current period | (5,754.9 | ) | | (4,533.9 | ) | | (4,084.6 | ) |
| Prior periods | (560.8 | ) | | (412.3 | ) | | (569.8 | ) |
| Total | (6,315.7 | ) | | (4,946.2 | ) | | (4,654.4 | ) |
| Balances as of end of period | $ | 733.0 |
| | $ | 744.8 |
| | $ | 743.0 |
|
Medical benefits payable recorded at December 31, 2011, 2010 and 2009 developed favorably by approximately $146.6 million, $252.1 million and $116.3 million in 2012, 2011 and 2010, respectively. A portion of the prior period development was attributable to the release of the provision for moderately adverse conditions, which is included as part of the assumptions. The release of the provision for moderately adverse conditions was substantially offset by the provision for moderately adverse conditions established for claims incurred in the current year. Accordingly, the change in the amount of the incurred claims related to prior years in the Medical benefits payable does not directly correspond to an increase in net income recognized during the period.
In addition to the release of the provision for moderately adverse conditions, medical benefits expense for the years ended December 31, 2012, 2011 and 2010 was impacted by approximately $76.7 million, $191.2 million and $56.2 million respectively, of net favorable development related to prior years. The net favorable development in 2012 was due to the medical cost trend emerging favorably, mostly in our Medicaid segment and to a lesser extent in our MA and PDP segments, primarily due to lower than projected utilization, partially offset by higher than expected medical services in Kentucky. The net favorable development during 2011 was attributable to the 2010 medical cost trend emerging favorably than we originally estimated, mostly in our Medicaid segment and to a lesser extent in our MA segment, primarily due to lower than projected utilization. The net favorable development in 2010 was primarily associated with the exit of the PFFS product on December 31, 2009. The factors impacting the changes in the determination of medical benefits payable discussed above were not discernible in advance. The impact became clearer over time as claim payments were processed and more complete claims information was obtained.
Goodwill and Other Intangible Assets
We review goodwill and intangible assets for impairment at least annually, or more frequently if events or changes in our business climate occur that may potentially affect the estimated useful life or the recoverability of the remaining balance of goodwill or intangible assets. Events or changes in circumstances would include significant changes in membership, state funding, federal and state government contracts and provider networks. Goodwill is evaluated for impairment by first performing a qualitative assessment to determine whether a quantitative assessment is necessary. If, based on the qualitative assessment, we determine the fair value of the reporting unit is more likely than not less than the carrying value, we perform a two-step quantitative goodwill impairment test. The first step is to determine the fair value of the reporting unit using both the income and market approach. In doing so, we must make assumptions and estimates, such as projected revenues and the discount factor, in estimating fair values. While we believe these assumptions and estimates are appropriate, other assumptions and estimates could be applied and may produce significantly different results. If the fair value of the reporting unit is less than its carrying value, we measure and record the amount of the goodwill impairment, if any, by comparing the implied fair value of the reporting unit's goodwill with the carrying value. We select the second quarter of each year for our annual goodwill impairment test, which generally coincides with the finalization of federal and state contract negotiations and our initial budgeting process, with the test completed during the third quarter of that year. Based on the results of the qualitative assessments performed as of our most recent testing date in 2012, and our review at December 31, 2012, we determined that the fair value of our Medicaid reporting unit is more likely than not greater than the carrying value as of December 31, 2012. Our review included consideration of the termination of our Missouri and Ohio Medicaid contracts as discussed in Part I – Item 1 – Business – "OUR PRODUCT SEGMENTS."
RECENTLY ADOPTED ACCOUNTING STANDARDS
Refer to Note 2 – Summary of Significant Accounting Policies, included in the Consolidated Financial Statements for information and disclosures related to new accounting standards which are incorporated herein by reference.
Item 7A. Qualitative and Quantitative Disclosures about Market Risk.
Investment Return Market Risk
As of December 31, 2012 and 2011, our short-term investment portfolio of $220.3 million and $198.6 million, respectively, consisted of highly liquid securities with maturities between three and 12 months, as well as longer term bonds with floating interest rates that we consider available for sale. We held restricted investments of $67.4 million and $60.7 million, at December 31, 2012 and 2011, respectively, which consist principally of cash, cash equivalents and other short-term investments required by various state statutes or regulations. These restricted assets are classified as long-term regardless of the contractual maturity date due to the nature of the states' requirements. Because of the short-term nature of short-term and restricted investments, we would not expect the value of these investments to decline significantly as a result of a sudden change in market interest rates. At December 31, 2012 and 2011, we held investments classified as long-term in the amount of $96.7 million and $83.0 million, respectively. The investments classified as long term are subject to interest rate risk and will decrease in value if market rates increase. Assuming a hypothetical and immediate 1% increase in market interest rates at December 31, 2012, the fair value of our long-term fixed income investments would decrease by approximately $3.1 million. Similarly, a 1% decrease in market interest rates would result in an increase of the fair value of our investments by less than $3.2 million.
Interest Rate Market Risk
We are exposed to changes in interest rates on our Amended Credit Agreement, as amended, which is subject to variable interest rates dependent upon the Adjusted LIBOR for the interest period in effect for such borrowing plus an applicable margin. Interest rate changes impact the amount of our interest payments and, therefore, our future earnings and cash flows, assuming other factors are held constant. Based on outstanding debt balances and interest rates as of December 31, 2012, a 100 basis point increase in interest rates on our Amended Credit Agreement would increase annual interest expense by approximately $1.4 million. Similarly, a 100 basis point decrease in assumed interest rates would decrease annual interest expense by $1.4 million.
Item 8. Financial Statements and Supplementary Data.
Our consolidated financial statements and related notes required by this item are set forth in the WellCare Health Plans, Inc. financial statements included in Part IV, Item 15 of this filing.
Item 9. Changes In and Disagreements with Accountants on Accounting and Financial Disclosure.
None.
Item 9A. Controls and Procedures.
| |
| (a) | Evaluation of Disclosure Controls and Procedures |
Management, under the leadership of our Chief Executive Officer ("CEO") and our Chief Financial Officer ("CFO"), is responsible for maintaining disclosure controls and procedures (as defined in Rules 13a-15(e) and 15d-15(e) under the Exchange Act) that are designed to ensure that information required to be disclosed in reports filed or submitted under the Exchange Act is recorded, processed, summarized and reported within the time periods specified in the SEC rules and forms and that such information is accumulated and communicated to management, including our CEO and CFO, to allow timely decisions regarding required disclosures.
In connection with the preparation of this 2012 Form 10-K, our management, under the leadership of our CEO and CFO, evaluated the effectiveness of our disclosure controls and procedures ("Disclosure Controls"). Based on that evaluation, our CEO and CFO concluded that, as of December 31, 2012, our Disclosure Controls were effective in timely alerting them to material information required to be included in our reports filed with the SEC.
| |
| (b) | Management's Report on Internal Control Over Financing Reporting |
Our management is responsible for establishing and maintaining adequate internal control over financial reporting (as such term is defined in Rule 13a-15(f) under the Exchange Act). An evaluation was performed under the supervision and with the participation of our management, including our CEO and CFO, of the effectiveness of our internal control over financial reporting based on the framework in Internal Control — Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (the "COSO Framework"). Based on our evaluation under the COSO Framework, our management concluded that our internal control over financial reporting was effective as of December 31, 2012. Our independent registered public accounting firm, Deloitte & Touche, LLP, has issued an attestation report on the effectiveness of our internal control over financial reporting as of December 31, 2012, that is included herein.
| |
| (c) | Changes in Internal Controls |
There has not been any change in our internal control over financial reporting (as defined in Rule 13a-15(f) of the Exchange Act) identified in connection with the evaluation required by Rule 13a-15(d) under the Exchange Act during the quarter ended December 31, 2012 that has materially affected, or is reasonably likely to materially affect, those controls.
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Board of Directors and Stockholders of
WellCare Health Plans, Inc. and Subsidiaries
Tampa, Florida
We have audited the internal control over financial reporting of WellCare Health Plans, Inc. and subsidiaries (the "Company") as of December 31, 2012, based on criteria established in Internal Control — Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission. The Company's management is responsible for maintaining effective internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting, included in the accompanying Management's Report on Internal Control over Financial Reporting. Our responsibility is to express an opinion on the Company's internal control over financial reporting based on our audit.
We conducted our audit in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, testing and evaluating the design and operating effectiveness of internal control based on the assessed risk, and performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
A company's internal control over financial reporting is a process designed by, or under the supervision of, the company's principal executive and principal financial officers, or persons performing similar functions, and effected by the company's board of directors, management, and other personnel to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company's internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company's assets that could have a material effect on the financial statements.
Because of the inherent limitations of internal control over financial reporting, including the possibility of collusion or improper management override of controls, material misstatements due to error or fraud may not be prevented or detected on a timely basis. Also, projections of any evaluation of the effectiveness of the internal control over financial reporting to future periods are subject to the risk that the controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
In our opinion, the Company maintained, in all material respects, effective internal control over financial reporting as of December 31, 2012, based on the criteria established in Internal Control — Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission.
We have also audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the consolidated financial statements and financial statement schedules as of and for the year ended December 31, 2012 of the Company and our report dated February 13, 2013 expressed an unqualified opinion on those financial statements and financial statement schedules.
/s/ Deloitte & Touche, LLP
Certified Public Accountants
Tampa, Florida
February 13, 2013
Item 9B. Other Information.
Second Amendment to the Credit Agreement
On February 12, 2013, we amended the senior secured credit agreement (as amended to date, the "Credit Agreement") to provide for an additional $230,000,000 in term loans, for a total available principal amount of $515,000,000. Concurrent with the executed amendment, we borrowed an additional $230,000,000 in term loans, resulting in a total $365,000,000 outstanding under the Credit Agreement as of February 12, 2103.
The other terms of the Credit Agreement did not change and the amortization schedule is substantially the same.
The foregoing description does not purport to be a complete description of the parties' rights and obligations under the above-described Second Amendment. The above description is qualified in its entirety by reference to the complete Credit Agreement attached as Exhibit 10.33b to this 2012 Form 10-K and incorporated herein by reference.
Amendment to Medicaid Contract with the Commonwealth of Kentucky
On February 8, 2013, we entered into an Amendment to the Medicaid Managed Care Contract dated July 5, 2011 (the "Contract") with The Commonwealth of Kentucky's Cabinet for Finance and Administration, on behalf of the Cabinet for Health and Family Services, Department for Medicaid (the "Commonwealth") regarding the Kentucky Medicaid program (the "Amendment"). Pursuant to the Amendment, we received an approximate 7.0% premium rate increase for the Kentucky Medicaid program, retroactive to January 1, 2013. The Commonwealth also has accelerated to July 1, 2013, our 3.0% rate increase previously scheduled for October 1, 2013. These rate increases apply to all of the Medicaid geographic regions of the Commonwealth other than Region 3. Subject to certain conditions, the Commonwealth also agreed to offer the Company the opportunity for contract renewal at rates no less than those in place at the end of the existing term. The parties also agreed to certain operational changes for improved member services and provider relations. The Amendment also included a release for any claims by us regarding rate sufficiency during the initial contract term.
PART III
Items 10, 11, 12, 13 and 14.
The information required by Items 10, 11, 12, 13 and 14 is omitted because, no later than 120 days after December 31, 2012, we will file and distribute our definitive proxy statement for our annual meeting of stockholders containing the information required by such Items. Such omitted information is incorporated herein by reference.
PART IV
Item 15. Exhibits, Financial Statement Schedules.
(a) Financial Statements and Financial Statement Schedules
| |
| (1) | Financial Statements are listed in the Index to Consolidated Financial Statements on page F-1 of this report. |
| |
| (2) | Financial Statement Schedules are listed in the Index to Consolidated Financial Statements on Page F-1 of this report. |
(b) Exhibits
For a list of exhibits to this 2012 Form 10-K, see the Exhibit Index which is incorporated herein by reference.
We have re-evaluated the materiality criteria for each our operational contracts. In previous years, if we derived from a particular government customer 10% or greater of our total annual consolidated revenues, we determined that all the contracts with that customer were material. As our relationships with our customers and the marketplace has evolved, we believe the more appropriate criteria is to evaluate each of our operational contracts based on whether we derived 10% or greater of our total annual consolidated revenues from that particular contract, in addition to other subjective criteria such as whether two or more contracts were entered at the same time with the same parties with substantively the same terms and similar scope.
(c) Financial Statements
We file as part of this report the financial schedules listed on the index immediately preceding the financial statements at the end of this report.
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the Registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
|
| |
| WellCare Health Plans, Inc. |
| By: | /s/ Alec Cunningham |
| | Alec Cunningham |
| | Chief Executive Officer |
Date: February 13, 2013
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons in the capacities and on the dates indicated:
|
| | | | |
| Signatures | | Title | | Date |
/s/Alec Cunningham | | Chief Executive Officer (Principal Executive Officer and Director) | | February 13, 2013 |
Alec Cunningham | | | | |
| | | | | |
| /s/Thomas L. Tran | | Senior Vice President and Chief Financial Officer (Principal Financial Officer) | | February 13, 2013 |
Thomas L. Tran | | | | |
| | | | | |
| /s/Maurice S. Hebert | | Chief Accounting Officer (Principal Accounting Officer) | | February 13, 2013 |
| Maurice S. Hebert | | | | |
| | | | | |
| /s/Charles G. Berg | | Director | | February 13, 2013 |
| Charles G. Berg | | | | |
| | | | | |
| /s/Carol J. Burt | | Director | | February 13, 2013 |
| Carol J. Burt | | | | |
| | | | | |
| /s/ Roel C. Campos | | Director | | February 13, 2013 |
| Roel C. Campos | | | | |
| | | | | |
| /s/David J. Gallitano | | Director | | February 13, 2013 |
| David J. Gallitano | | | | |
| | | | | |
| /s/D. Robert Graham | | Director | | February 13, 2013 |
| D. Robert Graham | | | | |
| | | | | |
| /s/Kevin F. Hickey | | Director | | February 13, 2013 |
| Kevin F. Hickey | | | | |
| | | | | |
| /s/Christian P. Michalik | | Director | | February 13, 2013 |
| Christian P. Michalik | | | | |
| | | | | |
| /s/Glenn D. Steele, Jr. | | Director | | February 13, 2013 |
| Glenn D. Steele, Jr. | | | | |
| | | | | |
| /s/William L. Trubeck | | Director | | February 13, 2013 |
| William L. Trubeck | | | | |
| | | | | |
| /s/ Paul E. Weaver | | Director | | February 13, 2013 |
| Paul E. Weaver | | | | |
Index to Consolidated Financial Statements and Schedules
WellCare Health Plans, Inc.
|
| |
| Page |
| Report of Independent Registered Public Accounting Firm | |
| Consolidated Statements of Comprehensive Income (Loss) for the years ended December 31, 2012, 2011 and 2010 | |
| Consolidated Balance Sheets as of December 31, 2012 and 2011 | |
| Consolidated Statements of Changes in Stockholders' Equity for the years ended December 31, 2012, 2011 and 2010 | |
| Consolidated Statements of Cash Flows for the years ended December 31, 2012, 2011 and 2010 | |
| Notes to Consolidated Financial Statements | |
Financial Statement Schedules
|
| |
| Schedule I — Condensed Financial Information of Registrant | |
| Schedule II — Valuation and Qualifying Accounts | |
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Board of Directors and Stockholders of
WellCare Health Plans, Inc. and Subsidiaries
Tampa, Florida
We have audited the accompanying consolidated balance sheets of WellCare Health Plans, Inc. and subsidiaries (the "Company") as of December 31, 2012 and 2011, and the related consolidated statements of comprehensive income (loss), changes in stockholders' equity, and cash flows for each of the three years in the period ended December 31, 2012. Our audits also included the financial statement schedules listed in the Index at Item 15. These financial statements and financial statement schedules are the responsibility of the Company's management.
Our responsibility is to express an opinion on the financial statements and financial statement schedules based on our audits. We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit also includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, such consolidated financial statements present fairly, in all material respects, the financial position of WellCare Health Plans, Inc. and subsidiaries as of December 31, 2012 and 2011, and the results of their operations and their cash flows for each of the three years in the period ended December 31, 2012, in conformity with accounting principles generally accepted in the United States of America. Also, in our opinion, such financial statement schedules, when considered in relation to the basic consolidated financial statements taken as a whole, present fairly in all material respects the information set forth therein.
We have also audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the Company's internal control over financial reporting as of December 31, 2012, based on the criteria established in Internal Control-Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission and our report dated February 13, 2013 expressed an unqualified opinion on the Company's internal control over financial reporting.
/s/ Deloitte & Touche, LLP
Certified Public Accountants
Tampa, Florida
February 13, 2013
WELLCARE HEALTH PLANS, INC.
CONSOLIDATED STATEMENTS OF COMPREHENSIVE INCOME (LOSS)
(In thousands, except per share and share data)
|
| | | | | | | | | | | |
| | For the Years Ended December 31, |
| | 2012 | | 2011 | | 2010 |
| Revenues: | | | | | |
| Premium | $ | 7,400,217 |
| | $ | 6,098,130 |
| | $ | 5,430,190 |
|
| Investment and other income | 8,815 |
| | 8,738 |
| | 10,035 |
|
| Total revenues | 7,409,032 |
| | 6,106,868 |
| | 5,440,225 |
|
| Expenses: | | | | | |
| Medical benefits | 6,303,934 |
| | 4,947,967 |
| | 4,594,537 |
|
| Selling, general and administrative | 690,842 |
| | 642,107 |
| | 837,988 |
|
| Medicaid premium taxes | 82,164 |
| | 76,163 |
| | 56,374 |
|
| Depreciation and amortization | 31,531 |
| | 26,454 |
| | 23,946 |
|
| Interest | 4,122 |
| | 6,510 |
| | 229 |
|
| Total expenses | 7,112,593 |
| | 5,699,201 |
| | 5,513,074 |
|
| Income (loss) from operations | 296,439 |
| | 407,667 |
| | (72,849 | ) |
| Gain on repurchase of subordinated notes | — |
| | 10,807 |
| | — |
|
| Income (loss) before income taxes | 296,439 |
| | 418,474 |
| | (72,849 | ) |
| Income tax expense (benefit) | 111,711 |
| | 154,228 |
| | (19,449 | ) |
| Net income (loss) | 184,728 |
| | 264,246 |
| | (53,400 | ) |
| | | | | | |
| Other comprehensive income, before tax: | | | | | |
Change in net unrealized gains and losses on available-for-sale securities | 1,544 |
| | 959 |
| | 1,317 |
|
Income tax expense related to other comprehensive income | 571 |
| | 411 |
| | 507 |
|
| Other comprehensive income, net of tax | 973 |
| | 548 |
| | 810 |
|
| Comprehensive income (loss) | $ | 185,701 |
| | $ | 264,794 |
| | $ | (52,590 | ) |
| | | | | | |
| Net income (loss) per common share (see Note 4): | |
| | |
| | |
|
| Basic | $ | 4.29 |
| | $ | 6.17 |
| | $ | (1.26 | ) |
| Diluted | $ | 4.22 |
| | $ | 6.10 |
| | $ | (1.26 | ) |
| | | | | | |
| Weighted average common shares outstanding: | | | | | |
| Basic | 43,104,216 |
| | 42,817,466 |
| | 42,365,061 |
|
| Diluted | 43,826,285 |
| | 43,328,756 |
| | 42,365,061 |
|
See notes to consolidated financial statements.
WELLCARE HEALTH PLANS, INC.
CONSOLIDATED BALANCE SHEETS
(In thousands, except share data)
|
| | | | | | | |
| | December 31, |
| | 2012 | | 2011 |
| Assets | | | |
| Current Assets: | | | |
| Cash and cash equivalents | $ | 1,100,495 |
| | $ | 1,325,098 |
|
| Investments | 220,344 |
| | 198,569 |
|
| Premiums receivable, net | 387,294 |
| | 217,509 |
|
| Pharmacy rebates receivable, net | 126,832 |
| | 109,933 |
|
| Funds receivable for the benefit of members | 126,646 |
| | 162,745 |
|
| Income taxes receivable | 15,615 |
| | 20,655 |
|
| Prepaid expenses and other current assets, net | 96,276 |
| | 63,053 |
|
| Deferred income tax asset | 27,208 |
| | 22,332 |
|
| Total current assets | 2,100,710 |
| | 2,119,894 |
|
| Property, equipment and capitalized software, net | 131,518 |
| | 98,238 |
|
| Goodwill | 223,839 |
| | 111,131 |
|
| Other intangible assets, net | 53,028 |
| | 9,896 |
|
| Long-term investments | 96,700 |
| | 83,019 |
|
| Restricted investments | 67,364 |
| | 60,663 |
|
| Other assets | 2,357 |
| | 5,270 |
|
| Total Assets | $ | 2,675,516 |
| | $ | 2,488,111 |
|
| | | | |
| Liabilities and Stockholders' Equity | | | |
|
| Current Liabilities: | | | |
| Medical benefits payable | $ | 732,994 |
| | $ | 744,821 |
|
| Unearned premiums | 146 |
| | 164 |
|
| Accounts payable | 18,582 |
| | 3,294 |
|
| Other accrued expenses and liabilities | 221,055 |
| | 215,817 |
|
| Current portion of amount payable related to investigation resolution | 37,305 |
| | 49,557 |
|
| Current portion of long-term debt | 15,000 |
| | 11,250 |
|
| Other payables to government partners | 88,344 |
| | 98,237 |
|
| Total current liabilities | 1,113,426 |
| | 1,123,140 |
|
| Deferred income tax liability | 42,058 |
| | 1,026 |
|
| Amount payable related to investigation resolution | 68,171 |
| | 101,705 |
|
| Long-term debt | 120,000 |
| | 135,000 |
|
| Other liabilities | 8,697 |
| | 10,394 |
|
| Total liabilities | 1,352,352 |
| | 1,371,265 |
|
| | | | |
| Commitments and contingencies (see Note 12) |
| |
|
WELLCARE HEALTH PLANS, INC.
CONSOLIDATED BALANCE SHEETS
(In thousands, except share data) - Continued
|
| | | | | | | |
| | December 31, |
| | 2012 | | 2011 |
| Stockholders' Equity: | | | |
|
| Preferred stock, $0.01 par value (20,000,000 authorized, no shares issued or outstanding) | — |
| | — |
|
| Common stock, $0.01 par value (100,000,000 authorized, 43,212,375 and 42,848,798 shares issued and outstanding at December 31, 2012 and December 31, 2011, respectively) | 432 |
| | 429 |
|
| Paid-in capital | 469,434 |
| | 448,820 |
|
| Retained earnings | 854,086 |
| | 669,358 |
|
| Accumulated other comprehensive loss | (788 | ) | | (1,761 | ) |
| Total stockholders' equity | 1,323,164 |
| | 1,116,846 |
|
| Total Liabilities and Stockholders' Equity | $ | 2,675,516 |
| | $ | 2,488,111 |
|
See notes to consolidated financial statements.
WELLCARE HEALTH PLANS, INC.
CONSOLIDATED STATEMENTS OF CHANGES IN STOCKHOLDERS' EQUITY
(In thousands, except share data)
|
| | | | | | | | | | | | | | | | | | | | | | |
| | Common Stock | | Paid in Capital | | Retained Earnings | | Accumulated
Other
Comprehensive Loss | | Total
Stockholders' Equity |
| | Shares | | Amount | | | | |
| Balance at January 1, 2010 | 42,361,207 |
| | $ | 424 |
| | $ | 425,083 |
| | $ | 458,512 |
| | $ | (3,119 | ) | | $ | 880,900 |
|
| Common stock issued for stock options | 90,853 |
| | 1 |
| | 1,443 |
| | — |
| | — |
| | 1,444 |
|
| Purchase of treasury stock | (36,032 | ) | | (1 | ) | | (6,237 | ) | | — |
| | — |
| | (6,238 | ) |
| Vesting of restricted stock grants and restricted stock units, net of forfeitures | 125,697 |
| | 1 |
| | 11,752 |
| | — |
| | — |
| | 11,753 |
|
| Other equity-based compensation expense | — |
| | — |
| | 3,049 |
| | — |
| | — |
| | 3,049 |
|
| Incremental tax decrement from option exercises | — |
| | — |
| | (6,272 | ) | | — |
| | — |
| | (6,272 | ) |
| Comprehensive loss | — |
| | — |
| | — |
| | (53,400 | ) | | 810 |
| | (52,590 | ) |
| Balance at December 31, 2010 | 42,541,725 |
| | $ | 425 |
| | $ | 428,818 |
| | $ | 405,112 |
| | $ | (2,309 | ) | | $ | 832,046 |
|
| Common stock issued for stock options | 226,036 |
| | 3 |
| | 6,285 |
| | — |
| | — |
| | 6,288 |
|
| Purchase of treasury stock | (69,652 | ) | | (1 | ) | | (3,683 | ) | | — |
| | — |
| | (3,684 | ) |
| Vesting of restricted stock grants and restricted stock units, net of forfeitures | 150,689 |
| | 2 |
| | 16,975 |
| | — |
| | — |
| | 16,977 |
|
| Other equity-based compensation expense | — |
| | — |
| | 2,552 |
| | — |
| | — |
| | 2,552 |
|
| Incremental tax decrement from option exercises | — |
| | — |
| | (2,127 | ) | | — |
| | — |
| | (2,127 | ) |
| Comprehensive income | — |
| | — |
| | — |
| | 264,246 |
| | 548 |
| | 264,794 |
|
| Balance at December 31, 2011 | 42,848,798 |
| | $ | 429 |
| | $ | 448,820 |
| | $ | 669,358 |
| | $ | (1,761 | ) | | $ | 1,116,846 |
|
| Common stock issued for stock options | 243,307 |
| | 2 |
| | 9,405 |
| | — |
| | — |
| | 9,407 |
|
| Purchase of treasury stock | (8,570 | ) | | — |
| | (6,477 | ) | | — |
| | — |
| | (6,477 | ) |
| Vesting of restricted stock grants and restricted stock units, net of forfeitures | 128,840 |
| | 1 |
| | 8,788 |
| | — |
| | — |
| | 8,789 |
|
| Other equity-based compensation expense | — |
| | — |
| | 6,097 |
| | — |
| | — |
| | 6,097 |
|
| Incremental tax benefit from option exercises | — |
| | — |
| | 2,801 |
| | — |
| | — |
| | 2,801 |
|
| Comprehensive income | — |
| | — |
| | — |
| | 184,728 |
| | 973 |
| | 185,701 |
|
| Balance at December 31, 2012 | 43,212,375 |
| | $ | 432 |
| | $ | 469,434 |
| | $ | 854,086 |
| | $ | (788 | ) | | $ | 1,323,164 |
|
See notes to consolidated financial statements.
WELLCARE HEALTH PLANS, INC.
CONSOLIDATED STATEMENTS OF CASH FLOWS
(In thousands)
|
| | | | | | | | | | | |
| | For the Years Ended December 31, |
| | 2012 | | 2011 | | 2010 |
| Cash (used in) provided by operating activities: | | | | | |
| Net income (loss) | $ | 184,728 |
| | $ | 264,246 |
| | $ | (53,400 | ) |
| Adjustments to reconcile net income (loss) to net cash (used in) provided by operating activities: |
|
| | | | |
| Depreciation and amortization | 31,531 |
| | 26,454 |
| | 23,946 |
|
| Equity-based compensation expense | 14,886 |
| | 19,530 |
| | 14,801 |
|
| Incremental tax benefit from equity-based compensation | (3,763 | ) | | (2,778 | ) | | — |
|
| Gain on repurchase of subordinated notes | — |
| | (10,807 | ) | | — |
|
| Deferred taxes, net | 18,791 |
| | 98,170 |
| | (61,204 | ) |
| Provision for doubtful receivables | 16,535 |
| | 11,080 |
| | (6,889 | ) |
| Changes in operating accounts, net of effects from acquisitions: | | | | | |
| Premiums receivable, net | (180,262 | ) | | (96,770 | ) | | 158,124 |
|
| Pharmacy rebates receivable, net | (12,441 | ) | | (24,746 | ) | | (551 | ) |
| Prepaid expenses and other current assets, net | (28,969 | ) | | (37,270 | ) | | (3,083 | ) |
| Medical benefits payable | (38,588 | ) | | 1,831 |
| | (59,525 | ) |
| Unearned premiums | (18 | ) | | (67,219 | ) | | (23,113 | ) |
| Accounts payables and other accrued expenses | 14,922 |
| | 14,018 |
| | 752 |
|
| Other payables to government partners | (12,156 | ) | | 51,632 |
| | 8,458 |
|
| Amount payable related to investigation resolution | (45,786 | ) | | (73,780 | ) | | 256,207 |
|
| Income taxes receivable/payable, net | 7,841 |
| | (12,809 | ) | | (21,134 | ) |
| Other, net | 2,010 |
| | 1,217 |
| | (10,332 | ) |
| Net cash (used in) provided by operating activities | (30,739 | ) | | 161,999 |
| | 223,057 |
|
| | | | | | |
| Cash used in investing activities: | | | | | |
| Acquisitions, net of cash acquired | (126,571 | ) | | — |
| | — |
|
| Purchases of investments | (465,629 | ) | | (386,186 | ) | | (219,961 | ) |
| Proceeds from sale and maturities of investments | 436,839 |
| | 277,486 |
| | 163,993 |
|
| Purchases of restricted investments | (36,660 | ) | | (34,828 | ) | | (21,820 | ) |
| Proceeds from maturities of restricted investments | 30,452 |
| | 81,524 |
| | 44,800 |
|
| Additions to property, equipment and capitalized software, net | (61,268 | ) | | (49,576 | ) | | (27,516 | ) |
| Net cash used in investing activities | (222,837 | ) | | (111,580 | ) | | (60,504 | ) |
| | | | | | |
| Cash provided by (used in) financing activities: | | | | | |
| Proceeds from debt, net of issuance costs | (585 | ) | | 147,473 |
| | — |
|
| Proceeds from option exercises and other | 9,407 |
| | 6,287 |
| | 1,443 |
|
| Incremental tax benefit from equity-based compensation | 3,763 |
| | 2,778 |
| | — |
|
| Purchase of treasury stock | (6,477 | ) | | (3,684 | ) | | (6,237 | ) |
| Payments on debt | (11,250 | ) | | (3,750 | ) | | — |
|
| Repurchase of subordinated notes | — |
| | (101,693 | ) | | — |
|
| Payments on capital leases | (2,219 | ) | | (2,717 | ) | | (1,011 | ) |
| Funds receivable for the benefit of members | 36,334 |
| | (129,563 | ) | | 44,669 |
|
| Net cash provided by (used in) financing activities | 28,973 |
| | (84,869 | ) | | 38,864 |
|
WELLCARE HEALTH PLANS, INC. CONSOLIDATED STATEMENTS OF CASH FLOWS (In thousands) - Continued |
| | | | | | | | | | | |
| | | | | | |
| | For the Years Ended December 31, |
| | 2012 | | 2011 | | 2010 |
| Increase (decrease) in cash and cash equivalents | (224,603 | ) | | (34,450 | ) | | 201,417 |
|
| Balance at beginning of period | 1,325,098 |
| | 1,359,548 |
| | 1,158,131 |
|
| Balance at end of period | $ | 1,100,495 |
| | $ | 1,325,098 |
| | $ | 1,359,548 |
|
| | | | | | |
| SUPPLEMENTAL DISCLOSURES OF CASH FLOW INFORMATION: | |
| | | | |
| Cash paid for taxes | $ | 101,023 |
| | $ | 69,846 |
| | $ | 75,962 |
|
| Cash paid for interest | $ | 3,612 |
| | $ | 5,920 |
| | $ | 228 |
|
| | | | | | |
| SUPPLEMENTAL DISCLOSURES OF NON-CASH TRANSACTIONS: | | | | | |
| Non-cash issuance of subordinated notes | $ | — |
| | $ | 112,500 |
| | $ | — |
|
| Non-cash additions to property, equipment, and capitalized software | $ | 3,278 |
| | $ | 2,449 |
| | $ | 2,354 |
|
| Equipment acquired through capital leases | $ | — |
| | $ | — |
| | $ | 8,868 |
|
See notes to consolidated financial statements.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Years Ended December 31, 2012, 2011, and 2010
(In thousands, except member, per share and share data)
1. ORGANIZATION AND BASIS OF PRESENTATION
WellCare Health Plans, Inc., (the "Company," "we," "us," or "our"), provides managed care services exclusively to government-sponsored health care programs. The Company was formed as a Delaware limited liability company in May 2002 to acquire our Florida, New York and Connecticut health plans. We completed the acquisition of the health plans through two concurrent transactions in July 2002. In July 2004, immediately prior to the closing of our initial public offering, we merged the limited liability company into a Delaware corporation and changed our name to WellCare Health Plans, Inc.
As of December 31, 2012, we served approximately 2,669,000 members. In 2012, we operated Medicaid health plans in Florida, Georgia, Hawaii, Illinois, Kentucky, Missouri, New York and Ohio. We also operated Medicare Advantage ("MA") coordinated care plans ("CCPs") in California, Connecticut, Florida, Georgia, Hawaii, Illinois, Louisiana, Missouri, New Jersey, New York, Ohio and Texas, as well as a stand-alone Medicare prescription drug plan ("PDP") in 49 states and the District of Columbia.
The Kentucky Cabinet for Health and Family Services awarded us a contract to serve the Commonwealth of Kentucky's (Kentucky's) Medicaid program beginning November 1, 2011. We served approximately 207,000 beneficiaries under this program as of December 31, 2012.
Our Medicaid contract in Missouri, which expired on June 30, 2012, was not renewed. Our Medicaid contract in Ohio expired on June 30, 2012. We were not awarded a Medicaid contract in Ohio for the 2013 fiscal year; however, the state contracted with us to provide services to Ohio Medicaid beneficiaries through the transition period. The transition of our Ohio Medicaid members to other plans should be substantially complete in the first quarter of 2013, but it may extend through June 30, 2013. The Ohio Medicaid contract accounted for approximately 97,000, or 4% of our consolidated membership as of December 31, 2012 and approximately $265,300, or 4%, of our consolidated premium revenue, net of premium taxes, for the year ended December 31, 2012. The Missouri Medicaid contract accounted for approximately $20,200, or less than 1%, of our consolidated premium revenue, net of premium taxes, for the year ended December 31, 2012.
In November 2012, we acquired all outstanding interests in America's 1st Choice California Holdings, LLC, the sole shareholder of Easy Choice Health Plan, Inc. of California (collectively, "Easy Choice"). As of December 2012, we served approximately 39,000 Easy Choice MA plan members in California.
Basis of Presentation and Use of Estimates
The consolidated balance sheets and statements of comprehensive income (loss), changes in stockholders' equity, and cash flows include the accounts of the Company and all of its majority-owned subsidiaries. We eliminated all intercompany accounts and transactions.
We prepared the consolidated financial statements in accordance with accounting principles generally accepted in the United States ("GAAP"), which requires us to make estimates and assumptions that affect the amounts reported in the consolidated financial statements and accompanying notes. We base these estimates on our knowledge of current events and anticipated future events and evaluate and update our assumptions and estimates on an ongoing basis; however, actual results may differ from our estimates. We evaluated all material events subsequent to the date of these consolidated financial statements.
We reclassified certain items related to prior years in these consolidated financial statements to conform to our current year presentation. These reclassifications had no effect on stockholders' equity, net income, or comprehensive income (loss) as previously reported. We reclassified certain costs related to quality improvement activities as medical benefits expense. Prior to January 1, 2012, we reported these costs as selling, general and administrative expenses. The quality improvement costs that we reclassified are consistent with the criteria specified and defined in guidance issued by the Department of Health and Human Services ("HHS") for costs that qualify to be reported as medical benefits under the minimum medical loss ratio provision of The Patient Protection and Affordable Care Act and The Health Care and Education Reconciliation Act of 2010 (collectively, the "2010 Acts") and include:
• preventive health and wellness and care management;
• case and disease management;
• health plan accreditation costs;
• provider education and incentives for closing care gaps;
• health risk assessments and member outreach; and
• information technology costs related to the above activities.
The reclassification of these quality improvement costs impacted previously-reported medical benefits expense, by reportable segment, and selling, general and administrative expenses for the years ended December 31, 2011 and 2010 as follows:
|
| | | | | | | | | | | | | | | | | | | | | | | |
| | For the Year Ended
December 31, 2011 | | For the Year Ended
December 31, 2010 |
| | Previously Reported | | Amounts Reclassified | | As Adjusted | | Previously Reported | | Amounts Reclassified | | As Adjusted |
| Medical benefits expense: | | | | | | | | | | | |
| Medicaid | $ | 2,837,639 |
| | $ | 52,451 |
| | $ | 2,890,090 |
| | $ | 2,847,315 |
| | $ | 41,152 |
| | $ | 2,888,467 |
|
| MA | 1,180,500 |
| | 18,264 |
| | 1,198,764 |
| | 1,054,071 |
| | 13,107 |
| | 1,067,178 |
|
| PDP | 853,932 |
| | 5,181 |
| | 859,113 |
| | 635,245 |
| | 3,647 |
| | 638,892 |
|
| Total medical benefits expense | $ | 4,872,071 |
| | $ | 75,896 |
| | $ | 4,947,967 |
| | $ | 4,536,631 |
| | $ | 57,906 |
| | $ | 4,594,537 |
|
Selling, general and administrative expenses | $ | 718,003 |
| | $ | (75,896 | ) | | $ | 642,107 |
| | $ | 895,894 |
| | $ | (57,906 | ) | | $ | 837,988 |
|
2. SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES
Revenue Recognition
We earn premium revenue through our participation in Medicaid, Medicaid-related and Medicare programs.
State governments individually operate and implement and, together with the federal government's Centers for Medicare and Medicaid Services ("CMS"), fund and regulate the Medicaid program. We provide benefits to low-income and disabled persons under the Medicaid program and are paid premiums based on contracts with government agencies in the states in which we operate health plans. Our Medicaid contracts are generally multi-year contracts subject to annual renewal provisions. We record annual rate changes when they become effective. Such adjustments are typically made at the commencement of each new contract renewal period. In some instances, our fixed Medicaid premiums are subject to risk score adjustments based on the acuity of our membership. State agencies analyze encounter submissions of processed claims data to determine the acuity of our membership relative to the entire state's Medicaid membership.
We operate our MA plans under the Medicare Part C program and provide benefits comparable to Medicare Part A and B to eligible members. Most of our MA plans and our PDP plan offer prescription drug benefits to eligible members under the Medicare Part D program. Premiums for each MA member are established by contract, although the rates vary according to a combination of factors, including upper payment limits established by CMS, the members' geographic location, age, gender, medical history or condition, or the services rendered to the member. Our MA contracts with CMS generally have terms of one year and expire at the end of each calendar year. PDP premiums are also based upon a contract with CMS that has a term of one year and expires at the end of each calendar year. We provide annual written bids to CMS for our PDPs, which reflect the estimated costs of providing prescription drug benefits over the plan year. Changes in MA and PDP members' health status also impact monthly premiums as described under "Risk-Adjusted Medicare Premiums" below. CMS pays all premium for Medicare Part C and substantially all of the premium for Medicare Part D coverage. We bill the remaining Medicare Part D premium to PDP and MA members with Part D benefits based on the plan year bid submitted to CMS. For qualifying low-income subsidy ("LIS") members, CMS pays for some or all of the LIS members' monthly premium. The CMS payment is dependent upon the member's income level as determined by the Social Security Administration.
We receive premiums from CMS and state agencies on a per member per month ("PMPM") basis for the members that are assigned to, or have selected, us to provide health care services under our Medicare and Medicaid contracts. We recognize premium revenue in the period in which we are obligated to provide services to our members. CMS and state agencies generally pay us in the month in which we provide services. We record premiums earned but not received as premiums receivable and record premiums received in advance of the period of service as unearned premiums in the consolidated balance sheets. Unearned premiums are recognized as revenue when we provide the related services. On a monthly basis, we bill members for any premiums for which they are responsible according to their respective plan. Member premiums are recognized as revenue in the period of service. We reduce recorded premium revenue and member premiums receivable by the amount we estimate may not be collectible, based on our evaluation of historical trends.We also routinely monitor the collectability of specific premiums receivable from CMS and state agencies, including Medicaid receivables for obstetric deliveries and newborns and net receivables for member retroactivity and reduce revenue and premiums receivable by the amount we estimate may not be collectible. We reported premiums receivable net of an allowance for uncollectible premiums receivable of $14,843 and $10,367 at December 31, 2012 and 2011, respectively. Historically, the allowance for member premiums receivable has not been material relative to consolidated premium revenue.
We record retroactive adjustments to revenues based on changes in the number and eligibility status of our members subsequent to when we recorded revenue related to those members and months of service. We receive premium payments based upon eligibility lists produced by CMS and state agencies. We verify these lists to determine whether we have been paid for the correct premium category and program. From time to time, CMS and state agencies require us to reimburse them for premiums that we received for individuals who were subsequently determined by us, or by CMS or state agencies, to be ineligible for any government-sponsored program or to belong to a plan other than ours. We receive additional premiums from CMS and state agencies for individuals who were subsequently determined to belong to our plan for periods in which we received no premium for those members. We estimate the amount of outstanding retroactivity adjustments and adjust premium revenue based on historical trends, premiums billed, the volume of member and contract renewal activity and other information. We record amounts receivable or payable in premiums receivable, net and other accrued expenses and liabilities in the consolidated balance sheets. In 2011, we reached a settlement with the Georgia Department of Community Health (the "Georgia DCH") to resolve issues with certain premium payments from the inception of the program in 2006 through the date of settlement related to the reconciliation of duplicate member records. The settlement resulted from a comprehensive review and negotiation involving the three health plans that operate in the program. During the year ended December 31, 2011, we recorded additional retroactive premium revenue and a receivable from the Georgia DCH related to the negotiated settlement. During the year ended December 31, 2012, CMS partially disallowed the settlement and we recorded a reduction of premium revenue of approximately $21,400. Amounts receivable from government agencies for member retroactivity were $28,024 and $28,267 at December 31, 2012 and 2011, respectively. The amounts due to government agencies for reconciling items were $19,944 and $7,292 at December 31, 2012 and 2011, respectively.
Supplemental Medicaid Premiums
We earn supplemental premium payments for eligible obstetric deliveries and newborns of our Medicaid members in Georgia, Illinois, Kentucky, New York and Ohio. We also earned supplemental payments for obstetric deliveries and newborns through the expiration of our Missouri contract on June 30, 2012. Each state Medicaid contract specifies how and when these supplemental payments are earned and paid. Upon delivery of a newborn, we notify the state agency according to the contract terms. We also earn supplemental Medicaid premium payments in some states for high cost drugs and certain services such as early childhood prevention screenings. We recognize supplemental premium revenue in the period we provide related services to our member. For the years ended December 31, 2012 and 2011, respectively, we recognized approximately $246,250 and $236,096 of supplemental Medicaid premium revenue.
Risk-Adjusted Medicare Premiums
CMS employs a risk-adjustment model to determine the premium amount it pays for each MA and PDP member. This model apportions premiums paid to all plans according to the health status of each beneficiary enrolled, resulting in higher risk scores for members with predictably higher costs. The model uses diagnosis data from inpatient and ambulatory treatment settings to calculate each risk score. We collect claims and encounter data for our MA members and submit the necessary diagnosis data to CMS within prescribed deadlines. After reviewing the respective submissions, CMS establishes the premium payments to MA plans at the beginning of the plan year, and then adjusts premium levels on a retroactive basis. The first retroactive adjustment for a given plan year generally occurs during the third quarter of that year and represents the update of risk scores for the current plan year based on the severity of claims incurred in the prior plan year. CMS then issues a final retroactive risk-adjusted premium settlement for that plan year in the following year.
We develop our estimates for risk-adjusted premiums utilizing historical experience and predictive models as sufficient member risk score data becomes available over the course of each CMS plan year. We populate our models with available risk score data on our members and base risk premium adjustments on risk score data from the previous year. We are not privy to risk score data for members new to our plans in the current plan year; therefore we include assumptions regarding these members' risk scores in our models. As we do not have access to diagnosis data with respect to our stand-alone PDP members, we cannot fully anticipate changes in our members' risk scores. We periodically revise our estimates of risk-adjusted premiums as additional diagnosis code information is reported to CMS and adjust our estimates to actual amounts when the ultimate adjustment settlements are either received from CMS or we receive notification from CMS of such settlement amounts. As a result of the variability of factors that determine our estimates for risk-adjusted premiums, the actual amount of the CMS retroactive payment could be materially more or less than our estimates and could have a material effect on our results of operations, financial position and cash flows. We record any changes in estimates in current operations as adjustments to premium revenue. Historically, we have not experienced significant differences between our estimates and amounts ultimately received. Additionally, the data provided to CMS to determine members' risk scores is subject to audit by CMS even after the annual settlements occur. An audit may result in the refund of premiums to CMS. While our experience to date has not resulted in a material refund, future refunds could materially reduce premium revenue in the year in which CMS determines a refund is required and could be material to our results of operations, financial position and cash flows. Premiums receivable in the accompanying consolidated balance sheets include MA risk adjusted premiums receivable of $74,767 and $35,772 and PDP risk-adjusted premiums receivable of $4,813 and $5,394, as of December 31, 2012 and 2011, respectively.
Minimum Medical Expense and Risk Corridor Provisions
We may be required to refund certain premium revenue to CMS and state government agencies under various contractual and plan arrangements. We estimate the impact of the following arrangements on a monthly basis and reflect any adjustments to premium revenues in current operations. We report the estimated amounts due to CMS and state agencies in other payables to government partners in the consolidated balance sheets.
Certain of our Florida Medicaid contracts and our Illinois Medicaid contract require us to expend a minimum percentage of premiums on eligible medical benefits expense. To the extent that we expend less than the minimum percentage of the premiums on eligible medical benefits expense, we are required to refund to the state all or some portion of the difference between the minimum and our actual allowable medical benefits expense. We estimate the amounts due to the state agencies as a return of premium based on the terms of our contracts with the applicable state agency.
Our MA and PDP prescription drug plan premiums are subject to risk sharing through the CMS Medicare Part D risk corridor provisions. The risk corridor calculation compares our actual experience to the target amount of prescription drug costs, limited to costs under the standard coverage as defined by CMS, less rebates in our submitted plan year bid. We receive additional premium from CMS if our actual experience is more than 5% above the target amount. We refund premiums to CMS if our actual experience is more than 5% below the target amount. After the close of the annual plan year, CMS performs the risk corridor calculation and any differences are settled between CMS and our plans. We have not historically experienced material differences between the subsequent CMS settlement amount and our estimates.
A summary of other payables to government partners is as follows:
|
| | | | | | | |
| | As of December 31, |
| | 2012 | | 2011 |
| Liability to states under minimum medical expense provisions | $ | 14,529 |
| | $ | 12,251 |
|
| Liability to CMS under risk corridor provision | 73,815 |
| | 85,986 |
|
| Other payables to government partners | $ | 88,344 |
| | $ | 98,237 |
|
Medicare Part D Settlements
We receive certain Part D prospective premium subsidy payments from CMS for our MA and PDP members based on the estimated costs of providing prescription drug benefits over the plan year. After the close of the annual plan year, CMS reconciles our actual experience to the prospective payments we received and any differences are settled between CMS and our plans. As such, these subsidies represent funding from CMS for which we assume no risk. We do not recognize the receipt of these subsidies as premium revenue and we do not recognize the payments of related prescription drug benefits as medical benefits expense. We report the subsidies received and benefits paid on a net basis as funds receivable (held) for the benefit of members in the consolidated balance sheets. We also report the net receipts and payments as a financing activity in our consolidated statements of cash flows. CMS pays the following subsidies prospectively as a fixed PMPM amount based upon the plan year bid submitted by us:
Low-Income Cost Sharing Subsidy—For qualifying LIS members, CMS reimburses us for all or a portion of deductible, coinsurance and co-payment amounts above the out-of-pocket threshold.
Catastrophic Reinsurance Subsidy—CMS reimburses us for 80% of the drug costs after a member reaches his or her out-of-pocket catastrophic threshold through a catastrophic reinsurance subsidy.
Coverage Gap Discount Subsidy—We advance the pharmaceutical manufacturers gap coverage discounts at the point of sale. On a periodic basis, CMS bills pharmaceutical manufacturers for discounts advanced by us. Pharmaceutical manufacturers remit payments for invoiced amounts directly to us. CMS reduces subsequent prospective payments made to us by the discount amounts billed to manufacturers.
CMS generally performs the Part D payment reconciliation in the fourth quarter of the following plan year based on prescription drug event ("PDE") data we submit to CMS within prescribed deadlines. After the Part D payment reconciliation for coverage gap discount subsidies, we may continue to report discounts to CMS for thirty-seven months following the end of the plan year. CMS will invoice manufacturers for these discounts and we will be paid through the quarterly manufacturer payments. Historically, we have not experienced material adjustments related to the CMS annual reconciliation of prior plan year low-income cost sharing and catastrophic reinsurance subsidies. We do not have a history of adjustments for the coverage gap discount subsidy as the 2011 plan year, which was the year CMS implemented the coverage gap discount subsidy, has not yet been settled by CMS.
Funds receivable (held) for the benefit of members consisted of the following:
|
| | | | | | | |
| | As of December 31, |
| | 2012 | | 2011 |
| Low-income cost sharing subsidy | $ | 52,861 |
| | $ | 54,659 |
|
| Catastrophic reinsurance subsidy | 90,384 |
| | 128,701 |
|
| Coverage gap discount subsidy | (16,418 | ) | | (20,586 | ) |
| Other, net | (181 | ) | | (29 | ) |
| Funds receivable for the benefit of members | $ | 126,646 |
| | $ | 162,745 |
|
Medical Benefits Expense and Medical Benefits Payable
We recognize the cost of medical benefits in the period in which services are provided, including an estimate of the cost of medical benefits incurred but not reported ("IBNR"). Medical benefits expense includes direct medical expenses and certain medically-related administrative costs.
Direct medical expenses include amounts paid or payable to hospitals, physicians and providers of ancillary services, such as laboratories and pharmacies. We also record direct medical expenses for estimated referral claims related to health care providers under contract with us who are financially troubled or insolvent and who may not be able to honor their obligations for the costs of medical services provided by others. In these instances, we may be required to honor these obligations for legal or business reasons. Based on our current assessment of providers under contract with us, such losses have not been and are not expected to be significant.We record direct medical expense for our estimates of provider settlements due to clarification of contract terms, out-of-network reimbursement, claims payment differences and amounts due to contracted providers under risk-sharing arrangements. We estimate pharmacy rebates earned based on historical utilization of specific pharmaceuticals, current utilization and contract terms and record amounts as a reduction of recorded direct medical expenses.
Consistent with the criteria specified and defined in guidance issued by HHS for costs that qualify to be reported as medical benefits under the minimum medical loss ratio provision of the 2010 Acts, we record certain medically-related administrative costs such as preventive health and wellness, care management, and other quality improvement costs, as medical benefits expense. All other medically-related administrative costs, such as utilization review services, network and provider credentialing and claims handling costs, are recorded in selling, general, and administrative expense.
Medical benefits payable represents amounts for claims fully adjudicated but not yet paid and estimates for IBNR. Our estimate of IBNR is the most significant estimate included in our consolidated financial statements.We determine our best estimate of the base liability for IBNR utilizing consistent standard actuarial methodologies based upon key assumptions which vary by business segment. Our assumptions include current payment experience, trend factors, and completion factors. Trend factors used in our standard actuarial methodologies include contractual requirements, historic utilization trends, the interval between the date services are rendered and the date claims are paid, denied claims activity, disputed claims activity, benefits changes, expected health care cost inflation, seasonality patterns, maturity of lines of business, changes in membership and other factors.
After determining an estimate of the base liability for IBNR, we make an additional estimate, also using standard actuarial techniques, to account for adverse conditions that may cause actual claims to be higher than the estimated base reserve. We refer to this additional liability as the provision for moderately adverse conditions. Our estimate of the provision for moderately adverse conditions captures the potential adverse development from factors such as:
•our entry into new geographical markets;
•our provision of services to new populations such as the aged, blind and disabled;
•variations in utilization of benefits and increasing medical costs;
•changes in provider reimbursement arrangements;
•variations in claims processing speed and patterns, claims payment and the severity of claims; and
•health epidemics or outbreaks of disease such as the flu.
We consider the base actuarial model liability and the provision for moderately adverse conditions as part of our overall assessment of our IBNR estimate to properly reflect the complexity of our business, the number of states in which we operate, and the need to account for different health care benefit packages among those states. We evaluate our estimates of medical benefits payable as we obtain more complete claims information and medical expense trend data over time. Volatility in members' needs for medical services, provider claims submissions and our payment processes result in identifiable patterns emerging several months after the causes of deviations from our assumed trends occur. Changes in our estimates of medical benefits payable cannot typically be explained by any single factor, but are the result of a number of interrelated variables, all of which influence the resulting medical cost trend. We record differences between actual experience and estimates used to establish the liability, which we refer to as favorable and unfavorable prior period developments, as increases or decreases to medical benefits expense in the period we identify the differences.
Reinsurance
We cede certain premiums and medical benefits to other insurance companies under various reinsurance agreements in order to increase our capacity to write larger risks and maintain our exposure to loss within our capital resources. We are contingently liable in the event the reinsurance companies do not meet their contractual obligations. We evaluate the financial condition of the reinsurance companies on a regular basis and only contract with well-known, well-established reinsurance companies that are supported by strong financial ratings.
We account for reinsurance premiums and medical expense recoveries according to the terms of the underlying reinsurance contracts. We recorded reinsurance premium payments of $2,999, $2,117, and $1,241 for the years ended December 31, 2012, 2011 and 2010, respectively, as a reduction to premium revenue in the accompanying consolidated statements of comprehensive income (loss). We recorded reinsurance recoveries of $4,903, $2,015, and $1,223 for the years ended December 31, 2012, 2011 and 2010, respectively, as a reduction of medical benefits expense in the accompanying consolidated statements of comprehensive income (loss). Reinsurance receivables of $6,539 and $2,242 as of December 31, 2012 and 2011, respectively, are included in prepaid and other current assets, net in the accompanying consolidated balance sheets.
Equity-Based Employee Compensation
The Compensation Committee of our Board of Directors (the "Compensation Committee") awards certain equity-based compensation under our 2004 Equity Incentive Plan, including stock options, restricted stock, restricted stock units ("RSUs"), performance stock units ("PSUs") and market stock units ("MSUs"). We estimate equity-based compensation expense based on awards ultimately expected to vest. We make assumptions of forfeiture rates at the time of grant and continuously reassess our assumptions based on actual forfeiture experience.
We estimate compensation cost for stock options, restricted stock and RSUs based on fair value at the time of grant and recognize the expense over the vesting period of the award. We measure the grant date fair value of stock options using the Black-Scholes options-pricing model. We measure the grant date fair value of restricted stock and RSUs based on the closing price of our common stock on the grant date.
At its sole discretion, the Compensation Committee sets certain financial and quality-based performance goals and a target award amount for each award of PSUs. PSUs generally cliff-vest approximately three years from the grant date based on the achievement of the performance goals and conditioned on the employee's continued service through the vesting date. The actual number of common stock shares earned upon vesting will range from zero shares to 150% of the target award amount. PSUs do not have a grant date or grant date fair value for accounting purposes as the subjective nature of the terms of the PSUs precludes a mutual understanding of the key terms and conditions. We recognize expense for PSUs ultimately expected to vest over the requisite service period based our estimates of progress made towards the achievement of the predetermined performance measures and changes in the market price of our common stock.
We estimate the fair value of MSUs at grant date using a Monte Carlo simulation approach based on randomly generated simulated stock-price paths through a lattice-type structure. We recognize compensation expense for MSUs expected to vest on a straight-line basis over the vesting period, generally three years. We calculate the number of shares of common stock earned upon vesting based on the number of base units granted multiplied by the ratio of the market price of our common stock during the last 30 market trading days of the calendar year immediately preceding both the vesting date and the grant date. The ratio is capped at 150%. If the ratio is less than 50%, no shares are earned by the recipient.
Member Acquisition Costs
We incur member acquisition costs, including internal commissions, external agent commissions on renewal policies, agent referral commissions, policy issuance and other administrative costs, in the acquisition and retention of our members. We record these costs as selling, general and administrative expense in the period we incur them.
We advance commissions to external agents and brokers for the acquisition of new members to our MA and PDP plans and defer amortization of these costs to the period in which we earn associated premium revenue, which is generally not more than one year.
Advertising Costs
We record the production costs of advertising activities as selling, general and administrative expense when incurred. We expense the costs of communicating advertising campaigns in the period the advertising takes place. We recorded advertising and related marketing expense of $7,238, $8,068, and $7,010 for the years ended December 31, 2012, 2011 and 2010, respectively.
Medicaid Premium Taxes
Premium rates established in the Medicaid contracts with state agencies in Hawaii, Missouri, New York and Ohio include an assessment or tax on Medicaid premiums. We recognize the premium tax assessment as expense in the period we earn the related premium revenue and remit the taxes back to the state agencies on a periodic basis. We incurred Medicaid premium taxes of $82,164, $76,163 and $56,374 for the years ended December 31, 2012, 2011 and 2010, respectively.
Income Tax Expense (Benefit)
We record income tax expense (benefit) as incurred based on enacted tax rates, estimates of book-to-tax differences in income, and projections of income that will be earned in each taxing jurisdiction. We recognize deferred tax assets and liabilities for the estimated future tax consequences of differences between the carrying amounts of existing assets and liabilities and their respective tax basis. We measure deferred tax assets and liabilities using tax rates applicable to taxable income in the years in which we expect to recover or settle those temporary differences. We record a valuation allowance on deferred taxes if we determine it is more likely than not that we will not fully realize the future benefit of deferred tax assets. We file tax returns after the close of our fiscal year end and adjust our estimated tax receivable or liability to the actual tax receivable or due per the filed state and federal tax returns. Historically, we have not experienced significant differences between our estimates of income tax expense (benefit) and actual amounts incurred.
State and federal taxing authorities may challenge the positions we take on our filed tax returns. We evaluate our tax positions and only recognize a tax benefit if it is more likely than not that a tax audit will sustain our conclusion. Based on our evaluation of tax positions, we believe that potential tax exposures have been recorded appropriately. State and federal taxing authorities may propose additional tax assessments based on periodic audits of our tax returns. We believe our tax positions comply with applicable tax law in all material aspects and we will vigorously defend our positions on audit. The ultimate resolution of these audits may materially impact our financial position, results of operations or cash flows. We have not experienced material adjustments to our consolidated financial statements as a result of these audits.
We participate in the Internal Revenue Service ("IRS") Compliance Assurance Program ("CAP"). The objective of CAP is to reduce taxpayer burden and uncertainty by working with the IRS to ensure tax return accuracy prior to filing, thereby reducing or eliminating the need for post-filing examinations.
Other Comprehensive Income
We record changes in net unrealized gains and losses on investments as a separate component of other comprehensive income, net of deferred income taxes, in the consolidated statements of comprehensive income (loss).
Cash and Cash Equivalents
We classify unrestricted cash and short-term investments with original maturities of three months or less as cash and cash equivalents in the consolidated balance sheets. We record cash and cash equivalents at cost, which approximates fair value.
Investments
We classify our fixed maturity securities, including short-term, long-term, and restricted investments, as available-for-sale and report them at fair value. We record unrealized gains and losses on securities, net of deferred income taxes, as a separate component of accumulated other comprehensive loss in the consolidated balance sheets. We record investment income when earned and classify investment income earned but not received in prepaid expenses and other current assets in the consolidated balance sheets. We may purchase fixed maturity securities at a premium or discount. We amortize these premiums and discounts as adjustments to investment income over the estimated remaining term of the securities. We determine realized gains and losses on sales of securities on a specific identification basis.
We determine the fair value of fixed maturity securities based on quoted prices in active markets or market prices provided by a third-party pricing service. The third-party pricing service determines market prices using inputs such as reported trades, benchmark yields, issuer spreads, bids, offers and estimated cash flows and prepayment spreads. Based on the typical trading volumes and the lack of quoted market prices for fixed maturities, third party pricing services will normally derive the security prices through recent reported trades for identical or similar securities making adjustments through the reporting date based upon available market observable information. If there are no recent reported trades, the pricing services may use matrix or model processes to develop a security price using future cash flow expectations based upon collateral performance and discount this at an estimated market rate. Our long-term investments include municipal note investments with an auction reset feature ("auction-rate securities"). We record the fair value of these auction-rate securities based on a discounted cash flow analysis.
We regularly compare the fair value of our investments to amortized cost of those investments. The evaluation of impairment is a quantitative and qualitative process which is subject to risk and uncertainties. Our fixed maturity investments are exposed to four primary sources of investment risk: credit, interest rate, liquidity and market valuation. The financial statement risks are those associated with the recognition of impairments and income, as well as the determination of fair values.
We perform a case-by-case evaluation of the underlying reasons for the decline in fair value and consider a wide range of factors about the security issuer, including assumptions and estimates about the operations of the issuer and its future earnings potential. We use our best judgment in evaluating the cause of the decline in the estimated fair value of the security and in assessing the prospects for near-term recovery. Our evaluation of impairment includes, but is not limited to:
| |
| • | the length of time and the extent to which the market value has been below cost; |
| |
| • | the potential for impairments of securities when the issuer is experiencing significant financial difficulties; |
| |
| • | the potential for impairments in an entire industry sector or sub-sector; |
| |
| • | the potential for impairments in certain economically depressed geographic locations; |
| |
| • | the potential for impairments of securities where the issuer, series of issuers or industry has suffered a catastrophic type of loss or has exhausted natural resources; |
| |
| • | unfavorable changes in forecasted cash flows on asset-backed securities; and |
| |
| • | other subjective factors, including concentrations and information obtained from regulators and rating agencies. |
We recognize impairments of securities when we consider a decline in fair value below the amortized cost basis to be other-than-temporary. If we intend to sell a security, or it is more likely than not that we will be required to sell the security before recovery of its amortized cost basis, we recognize an other-than-temporary impairment (OTTI) in earnings equal to the entire difference between the security's amortized cost basis and its fair value. If we do not intend to sell the security and it is more likely than not that we will not be required to sell the security before recovery of its amortized cost basis, but the present value of the cash flows expected to be collected is less than the amortized cost basis of the security (referred to as the credit loss), we conclude an OTTI has occurred. In this instance, we bifurcate the total OTTI into the amount related to the credit loss, which we recognize in earnings as investment income, net, with the remaining amount of the total OTTI attributed to other factors (referred to as the noncredit portion) recognized as a separate component in other comprehensive income. After the recognition of an OTTI, we account for the security as if it had been purchased on the measurement date of the OTTI, with an amortized cost basis equal to the previous amortized cost basis less than the OTTI recognized in earnings.
Restricted Investments
As a condition for licensure, we are required to maintain certain funds on deposit or pledged to various state agencies. Certain of our state contracts require the issuance of surety bonds. Through December 31, 2011, we were also required to maintain collateral deposits of cash, cash equivalents or securities in order to secure those surety bonds. In 2012, we no longer were required to collateralize our surety bonds. We record our restricted investments, which include cash, cash equivalents, and other short-term investments, at fair value. We classify restricted investments as long-term regardless of the contractual maturity date of the securities held, due to the nature of the states' requirements.
Prepaid Expenses and Other Current Assets
Prepaid expenses and other current assets, net, are comprised of the following: |
| | | | | | | |
| | As of December 31, |
| 2012 | | 2011 |
| Prepaid expenses | $ | 61,439 |
| | $ | 32,556 |
|
| Pharmaceutical coverage gap discounts receivable | 7,145 |
| | 15,130 |
|
| Advances to providers | 5,628 |
| | 6,491 |
|
| Other | 23,564 |
| | 10,226 |
|
| 97,776 |
| | 64,403 |
|
| Allowance for uncollectible advances to providers | (1,500 | ) | | (1,350 | ) |
| Prepaid expenses and other current assets, net | $ | 96,276 |
| | $ | 63,053 |
|
We record pharmaceutical coverage gap discounts receivable for amounts billed to pharmaceutical manufacturers by CMS for Medicare Part D coverage gap discounts advanced by us. Pharmaceutical manufacturers remit payments directly to us (see "Revenue Recognition - Medicare Prospective Premium Payments"). We also advance amounts to certain health care providers that are under contract with us to provide medical benefits to our members. We perform an analysis of our ability to collect outstanding advances based upon a review of the financial condition and solvency of the provider. We record a valuation allowance for advances we believe may not be collectible.
Property, Equipment and Capitalized Software, net
Property, equipment and capitalized software are stated at historical cost, net of accumulated depreciation. We capitalize certain costs incurred in the development of internal-use software, including external direct costs of materials and services and payroll costs of employees devoted to specific software development. We expense other software development costs, such as training and data conversion costs, as incurred. We capitalize the costs of improvements that extend the useful lives of the related assets.
We record depreciation expense using the straight-line method over the estimated useful lives of the related assets, which ranges from three to ten years for leasehold improvements, five for furniture and equipment, and three to five years for computer equipment and software. We include amortization of equipment under capital leases in depreciation expense. We record maintenance and repair costs as selling, general and administrative expense when incurred.
On an ongoing basis, we review events or changes in circumstances that may indicate that the carrying value of an asset may not be recoverable. If the carrying value of an asset exceeds the sum of estimated undiscounted future cash flows, we recognize an impairment loss in the current period for the difference between estimated fair value and carrying value. If assets are determined to be recoverable but the useful lives are shorter than we originally estimated, we depreciate the remaining net book value of the asset over the newly determined remaining useful lives. We did not recognize any impairment losses during the years ended December 31, 2012, 2011 or 2010.
Acquisitions
We included the results of Easy Choice's operations from the date of acquisition, November 9, 2012, in our consolidated financial statements. Revenues of $71,992 and net income of $1,210 attributable to Easy Choice are included in our consolidated statement of comprehensive income (loss) for the year ended December 31, 2012.
The estimated fair values of assets acquired and liabilities assumed on the date of acquisition are as follows: |
| | | |
| | |
| Cash and cash equivalents | $ | 23,489 |
|
| Investments | 5,115 |
|
| Premiums receivable, net | 4,419 |
|
| Pharmacy rebates receivable, net | 4,458 |
|
| Other assets | 7,108 |
|
| Total assets acquired | 44,589 |
|
| | |
| Medical benefits payable | (26,761 | ) |
| Accrued expenses and other payables | (5,555 | ) |
| Other payables to government partners | (2,263 | ) |
| Total liabilities assumed | (34,579 | ) |
| Fair value of net assets acquired | $ | 10,010 |
|
| | |
In connection with the Easy Choice acquisition, we recorded $43,400 of identified intangible assets. We valued the intangible assets using a discounted future cash flow analysis based on our consideration of historical financial results and expected industry and market trends. We discounted the future cash flows by a weighted-average cost of capital based on an analysis of the cost of capital for guideline companies within our industry. We amortize the intangible assets on a straight-line basis over the period we expect these assets to contribute directly or indirectly to the future cash flows. The weighted average amortization period for these intangibles was 14.4 years.
We recorded $112,708 of goodwill for the excess of the purchase price over the estimated fair value of net assets and identifiable intangible assets acquired net of an estimated $16,058 deferred tax liability. Recorded goodwill and other intangible assets related to the Easy Choice acquisition are not deductible for tax purposes.
In December 2012, we acquired certain assets of Arcadian Health Plan, Inc.'s Desert Canyon Community Care ("Desert Canyon") MA plans. We will provide services to approximately 4,000 Desert Canyon plan members effective January 1, 2013. In connection with the Desert Canyon acquisition, we recorded $2,020 of identified intangible assets. We valued the intangible assets using a discounted future cash flow analysis based on our consideration of historical financial results and expected industry and market trends. We discounted the future cash flows by a weighted-average cost of capital based on an analysis of the cost of capital for guideline companies within our industry. We amortize the intangible assets on a straight-line basis over the period we expect these assets to contribute directly or indirectly to the future cash flows. The weighted average amortization period for these intangibles was 10.8 years.
Goodwill and Other Intangible Assets
Goodwill represents the excess of the cost over the fair market value of net assets acquired. Goodwill recorded at December 31, 2012 consists of $112,708 and $111,131 attributable to our Medicare Advantage and Medicaid reporting segments, respectively. Goodwill recorded at December 31, 2011 is fully attributable to our Medicaid reporting segment.
Other intangible assets include provider networks, broker networks, trademarks, state contracts, non-compete agreements, licenses and permits. We amortize other intangible assets over their estimated useful lives ranging from approximately 1 to 26 years. These assets are allocated to reporting segments for impairment testing purposes.
We review goodwill and intangible assets for impairment at least annually, or more frequently if events or changes in our business climate occur that may potentially affect the estimated useful life or the recoverability of the remaining balance of goodwill or intangible assets. Such events or changes in circumstances would include significant changes in membership, state funding, federal and state government contracts and provider networks.We evaluate goodwill for impairment by first performing a qualitative assessment to determine whether a quantitative assessment is necessary. If, based on the qualitative assessment, we determine the fair value of the reporting unit is more likely than not less than the carrying value, we perform a two-step quantitative goodwill impairment test. In the first step, we determine the fair value of the reporting unit using both income and market approaches. We calculate fair value based on our assumptions of key factors such as projected revenues and the discount factor. While we believe these assumptions and estimates are appropriate, other assumptions and estimates could be applied and may produce significantly different results. If the fair value of the reporting unit is less than its carrying value, we measure and record the amount of the goodwill impairment, if any, by comparing the implied fair value of the reporting unit's goodwill with the carrying value. We perform our impairment test during the third quarter of each year. We perform our annual goodwill impairment test based on our financial position and results of operations through the second quarter of each year, which generally coincides with the finalization of federal and state contract negotiations and our initial budgeting process. Based on the results of the qualitative assessments performed as of our most recent testing date in 2012, we determined that the fair values of our reporting units are more likely than not greater than the carrying values as of December 31, 2012.
Recently Adopted Accounting Standards
In May 2011, the Financial Accounting Standards Board ("FASB") issued ASU 2011-04, "Fair Value Measurement (Topic 820): Amendments to Achieve Common Fair Value Measurement and Disclosure Requirements in U.S. GAAP and IFRS," which amended guidance on fair value measurement and related disclosures. The new guidance clarifies the concepts applicable for fair value measurement of non-financial assets and requires the disclosure of quantitative information about the unobservable inputs used in a fair value measurement. We adopted this guidance effective January 1, 2012. The adoption of this guidance did not have a material impact on our consolidated financial position, results of operations or cash flows.
In June 2011, the FASB issued ASU 2011-05, "Presentation of Comprehensive Income," and in December 2011 also issued ASU 2011-12, "Comprehensive Income (Topic 220): Deferral of the Effective Date for Amendments to the Presentation of Reclassifications of Items Out of Accumulated Other Comprehensive Income in Accounting Standards Update No. 2011-05," which amended guidance on the presentation of comprehensive income. This amended guidance eliminates one of the presentation options previously provided, which was to present the components of other comprehensive income as part of the statement of changes in stockholders' equity, and requires utilization of one of two optional methods. The amended guidance allows an entity to present the total of comprehensive income, the components of net income, and the components of other comprehensive income either in a single continuous statement of comprehensive income or in two separate but consecutive statements. We adopted this guidance effective January 1, 2012 and applied it retrospectively for all periods presented. The adoption of this guidance did not have an impact on our consolidated financial position, results of operations or cash flows.
In September 2011, the FASB issued ASU 2011-08, "Intangibles - Goodwill and Other." This guidance allows a qualitative assessment of whether it is more likely than not that a reporting unit's fair value is less than its carrying amount before applying the two-step goodwill impairment test. If it is more likely than not that the fair value of a reporting unit is less than its carrying amount, then the two-step impairment test for that reporting unit would be performed. We adopted this guidance effective January 1, 2012. The adoption of this guidance did not have a material impact on our consolidated financial position, results of operations or cash flows.
Recently Issued Accounting Standards
In July 2012, the FASB issued ASU 2012-02, "Testing Indefinite-Lived Intangible Assets for Impairment," which allows an entity to assess qualitative factors to determine whether it is necessary to perform a quantitative impairment test. An entity would not be required to calculate the fair value of indefinite-lived intangible assets unless the entity determines, based on qualitative assessment, that it is not more likely than not, the indefinite-lived intangible asset is impaired. ASU 2012-02 is effective for annual and interim impairment tests performed for fiscal years beginning after September 15, 2012, with early adoption permitted. We will adopt this guidance effective January 1, 2013. We do not believe the adoption of this standard will have a material impact on our consolidated financial position, results of operations or cash flows.
In July 2011, the FASB issued ASU 2011-06, "Other Expenses - Fees Paid to the Federal Government by Health Insurers." This update to the Accounting Standards Codification addresses accounting for the annual fees mandated by the 2010 Acts. The 2010 Acts impose an annual fee on health insurers, payable to the U.S. government, calculated on net premiums and third-party administrative agreement fees. The updated standard requires that the liability for the fee be estimated and accrued in full once the entity provides qualifying health insurance in the applicable calendar year in which the fee is payable with a corresponding deferred cost that is amortized to expense. The fees are initiated for calendar years beginning January 1, 2014, and the amendments provided by this update become effective for calendar years beginning after December 31, 2013. We are unable to estimate the magnitude of this fee on our consolidated financial position, results of operations or cash flows at this time.
In December 2011, the FASB issued ASU 2011-11, "Balance Sheet (Topic 210): Disclosures about Offsetting Assets and Liabilities." This update requires an entity to disclose information about offsetting and related arrangements to enable users of its financial statements to understand the effect of those arrangements on its financial position. ASU 2011-11 is effective for fiscal years beginning on or after January 1, 2013. We do not believe that the adoption of this standard will have a material impact on our consolidated financial position, results of operations or cash flows.
3. SEGMENT REPORTING
On a regular basis, we evaluate discrete financial information and assess the performance of our three reportable segments, Medicaid, MA and PDP, to determine the most appropriate use and allocation of Company resources.
Medicaid
Our Medicaid segment includes plans for beneficiaries of Temporary Assistance for Needy Families ("TANF"), Supplemental Security Income ("SSI"), Aged Blind and Disabled ("ABD") and other state-based programs that are not part of the Medicaid program, such as Children's Health Insurance Program ("CHIP"), Family Health Plus ("FHP"), and Managed Long-Term Care ("MLTC") programs. TANF generally provides assistance to low-income families with children. ABD and SSI generally provide assistance to low-income aged, blind or disabled individuals. CHIP and FHP programs provide assistance to qualifying families who are not eligible for Medicaid because their income exceeds the applicable income thresholds. The MLTC program is designed to help people with chronic illnesses or who have disabilities and need health and long-term care services, such as home care or adult day care, to enable them to stay in their homes and communities as long as possible.
Medicaid premium revenue attributable to Florida, Georgia, and for 2012, Kentucky, each individually accounts for 10% or more of our consolidated premium revenue, net of premium tax, as follows:
|
| | | | | | |
| | | For the Years Ended December 31, |
| | | 2012 | | 2011 | | 2010 |
| Florida | | 13% | | 15% | | 17% |
| Georgia | | 20% | | 24% | | 26% |
| Kentucky | | 10% | | 1% | | —% |
The state of Florida renewed our Florida Medicaid contracts for a three-year period beginning September 1, 2012 through August 31, 2015. This contract term may be superseded by the implementation of a reform of the statewide Medicaid Managed Care program (the "Medicaid Reform Program"). In 2013, the state began a competitive procurement program to award contracts for the Medicaid Reform Program. As a result, the state may terminate these contracts as early as the end of 2013, with the new contracts expected to begin in the first quarter of 2014.
Our Georgia Medicaid contract provides for two one-year renewal options exercisable by the Georgia Department of Community Health (the "Georgia DCH"). The Georgia DCH exercised its option to extend the term of our Georgia Medicaid contract until June 30, 2013 and the remaining renewal option potentially extends the contract through June 30, 2014. The Georgia DCH also indicated its intent to amend our Georgia Medicaid contract to include two additional one-year renewal options, exercisable by the Georgia DCH, that could potentially extend the contract term to June 30, 2016.
Our original Kentucky contract commenced in July 2011 and we began offering services to members on November 1, 2011. The contract has an initial three-year term and provides for four additional one-year option terms, exercisable upon mutual agreement of the parties, which potentially extends the total term until July 2018.
MA
Medicare is a federal program that provides eligible persons age 65 and over and some disabled persons with a variety of hospital, medical and prescription drug benefits. MA is Medicare's managed care alternative to the original Medicare program, which provides individuals standard Medicare benefits directly through CMS. Our MA CCPs generally require members to seek health care services and select a primary care physician from a network of health care providers. In addition, we offer coverage of prescription drug benefits under the Medicare Part D program as a component of most of our MA plans.
PDP
We offer stand-alone Medicare Part D coverage to Medicare-eligible beneficiaries in our PDP segment. The Medicare Part D prescription drug benefit is supported by risk sharing with the federal government through risk corridors designed to limit the losses and gains of the participating drug plans and by reinsurance for catastrophic drug costs. The government subsidy is based on the national weighted average monthly bid for this coverage, adjusted for risk factor payments. Additional subsidies are provided for dually-eligible beneficiaries and specified low-income beneficiaries. The Part D program offers national in-network prescription drug coverage that is subject to limitations in certain circumstances.
Summary of Financial Information
We allocate goodwill and other intangible assets to our reportable operating segments. We do not allocate any other assets and liabilities, investment and other income, or selling, general and administrative, depreciation and amortization, or interest expense to our reportable operating segments. The Company's decision-makers primarily use premium revenue, medical benefits expense and gross margin to evaluate the performance of our reportable operating segments. A summary of financial information for our reportable operating segments through the gross margin level, including the reclassification of prior year medical benefits expense as discussed in Note 1, and a reconciliation to income before income taxes, are presented in the following tables.
|
| | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | For the Years Ended December 31, |
| | 2012 | | | | 2011 | | | | | | 2010 | | |
| | | | Previously
Reported | | Amounts
Reclassified | | As
Adjusted | | Previously
Reported | | Amounts
Reclassified | | As
Adjusted |
| Premium revenue: | | | | | | | | | | | | | |
| Medicaid | $ | 4,471,232 |
| | $ | 3,581,611 |
| | $ | — |
| | $ | 3,581,611 |
| | $ | 3,308,751 |
| | $ | — |
| | $ | 3,308,751 |
|
| MA | 1,936,378 |
| | 1,479,750 |
| | — |
| | 1,479,750 |
| | 1,336,089 |
| | — |
| | 1,336,089 |
|
| PDP | 992,607 |
| | 1,036,769 |
| | — |
| | 1,036,769 |
| | 785,350 |
| | — |
| | 785,350 |
|
| Total premium revenue | 7,400,217 |
| | 6,098,130 |
| | — |
| | 6,098,130 |
| | 5,430,190 |
| | — |
| | 5,430,190 |
|
| Medical benefits expense: | | | |
| | |
| | |
| | | | | | |
| Medicaid | 3,892,076 |
| | 2,837,639 |
| | 52,451 |
| | 2,890,090 |
| | 2,847,315 |
| | 41,152 |
| | 2,888,467 |
|
| MA | 1,630,565 |
| | 1,180,500 |
| | 18,264 |
| | 1,198,764 |
| | 1,054,071 |
| | 13,107 |
| | 1,067,178 |
|
| PDP | 781,293 |
| | 853,932 |
| | 5,181 |
| | 859,113 |
| | 635,245 |
| | 3,647 |
| | 638,892 |
|
| Total medical benefits expense | 6,303,934 |
| | 4,872,071 |
| | 75,896 |
| | 4,947,967 |
| | 4,536,631 |
| | 57,906 |
| | 4,594,537 |
|
| Gross margin: | | | |
| | | | | | | | | | |
| Medicaid | 579,156 |
| | 743,972 |
| | (52,451 | ) | | 691,521 |
| | 461,436 |
| | (41,152 | ) | | 420,284 |
|
| MA | 305,813 |
| | 299,250 |
| | (18,264 | ) | | 280,986 |
| | 282,018 |
| | (13,107 | ) | | 268,911 |
|
| PDP | 211,314 |
| | 182,837 |
| | (5,181 | ) | | 177,656 |
| | 150,105 |
| | (3,647 | ) | | 146,458 |
|
| Total gross margin | 1,096,283 |
| | 1,226,059 |
| | (75,896 | ) | | 1,150,163 |
| | 893,559 |
| | (57,906 | ) | | 835,653 |
|
| Investment and other income | 8,815 |
| | 8,738 |
| | — |
| | 8,738 |
| | 10,035 |
| | — |
| | 10,035 |
|
| Other expenses | (808,659 | ) | | (827,130 | ) | | 75,896 |
| | (751,234 | ) | | (976,443 | ) | | 57,906 |
| | (918,537 | ) |
| Income (loss) from operations | $ | 296,439 |
| | $ | 407,667 |
| | $ | — |
| | $ | 407,667 |
| | $ | (72,849 | ) | | $ | — |
| | $ | (72,849 | ) |
Private Fee For Service Plan Exit
We previously offered MA private fee for service ("PFFS") plans through December 31, 2009. We did not renew our contracts to participate in the PFFS program due to costs that would have been required to meet additional regulations for PFFS plans imposed by CMS. The wind-down of our PFFS plans contributed approximately $10,883 and $36,945, respectively, in gross margin for the years ended December 31, 2011 and 2010, primarily as a result of the favorable development of PFFS medical benefits payable for service dates on or before December 31, 2009.
4. NET INCOME (LOSS) PER COMMON SHARE
We compute basic net income (loss) per common share on the basis of the weighted-average number of unrestricted common shares outstanding. We compute diluted net income per common share on the basis of the weighted-average number of unrestricted common shares outstanding plus the dilutive effect of outstanding stock options, restricted stock, restricted stock units, market stock units and performance stock units using the treasury stock method.
We calculated weighted-average common shares outstanding — diluted as follows:
|
| | | | | | | | |
| | For the Years Ended
December 31, |
| | 2012 | | 2011 | | 2010 |
| Weighted-average common shares outstanding — basic | 43,104,216 |
| | 42,817,466 |
| | 42,365,061 |
|
| Dilutive effect of: | | | | | |
| Unvested restricted stock, restricted stock units, market stock units and performance stock units | 526,030 |
| | 305,622 |
| | — |
|
| Stock options | 196,039 |
| | 205,668 |
| | — |
|
| Weighted-average common shares outstanding — diluted | 43,826,285 |
| | 43,328,756 |
| | 42,365,061 |
|
| Anti-dilutive stock options, restricted stock awards and performance equity awards excluded from computation | 57,455 |
| | 63,834 |
| | 1,871,567 |
|
For the years ended December 31, 2012 and 2011, we excluded certain equity awards from the computation of weighted-average common shares outstanding — diluted because their exercise prices were greater than the average market price of our common stock for the period. For the year ended December 31, 2010, we excluded all equity awards from the computation of diluted loss per share due to their anti-dilutive effect on the 2010 net loss per share.
5. INVESTMENTS
Short – term investments
The amortized cost, gross unrealized gains, gross unrealized losses and fair value of available-for-sale, short-term investments are as follows:
|
| | | | | | | | | | | | | | | |
| | Amortized
Cost | | Gross
Unrealized
Gains | | Gross
Unrealized
Losses | | Estimated
Fair Value |
| December 31, 2012 | | | | | | | |
| Corporate debt and other securities | $ | 35,287 |
| | $ | 15 |
| | $ | (2 | ) | | $ | 35,300 |
|
| Money market funds | 9,513 |
| | — |
| | — |
| | 9,513 |
|
| Municipal securities | 94,676 |
| | 16 |
| | (46 | ) | | 94,646 |
|
| Variable rate bond fund | 75,000 |
| | 686 |
| | — |
| | 75,686 |
|
| U.S. government securities | 5,197 |
| | 2 |
| | — |
| | 5,199 |
|
| Total | $ | 219,673 |
| | $ | 719 |
| | $ | (48 | ) | | $ | 220,344 |
|
| December 31, 2011 | |
| | |
| | |
| | |
|
| Certificates of deposit | $ | 12,401 |
| | $ | 2 |
| | $ | (2 | ) | | $ | 12,401 |
|
| Corporate debt and other securities | 27,364 |
| | 13 |
| | (5 | ) | | 27,372 |
|
| Money market funds | 41,720 |
| | — |
| | — |
| | 41,720 |
|
| Municipal securities | 66,736 |
| | 15 |
| | (27 | ) | | 66,724 |
|
| Variable rate bond fund | 50,000 |
| | — |
| | (55 | ) | | 49,945 |
|
| U.S. government securities | 399 |
| | 8 |
| | — |
| | 407 |
|
| Total | $ | 198,620 |
| | $ | 38 |
| | $ | (89 | ) | | $ | 198,569 |
|
Our short-term available-for-sale investments have contractual maturities within 1 year. We are not exposed to any significant concentration of credit risk in our short-term fixed maturities portfolio.
Long – term investments
The amortized cost, gross unrealized gains, gross unrealized losses and fair value of available-for-sale, long-term investments are as follows: |
| | | | | | | | | | | | | | | |
| | Amortized
Cost | | Gross
Unrealized
Gains | | Gross
Unrealized
Losses | | Estimated
Fair Value |
| December 31, 2012 | | | | | | | |
| Auction rate securities | $ | 34,150 |
| | $ | — |
| | $ | (2,104 | ) | | $ | 32,046 |
|
| Corporate debt and other securities | 26,879 |
| | 62 |
| | (11 | ) | | 26,930 |
|
| Municipal securities | 24,089 |
| | 28 |
| | (17 | ) | | 24,100 |
|
| U.S. government securities | 13,505 |
| | 119 |
| | — |
| | 13,624 |
|
| Total | $ | 98,623 |
| | $ | 209 |
| | $ | (2,132 | ) | | $ | 96,700 |
|
| December 31, 2011 | |
| | |
| | |
| | |
|
| Auction rate securities | $ | 34,950 |
| | $ | — |
| | $ | (2,551 | ) | | $ | 32,399 |
|
| Certificates of deposit | 5,000 |
| | 3 |
| | — |
| | 5,003 |
|
| Corporate debt and other securities | 13,340 |
| | 7 |
| | (356 | ) | | 12,991 |
|
| U.S. government securities | 32,481 |
| | 153 |
| | (8 | ) | | 32,626 |
|
| Total | $ | 85,771 |
| | $ | 163 |
| | $ | (2,915 | ) | | $ | 83,019 |
|
Contractual maturities of long-term available-for-sale investments at December 31, 2012 are as follows:
|
| | | | | | | | | | | | | | | | | | | |
| | Total | | Within
1 Year | | 1 Through 5
Years | | 5 Through 10
Years | | Thereafter |
| Auction rate securities | $ | 32,046 |
| | $ | — |
| | $ | — |
| | $ | — |
| | $ | 32,046 |
|
| Corporate debt and other securities | 26,930 |
| | — |
| | 22,405 |
| | — |
| | 4,525 |
|
| Municipal securities | 24,100 |
| | — |
| | 24,100 |
| | — |
| | — |
|
| U.S. government securities | 13,624 |
| | — |
| | 13,624 |
| | — |
| | — |
|
| Total | $ | 96,700 |
| | $ | — |
| | $ | 60,129 |
| | $ | — |
| | $ | 36,571 |
|
Actual maturities may differ from contractual maturities due to the exercise of pre-payment options.
Excluding investments in U.S. government securities, we are not exposed to any significant concentration of credit risk in our fixed maturities portfolio. Our long-term investments include auction rate securities, which are issued by various state and local municipal entities for the purpose of financing student loans, public projects and other activities. The auction rate securities carry investment grade credit ratings but are believed to be in an inactive market as discussed in Note 9. During the years ended December 31, 2012, 2011, and 2010, respectively, we redeemed $800, $11,200 and $10,850 auction rate securities at par. We did not realize any losses associated with selling or redeeming our auction rate securities for those years.
During the years ended December 31, 2012, 2011, and 2010, respectively, we sold or redeemed fixed maturity bond investments totaling $378,128, $200,516, $51,015, respectively. We realized gross losses of $54 associated with selling or redeeming fixed maturity bond securities for the year ended December 31, 2012, all attributable to sales of acquired Easy Choice investments to comply with our investment policies. We net the realized losses in investment and other income in the accompanying consolidated statements of comprehensive income (loss) for the year ended December 31, 2012. We did not realize any losses associated with selling or redeeming our fixed maturity bond securities for the years ended December 31, 2011 and 2010.
We recorded gross gains on sales or redemptions of our investments of $101 and $42 for the years ended December 31, 2012 and 2011, respectively. We did not realize any gains on sales or redemptions of investments during the year ended December 31, 2010.
We did not realize any OTTI for the years ended December 31, 2012, 2011 or 2010.
6. RESTRICTED INVESTMENT ASSETS
The amortized cost, gross unrealized gains, gross unrealized losses and fair value of our restricted investment securities are as follows:
|
| | | | | | | | | | | | | | | |
| | Amortized
Cost | | Gross
Unrealized
Gains | | Gross
Unrealized
Losses | | Estimated
Fair Value |
| December 31, 2012 | | | | | | | |
| Money market funds | $ | 18,630 |
| | $ | — |
| | $ | — |
| | $ | 18,630 |
|
| Cash | 29,179 |
| | — |
| | — |
| | 29,179 |
|
| Certificates of deposit | 1,551 |
| | — |
| | — |
| | 1,551 |
|
| U.S. government securities | 18,003 |
| | 2 |
| | (1 | ) | | 18,004 |
|
| Total | $ | 67,363 |
| | $ | 2 |
| | $ | (1 | ) | | $ | 67,364 |
|
| December 31, 2011 | |
| | |
| | |
| | |
|
| Money market funds | $ | 18,897 |
| | $ | — |
| | $ | — |
| | $ | 18,897 |
|
| Cash | 25,864 |
| | — |
| | — |
| | 25,864 |
|
| Certificates of deposit | 1,051 |
| | — |
| | — |
| | 1,051 |
|
| U.S. government securities | 14,843 |
| | 9 |
| | (1 | ) | | 14,851 |
|
| Total | $ | 60,655 |
| | $ | 9 |
| | $ | (1 | ) | | $ | 60,663 |
|
We did not realize any gains or losses related to restricted investments for the years ended December 31, 2012, 2011, or 2010.
7. PROPERTY, EQUIPMENT AND CAPITALIZED SOFTWARE
Property, equipment and capitalized software and related accumulated depreciation is as follows:
|
| | | | | | | |
| | December 31, |
| | 2012 | | 2011 |
| Leasehold improvements | $ | 20,570 |
| | $ | 16,492 |
|
| Computer equipment | 52,946 |
| | 47,273 |
|
| Capitalized software | 115,612 |
| | 84,958 |
|
| Furniture and equipment | 19,200 |
| | 17,621 |
|
| Property and equipment clearing | 3,278 |
| | 2,449 |
|
| Construction in progress | 28,700 |
| | 20,893 |
|
| | 240,306 |
| | 189,686 |
|
| Less accumulated depreciation | (108,788 | ) | | (91,448 | ) |
| Total property and equipment, net | $ | 131,518 |
| | $ | 98,238 |
|
We recognized depreciation expense on property, equipment and capitalized software of $29,243, $24,922, and $22,413 for the years ended December 31, 2012, 2011, and 2010, respectively, including amortization expense on capitalized software of $15,421, $11,482 and $10,512 for the years ended December 31, 2012, 2011, and 2010, respectively.
8. OTHER INTANGIBLE ASSETS
Other intangible assets as of December 31, 2012 and 2011, and related weighted-average amortization periods as of December 31, 2012, are as follows:
|
| | | | | | | | | | | | | | | | | | | | | | | | | |
| | As of December 31, |
| | 2012 | | 2011 |
| | Weighted Average Amortization Period (In Years) | | Gross Carrying Amount | | Accumulated Amortization | | Other Intangibles, Net | | Gross Carrying Amount | | Accumulated Amortization | | Other Intangibles, Net |
| Provider networks | 16.6 | | $ | 4,006 |
| | $ | (2,100 | ) | | $ | 1,906 |
| | $ | 4,878 |
| | $ | (4,434 | ) | | $ | 444 |
|
| Trademarks | 13.5 | | 12,143 |
| | (6,878 | ) | | 5,265 |
| | 10,443 |
| | (6,111 | ) | | 4,332 |
|
| Licenses and permits | 15.0 | | 5,271 |
| | (2,509 | ) | | 2,762 |
| | 5,270 |
| | (2,157 | ) | | 3,113 |
|
| State contracts | 14.8 | | 43,536 |
| | (2,309 | ) | | 41,227 |
| | 3,336 |
| | (1,329 | ) | | 2,007 |
|
| Broker networks | 10.0 | | 1,900 |
| | (32 | ) | | 1,868 |
| | — |
| | — |
| | — |
|
| Total other intangible assets | 14.5 | | $ | 66,856 |
| | $ | (13,828 | ) | | $ | 53,028 |
| | $ | 23,927 |
| | $ | (14,031 | ) | | $ | 9,896 |
|
We recorded amortization expense of $2,288, $1,532, and $1,533 for the years ended December 31, 2012, 2011 and 2010, respectively. Amortization expense expected to be recognized during fiscal years subsequent to December 31, 2012 is as follows:
|
| | | |
| | Expected Amortization Expense |
| 2013 | $ | 4,872 |
|
| 2014 | 4,820 |
|
| 2015 | 4,735 |
|
| 2016 | 4,735 |
|
| 2017 | 4,729 |
|
| 2018 and thereafter | 29,137 |
|
| Total | $ | 53,028 |
|
9. FAIR VALUE MEASUREMENTS
Our consolidated balance sheets include the following financial instruments: cash and cash equivalents, investments, receivables, accounts payable, medical benefits payable, long-term debt, and other liabilities. We consider the carrying amounts of cash and cash equivalents, receivables, other current assets and current liabilities to approximate their fair value due to the short period of time between the origination of these instruments and the expected realization or payment.
For other financial instruments, including short- and long-term investments, restricted investments, amounts accrued related to investigation resolution, and long-term debt, fair value is defined as the price that would be received to sell an asset or paid to transfer a liability in an orderly transaction between market participants at the measurement date. Assets and liabilities measured at fair value are classified using the following hierarchy, which is based upon the transparency of inputs to the valuation as of the measurement date.
Level 1—Quoted (unadjusted) prices for identical assets or liabilities in active markets: We include investments in commercial paper, money market funds, cash, U.S. government securities and the variable rate bond fund, as well as certain certificates of deposit and corporate debt, asset-backed and other municipal securities in Level 1. The carrying amounts of money market funds and cash approximate fair value because of the short-term nature of these instruments. We base fair values of the other investments included in Level 1 on unadjusted quoted market prices for identical securities in active markets.
Level 2—Inputs other than quoted prices in active markets: We include in Level 2 investments in certain certificates of deposit, corporate debt, asset-backed and other municipal securities for which fair market valuations are based on quoted prices for identical securities in markets that are not active, quoted prices for similar securities in active markets, broker or dealer quotations, or alternative pricing sources or for which all significant inputs are observable, either directly or indirectly, including interest rates and yield curves observable at commonly quoted intervals, volatilities, prepayment speeds, loss severities, credit risks, and default rates.
In addition to using market data, we make assumptions when valuing our assets and liabilities, including assumptions about risks inherent in the inputs to the valuation technique. When there is not an observable market price for an identical or similar asset or liability, we use an income approach reflecting our best assumptions regarding expected cash flows, discounted using a commensurate risk-adjusted discount rate. We estimated the fair value of the future payments related to investigation resolution using a discounted cash flow analysis and recorded these amounts at fair value in the short- and long-term portions of amounts accrued related to investigation resolution line items in our consolidated balance sheets. The carrying value of long-term debt was $135,000 at December 31, 2012. Based on a discounted cash flow analysis, the fair value of long-term debt was $131,770 at December 31, 2012.
Level 3—Unobservable inputs that cannot be corroborated by observable market data: We hold investments in auction rate securities, designated as available for sale and reported at fair value. At December 31, 2012, the auction rate securities had par values of $34,150. Liquidity for these auction rate securities is typically provided by an auction process which allows holders to sell their notes and resets the applicable interest rate at pre-determined intervals, usually every seven or 35 days. Auctions for these auction rate securities continued to fail during the twelve months ended December 31, 2012. An auction failure means that the parties wishing to sell their securities could not be matched with an adequate volume of buyers. As a result, our ability to liquidate and fully recover the carrying value of our remaining auction rate securities in the near term may be limited or non-existent. However, when there is a failed auction, the indenture governing the security requires the issuer to pay interest at a contractually defined rate that is generally above market rates for other types of similar instruments. We continue to receive interest payments on the auction rate securities we hold. Based on our analysis of anticipated cash flows, we have determined that it is more likely than not that we will be able to hold these securities until maturity or until market stability is restored. Additionally, there are government guarantees or municipal bond insurance in place and we have the ability and the present intent to hold these securities until maturity or market stability is restored. Based on this, we do not believe our auction rate securities are impaired and as a result, we have not recorded any impairment losses for our auction rate securities. However, as these securities are believed to be in an inactive market, we have estimated the fair value of these securities using a discounted cash flow model and update these estimates on a quarterly basis. Our analysis considered, among other things, the collateralization underlying the securities, the creditworthiness of the counterparty, the timing of expected future cash flows and the capital adequacy and expected cash flows of the subsidiaries that hold the securities. The estimated values of these securities were also compared, when possible, to valuation data with respect to similar securities held by other parties. Significant unobservable inputs used in the discounted cash flow model include the historical municipal bond index return rate and individual security credit ratings. Increases or decreases in the municipal bond index return rate or changes in security credit ratings could result in a significant change in the fair value estimation of our auction rate securities. Unobservable inputs included in our estimation of fair value of auction rate securities at December 31, 2012 included security credit ratings ranging from triple AAA/Aaa to BBB-/Baa3 and historical municipal bond index returns ranging from 0% to 8.5%. The fair values of auction rate securities are based on an approach that relies heavily on management assumptions and qualitative observations and therefore fall within Level 3 of the fair value hierarchy.
We determine transfers between levels at the end of the reporting period. No transfers between levels were recognized for the years ended December 31, 2012 and 2011.
Assets and liabilities measured at fair value at December 31, 2012:
|
| | | | | | | | | | | | | | | |
| | | | Fair Value Measurements Using |
| | Carrying Value | | Quoted Prices in
Active Markets
for Identical
Assets
(Level 1) | | Significant Other
Observable
Inputs
(Level 2) | | Significant
Unobservable
Inputs
(Level 3) |
| Investments: | | | | | | | |
| Auction rate securities | $ | 32,046 |
| | $ | — |
| | $ | — |
| | $ | 32,046 |
|
| Corporate debt securities | 57,705 |
| | — |
| | 57,705 |
| | — |
|
| Asset backed securities | 4,525 |
| | — |
| | 4,525 |
| | — |
|
| Money market funds | 9,513 |
| | 9,513 |
| | — |
| | — |
|
| Municipal securities | 118,746 |
| | — |
| | 118,746 |
| | — |
|
| Variable rate bond fund | 75,686 |
| | 75,686 |
| | — |
| | — |
|
| U.S. government securities | 18,823 |
| | 18,823 |
| | — |
| | — |
|
| Total investments | $ | 317,044 |
| | $ | 104,022 |
| | $ | 180,976 |
| | $ | 32,046 |
|
| | | | | | | | |
| Restricted investments: | |
| | |
| | |
| | |
|
| Money market funds | $ | 18,630 |
| | $ | 18,630 |
| | $ | — |
| | $ | — |
|
| Cash | 29,179 |
| | 29,179 |
| | — |
| | — |
|
| Certificates of deposit | 1,551 |
| | — |
| | 1,551 |
| | — |
|
| U.S. government securities | 18,004 |
| | 18,004 |
| | — |
| | — |
|
| Total restricted investments | $ | 67,364 |
| | $ | 65,813 |
| | $ | 1,551 |
| | $ | — |
|
| Amounts payable related to investigation resolution | $ | 105,476 |
| | $ | — |
| | $ | 105,476 |
| | $ | — |
|
Assets and liabilities measured at fair value at December 31, 2011:
|
| | | | | | | | | | | | | | | |
| | | | Fair Value Measurements Using |
| | Carrying Value | | Quoted Prices in Active Markets for Identical Assets
(Level 1) | | Significant Other Observable Inputs
(Level 2) | | Significant Unobservable Inputs
(Level 3) |
| Investments: | | | | | | | |
| Auction rate securities | $ | 32,399 |
| | $ | — |
| | $ | — |
| | $ | 32,399 |
|
| Certificates of deposit | 17,404 |
| | — |
| | 17,404 |
| | — |
|
| Corporate debt securities | 28,716 |
| | — |
| | 28,716 |
| | — |
|
| Commercial paper | 1,999 |
| | — |
| | 1,999 |
| | — |
|
| Asset backed securities | 9,648 |
| | — |
| | 9,648 |
| | — |
|
| Money market funds | 41,720 |
| | 41,720 |
| | — |
| | — |
|
| Municipal securities | 66,724 |
| | — |
| | 66,724 |
| | — |
|
| Variable rate bond fund | 49,945 |
| | 49,945 |
| | — |
| | — |
|
| U.S. government securities | 33,033 |
| | 33,033 |
| | — |
| | — |
|
| Total investments | $ | 281,588 |
| | $ | 124,698 |
| | $ | 124,491 |
| | $ | 32,399 |
|
| | | | | | | | |
| Restricted investments: | |
| | |
| | |
| | |
|
| Money market funds | $ | 18,897 |
| | $ | 18,897 |
| | $ | — |
| | $ | — |
|
| Cash | 25,864 |
| | 25,864 |
| | — |
| | — |
|
| Certificates of deposit | 1,051 |
| | — |
| | 1,051 |
| | — |
|
| U.S. government securities | 14,851 |
| | 14,851 |
| | — |
| | — |
|
| Total restricted investments | $ | 60,663 |
| | $ | 59,612 |
| | $ | 1,051 |
| | $ | — |
|
| Amounts payable related to investigation resolution | $ | 151,262 |
| | $ | — |
| | $ | 151,262 |
| | $ | — |
|
Changes in the fair value of our Level 3 auction rate securities:
|
| | | | | | | | | | | |
| | Fair Value Measurements Using Significant Unobservable Inputs (Level 3) For the Years Ended December 31, |
| | 2012 | | 2011 | | 2010 |
| Balance as of January 1 | $ | 32,399 |
| | $ | 42,245 |
| | $ | 51,710 |
|
| Realized gains (losses) in earnings | — |
| | — |
| | — |
|
| Changes in net unrealized gains and losses in other comprehensive income | 447 |
| | 1,354 |
| | 1,385 |
|
| Purchases, sales and redemptions | (800 | ) | | (11,200 | ) | | (10,850 | ) |
| Net transfers in or (out) of Level 3 | — |
| | — |
| | — |
|
| Balance as of December 31 | $ | 32,046 |
| | $ | 32,399 |
| | $ | 42,245 |
|
As a result of the increase in the fair value of our investments in auction rate securities, we recorded net unrealized gains of $447, $1,354, and $1,385 to accumulated other comprehensive loss during the years ended December 31, 2012, 2011 and 2010, respectively. The increase in the fair value was driven by improvement in the municipal bond market. We redeemed auction rate securities at par in the amount of $800 in July 2012, $6,700 in December 2011, $4,500 in May 2011, $4,550 in May 2010, and $6,300 in March 2010.
10. MEDICAL BENEFITS PAYABLE
Medical benefits payable consists of: |
| | | | | | | | | | | |
| | As of December 31, 2012 | | % of Total | | As of December 31, 2011 | | % of Total |
| IBNR | $ | 547,416 |
| | 75% | | $ | 526,736 |
| | 71% |
| Other medical benefits payable | 185,578 |
| | 25% | | 218,085 |
| | 29% |
| Total medical benefits payable | $ | 732,994 |
| | 100% | | $ | 744,821 |
| | 100% |
A reconciliation of the beginning and ending balances of medical benefits payable is as follows:
|
| | | | | | | | | | | |
| | For the Years Ended December 31, |
| | 2012 | | 2011 | | 2010 |
| Beginning balance | $ | 744,821 |
| | $ | 742,990 |
| | $ | 802,515 |
|
| Medical benefits incurred related to: | | | | | |
| Current period | 6,450,513 |
| | 5,200,106 |
| | 4,711,191 |
|
| Prior period | (146,579 | ) | | (252,139 | ) | | (116,254 | ) |
| Total | 6,303,934 |
| | 4,947,967 |
| | 4,594,937 |
|
| Medical benefits paid related to: | | | | | |
| Current period | (5,754,917 | ) | | (4,533,868 | ) | | (4,084,642 | ) |
| Prior periods | (560,844 | ) | | (412,268 | ) | | (569,820 | ) |
| Total | (6,315,761 | ) | | (4,946,136 | ) | | (4,654,462 | ) |
| Ending balance | $ | 732,994 |
| | $ | 744,821 |
| | $ | 742,990 |
|
Our estimates of medical benefits expense recorded at December 31, 2011, 2010 and 2009 developed favorably by approximately $146,579, $252,139, and $116,254 in 2012, 2011 and 2010, respectively. The release of the provision for moderately adverse conditions included in our prior period estimates was substantially offset by the provision for moderately adverse conditions established for claims incurred in the current year. Accordingly, the favorable development in our estimate of medical benefits payable related to claims incurred in prior years does not directly correspond to a decrease in medical benefits expense recognized during the period.
Excluding the prior period development related to the release of the provision for moderately adverse conditions, our estimates of medical benefits expense recorded at December 31, 2011, 2010 and 2009, developed favorably by approximately $76,681, $191,205 and $56,185 in 2012, 2011 and 2010, respectively. Our medical cost trend, mostly in our Medicaid segment and to a lesser extent in our MA and PDP segments, emerged favorably in 2012 and 2011, due primarily to lower than projected utilization. Higher than expected medical services in Kentucky in 2012 partially offset the favorable development related to the medical cost trend. The wind-down of PFFS claims related to service dates on or before December 31, 2009, following our exit from the PFFS program, contributed significantly to the favorable development in 2010, and to a lessor extent, in 2011. The impact of these developments was not discernible in advance and became clearer over time as we processed more claim payments and obtained more complete claims information.
11. DEBT
Credit Agreement
In August 2011, we entered into a $300,000 senior secured credit agreement, amended on July 20, 2012 (the "Amended Credit Agreement"), that provides for a $150,000 term loan facility as well as a $150,000 revolving credit facility. The term loan and revolving credit facility expire in August 2016. Payments of principal on the term loan are due on a quarterly basis through July 31, 2016. Upon closing, we borrowed $150,000 pursuant to the term loan facility. At December 31, 2012, $135,000 is outstanding under the Amended Credit Agreement, including $15,000 classified as a current liability in the accompanying consolidated balance sheet.
Our term loan bears interest at 1.75% as of December 31, 2012. Under the Amended Credit Agreement, outstanding credit facility borrowings designated as Alternate Base Rate ("ABR") loans bear interest at a rate per annum equal to an applicable margin ranging from 0.50% to 2.25% plus the greatest of:
| |
| • | the prime rate in effect on such day; |
| |
| • | the federal funds effective rate in effect on such day plus 0.50%; and |
| |
| • | the adjusted London Inter-Bank Offered Rate ("Adjusted LIBOR") for a 1-month interest period on such day plus 1%. |
Outstanding credit facility borrowings designated as Eurodollar loans bear interest at a rate per annum equal to Adjusted LIBOR for the interest period in effect plus an applicable margin ranging from 1.50% to 3.25%. Our ratio of total consolidated debt to consolidated earnings before interest, taxes, depreciation and amortization, as defined in the Amended Credit Agreement (our "Cash Flow Leverage Ratio") determines the applicable margin for both ABR and Eurodollar loans.
We incur a fee of 0.25% to 0.50% for unutilized commitments under the Amended Credit Agreement, depending upon our Cash Flow Leverage Ratio. We recorded total interest expense under the Amended Credit Agreement of $3,379 for the year ended December 31, 2012, including commitment fees and interest of $402 and $2,977, respectively. We recorded total interest expense under the Amended Credit Agreement of $1,838 for the year ended December 31, 2011, including commitment fees and interest of $305 and $1,533, respectively. We make interest payments based on the LIBOR election period, which ranges from a period of one to six months, and pay the commitment fees quarterly. As of December 31, 2012 and 2011, accrued interest payable was $171 and $271, respectively.
We defer and amortize debt issuance costs over the life of the Amended Credit Agreement using the straight-line method. Debt issuance costs, net of accumulated amortization, of $2,274 and $2,300 are included in the accompanying consolidated balance sheets at December 31, 2012 and 2011, respectively. We recorded amortization expense of $611 and $227 for the years ended December 31, 2012 and 2011, respectively.
Payments of principal on the term loan for the years succeeding December 31, 2012 are as follows:
|
| | | |
| | Future Principal Payments |
| 2013 | $ | 15,000 |
|
| 2014 | 18,750 |
|
| 2015 | 26,250 |
|
| 2016 | 75,000 |
|
| | $ | 135,000 |
|
The Amended Credit Agreement includes customary covenants and restrictions which, among other things, limit our ability to incur additional indebtedness. We may incur additional senior and subordinated unsecured indebtedness provided that our Cash Flow Leverage Ratio, calculated to include any such debt incurred, is at least 0.25 times less than the maximum Cash Flow Leverage Ratio. In addition, the Amended Credit Agreement requires that we maintain:
| |
| • | a Cash Flow Leverage Ratio of not more than 2.75 times; |
| |
| • | a minimum fixed charge coverage ratio of 3.00 times; |
| |
| • | a minimum level of statutory net worth for our regulated subsidiaries; and |
| |
| • | cash in an amount equal to one year of payment obligations due and payable to the U.S. Department of Justice during the next twelve consecutive months, so long as such obligations remain outstanding. For more information regarding our obligations to the Department of Justice see Note 12. |
The Amended Credit Agreement also contains customary representations and warranties and events of default. Payment of outstanding principal and related accrued interest may be accelerated and become immediately due and payable upon our default of payment or other performance obligations, or our failure to comply with financial or other covenants in the Amended Credit Agreement, subject to applicable notice requirements and cure periods.
As of the date of this filing, we have not drawn upon the revolving credit facility and we remain in compliance with all covenants.
Subordinated Notes
On September 30, 2011, we issued tradable unsecured subordinated notes with an aggregate par value of $112,500 in connection with a Stipulation and Agreement of Settlement (the "Stipulation Agreement") with the lead plaintiffs in the consolidated securities class action Eastwood Enterprises, L.L.C. v. Farha, et al., Case No. 8:07-cv-1940-VMC-EAJ. The stipulation and settlement agreement was approved on May 4, 2011 and resolved the putative class action complaints filed against us in 2007. On December 15, 2011, we repurchased all of the outstanding subordinated notes at a 10% discount and recorded a gain on the repurchase of $10,807. We recorded interest on the subordinated notes of approximately $4,254 during the year ended December 31, 2011.
12. COMMITMENTS AND CONTINGENCIES
Government Investigations
Under the terms of settlement agreements entered into on April 26, 2011, and finalized on March 23, 2012, to resolve matters under investigation by the Civil Division of the U.S. Department of Justice ("Civil Division") and certain other federal and state enforcement agencies (the "Settlement"), we agreed to pay the Civil Division a total of $137,500 over 36 months plus interest accrued at 3.125%. The estimated fair value of the discounted remaining liability, to be paid in three annual installments of $34,375, and related interest, was $105,476 at December 31, 2012, of which $37,305 and $68,171 has been included in the current and long-term portions, respectively, of amounts payable related to the investigation resolution in the accompanying consolidated balance sheet as of December 31, 2012.
The Settlement also provides for a contingent payment of an additional $35,000 in the event that we are acquired or otherwise experience a change in control within three years of the effective date of the Settlement, provided that the change in control transaction exceeds certain minimum transaction value thresholds as specified in the Settlement.
On April 12, 2012, joint stipulations of dismissal were filed in this action, dismissing underlying qui tam complaints. On April 30, 2012, the United States District Court for the Middle District of Florida entered an order dismissing the action.
Securities Class Action Complaint
We remain subject to two contingencies related to the Stipulation Agreement (Note 11). If, within three years of May 4, 2011, we are acquired or otherwise experience a change in control at a share price of $30.00 or more, we must pay an additional $25,000 to the class action plaintiffs. The Stipulation Agreement also requires us to pay to the class action plaintiffs 25.00% of any sums we recover from Todd Farha, Paul Behrens and/or Thaddeus Bereday related to the same facts and circumstances that gave rise to the consolidated securities class action.
Corporate Integrity Agreement
We operate under a Corporate Integrity Agreement (the "Corporate Integrity Agreement") with the Office of Inspector General of the United States Department of Health and Human Services ("OIG-HHS"). The Corporate Integrity Agreement has a term of five years from its effective date of April 26, 2011 and mandates various ethics and compliance programs designed to help ensure our ongoing compliance with federal health care program requirements. The terms of the Corporate Integrity Agreement include certain organizational structure requirements, internal monitoring requirements, compliance training, screening processes for new employees, reporting requirements to OIG-HHS, and the engagement of an independent review organization to review and prepare written reports regarding, among other things, WellCare's reporting practices and bid submissions to federal health care programs.
Indemnification Obligations
Under Delaware law, our charter and bylaws and certain indemnification agreements to which we are a party, we are obligated to indemnify, or have otherwise agreed to indemnify, certain of our current and former directors, officers and associates with respect to current and future investigations and litigation, including the matters discussed in this Note 12. The indemnification agreements for our directors and executive officers with respect to events occurring prior to May 2009 require us to indemnify an indemnitee to the fullest extent permitted by law if the indemnitee was or is or becomes a party to or witness or other participant in any proceeding by reason of any event or occurrence related to the indemnitee's status as a director, officer, employee agent or fiduciary of the Company or any of our subsidiaries and all expenses, including attorney's fees, judgments, fines, settlement amounts and interest and other charges, and any taxes as a result of the receipt of payments under the indemnification agreement. We will not indemnify the indemnitee if not permitted under applicable law. We are required to advance all expenses incurred by the indemnitee. We are entitled to reimbursement by an indemnitee if the indemnitee is not permitted to be reimbursed under applicable law after a final judicial determination is made and all rights of appeal have been exhausted or lapsed.
We amended and restated our indemnification agreements in May 2009. The revised agreements apply to our officers and directors with respect to events occurring after that time. Pursuant to the 2009 indemnification agreements, we will indemnify the indemnitee against all expenses, including attorney's fees, judgments, penalties, fines, settlement amounts and any taxes imposed as a result of payments made under the indemnification agreement incurred in connection with any proceedings that relate to the indemnitee's status as a director, officer or employee of the Company or any of our subsidiaries or any other enterprise that the indemnitee was serving at our request. We will also indemnify for expenses incurred by the indemnitee if an indemnitee, by reason of his or her corporate status, is a witness in any proceeding. Further, we are required to indemnify for expenses incurred by an indemnitee in defense of a proceeding to the extent the indemnitee has been successful on the merits or otherwise. Finally, if the indemnitee is involved in certain proceedings as a result of the indemnitee's corporate status, we are required to advance the indemnitee's reasonable expenses incurred in connection with such proceeding, subject to the requirement that the indemnitee repay the expenses if it is ultimately determined that the indemnitee is not entitled to be indemnified.We are not obligated to indemnify an indemnitee for losses incurred in connection with any proceeding if a determination has not been made by the Board of Directors, a committee of disinterested directors or independent legal counsel in the specific case that the indemnitee has satisfied any standards of conduct required as a condition to indemnification under Section 145 of the Delaware General Corporation Law.
Pursuant to our obligations, we have advanced, and will continue to advance, legal fees and related expenses to three former officers and two additional associates who were criminally indicted in connection with the government investigations of the Company that commenced in 2007 of various federal criminal health care fraud charges including conspiracy to defraud the United States, false statements relating to health care matters, and health care fraud in connection with their defense of criminal charges. The trial is scheduled to begin in the first quarter of 2013.
We have also previously advanced legal fees and related expenses to these five criminally-indicted individuals regarding disputes in Delaware Chancery Court related to whether we were legally obligated to advance fees or indemnify certain of these executives; the class actions titled Eastwood Enterprises, L.L.C. v. Farha, et al. and Hutton v. WellCare Health Plans, Inc. et al. filed in federal court; six stockholder derivative actions filed in federal and state courts between October 2007 and January 2008; an investigation by the United States Securities & Exchange Commission (the "Commission"); and an action by the Commission filed in January 2012 against Messrs. Farha, Behrens and Bereday. The Delaware Chancery Court cases have concluded. We settled the class actions in May 2011. In 2010, we settled the stockholder derivative actions and we were realigned as the plaintiff to pursue our claims against Messrs. Farha, Behrens and Bereday. These actions, as well as the action by the Commission, have been stayed until the conclusion of the criminal trial.
In connection with these matters, we have advanced to the five criminally-indicted individuals legal fees and related expenses of approximately $109,887 from the inception of the investigations to December 31, 2012. We expensed these costs as incurred and classified the costs as selling, general and administrative expense incurred in connection with the investigations and related matters.
In August 2010, we entered into an agreement and release with the carriers of our directors and officers ("D&O") liability insurance relating to coverage we sought for claims relating to the previously disclosed government investigations and related litigation. We agreed to accept payment of $32,500 in satisfaction of the $45,000 face amount of the relevant D&O insurance policies and the carriers agreed to waive any rights they may have to challenge our coverage under the policies. As a result, we have exhausted our insurance policies related to reimbursement of our advancement of fees related to these matters. We received payment of $6,700 prior to 2010 and recorded the receipt of the remaining $25,800 of insurance proceeds as a reduction to selling, general and administrative expense during the year ended December 31, 2010.
We expect the continuing cost of our obligations to the five criminally-indicted former employees in connection with their defense of criminal charges to be significant and to continue for a number of years. We are unable to estimate the total amount of these costs or a range of possible loss. Accordingly, we continue to expense these costs as incurred. Our indemnification obligations and requirements to advance legal fees and expenses may have a material adverse effect on our financial condition, results of operations and cash flows.
Other Lawsuits and Claims
Based on the nature of our business, we are subject to regulatory reviews or other investigations by various state insurance and health care regulatory authorities and other state and federal regulatory authorities. These authorities regularly scrutinize the business practices of health insurance and benefits companies and their reviews focus on numerous facets of our business, including claims payment practices, provider contracting, competitive practices, commission payments, privacy issues and utilization management practices, among others. Some of these reviews have historically resulted in fines imposed on us and some have required changes to our business practices. We continue to be subject to such reviews, which may result in additional fines and/or sanctions being imposed or additional changes in our business practices.
Separate and apart from the legal matters described above, we are also involved in other legal actions in the normal course of our business, including, without limitation, wage and hour claims and provider disputes regarding payment of claims. Some of these actions seek monetary damages, including claims for liquidated or punitive damages, which are not covered by insurance. We review relevant information with respect to litigation matters and we update our estimates of reasonably possible losses and related disclosures. We accrue an estimate for contingent liabilities, including attorney's fees related to these matters, if a loss is deemed probable and is estimable. Currently, we do not expect that the resolution of any currently pending actions, either individually or in the aggregate, will differ materially from our current estimates or have a material adverse effect on our results of operations, financial position, and cash flows. However, the outcome of any legal actions cannot be predicted, and therefore, actual results may differ from those estimates.
Operating Leases
We recorded rental expense of $17,047, $18,002, and $17,312 for the years ended December 31, 2012, 2011 and 2010, respectively, related to our operating leases for office space. Future minimum lease payments under non-cancelable operating leases with initial or remaining lease terms in excess of one year at December 31, 2012 are as follows:
|
| | | |
| | Minimum Lease Payments |
| 2013 | $ | 19,323 |
|
| 2014 | 16,437 |
|
| 2015 | 13,081 |
|
| 2016 | 8,012 |
|
| 2017 | 5,790 |
|
| 2018 and thereafter | 8,288 |
|
| Total | $ | 70,931 |
|
13. INCOME TAXES
The Company and subsidiaries file a consolidated federal income tax return and separate state franchise, income and premium tax returns, as applicable. The following table provides components of income tax expense (benefit):
|
| | | | | | | | | | | |
| | For the Years Ended December 31, |
| | 2012 | | 2011 | | 2010 |
| Current: | | | | | |
| Federal | $ | 83,955 |
| | $ | 59,541 |
| | $ | 44,389 |
|
| State | 8,595 |
| | (1,166 | ) | | 4,116 |
|
| | 92,550 |
| | 58,375 |
| | 48,505 |
|
| Deferred: | | | | | |
| Federal | 18,126 |
| | 87,039 |
| | (61,742 | ) |
| State | 1,035 |
| | 8,814 |
| | (6,212 | ) |
| | 19,161 |
| | 95,853 |
| | (67,954 | ) |
| Total income tax expense (benefit) | $ | 111,711 |
| | $ | 154,228 |
| | $ | (19,449 | ) |
A reconciliation of income tax at the statutory federal rate of 35% to income tax at the effective rate is as follows:
|
| | | | | | | | | | | |
| | For the Years Ended December 31, |
| | 2012 | | 2011 | | 2010 |
| Income tax expense (benefit) at statutory federal rate | $ | 103,754 |
| | $ | 146,466 |
| | $ | (25,497 | ) |
| Adjustments resulting from: | | | | | |
| State income tax, net of federal benefit | 6,670 |
| | 8,058 |
| | (3,785 | ) |
| Provision-to-return differences | — |
| | (2,257 | ) | | 893 |
|
| Non-deductible executive compensation | 2,415 |
| | 1,640 |
| | 2,079 |
|
| Non-deductible amounts related to investigation resolution | (1,302 | ) | | 236 |
| | 5,703 |
|
| Interest on unrecognized tax benefits | (114 | ) | | (318 | ) | | (91 | ) |
| Other, net | 288 |
| | 403 |
| | 1,249 |
|
| Total income tax expense (benefit) | $ | 111,711 |
| | $ | 154,228 |
| | $ | (19,449 | ) |
Our effective income tax rate on pre-tax income was 37.7% for the year ended December 31, 2012, compared to 36.9% for the year ended December 31, 2011 and 26.7% on a pre-tax loss for the year ended December 31, 2010. The 2012 effective tax rate was 0.8% higher than 2011 due primarily to a settlement of a state tax matter, partially offset by a decrease in the prevailing state income tax rate.
Significant components of our deferred tax assets and liabilities are: |
| | | | | | | |
| | As of December 31, |
| Deferred tax assets: | 2012 | | 2011 |
| Medical and other benefits discounting | $ | 12,261 |
| | $ | 12,085 |
|
| Unearned premium discounting | 11 |
| | 12 |
|
| Tax basis assets | 8,441 |
| | 7,154 |
|
| Allowance for doubtful accounts | 5,742 |
| | 3,893 |
|
| Amount payable related to investigation resolution | 13,042 |
| | 22,280 |
|
| Accrued expenses and other | 27,768 |
| | 22,192 |
|
| | 67,265 |
| | 67,616 |
|
| Deferred tax liabilities: | | | |
| Goodwill, other intangible assets and property and equipment | 28,666 |
| | 10,222 |
|
| Software development costs | 42,980 |
| | 30,193 |
|
| Prepaid assets | 10,469 |
| | 5,895 |
|
| | 82,115 |
| | 46,310 |
|
| Net deferred tax (liability) asset | $ | (14,850 | ) | | $ | 21,306 |
|
We have not recorded a valuation allowance at December 31, 2012 and 2011 as we expect that we will fully realize our deferred tax assets.
We classify deferred tax assets and liabilities in the consolidated balance sheets as follows:
|
| | | | | | | |
| | As of December 31, |
| | 2012 | | 2011 |
| Current assets | $ | 27,208 |
| | $ | 22,332 |
|
| Non-current liabilities | (42,058 | ) | | (1,026 | ) |
| Net deferred tax (liability) asset | $ | (14,850 | ) | | $ | 21,306 |
|
A reconciliation of the beginning and ending amount of unrecognized tax benefits is as follows:
|
| | | | | | | |
| | Years Ended December 31, |
| | 2012 | | 2011 |
| Gross unrecognized tax benefits, beginning of period | $ | 3,525 |
| | $ | 3,370 |
|
| Gross increases: | | | |
| Prior year tax positions | — |
| | 155 |
|
| Current year tax positions | — |
| | — |
|
| Gross decreases: | | | |
| Prior year settlements | — |
| | — |
|
| Prior year tax positions | (3,525 | ) | | — |
|
| Statute of limitations lapses | — |
| | — |
|
| Gross unrecognized tax benefits, end of period | $ | — |
| | $ | 3,525 |
|
We believe it is reasonably possible that our liability for unrecognized tax benefits will not significantly increase or decrease in the next twelve months as a result of audit settlements and the expiration of statutes of limitations in certain major jurisdictions.
We classify interest and penalties associated with uncertain income tax positions as income taxes within our consolidated financial statements. During the years ended December 31, 2012 and 2011, we recognized interest benefit of $114 and $318, respectively. We did not incur or record accrued penalties for the years ended December 31, 2012 and 2011. As of December 31, 2012 there were no unrecognized tax benefits that would affect the effective tax rate.
We file our income tax returns in the U.S. federal jurisdiction and various states. The U.S. IRS recently issued a "no change" report for our federal income tax return for the 2011 tax year after advance review under CAP. We are no longer subject to state and local tax examinations prior to 2004. As of December 31, 2012 we are not aware of any material proposed adjustments.
14. EQUITY-BASED COMPENSATION
We recorded equity-based compensation expense of $14,886, $19,527 and $14,801 for the years ended December 31, 2012, 2011, and 2010, respectively. As of December 31, 2012, we expect $14,394 of unrecognized compensation cost related to non-vested equity-based compensation arrangements to be recognized over a weighted-average period of 1.8 years.
The weighted-average grant-date fair values of shares granted during the years ended December 31, 2012 , 2011, and 2010 were $64.19, $41.66, and $29.23, respectively. The total fair value of all shares vested during the year ended December 31, 2012 was $9,341. We generally repurchase vested shares to satisfy tax withholding requirements and then retire the repurchased shares.
Stock Options
A summary of our stock option activity for the year ended December 31, 2012, and the aggregate intrinsic value and weighted average remaining contractual term for our stock options as of December 31, 2012, is:
|
| | | | | | | | | | | | |
| | Shares | | Weighted
Average
Exercise
Price | | Aggregate
Intrinsic
Value | | Weighted
Average
Remaining
Contractual
Term (Years) |
| Outstanding as of January 1, 2012 | 693,288 |
| | $ | 26.94 |
| | | | |
| Granted | — |
| | — |
| | | | |
| Exercised | (251,483 | ) | | 27.90 |
| | | | |
| Forfeited and expired | (5,929 | ) | | 26.68 |
| | | | |
| Outstanding as of December 31, 2012 | 435,876 |
| | 26.40 |
| | $ | 9,724 |
| | 2.6 |
| Exercisable as of December 31, 2012 | 430,001 |
| | 26.50 |
| | $ | 9,547 |
| | 2.5 |
| Vested and expected to vest as of December 31, 2012 | 435,876 |
| | 26.40 |
| | $ | 9,724 |
| | 2.6 |
The Compensation Committee did not grant any stock option awards during the years ended December 31, 2012 and 2011. For options granted during the year ended December 31, 2010, we estimated the fair value of each option award on the date of grant using a Black-Scholes option pricing model with the following assumptions:
|
| | |
| Weighted average risk-free interest rate | 2.01 | % |
| Range of risk-free rates | 1.14% - 2.30% |
|
| Expected term (in years) | 4.29 |
|
| Expected dividend yield | — | % |
| Expected volatility | 65.15 | % |
We base expected volatility assumptions on the historical volatility of our common stock. We determine the expected term of options granted using historical and industry data to estimate option exercise patterns and forfeitures resulting from employee terminations. We derive our forfeiture estimate at the time of grant and continuously reassess this estimate to determine if our assumptions are indicative of actual forfeitures. Our forfeiture rate assumptions vary by equity award type. We have not historically declared dividends, nor do we intend to in the foreseeable future. We base the risk-free rate for options granted on the rate for zero-coupon U.S. treasury bonds with terms commensurate with the expected term of the granted option.
The weighted-average grant-date fair value of options granted during the year ended December 31, 2010 was $15.40. The total intrinsic value of options exercised during the years ended December 31, 2012, 2011, and 2010 was $9,780, $4,390, and $1,130, respectively.
For the years ended December 31, 2012, 2011, and 2010, we received cash from option exercises of $9,407, $6,288, and $1,444, respectively. We currently expect to satisfy equity-based compensation awards with available unissued registered shares.
Restricted Stock and RSUs
A summary of our restricted stock and RSU activity for the year ended December 31, 2012 is:
|
| | | | | | |
| | Restricted
Stock and
RSUs | | Weighted
Average
Grant-Date
Fair Value |
| Outstanding as of January 1, 2012 | 396,924 |
| | $ | 33.19 |
|
| Granted | 145,856 |
| | 61.26 |
|
| Vested | (217,051 | ) | | 33.82 |
|
| Forfeited and expired | (52,555 | ) | | 42.48 |
|
| Outstanding as of December 31, 2012 | 273,174 |
| | 45.90 |
|
MSUs
A summary of our MSU activity for the year ended December 31, 2012 is:
|
| | | | | | |
| | MSUs | | Weighted
Average
Grant-Date
Fair Value |
| Outstanding as of January 1, 2012 | — |
| | $ | — |
|
| Granted | 69,871 |
| | 74.16 |
|
| Vested | — |
| | — |
|
| Forfeited and expired | (7,678 | ) | | 75.21 |
|
| Outstanding as of December 31, 2012 | 62,193 |
| | 74.03 |
|
For MSU's granted during the year ended December 31, 2012, we estimated the fair value of each MSU award on the date of the grant using a Monte Carlo simulation model based on the following assumptions: weighted average expected volatility 44.11%, range of risk-free interest rates of 0.26% - 0.41% and a dividend yield of 0%. Expected volatilities are based on a blended volatility calculated based on the historical volatility of our stock price and implied volatility from traded options of our stock. Risk-free interest rates for MSU awards are based on the zero-coupon U.S. treasury yield curve.
PSUs
A summary of our PSU activity for the year ended December 31, 2012 is:
|
| | | | | | |
| | PSUs | | Weighted
Average
Grant-Date
Fair Value |
| Outstanding as of January 1, 2012 | 286,894 |
| | $ | 35.65 |
|
| Granted | 196,436 |
| | 62.83 |
|
| Vested | — |
| | — |
|
| Forfeited and expired | (61,764 | ) | | 45.89 |
|
| Outstanding as of December 31, 2012 | 421,566 |
| | 46.81 |
|
15. RELATED-PARTY TRANSACTIONS
The Graham Companies
We lease office space from The Graham Companies, in which a member of the board of directors and his immediate family has a 23% ownership interest. During the years ended 2012, 2011 and 2010, respectively, we paid $145, $134, and $139 in rental expense to The Graham Companies.
DaVita
We conduct business with DaVita, Inc. ("DaVita") pursuant to which DaVita provides medical services to a portion of our member base. The Chairman of our board of directors is also a member of DaVita's board of directors. During the years ended December 31, 2012, 2011 and 2010, we purchased $3,977, $3,418, and $3,139, respectively, of services from DaVita. For the year ended December 31, 2012, we paid capitation payments of $6,361 to a subsidiary acquired by DaVita in 2012.
The WellCare Community Foundation
We provide charitable support to The WellCare Community Foundation ("the Foundation"). We established the Foundation to promote the health and quality of life for medically under-served populations including the elderly, young and indigent. We did not make or commit to make any contributions to the Foundation during 2012. During the years ended December 31, 2011 and 2010, we recorded total contribution expense of $1,000 and $500, respectively, included in selling, general and administrative expense.
16. REGULATORY CAPITAL AND DIVIDEND RESTRICTIONS
State insurance laws and regulations prescribe accounting practices for determining statutory net income and capital and surplus. Each of our health maintenance organization ("HMO") and insurance subsidiaries must maintain a minimum amount of statutory capital determined by statute or regulation. Minimum statutory capital requirements differ by state and are generally based on a percentage of annualized premium revenue, a percentage of annualized health care costs, a percentage of certain liabilities, a statutory minimum risk-based capital ("RBC") requirement or other financial ratios. Most states have adopted RBC requirements based on guidelines established by the National Association of Insurance Commissioners ("NAIC"). Each state legislature may modify the NAIC's RBC requirements as it deems appropriate. The RBC formula, based on asset risk, underwriting risk, credit risk, business risk and other factors, computes the amount of capital required to support an entity's business, referred to as the authorized control level ("ACL"). For states in which the RBC requirements have been adopted, the regulated entity typically must maintain a minimum of the greater of 200% of the required ACL or the minimum statutory net worth requirement calculated pursuant to pre-RBC guidelines. As of December 31, 2012, our operating HMO and insurance company subsidiaries in all states except California, New York and Florida were subject to RBC requirements. Our subsidiaries operating in Texas and Ohio are required to maintain statutory capital at RBC levels equal to 225% and 300%, respectively, of the applicable ACL. Failure to maintain these requirements would trigger regulatory action by the state. At December 31, 2012, our HMO and insurance subsidiaries were in compliance with these minimum capital requirements. The combined statutory capital and surplus of our HMO and insurance subsidiaries was approximately $926,000 and $858,000 at December 31, 2012 and 2011, respectively, compared to the required statutory surplus of approximately $383,000 and $310,000 at December 31, 2012 and 2011, respectively.
In addition to the foregoing requirements, our regulated subsidiaries are subject to restrictions, which vary by state, on their ability to make dividend payments, loans and other transfers of cash. The maximum amount of dividends which can be paid without prior approval from the applicable state is subject to restrictions relating to statutory capital, surplus and net income for the previous year. States may disapprove any dividend that, together with other dividends paid by a subsidiary in the prior twelve months, exceeds the regulatory maximum as computed for the subsidiary based on its statutory surplus and net income. For the years ended December 31, 2012, 2011 and 2010, we received $192,000, $92,000 and $45,700 respectively, in cash dividends from our regulated subsidiaries.
17. EMPLOYEE BENEFIT PLANS
401(k) Plan
We offer a defined contribution 401(k) plan. Eligible employees of the Company and its subsidiaries may elect to participate in this plan. Participants may contribute a certain percentage of their compensation, subject to maximum Federal and plan limits. We incurred matching contribution expense of $4,297, $3,392 and $3,247 during the years ended December 31, 2012, 2011 and 2010, respectively.
Long-term Incentive Program
Certain of our senior level employees, including executive officers, are eligible for long-term incentive awards ("LTI Program"), consisting of a mix of cash and equity awards, which are granted pursuant to the 2004 Equity Incentive Plan. We designed the LTI Program to motivate and promote the achievement of our long-term financial and operating goals and improve retention. Under the LTI Program, we grant multi-year performance period awards that are not realized by employees and officers until subsequent years. We base award amounts on each participant's pre-established long-term incentive target and allocate the awards to various types of equity awards and performance-based cash, depending on job level. The Compensation Committee has sole discretion of the ultimate funding and payout of awards under the LTI program. We accrued compensation costs related to the LTI Program performance-based cash bonus of $9,700 and $6,880 as of December 31, 2012 and 2011, respectively.
18. QUARTERLY FINANCIAL INFORMATION
Selected unaudited quarterly financial data is as follows (in thousands, except membership and per share data):
|
| | | | | | | | | | | | | | | |
| | For the Three Month Periods Ended |
| | March 31, 2012 | | June 30, 2012 | | September 30, 2012 | | December 31, 2012 |
| Total revenues | $ | 1,791,333 |
| | $ | 1,811,175 |
| | $ | 1,818,395 |
| | $ | 1,988,129 |
|
| Gross margin | 266,756 |
| | 263,043 |
| | 266,921 |
| | 299,563 |
|
| Income from operations | 79,358 |
| | 77,374 |
| | 62,352 |
| | 77,355 |
|
| Income before income taxes | 79,358 |
| | 77,374 |
| | 62,352 |
| | 77,355 |
|
| Net income | 51,232 |
| | 46,442 |
| | 38,287 |
| | 48,767 |
|
| | | | | | | | |
| Net income per share - basic | $ | 1.19 |
| | $ | 1.08 |
| | $ | 0.89 |
| | $ | 1.13 |
|
| Net income per share - diluted | 1.18 |
| | 1.06 |
| | 0.87 |
| | 1.11 |
|
| | | | | | | | |
| Period end membership | 2,533,000 |
| | 2,562,000 |
| | 2,561,000 |
| | 2,669,000 |
|
|
| | | | | | | | | | | | | | | |
| | For the Three Month Periods Ended |
| | March 31, 2011 | | June 30, 2011 | | September 30, 2011 | | December 31, 2011 |
| Total revenues | $ | 1,474,743 |
| | $ | 1,487,635 |
| | $ | 1,544,360 |
| | $ | 1,600,130 |
|
| Gross margin | 209,099 |
| | 283,338 |
| | 327,104 |
| | 330,622 |
|
| Income from operations | 35,043 |
| | 113,475 |
| | 139,976 |
| | 119,173 |
|
| Income before income taxes (a) | 35,043 |
| | 113,475 |
| | 139,976 |
| | 129,980 |
|
| Net income | 21,330 |
| | 69,600 |
| | 88,255 |
| | 85,061 |
|
| | | | | | | | |
| Income from operations per share - basic | $ | 0.82 |
| | $ | 2.65 |
| | $ | 3.26 |
| | $ | 2.77 |
|
| Income from operations per share - diluted | 0.81 |
| | 2.62 |
| | 3.22 |
| | 2.74 |
|
| | | | | | | | |
| Net income per share - basic | $ | 0.50 |
| | $ | 1.63 |
| | $ | 2.06 |
| | $ | 1.98 |
|
| Net income per share - diluted | 0.50 |
| | 1.61 |
| | 2.03 |
| | 1.96 |
|
| | | | | | | | |
| Period end membership | 2,383,000 |
| | 2,391,000 |
| | 2,410,000 |
| | 2,562,000 |
|
| |
| (a) | Income before income taxes for the three month period ended December 31, 2011 includes a gain in the amount of $10,807 resulting from the December 15, 2011 repurchase of all of the tradable unsecured subordinated notes we issued on September 30, 2011 in connection with the stipulation and settlement agreement, which was approved in May 2011, to resolve the putative class-action complaints previously filed against us in 2007. |
The sum of the quarterly earnings per share amounts may not equal the amount reported for the full year since per share amounts are computed independently for each quarter and for the full year based on respective weighted-average shares outstanding and other dilutive potential shares and units.
19. SUBSEQUENT EVENTS
Acquisitions
On January 22, 2013, we entered into an agreement to acquire Missouri Care, Inc., a subsidiary of Aetna, Inc. ("Missouri Care"). As of December 2012, Missouri Care served more than 100,000 Missouri HealthNet Medicaid program members in 54 counties across the state. The transaction is subject to regulatory approvals and certain other closing conditions. We anticipate the transaction will close in the first half of 2013.
On January 31, 2013, we acquired UnitedHealthcare of South Carolina, Inc. ("UHSC"), a South Carolina Medicaid subsidiary of UnitedHealth Group Incorporated that participates in the South Carolina Healthy Connections Choices program in 39 of the state's 46 counties. We will include UHSC's results of operations in our 2013 consolidated financial statements from the date of the acquisition. Due to the timing of the acquisition, we are unable to make a reasonable estimate of the financial effect of the acquisition at this time.
Debt
On February 12, 2013, we borrowed an additional $230,000 in term loans in connection with the execution of an amended senior secured credit agreement (the "Second Amended Credit Agreement"). The Second Amended Credit Agreement provides for an additional $230,000 in term loans and a total available credit facility of $515,000. As of the date of this 2012 Form 10-K, $365,000 total borrowings were outstanding under the Second Amended Credit Agreement. Payments of principal under the Second Amended Credit Agreement term for the years succeeding December 31, 2012 are as follows:
|
| | | |
| | Amended Future Principal Payments |
| 2013 | $ | 38,000 |
|
| 2014 | 41,750 |
|
| 2015 | 60,750 |
|
| 2016 | 224,500 |
|
| | $ | 365,000 |
|
All other terms of the credit facility remain unchanged.
Schedule I
CONDENSED FINANCIAL INFORMATION OF REGISTRANT
WELLCARE HEALTH PLANS, INC. (Parent Company Only)
STATEMENTS OF COMPREHENSIVE INCOME (LOSS)
(In thousands)
|
| | | | | | | | | | | |
| | For the Years Ended December 31, |
| | 2012 | | 2011 | | 2010 |
| Revenues: | | | | | |
| Investment and other income | $ | 82 |
| | $ | 156 |
| | $ | 23 |
|
| Total revenues | 82 |
| | 156 |
| | 23 |
|
| Expenses: | |
| | |
| | |
|
| Selling, general and administrative | 17,418 |
| | 23,408 |
| | 17,432 |
|
| Interest expense | 3,990 |
| | 2,065 |
| | — |
|
| Total expenses | 21,408 |
| | 25,473 |
| | 17,432 |
|
| Loss before income taxes | (21,326 | ) | | (25,317 | ) | | (17,409 | ) |
| Income tax benefit | 5,720 |
| | 7,542 |
| | 5,858 |
|
| Loss before equity in subsidiaries | (15,606 | ) | | (17,775 | ) | | (11,551 | ) |
| Equity in earnings (loss) of subsidiaries | 200,334 |
| | 282,021 |
| | (41,849 | ) |
| Net income (loss) | 184,728 |
| | 264,246 |
| | (53,400 | ) |
| Other comprehensive income, before tax: | | | | | |
| Change in net unrealized gains and losses on available-for-sale securities | 1,544 |
| | 959 |
| | 1,317 |
|
| Income tax expense related to other comprehensive income | 571 |
| | 411 |
| | 507 |
|
| Other comprehensive income, net of tax | 973 |
| | 548 |
| | 810 |
|
| Comprehensive income (loss) | $ | 185,701 |
| | $ | 264,794 |
| | $ | (52,590 | ) |
See notes to consolidated financial statements.
CONDENSED FINANCIAL INFORMATION OF REGISTRANT
WELLCARE HEALTH PLANS, INC. (Parent Company Only)
BALANCE SHEETS
(In thousands, except share data)
|
| | | | | | | |
| | As of December 31, |
| | 2012 | | 2011 |
| Assets | | | |
| Current Assets: | | | |
| Cash and cash equivalents | $ | 3,651 |
| | $ | 72,358 |
|
| Investments | 2,314 |
| | 2,279 |
|
| Taxes receivable | 9,477 |
| | 7,503 |
|
| Deferred income taxes | 70 |
| | 149 |
|
| Affiliate receivables and other current assets | 217,042 |
| | 212,852 |
|
| Total current assets | 232,554 |
| | 295,141 |
|
| Deferred tax asset | 11,799 |
| | 13,211 |
|
| Investment in subsidiaries | 1,269,700 |
| | 1,047,802 |
|
| Deposits and other assets | 1,618 |
| | 1,799 |
|
| Total Assets | $ | 1,515,671 |
| | $ | 1,357,953 |
|
| | | | |
| Liabilities and Stockholders' Equity | |
| | |
|
| Current Liabilities: | |
| | |
|
| Current portion of long-term debt | $ | 15,000 |
| | $ | 11,250 |
|
| Other current liabilities | 57,443 |
| | 94,857 |
|
| Total current liabilities | 72,443 |
| | 106,107 |
|
| Long-term debt | 120,000 |
| | 135,000 |
|
| Total liabilities | 192,443 |
| | 241,107 |
|
| | | | |
| Commitments and contingencies (see Note 12) |
|
| |
|
|
| | | | |
| Stockholders' Equity: | |
| | |
|
| Preferred stock, $0.01 par value (20,000,000 authorized, no shares issued or outstanding) | — |
| | — |
|
| Common stock, $0.01 par value (100,000,000 authorized, 43,212,375 and 42,848,798 shares issued and outstanding at December 31, 2012 and 2011, respectively) | 432 |
| | 429 |
|
| Paid-in capital | 469,498 |
| | 448,820 |
|
| Retained earnings | 854,086 |
| | 669,358 |
|
| Accumulated other comprehensive loss | (788 | ) | | (1,761 | ) |
| Total stockholders' equity | 1,323,228 |
| | 1,116,846 |
|
| Total Liabilities and Stockholders' Equity | $ | 1,515,671 |
| | $ | 1,357,953 |
|
See notes to consolidated financial statements.
CONDENSED FINANCIAL INFORMATION OF REGISTRANT
WELLCARE HEALTH PLANS, INC. (Parent Company Only)
STATEMENTS OF CASH FLOWS
(In thousands)
|
| | | | | | | | | | | |
| | For the Years Ended December 31, |
| | 2012 | | 2011 | | 2010 |
| Net cash (used in) provided by operating activities | $ | (23,356 | ) | | $ | 8,518 |
| | $ | 24,281 |
|
| | | | | | |
| Cash used in investing activities: | |
| | |
| | |
|
| Net proceeds (payments) from purchases and sales and maturities of investments | 938 |
| | (25 | ) | | 1,470 |
|
| Payments to subsidiaries, net | (41,147 | ) | | (95,865 | ) | | (12,394 | ) |
| Net cash used in investing activities | (40,209 | ) | | (95,890 | ) | | (10,924 | ) |
| | | | | | |
| Cash (used in) provided by financing activities: | |
| | |
| | |
|
| Proceeds from debt, net of payment of issuance costs | (585 | ) | | 147,974 |
| | — |
|
| Payments on debt | (11,250 | ) | | (3,750 | ) | | — |
|
| Proceeds from options exercised and other, net | 9,407 |
| | 6,287 |
| | 1,443 |
|
| Purchase of treasury stock | (6,477 | ) | | (3,684 | ) | | (6,237 | ) |
| Incremental tax benefit from option exercises | 3,763 |
| | 2,778 |
| | — |
|
| Net cash (used in) provided by financing activities | (5,142 | ) | | 149,605 |
| | (4,794 | ) |
| | | | | | |
| Cash and cash equivalents: | |
| | |
| | |
|
| (Decrease) increase during year | (68,707 | ) | | 62,233 |
| | 8,563 |
|
| Balance at beginning of year | 72,358 |
| | 10,125 |
| | 1,562 |
|
| Balance at end of year | $ | 3,651 |
| | $ | 72,358 |
| | $ | 10,125 |
|
See notes to consolidated financial statements.
Schedule II — Valuation and Qualifying Accounts
|
| | | | | | | | | | | | | | | |
| | Balance at
Beginning of Period | | Charged to
Costs and
Expenses | | Write Offs | | Balance at
End of Period |
| Year Ended December 31, 2012 | | | | | | | |
| Deducted from assets: | | | | | | | |
| Allowance for uncollectible accounts: | | | | | | | |
| Premiums receivable | $ | 10,367 |
| | $ | 14,896 |
| | $ | 10,420 |
| | $ | 14,843 |
|
| Receivables for non-member claims paid | 4,023 |
| | 1,489 |
| | 5,512 |
| | — |
|
| Medical advances | 1,350 |
| | 150 |
| | — |
| | 1,500 |
|
| Total | $ | 15,740 |
| | $ | 16,535 |
| | $ | 15,932 |
| | $ | 16,343 |
|
| Year Ended December 31, 2011 | | | | | | | |
| Deducted from assets: | | | | | | | |
| Allowance for uncollectible accounts: | | | | | | | |
| Premiums receivable | $ | 16,104 |
| | $ | 7,057 |
| | $ | 12,794 |
| | $ | 10,367 |
|
| Receivables for non-member claims paid | 1,061 |
| | 4,023 |
| | 1,061 |
| | 4,023 |
|
| Medical advances | 1,350 |
| | — |
| | — |
| | 1,350 |
|
| Total | $ | 18,515 |
| | $ | 11,080 |
| | $ | 13,855 |
| | $ | 15,740 |
|
| Year Ended December 31, 2010 | | | | | | | |
| Deducted from assets: | | | | | | | |
| Allowance for uncollectible accounts: | | | | | | | |
| Premiums receivable | $ | 16,216 |
| | $ | 16,086 |
| | $ | 16,198 |
| | $ | 16,104 |
|
| Receivables for non-member claims paid | 7,789 |
| | 1,053 |
| | 7,781 |
| | 1,061 |
|
| Medical advances | 1,350 |
| | — |
| | — |
| | 1,350 |
|
| Sales commissions | 50 |
| | — |
| | 50 |
| | — |
|
| Total | $ | 25,405 |
| | $ | 17,139 |
| | $ | 24,029 |
| | $ | 18,515 |
|
Exhibit Index
|
| | | | |
| | | INCORPORATED BY REFERENCE |
Exhibit Number | Description | Form | Filing Date with SEC | Exhibit Number |
| 2.1 | Agreement and Plan of Merger, dated as of February 12, 2004, between WellCare Holdings, LLC and WellCare Group, Inc. | S-1/A | June 8, 2004 | 2.1 |
| 2.2 | Purchase Agreement, dated as of May 17, 2002, by and among WellCare Holdings, LLC, WellCare Acquisition Company, the stockholders listed on the signature page thereto, WellCare HMO, Inc., HealthEase of Florida, Inc., Comprehensive Health Management of Florida, Inc. and Comprehensive Health Management, L.C. | S-1 | February 13, 2004 | 10.5 |
| 3.1 | Amended and Restated Certificate of Incorporation of the Registrant | 10-Q | August 13, 2004 | 3.1 |
| | a. Amendment to Amended and Restated Certificate of Incorporation | 10-Q | November 4, 2009 | 3.1.1 |
| 3.2 | Third Amended and Restated Bylaws of the Registrant | 8-K | November 2, 2010 | 3.2 |
| 4.1 | Specimen common stock certificate | 10-Q | November 4, 2010 | 4.1 |
| 10.1 | Registration Rights Agreement, dated as of September 6, 2002, by and among WellCare Holdings, LLC and certain equity holders | S-1 | February 13, 2004 | 10.13 |
| MATERIAL AGREEMENTS RELATING TO COMPENSATION AND INDEMNIFICATION | | | |
| 2004 Equity Incentive Plan and Forms Adopted Thereunder | | | |
| 10.2 | Registrant's 2004 Equity Incentive Plan* | 10-Q | August 13, 2004 | 10.4 |
| 10.3 | Forms of Stock Option Agreement under Registrant's 2004 Equity Incentive Plan | | | |
| | a. Adopted in 2004 (Non-Qualified)* | 10-Q | August 13, 2004 | 10.5 |
| | b. Adopted in 2004 (Incentive)* | 10-Q | August 13, 2004 | 10.6 |
| | c. Adopted May 28, 2009 (Non-Qualified)* | 8-K | June 3, 2009 | 10.4 |
| | d. Adopted December 17, 2010* | 8-K | December 20, 2010 | 10.6 |
| 10.4 | Forms of Restricted Stock Agreement under Registrant's 2004 Equity Incentive Plan | | | |
| | a. Adopted March 11, 2005* | 8-K | March 17, 2005 | 10.1 |
| | b. Adopted May 28, 2009 (associate version)* | 8-K | June 3, 2009 | 10.1 |
| | c. Adopted May 28, 2009 (director version)* | 8-K | June 3, 2009 | 10.2 |
| 10.5 | Forms of Restricted Stock Unit Agreement under the Registrant's 2004 Equity Incentive Plan | | | |
| |
a. Adopted May 28, 2009 (associate version)*
| 8-K | June 3, 2009 | 10.3 |
| | b. Adopted March 31, 2010 (associate version)* | 8-K | April 5, 2010 | 10.4 |
| | c. Adopted August 4, 2010 (director version)* | 10-Q | August 9, 2010 | 10.5 |
| | d. Adopted December 17, 2010 (associate version)* | 8-K | December 20, 2010 | 10.2 |
| | e. Adopted December 17, 2010 (with deferral feature; associate version)*
| 8-K | December 20, 2010 | 10.3 |
|
| | | | |
| | | INCORPORATED BY REFERENCE |
Exhibit Number | Description | Form | Filing Date with SEC | Exhibit Number |
| | f. Adopted February 13, 2012 (form of notice; associate version)* | 8-K | February 17, 2012 | 10.9 |
| | g. Adopted February 13, 2012 (form of agreement; associate version)* | 8-K | February 17, 2012 | 10.10 |
| | h. Adopted February 13, 2012 (with deferral feature; form of notice; associate version)* | 8-K | February 17, 2012 | 10.11 |
| | g. Adopted February 13, 2012 (with deferral feature; form of agreement; associate version)* | 8-K | February 17, 2012 | 10.12 |
| | h. Adopted February 13, 2012 (form of notice; director version)* | 8-K | February 17, 2012 | 10.13 |
| | i. Adopted February 13, 2012 (form of agreement; director version)* | 8-K | February 17, 2012 | 10.14 |
| | j. Adopted February 13, 2012 (with deferral feature; form of notice; director version)* | 8-K | February 17, 2012 | 10.15 |
| | k. Adopted February 13, 2012 (with deferral feature; form of agreement; director version)* | 8-K | February 17, 2012 | 10.16 |
| 10.6 | Forms of Performance Stock Unit Agreement under the Registrant's 2004 Equity Incentive Plan | | | |
| | a. Adopted March 31, 2010* | 8-K | April 5, 2010 | 10.3 |
| | b. Adopted December 17, 2010* | 8-K | December 20, 2010 | 10.4 |
| | c. Adopted December 17, 2010 (with deferral feature)* | 8-K | December 20, 2010 | 10.5 |
| | d. Amendment adopted March 24, 2011 (amending agreements on forms adopted March 31, 2010 and December 17, 2010)* | 8-K | March 28, 2011 | 10.4 |
| | e. Adopted March 24, 2011* | 8-K | March 28, 2011 | 10.1 |
| | f. Adopted March 24, 2011 (with deferral feature)* | 8-K | March 28, 2011 | 10.2 |
| | g. Adopted February 13, 2012 (notice)* | 8-K | February 17, 2012 | 10.1 |
| | h. Adopted February 13, 2012 (agreement)* | 8-K | February 17, 2012 | 10.2 |
| | i. Adopted February 13, 2012 (with deferral feature; form of notice)* | 8-K | February 17, 2012 | 10.3 |
| | j. Adopted February 13, 2012 (with deferral feature; form of agreement)*
| 8-K | February 17, 2012 | 10.4 |
| 10.7 | Forms of Market Stock Unit Agreement under the Registrant's 2004 Equity Incentive Plan | | | |
| | a. Adopted February 13, 2012 (form of notice)*
| 8-K | February 17, 2012 | 10.5 |
| | b. Adopted February 13, 2012 (form of agreement)*
| 8-K | February 17, 2012 | 10.6 |
| | c. Adopted February 13, 2012 (with deferral feature; form of notice)*
| 8-K | February 17, 2012 | 10.7 |
| | d. Adopted February 13, 2012 (with deferral feature; form of agreement)* | 8-K | February 17, 2012 | 10.8 |
| | | | | |
| | | | | |
|
| | | | |
| | | INCORPORATED BY REFERENCE |
Exhibit Number | Description | Form | Filing Date with SEC | Exhibit Number |
| 10.8 | Forms of Deferred Stock Unit Agreement under the Registrant's 2004 Equity Incentive Plan | | | |
| | a. Adopted August 4, 2010 (director version)* | 10-Q | August 9, 2010 | 10.6 |
| Other Compensation and Indemnification Plans and Forms of Agreement | | | |
| 10.9 | WellCare Holdings, LLC 2002 Senior Executive Equity Plan* | S-1 | February 13, 2004 | 10.14 |
| 10.10 | Form of Subscription Agreement under 2002 Senior Executive Equity Plan* | S-1 | February 13, 2004 | 10.15 |
| 10.11 | Form of Director Subscription Agreement* | 10-K | February 14, 2006 | 10.14 |
| 10.12 | Form of Non-Plan Time Vesting Option Agreement* | 10-K | February 14, 2006 | 10.20 |
| 10.13 | WellCare Holdings, LLC 2002 Employee Option Plan* | S-1 | February 13, 2004 | 10.16 |
| 10.14 | Form of Time Vesting Option Agreement under 2002 Employee Option Plan* | S-1 | February 13, 2004 | 10.17 |
| 10.15 | 2005 Employee Stock Purchase Plan (No. 333-120257)* | S-8/A | November 24, 2004 | 4.1 |
| | a. Amendment Number 1* | 8-K | September 29, 2006 | 10.1 |
| 10.16 | Long Term Incentive Cash Bonus Plan (with form of Award Agreement adopted March 31, 2010)* | 10-Q | May 6, 2010 | 10.5 |
| | a. Form of Award Agreement (adopted December 17, 2010)* | 8-K | December 20, 2010 | 10.7 |
| | b. Amendment adopted March 24, 2011 (amending awards on forms adopted March 31, 2010 and December 17, 2010) | 8-K | March 28, 2011 | 10.5 |
| | c. Form of Award Agreement (adopted March 24, 2011)* | 8-K | March 28, 2011 | 10.3 |
| 10.17 | Annual Cash Bonus Plan (adopted March 31, 2010)* | 10-Q | May 6, 2010 | 10.4 |
| | a. Amended and restated (adopted December 17, 2010)* | 8-K | December 20, 2010 | 10.8 |
| 10.18 | Summary of WellCare Health Plans, Inc. Relocation Program for Executive Officers * | 10-Q | August 9, 2010 | 10.13 |
| 10.19 | WellCare Health Plans, Inc. Executive Severance Plan* | 8-K | November 21, 2011 | 10.1 |
| | a. Amended and restated (adopted December 21, 2012)* | 8-K | December 28, 2012 | 10.1 |
| 10.20 | Non-Employee Director Compensation Policy as amended and effective for the fiscal quarter commencing January 1, 2011* | 8-K | December 20, 2010 | 10.1 |
| | a. Amended and restated (effective commencing July 1, 2012)* | 10-Q | October 31, 2012 | 10.1 |
| 10.21 | Forms of Indemnification Agreement | | | |
| | a. Adopted May 16, 2003 | S-1/A | June 8, 2004 | 10.24 |
| | b. Adopted May 8, 2009 | 8-K | May 14, 2009 | 10.1 |
| | c. Adopted August 5, 2010 | 10-Q | August 9, 2010 | 10.8 |
| | | | | |
| Agreements with Individual Officers and Directors | | | |
| 10.22 | Separation Agreement and General Release for All Claims, dated as of January 25, 2008, by and among the Registrant, Comprehensive Health Management, Inc. and Todd S. Farha* | 8-K | January 31, 2008 | 10.1 |
| 10.23 | Amended and Restated Non-Qualified Stock Option Agreement, dated as of August 10, 2009, by and between the Registrant and Charles Berg* | 10-Q | November 4, 2009 | 10.3 |
| 10.24 | Indemnification Agreement, dated as of May 14, 2009, by and between the Registrant and Charles Berg* | 8-K | May 14, 2009 | 10.3 |
| 10.25 | Form of Restricted Stock Agreement between the Registrant and Thomas L. Tran* | 8-K | July 17, 2008 | 10.3 |
|
| | | | |
| | | INCORPORATED BY REFERENCE |
Exhibit Number | Description | Form | Filing Date with SEC | Exhibit Number |
| 10.26 | Form of Non-Qualified Stock Option Agreement between the Registrant and Thomas L. Tran* | 8-K | July 17, 2008 | 10.4 |
| 10.27 | Employment Agreement, dated as of October 28, 2009, by and among the Registrant, Comprehensive Health Management, Inc. and Scott D. Law* | 10-Q | May 6, 2010 | 10.3 |
| MATERIAL AGREEMENTS RELATING TO LITIGATION AND INVESTIGATIONS | | | |
| 10.28 | Deferred Prosecution Agreement, made effective as of May 5, 2009, by and among the Registrant, certain subsidiaries and affiliates of the Registrant, the United States Attorney's Office for the Middle District of Florida and the Florida Attorney General's Office | 8-K | May 5, 2009 | 10.1 |
| 10.29 | Consent of Registrant dated May 13, 2009 with respect to Complaint filed by the Securities and Exchange Commission and form of Final Judgment entered by the court on June 1, 2009 | 8-K | May 18, 2009 | 10.1 |
| 10.30 | Stipulation and Agreement of Settlement dated December 17, 2010 between the Registrant and the lead plaintiffs in the matter Eastwood Enterprises, LLC v. Farha, et al. (Case No. 8:07-cv-1940-VMC-EAJ) | 10-K | February 16, 2011 | 10.44 |
| 10.31 | Settlement Agreement dated April 26, 2011 among the United States of America, the Registrant and certain of its subsidiaries and Relators Sean Hellein, Clark J. Bolton, Eugene Gonzalez, and SF United Partners | 10-Q | May 2, 2012 | 10.20 |
| | a. Settlement Agreement with the State of Connecticut | 10-Q | August 3, 2011 | 10.3 |
| | b. Settlement Agreement with the State of Florida | 10-Q | August 3, 2011 | 10.4 |
| | c. Settlement Agreement with the State of Georgia
| 10-Q | August 3, 2011 | 10.5 |
| | d. Settlement Agreement with the State of Hawaii
| 10-Q | August 3, 2011 | 10.6 |
| | e. Settlement Agreement with the State of Illinois | 10-Q | August 3, 2011 | 10.7 |
| | f. Settlement Agreement with the State of Indiana | 10-Q | August 3, 2011 | 10.8 |
| | g. Settlement Agreement with the State of Missouri | 10-Q | August 3, 2011 | 10.9 |
| | h. Settlement Agreement with the State of New York | 10-Q | August 3, 2011 | 10.10 |
| | i. Settlement Agreement with the State of Ohio | 10-Q | August 3, 2011 | 10.11 |
| 10.32 | Corporate Integrity Agreement dated April 26, 2011 between the Office of the Inspector General of the Department of Health and Human Services and the Registrant | 10-Q | August 3, 2011 | 10.1 |
| MATERIAL OPERATIONAL AGREEMENTS | | | |
| 10.33 | Credit Agreement, dated August 1, 2011, among WellCare Health Plans, Inc., The WellCare Management Group, Inc., the lenders party thereto, JPMorgan Chase Bank, N.A., as administrative agent, J.P. Morgan Securities LLC and Wells Fargo Securities, LLC, collectively, as the joint bookrunners and joint lead arrangers, and Wells Fargo Bank, National Association, as syndication agent (the "Credit Agreement") | 8-K | August 3, 2011 | 10.1 |
| | a. Amendment No. 1 | 8-K | July 23, 2012 | 10.1 |
| | b. Amendment No. 2 dated February 12, 2013† | | | |
| 10.34 | Pledge and Security Agreement, dated August 1, 2011, among WellCare Health Plans, Inc., The WellCare Management Group, Inc., the subsidiaries of WellCare Health Plans, Inc. named therein, and JPMorgan Chase Bank, N.A., as administrative agent, for itself and for the Secured Parties (as defined in the Credit Agreement) | 8-K | August 3, 2011 | 10.2 |
|
| | | | | |
| | | INCORPORATED BY REFERENCE |
Exhibit Number | Description | Form | Filing Date with SEC | Exhibit Number |
| 10.35 | Contract No. FA905 by and between the State of Florida, Agency for Health Care Administration and HealthEase of Florida, Inc. (Medicaid Non-Reform 2009-2012) | 8-K | September 16, 2009 | 10.3 |
| | a. Amendment No. 1 | 10-K | February 18, 2010 | 10.55.1 |
| | b. Amendment No. 2 | 10-K | February 18, 2010 | 10.55.2 |
| | c. Minor Modification No. 1 | 10-Q | May 6, 2010 | 10.2 |
| | d. Amendment No. 3 | 10-Q | August 9, 2010 | 10.12 |
| | e. Amendment No. 4 | 8-K | November 15, 2010 | 10.12 |
| | f. Amendment No. 5 | 10-Q | May 6, 2011 | 10.10 |
| | g. Amendment No. 6 | 10-Q | August 3, 2011 | 10.16 |
| | h. Amendment No. 7 | 10-K | February 15, 2012 | 10.55.8 |
| | i. Amendment No. 8 | 8-K | January 17, 2012 | 10.18 |
| | j. Amendment No. 9 | 10-Q | May 2, 2012 | 10.3 |
| | k. Amendment No. 10 | 10-Q | August 3, 2012 | 10.2 |
| | l. Amendment No. 11 | 10-Q | August 3, 2012 | 10.3 |
| | m. Amendment No. 12 | 10-Q | October 31, 2012 | 10.4 |
| 10.36 | Contract No. FA972 by and between the State of Florida, Agency for Health Care Administration and WellCare of Florida, Inc. d/b/a HealthEase (Medicaid Non-Reform 2012-2015) | 8-K | September 24, 2012 | 10.1 |
| | a. Minor Modification No. 1† | | | |
| 10.37 | Contract No. FA904 by and between the State of Florida, Agency for Health Care Administration and WellCare of Florida, Inc. d/b/a Staywell Health Plan of Florida (Medicaid Non-Reform 2009-2012) | 8-K | September 16, 2009 | 10.2 |
| | a. Amendment No. 1 | 10-K | February 18, 2010 | 10.57.1 |
| | b. Amendment No. 2 | 10-K | February 18, 2010 | 10.57.2 |
| | c. Minor Modification No. 1 | 10-Q | May 6, 2010 | 10.1 |
| | d. Amendment No. 3 | 10-Q | August 9, 2010 | 10.11 |
| | e. Amendment No. 4 | 8-K | November 15, 2010 | 10.6 |
| �� | f. Amendment No. 5 | 10-Q | May 6, 2011 | 10.9 |
| | g. Amendment No. 6 | 10-Q | August 3, 2011 | 10.15 |
| | h. Amendment No. 7 | 8-K | January 17, 2012 | 10.9 |
| | i. Amendment No. 8 | 10-Q | August 3, 2012 | 10.1 |
| | j. Amendment No. 9 | 10-Q | October 31, 2012 | 10.3 |
| 10.38 |
| Contract No. FA971 by and between the State of Florida, Agency for Health Care Administration and WellCare of Florida, Inc. d/b/a d/b/a Staywell Health Plan of Florida (Medicaid Non-Reform 2012-2015) | 8-K | September 24, 2012 | 10.2 |
| | a. Amendment No. 1†
| | | |
| 10.39 |
| Amendment No. 12 to Contract 0654 (Amended and Restated Contract 0654) by and between the Georgia Department of Community Health and WellCare of Georgia** | 8-K | January 5, 2012 | 10.1 |
| | a. Amendment No. 13 **
| 8-K | January 5, 2012 | 10.2 |
| | b. Amendment No. 14
| 10-Q | October 31, 2012 | 10.12 |
| 10.40 |
| Medicaid Managed Care Contract dated July 6, 2011, between WellCare Health Insurance of Illinois, Inc. (d/b/a WellCare of Kentucky, Inc.) and the Commonwealth of Kentucky, Finance and Administration Cabinet† | | | |
|
| | | | | |
| | | INCORPORATED BY REFERENCE |
Exhibit Number | Description | Form | Filing Date with SEC | Exhibit Number |
| 2012 Plan Year Agreements with the Centers for Medicare & Medicaid Services | | | |
| 10.41 |
| Contract S5967 dated September 16, 2011 between the Centers for Medicare & Medicaid Services and WellCare Prescription Insurance, Inc. | 8-K | October 13, 2011 | 10.1 |
| 10.42 |
| Form of Contract dated September 16, 2011 between the Centers for Medicare & Medicaid Services and WellCare of Florida, Inc. (H1032) | 8-K | October 13, 2011 | 10.2 |
| 10.43 |
| 2012 Benefit Attestation to Contract H1032 between the Centers for Medicare & Medicaid Services and WellCare of Florida, Inc. | 8-K | October 13, 2011 | 10.6 |
| 10.44 |
| Form of Medicare Mark License Agreement dated September 16, 2011 between the Centers for Medicare & Medicaid Services and each of (a) WellCare of Florida, Inc. (H1032) and (b) WellCare Prescription Insurance, Inc. (S5967) | 8-K | October 13, 2011 | 10.14 |
| 2013 Plan Year Agreements with the Centers for Medicare & Medicaid Services | | | |
| 10.45 |
| Contract S5967 between the Centers for Medicare & Medicaid Services and WellCare Prescription Insurance, Inc. | 8-K | September 19, 2012 | 10.1 |
| 10.46 |
| Form of Contract between the Centers for Medicare & Medicaid Services and WellCare of Florida, Inc. (H1032) | 8-K | September 19, 2012 | 10.2 |
| 10.47 |
| 2013 Benefit Attestation to Contract H1032 between the Centers for Medicare & Medicaid Services and WellCare of Florida, Inc. | 8-K | September 19, 2012 | 10.6 |
| 10.48 |
| Form of Medicare Mark License Agreement between the Centers for Medicare & Medicaid Services and each of (a) WellCare of Florida, Inc. (H1032) and (b) WellCare Prescription Insurance, Inc. (S5967) | 8-K | September 19, 2012 | 10.15 |
|
| | | | |
| 21.1 | List of subsidiaries † | | | |
| 23.1 | Consent of Deloitte & Touche LLP † | | | |
| 31.1 | Certification of Chief Executive Officer pursuant to Section 302 of Sarbanes-Oxley Act of 2002 † | | | |
| 31.2 | Certification of Chief Financial Officer pursuant to Section 302 of Sarbanes-Oxley Act of 2002 † | | | |
| 32.1 | Certification of Chief Executive Officer pursuant to Section 906 of Sarbanes-Oxley Act of 2002 † | | | |
| 32.2 | Certification of Chief Financial Officer pursuant to Section 906 of Sarbanes-Oxley Act of 2002 † | | | |
| 101.INS | XBRL Instance Document †† | | | |
| 101.SCH | XBRL Taxonomy Extension Schema Document †† | | | |
| 101.CAL | XBRL Taxonomy Calculation Linkbase Document †† | | | |
| 101.DEF | XBRL Taxonomy Definition Linkbase Document †† | | | |
| 101.LAB | XBRL Taxonomy Labels Linkbase Document †† | | | |
| 101.PRE | XBRL Taxonomy Presentation Linkbase Document †† | | | |
_______________
|
| | |
| | * | Denotes a management contract or compensatory plan, contract or arrangement |
| | ** | Portions of this exhibit have been omitted pursuant to a request for confidential treatment. |
| | † | Filed herewith |
| | †† | Furnished herewith and not filed for purposes of Section 11 and Section 12 of the Securities Act of 1933 and Section 18 of the Securities Exchange Act of 1934 |