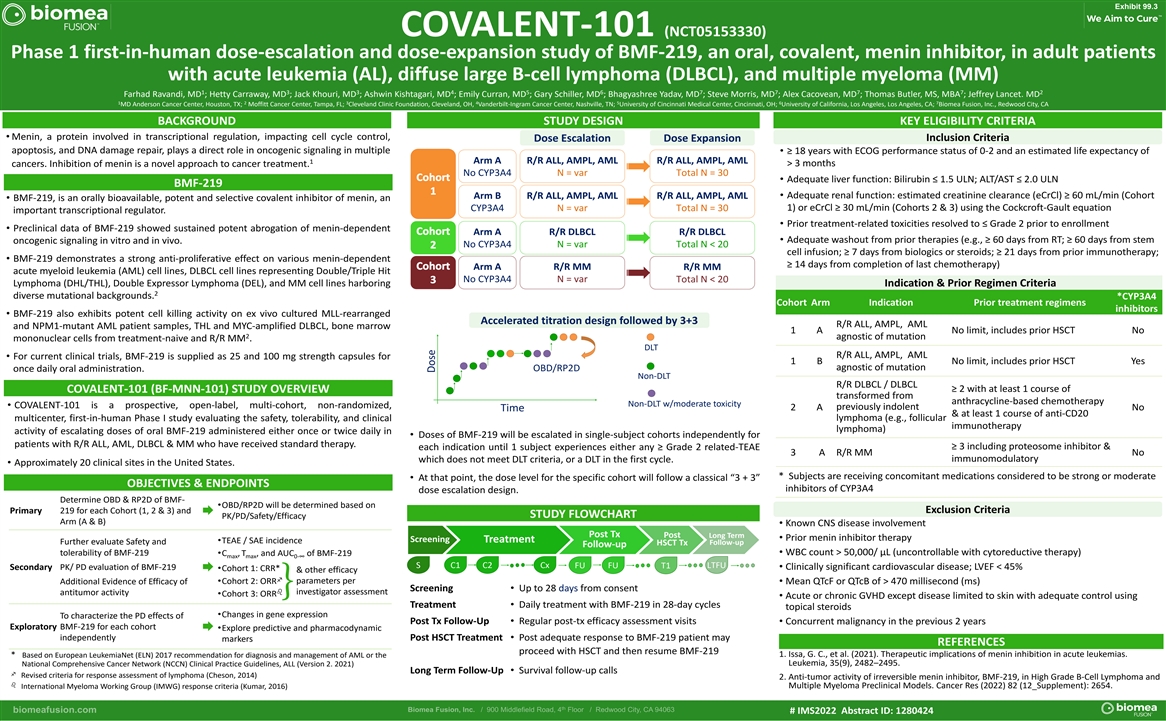
Exhibit 99.3 COVALENT-101 (NCT05153330) Phase 1 first-in-human dose-escalation and dose-expansion study of BMF-219, an oral, covalent, menin inhibitor, in adult patients with acute leukemia (AL), diffuse large B-cell lymphoma (DLBCL), and multiple myeloma (MM) 1 3 3 4 5 6 7 7 7 7 2 Farhad Ravandi, MD ; Hetty Carraway, MD ; Jack Khouri, MD ; Ashwin Kishtagari, MD ; Emily Curran, MD ; Gary Schiller, MD ; Bhagyashree Yadav, MD ; Steve Morris, MD ; Alex Cacovean, MD ; Thomas Butler, MS, MBA ; Jeffrey Lancet. MD 1 2 3 4 5 6 7 MD Anderson Cancer Center, Houston, TX; Moffitt Cancer Center, Tampa, FL; Cleveland Clinic Foundation, Cleveland, OH, Vanderbilt-Ingram Cancer Center, Nashville, TN; University of Cincinnati Medical Center, Cincinnati, OH; University of California, Los Angeles, Los Angeles, CA; Biomea Fusion, Inc., Redwood City, CA BACKGROUND STUDY DESIGN KEY ELIGIBILITY CRITERIA • Menin, a protein involved in transcriptional regulation, impacting cell cycle control, Inclusion Criteria Dose Escalation Dose Expansion apoptosis, and DNA damage repair, plays a direct role in oncogenic signaling in multiple • ≥ 18 years with ECOG performance status of 0-2 and an estimated life expectancy of Arm A R/R ALL, AMPL, AML R/R ALL, AMPL, AML 1 > 3 months cancers. Inhibition of menin is a novel approach to cancer treatment. No CYP3A4 N = var Total N = 30 • Adequate liver function: Bilirubin ≤ 1.5 ULN; ALT/AST ≤ 2.0 ULN BMF-219 • Adequate renal function: estimated creatinine clearance (eCrCl) ≥ 60 mL/min (Cohort Arm B R/R ALL, AMPL, AML R/R ALL, AMPL, AML • BMF-219, is an orally bioavailable, potent and selective covalent inhibitor of menin, an 1) or eCrCl ≥ 30 mL/min (Cohorts 2 & 3) using the Cockcroft-Gault equation CYP3A4 N = var Total N = 30 important transcriptional regulator. • Prior treatment-related toxicities resolved to ≤ Grade 2 prior to enrollment • Preclinical data of BMF-219 showed sustained potent abrogation of menin-dependent Arm A R/R DLBCL R/R DLBCL • Adequate washout from prior therapies (e.g., ≥ 60 days from RT; ≥ 60 days from stem oncogenic signaling in vitro and in vivo. No CYP3A4 N = var Total N < 20 cell infusion; ≥ 7 days from biologics or steroids; ≥ 21 days from prior immunotherapy; • BMF-219 demonstrates a strong anti-proliferative effect on various menin-dependent ≥ 14 days from completion of last chemotherapy) Arm A R/R MM R/R MM acute myeloid leukemia (AML) cell lines, DLBCL cell lines representing Double/Triple Hit No CYP3A4 N = var Total N < 20 Lymphoma (DHL/THL), Double Expressor Lymphoma (DEL), and MM cell lines harboring Indication & Prior Regimen Criteria 2 diverse mutational backgrounds. *CYP3A4 Cohort Arm Indication Prior treatment regimens inhibitors • BMF-219 also exhibits potent cell killing activity on ex vivo cultured MLL-rearranged Accelerated titration design followed by 3+3 R/R ALL, AMPL, AML and NPM1-mutant AML patient samples, THL and MYC-amplified DLBCL, bone marrow 1 A No limit, includes prior HSCT No 2 agnostic of mutation mononuclear cells from treatment-naive and R/R MM . DLT R/R ALL, AMPL, AML • For current clinical trials, BMF-219 is supplied as 25 and 100 mg strength capsules for 1 B No limit, includes prior HSCT Yes agnostic of mutation OBD/RP2D once daily oral administration. Non-DLT R/R DLBCL / DLBCL ≥ 2 with at least 1 course of COVALENT-101 (BF-MNN-101) STUDY OVERVIEW transformed from anthracycline-based chemotherapy Non-DLT w/moderate toxicity • COVALENT-101 is a prospective, open-label, multi-cohort, non-randomized, previously indolent 2 A No Time & at least 1 course of anti-CD20 lymphoma (e.g., follicular multicenter, first-in-human Phase I study evaluating the safety, tolerability, and clinical immunotherapy lymphoma) activity of escalating doses of oral BMF-219 administered either once or twice daily in • Doses of BMF-219 will be escalated in single-subject cohorts independently for patients with R/R ALL, AML, DLBCL & MM who have received standard therapy. ≥ 3 including proteosome inhibitor & each indication until 1 subject experiences either any ≥ Grade 2 related-TEAE 3 A R/R MM No immunomodulatory which does not meet DLT criteria, or a DLT in the first cycle. • Approximately 20 clinical sites in the United States. * Subjects are receiving concomitant medications considered to be strong or moderate • At that point, the dose level for the specific cohort will follow a classical “3 + 3” OBJECTIVES & ENDPOINTS inhibitors of CYP3A4 dose escalation design. Determine OBD & RP2D of BMF- •OBD/RP2D will be determined based on Exclusion Criteria 219 for each Cohort (1, 2 & 3) and Primary Æ STUDY FLOWCHART PK/PD/Safety/Efficacy Arm (A & B) • Known CNS disease involvement Post Tx Post Long Term • Prior menin inhibitor therapy Screening Treatment •TEAE / SAE incidence Further evaluate Safety and Follow-up HSCT Tx Follow-up • WBC count > 50,000/ μL (uncontrollable with cytoreductive therapy) tolerability of BMF-219 •C , T , and AUC of BMF-219 max max 0-∞ S C1 C2 Cx LTFU FU FU T1 PK/ PD evaluation of BMF-219 • Clinically significant cardiovascular disease; LVEF < 45% Secondary •Cohort 1: CRR* Æ & other efficacy f parameters per •Cohort 2: ORR Additional Evidence of Efficacy of • Mean QTcF or QTcB of > 470 millisecond (ms) Screening • Up to 28 days from consent } b investigator assessment antitumor activity •Cohort 3: ORR • Acute or chronic GVHD except disease limited to skin with adequate control using Treatment • Daily treatment with BMF-219 in 28-day cycles topical steroids •Changes in gene expression To characterize the PD effects of Post Tx Follow-Up • Regular post-tx efficacy assessment visits • Concurrent malignancy in the previous 2 years BMF-219 for each cohort Exploratory •Explore predictive and pharmacodynamic Æ independently Post HSCT Treatment • Post adequate response to BMF-219 patient may markers REFERENCES proceed with HSCT and then resume BMF-219 1. Issa, G. C., et al. (2021). Therapeutic implications of menin inhibition in acute leukemias. * Based on European LeukemiaNet (ELN) 2017 recommendation for diagnosis and management of AML or the Leukemia, 35(9), 2482–2495. National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines, ALL (Version 2. 2021) Long Term Follow-Up • Survival follow-up calls f Revised criteria for response assessment of lymphoma (Cheson, 2014) 2. Anti-tumor activity of irreversible menin inhibitor, BMF-219, in High Grade B-Cell Lymphoma and b Multiple Myeloma Preclinical Models. Cancer Res (2022) 82 (12_Supplement): 2654. International Myeloma Working Group (IMWG) response criteria (Kumar, 2016) # IMS2022 Abstract ID: 1280424 Dose