Exhibit 99.12
POSTER P2157
The pharmacokinetics (PK) and pharmacodynamics (PD) of the fluticasone furoate (FF) and vilanterol (VI) combination in subjects with hepatic impairment
Allen A(1), Hardes K(2), Kempsford RD(1), Tombs L(3)
(1)GlaxoSmithKline, Gunnels Wood Road, Stevenage Herts, SG1 2NY, UK; (2)GlaxoSmithKline, Stockley Park West, Uxbridge, Middlesex, UB11 1BT, UK; (3)Synergy, Slough, Berkshire, SL3 6EZ, UK
INTRODUCTION
· FF/VI, a novel inhaled corticosteroid/long-acting beta2-agonist combination (ICS/LABA) is being developed as a once-daily inhaled treatment for asthma and COPD.
· FF and VI both undergo extensive first-pass metabolism and are predominantly metabolised in the liver via cytochrome P450 3A4 (CYP3A4).(1),(2)
· Hepatic dysfunction can lead to substantial alterations in drug absorption, distribution and elimination(3),(4) and the Food and Drug Administration and the European Medicines Agency both recommend that the effect of liver disease on the pharmacokinetics of drugs under development is studied.(5),(6)
OBJECTIVES
· To investigate the effect of hepatic impairment (HI) on the pharmacokinetics, pharmacodynamics and safety of FF/VI.
METHODS
· Open-label, parallel-group repeat dose study.
· Subjects with mild (n=9; Child-Pugh A) and moderate (n=9; Child-Pugh B) hepatic impairment, and healthy subjects (n=9) received the FF/VI 200/25 mcg combination (as two inhalations of FF/VI 100/12.5 mcg) via a novel dry powder inhaler once daily for 7 days.
· An interim review showed subjects with moderate hepatic impairment to have 65% higher FF AUC(0–24) values than healthy subjects, hence the FF/VI dose was subsequently reduced to 100/12.5 mcg in subjects with severe hepatic impairment (n=8; Child-Pugh C).
· PK parameters of FF and VI were assessed on Days 1 and 7.
· Systemic PD effects of FF (0–24 hour serum cortisol) and VI (0–4 hour heart rate and serum potassium) were assessed on Day 7.
· PK concentrations and parameters were dose-normalised by multiplying the values for the severe hepatic impairment cohort by 2, putting the data on the same scale as the other 3 groups.
· PK parameter point estimates and corresponding 90% confidence intervals (CIs) were constructed for the ratio of the geometric means (each hepatically impaired group : healthy subject group).
· For the PK comparisons between the two groups, non-inferiority was defined as an upper 90% CI of <2 for the geometric mean ratio (hepatically impaired : healthy) on Day 7.
RESULTS
· Thirty-five subjects were enrolled. Demographic characteristics were generally similar across treatment groups, although the mean age of the severe hepatic impairment group was slightly greater than the other groups (57.8 years versus 50.3–52.1 years).
· Only one adverse event occurred (mild back pain in a healthy subject). There were no withdrawals.
· Following repeat inhaled FF/VI administration FF Cmax was observed at on average 0.5 to 3 hours post-dose (Figure 1). VI Cmax was observed at on average 5 minutes post-dose across all groups (Figure 2).
· Non-inferiority was established for all VI PK comparisons between hepatically impaired and healthy subjects as all upper 90% CI limits were <2 (Table 1).
· Non-inferiority between treatment groups was not demonstrated in terms of FF AUC(0–24), as the upper 90% CI limits for the ratios were all >2 (all hepatically impaired groups : healthy subjects [Table 1]).
· The FF elimination t½ was longer in hepatically impaired subject groups (mean 30.9 to 53.5 hours) compared with healthy subjects (mean 23.9 hours).
· Higher accumulation (Day 7 : Day 1) of FF and VI occurred in subjects with hepatic impairment than in healthy subjects in terms of AUC(0-8) and Cmax (Table 2).
Figure 1. Mean FF plasma concentration-time profiles (Day 1 and Day 7) after administration of FF/VI to subjects with hepatic impairment and healthy subjects (semi-log scale)
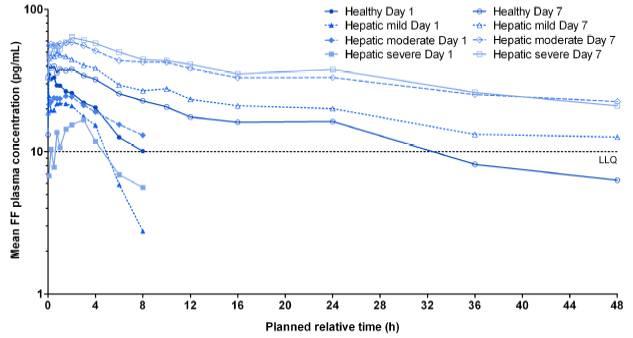
Note: Data for subjects with severe hepatic impairment normalised to 200/25 mcg
Figure 2. Mean VI plasma concentration-time profiles (Day 1 and Day 7) after administration of FF/VI to subjects with hepatic impairment and healthy subjects (semi-log scale).
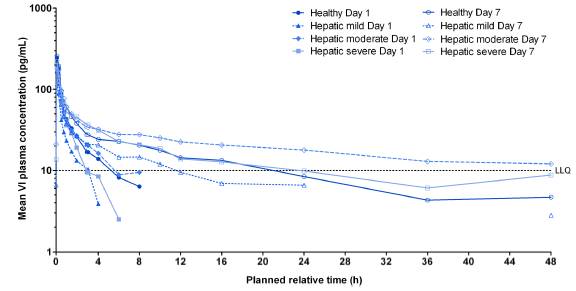
Note: Data for subjects with severe hepatic impairment normalised to 200/25 mcg
· There was no evidence of a difference (HI - healthy subjects) in systemic beta-agonist PD effects. Differences (90% CI) in heart rate for mild, moderate and severe HI were: 3.8 bpm (–1.2, 8.8), 3.2 bpm (–1.7, 8.1) and –2.4 bpm (–7.7, 3.0) and for serum potassium were 0.04 mmol/L (–0.19, 0.27), –0.11 mmol/L (–0.34, 0.12) and 0.15 mmol/L (–0.10, 0.40), respectively.
· No clinically relevant effects on weighted mean (0–24 hour) serum cortisol were noted in subjects with mild hepatic impairment, or subjects with severe hepatic impairment to whom a lower dose of FF/VI 100/12.5 mcg was given.
· In subjects with moderate hepatic impairment, there was an average decrease of 34% (90% CI: 11% decrease to 51% decrease) in weighted mean (0–24 hour) serum cortisol, compared with healthy subjects.
Table 1. Statistical comparison of PK parameters between subjects with hepatic impairment and healthy subjects
|
|
|
|
|
| Comparison with healthy subjects |
| ||
|
|
|
|
|
| Ratio of GM (90% CI) |
| ||
Parameter |
| Day |
| Group |
| Fluticasone furoate |
| Vilanterol |
|
AUC(0–8) |
| 1 |
| Mild HI |
| 0.67 (0.33, 1.35) |
| 0.40 (0.26, 0.62) |
|
(pg.h/mL) |
|
|
| Moderate HI |
| 0.98 (0.49, 1.98) |
| 0.93 (0.58, 1.48) |
|
|
|
|
| Severe HI |
| 0.18 (0.09, 0.38) |
| 0.58 (0.37, 0.91) |
|
AUC(0–24) |
| 7 |
| Mild HI |
| 1.34 (0.82, 2.20) |
| 0.66 (0.40, 1.08) |
|
(pg.h/mL) |
|
|
| Moderate HI |
| 1.83 (1.11, 2.99) |
| 1.33 (0.92, 1.91) |
|
|
|
|
| Severe HI |
| 1.75 (1.05, 2.91) |
| 0.72 (0.43, 1.20) |
|
Cmax |
| 1 |
| Mild HI |
| 0.81 (0.57, 1.15) |
| 0.47 (0.33, 0.69) |
|
(pg/mL) |
|
|
| Moderate HI |
| 0.81 (0.57, 1.16) |
| 0.74 (0.50, 1.11) |
|
|
|
|
| Severe HI |
| 0.60 (0.42, 0.86) |
| 0.74 (0.50, 1.09) |
|
Cmax |
| 7 |
| Mild HI |
| 1.18 (0.83, 1.69) |
| 0.63 (0.43, 0.91) |
|
(pg/mL) |
|
|
| Moderate HI |
| 1.43 (1.00, 2.04) |
| 0.78 (0.52, 1.17) |
|
|
|
|
| Severe HI |
| 1.37 (0.95, 1.98) |
| 0.83 (0.57, 1.23) |
|
GM = geometric mean; CI = confidence interval; HI = Hepatic impairment
Table 2. Determination of accumulation of FF and VI in subjects with hepatic impairment and healthy subjects
|
|
|
| Fluticasone furoate |
| Vilanterol |
|
|
|
|
| Day 7:Day 1 ratio of GM |
| Day 7:Day 1 ratio of GM |
|
Parameter |
| Group |
| (90% CI) |
| (90% CI) |
|
AUC(0–8) |
| Healthy |
| 1.60 (1.05, 2.44) |
| 1.50 (1.201 1.85) |
|
(pg.h/mL) |
| Mild HI |
| 2.89 (1.89, 4.40) |
| 2.57 (2.07, 3.18) |
|
|
| Moderate HI |
| 2.59 (1.70, 3.96) |
| 1.81 (1.42, 2.30) |
|
|
| Severe HI |
| NE |
| 2.18 (1.73, 2.73) |
|
Cmax |
| Healthy |
| 1.21 (0.90, 1.61) |
| 1.09 (0.89, 1.35) |
|
(pg/mL) |
| Mild HI |
| 1.77 (1.32, 2.36) |
| 1.44 (1.17, 1.78) |
|
|
| Moderate HI |
| 2.12 (1.59, 2.84) |
| 1.15 (0.91, 1.46) |
|
|
| Severe HI |
| 2.76 (2.03, 3.75) |
| 1.23 (0.99, 1.54) |
|
GM = geometric mean; CI = confidence interval; HI = Hepatic impairment
NE = not estimated (insufficient quantifiable data on Day 1 due to low dose)
Note: Data for subjects with severe hepatic impairment normalised to 200/25 mcg
CONCLUSIONS
· In subjects with hepatic impairment there was no increase in VI systemic exposure or beta-agonist mediated systemic effects.
· FF exposure was increased, on average, <2-fold in subjects with HI and was associated with a reduction in serum cortisol of approximately 30% compared with healthy subjects.
REFERENCES
(1) Hughes SC, et al. Drug Metab Dispos 2008;36:2337–2344.
(2) Harrell A, et al. ERS 2011. Abstract P821.
(3) McLean AJ, et al. Clin Pharmacokinet 1991;21:42–69.
(4) Westphal JF, et al. Drug Saf 1997;17:47–73.
(5) Guideline on the evaluation of the pharmacokinetics of medicinal products in patients with impaired hepatic function. Available at http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2009/09/WC500003122.pdf [Last accessed 11 July 2012].
(6) Guidance for Industry: Pharmacokinetics in patients with impaired hepatic function: study design, data analysis, and impact on dosing and labelling. Available at http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/ucm072123.pdf [Last accessed 11 July 2012].
ACKNOWLEDGEMENTS
· R. Kempsford is an employee of GlaxoSmithKline.
· This study was funded by GlaxoSmithKline; GSK Study Code HZA111789, Clinicaltrials.gov NCT01266941.
· Editorial support in the form of copyediting and assembling of figures was provided by Ian Grieve at Gardiner-Caldwell Communications and was funded by GlaxoSmithKline.
![]()
Presented at the Annual Conference of the European Respiratory Society, Vienna, September 1–5, 2012